Embed Size (px)
Citation preview

Persistent Pain in Older Persons:
Challenges and Solutions
Stephen J Gibson
Deputy Director, National Ageing Research Institute
Professor, Department of Medicine, University of Melbourne

Why should we be interested in pain in older age? – Prevalence and impact.
Evidence-based treatment approaches. – Multidisciplinary pain clinics.
– Providing training and best integrated treatment in residential aged care.
– Treatment approaches for pain and its impacts in persons with dementia.

Age
90 80 70 60 50 40 30 20 10
50
40
30
20
7-37%
17-50%
25-65%
25-56%
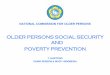
Pain prevalence across the life-span
13% 16% 27% 25% Blyth et al. 2001

Prevalence of Radiographic OA
0
25
50
75
100
Hands
Knees
Feet
Pre
vale
nce
(%
)
18-24 25-34 35-44 45-54 55-64 65-74 75-79
Age Range (years)
NHANES Study 2003

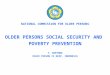
Prevalence Studies of Pain in Nursing Home Residents Adapted from Takai et al, Pain Management Nursing 2010
0%
10%
20%30%
40%
50%
60%
70%80%
90%
100%
Van
Her
k 20
09To
rvik
200
9Zw
akha
len
2009
Hal
on 2
009
Cado
gan
200
8R
eyn
olds
200
8B
oerl
age
2008
Saw
yer
2007
Smal
bru
gge
2007
Leo
ng 2
007
Ach
terb
erg
2007
d'A
stol
lo 2
006
Asg
hari
200
6Ts
e 20
05Ch
u 2
004
Teno
200
4Ts
ai 2
004
Won
200
4A
llcoc
k 20
02M
cCle
an 2
002
Proc
tor
2001
Won
199
9W
eine
r 1
999
Wag
ner
199
7Fe
rrel
l 199
5Se
ngst
aken
199
3Fe
rrel
l 199
0
Studies = 27 Median size = 341 Total Residents = 2,249,882
Median prevalence = 52%

“But Dr, I can’t learn to live with it!”
Biopsychosocial impacts of chronic pain

Disturbed Mood
40%-70% of older persons with pain have
depression. 2.6 times more likely to suicide

Dementia, depression and pain
* *
healthy

Impacts on function

Age and functional disability
Score
Yong, Bell, Workman, Gibson (2003), PAIN, 104, 673-681
18-39 y
40-59 y
60-79 y
80 + y
Physical Psychosocial
* *
* *

Other impacts of persistent pain
• Sleep
• Neurocognitive performance
• Addiction-polypharmacy
• Financial stress
• Social relationships
• Physical health
• Quality of life

Neuropsychological test performance in
older patients with chronic pain Measure Pain-Free (N = 160) CLBP (N = 163) P Value
RBANS—Immediate memory 103.56 (13.99) 95.53 (15.50) 0.002
RBANS—Visuospatial 96.48 (17.57) 95.67 (16.78) 0.671
RBANS—Language 102.87 (12.59) 97.14 (10.45) 0.004
RBANS—Attention 105.96 (15.53) 101.34 (14.53) 0.007
RBANS—Delayed memory 97.91 (15.31) 94.41 (16.11) 0.046
Trails B (T score)-Exec function 53.57 (11.36) 46.73 (10.22) 0.009
Grooved Pegboard 45.04 (9.39) 42.76 (11.02) 0.047
NART—VIQ 98.32 (14.77) 98.16 (13.29) 0.919
For all measures, higher scores indicate better performance.
RBANS = Repeatable Battery for the Assessment of Neuropsychological Status; CLBP = chronic
low back pain; NART—VIQ = National Adult Reading Test–– verbal IQ.
Weiner et al. Pain Med. (2010), 7, 60-70
*
*
*
*
*
No r/ship with depression or comorbidity

Other impacts of persistent pain
• Sleep
• Neurocognitive performance
• Addiction-polypharmacy
• Financial stress
• Social relationships
• Physical health
• Quality of life

Under-treatment of pain in older persons
System wide under-treatment of pain across
multiple health care settings (hospital, sub-
acute, long term care facilities). • Fewer standing orders for post-operative analgesia. (Morrison & Sui
2000, Pasero & McCaffery 1996).
• Relative under-prescription of analgesics in those with metastatic
cancer. (Bernabei et al. 1998, Cleeland et al. 1994).
• 31% with moderate pain in residential aged care receive no analgesics.
Only 13% of PRN orders given. (McClean et al. 2002, Scherder 1997).
Age bias against treatment at multidisciplinary
pain clinics. (Kee et al. 1998). • 28% of clinics never admitted a person over 70.
• 40% had indirect age barriers (i.e return to work, no comorbidity).
• Based on fictitious clinical vignette, where only age differed, older
persons were judged to be 15% less likely to be suitable for admission
and 12.5% less likely to succeed with treatment.

Staff attitudes (old don’t need as much
care, nothing can be done, takes too much
time, limited treatment options).
Patient fears and beliefs (addiction,
institutionalization, polypharmacy,
complainer, >stoicism,>pain a normal part
of ageing).
Fears and ageist beliefs

Treatment of Pain in the older person
“Wheeze in please”

The Melbourne Pain Clinic for Older Persons
• Clinic opened in 1987 within a comprehensive
aged care service.
• Conforms to IASP definition of a multidisciplinary
pain centre.
– Multimodal approach
– Caters for all types of chronic pain
– Several treatment specialties with communal case
conferencing (Dr, Physio, Psych, Nurse, OT, Pharm)
– Provides ongoing research and training
• Currently 3 pain clinics for older persons in
Melbourne and 10 throughout the World.

Melbourne Pain Clinic: Treatment Process
• Multidisciplinary assessment over 3 sessions. – Pain problem, comorbidity, medications, geriatric
syndrome
– Level of disability, mood disturbance, QoL, social issues
• Multidisciplinary case conference to discuss pain cause(s) and treatment options.
• Treatment plan presented to patient. – Individual medical only
– Individual medical + psychology, physiotherapy
– Multidisciplinary program with group CBT, exercise program, psychological therapy, home nursing
– Reject or refer to other services
• Program continues for about 3/12 although longer support is available if required.

Melbourne Pain Clinic Group Program • Week 1 - Activity analysis
– Introduction, Current lifestyle, Activity diary
• Week 2 - Relaxation and Stress – Understanding physical and psychological responses
– Relaxation tape, Stress management
• Week 3 - Time Management – Principles of time management & goal setting,
Prioritization, Relaxation
• Week 4 - Coping Strategies – Discussion re coping strategies,
– Affirmative statements
• Week 5 - Reconceptualisation – Negative thoughts, Problem solving, Relaxation
• Week 6 - Review – Discussion of program, Relaxation

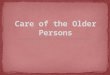
7%
29%
26%
15%
15% 6%
14%
Less Pain
More Activity
Melbourne Pain Clinic: Outcomes
Better Mood
Other RCT’s of CBT/pain clinics for older persons also show
benefits: Puder 1988, Cook 1998, Pawlick 2002, Ersek et al.
2006, Martire et al. 2013.

EBPRAC: Implementing the Australian Pain Society Guidelines
2007 2005

Aim of the Project
The major objective was to provide a comprehensive education and training program to aged care staff within five selected residential
aged care facilities and thereby establish a sustainable implementation of best practice pain
assessment and management.

Phase 1: Pre-operational activities: Involved securing ethics approvals; convening an expert working party, finalize access to facilities including recruitment of residents and development of project scheduling.
Phase 2: Facility specific audit , prepare for implementation: This phase involved the collection/analysis of current resident pain and management practice; pain documentation and management protocols; survey of staff, residents/families. The audit data was used to guide change management procedures and education activities.
Phase 3: Education, training and implementation: An intensive education program for all staff; familiarity with APS guidelines; use of pain-assessment instruments and revised in-house pain-management procedures. Activities involved dedicated 1:1 on-the-job training. The appointment of facility “pain champions” who coordinated activities within each facility.
Phase 4: Evaluation and sustainability: The collection of post-implementation data and comparing to baseline data. The evaluation addresses outcomes for residents, staff and the facility as well as sustainability as indexed by adoption of changes into institutional policy and practice.
Methods

APS Guidelines
Achieved? Comments
12. A combination of pharmacological and non-pharmacological treatment therapies are incorporated into pain management plans for residents.
Action Required
The range of non-pharmacological treatments is not comprehensive and is very limited availability. A coordinated non-pharmacological/pharmacological treatment plan does not exist for most
residents.
13. Pharmacological treatments are based on a diagnosis and consider co-existing medical conditions.
Yes
14. Medications are tailored to type of pain and it’s severity.
Action Required
Large number of PRN orders versus ATC orders for analgesics even in those with persistent pain.
15. There is around the clock
administration of analgesic medication for residents with persistent pain.
Action Required
See above
16. Residents who fail to respond to therapy and who continue to be distressed by pain should be referred to a pain medicine specialist or a multidisciplinary pain clinic.
Action Required
Note lack of use of external pain management resources.
Summary audit report to the facility

Resident Outcomes
0
10
20
30
40
50
60
Mild Moderate Severe Most Intense
% of residents
Average Self rated Pain: Pre-Post
Self-Rated pain BPI
Pre
Post
Self reported pain EBPRAC: Pain outcomes
n = 84
Savvas et al. JAGS In press

“You gotta be kidding! Your back still hurts?”

0
1
2
3
4
5
6
7
8
9
Abbey PAINAD NOPAIN
Pre
Post
*
*
*
Observer rated pain scales
Observer rated, n = 395
EBPRAC: Pain outcomes
Savvas et al. JAGS In press

*
*
*
0
5
10
15
20
25
30
35
40
mood activity enjoy
Pre
Post
Resident Outcomes
Self-rated interference of pain (% with moderate+ impact)
*
Self reported pain impact
* P<0.05
EBPRAC: Pain impacts
Savvas et al. JAGS In press

Analgesic medications: Outcomes
0
10
20
30
40
50
60
Nil PRN ATC ATC +PRN
Cog Imp-pre
Cog Imp-post
EBPRAC: Analgesic Use
Savvas et al. JAGS In press

0
5
10
15
20
25
30
Heatpacks
TENS Exercise CBT
Pre
Post
EBPRAC: Non-Pharmac treatments
Savvas et al. JAGS In press

Staff Outcomes: Knowledge
“I think what has changed is that I’m more aware of you know, signs
[of] pain, how to identify pain … So I would tell the nurses and they
would take it from there …but it’s more knowledge and the aware bit .”
“I think a lot of PCs realise they are responsible for it and not just the
RNs and ENs. That’s definitely changed. You’re seeing more hot packs
used, more rubs used, more repositioning. So they’re (PCAs) realising
they have more of a role to play with pain management, whereas that
was missing before. Yes, they’re more well informed..” RN
• Overall, approximately 350 aged care staff were involved
in the complete training program and over 4000 hours of
instruction and training were delivered across the project.

Facility Outcomes: Overall
standards met pre
standard improved post
Additional standards met post
Total compliance
Facility A 11 6 10 21
Facility B 10 7 10 20
Facility C 6 8 13 19
Facility D 8 10 9 17
Facility E 12 6 4 16
Assessed on 27 key pain standards pre and post training

Pain and BPSD
• Unrelieved pain has been identified as a possible cause of BPSD
• Pain is associated with higher levels of BPSD
• Those suffering from pain and dementia are consistently prescribed and administered fewer analgesics than cognitively intact residents
• Can appropriate analgesic treatment reduce pain-related BPSD?

Aim of the study: Provide an
analgesic intervention to residents to
specifically monitor changes in pain
and consequent changes in the
frequency of BPSD
• 90 participants will be split into 3
groups of 30
• Placebo
• Paracetamol
• Paracetamol + Codeine
• Double blind - research staff
and aged care staff will be
unaware of which group the
resident is in.

BMJ 2011;343:d4065 doi: 10.1136/bmj.d4065 Page 1 of 10
Efficacy of treating pain to reduce behavioural disturbances in residents of nursing homes with dementia: cluster randomised clinical trial Bettina S Husebo postdoctoral fellow1, Clive Ballard professor2, Reidun Sandvik registered nurse1, Odd Bjarte Nilsen statistician 3, Dag Aarsland professor 4
Research

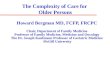
Mobid Pain scores
Husebo B et al. BMJ 2011
2
2.2
2.4
2.6
2.8
3
3.2
3.4
3.6
3.8
4
week 0 week 2 week 4 week 8 week 12
MO
BID
pai
n s
core
control
intervention

Treating pain to reduce BPSD
Standardised protocol to treat pain in NH residents with
moderate to severe dementia. N = 352
Husebo B et al. BMJ 2011

Treating pain to reduce BPSD
• Cohen-Mansfield agitation inventory improved by 17%
Comparison:
• 3 RCTs of risperidone for BPSD using the Cohen-Mansfield agitation inventory reported 3%, 13% and 18% advantages compared with placebo.
Husebo B et al. BMJ 2011
Deberdt WG et al. Am J Geriatr Psych 2005
Brodaty H et al. J Clin Psychiatry 2003
De Deyn PP et al. Neurology 1999

Summary, Future Directions & Challenges
Pain is very common in older persons but is under-treated. It can have major impacts on mood, function, cognition and Q of L.
Our studies show that appropriate treatment can greatly reduce pain and suffering in older persons.
– Integrated multidisciplinary care in the community.
– Multimodal evidence-based programs in residential care.
– Reduced pain impacts in persons with dementia.
Further research and improved training is needed.
– Must implement current knowledge into better practice.
– Need widespread education on pain in older persons.
– Development of new treatment approaches.

“Although coordination of care can always be improved at the "micro" level via local initiative and the efforts of enlightened individuals, it is only with the improvement of national systems of care that the appropriate conditions and incentives for coordination and integration of care for older people will truly exist and flourish.”
Clarfield M, Bergman H, Kane R. Fragmentation of Care for Frail Older People an
International Problem. Experience from Three Countries: Israel, Canada, and the United States
Journal of the American Geriatrics Society 2001 49 12 1714


Melbourne Pain Clinic: Staffing & Roles
• Medical
– Full Ax, Medical Hx
–Pharmacological
–Referral, eg. joint
replacement, laminectomy
Physiotherapy
– Functional Ax
–Exercise programs
– TENS
• Psychological / OT – Cognitive-behavioural
approach
– Relaxation, guided imagery, goal setting, stress management
– Individual counselling
• Nursing – Home visit, assist with
initial questionnaire information
• Pharmacy – Review medications,
information on drug use

Stepwise pain treatment protocol
Step
Pain treatment at baseline
Study treatment
Dosage
No (%) of residents (n=175)
1
No analgesics, or low dose of paracetamol
Paracetamol (acetaminophen)
Maximum dose 3 g/day
120 (69)*
2
Full dose of paracetamol or low dose morphine
Morphine 5 mg twice daily; maximum dose 10 mg twice daily
4 (2)
3
Low dose buprenorphine or inability to swallow
Buprenorphine transdermal patch
5 µg/h, maximum dose 10 µg/h
39 (22)†
4 Neuropathic pain Pregabalin
25 mg once daily; maximum dose 300 mg/day
12 (7)

Behavioral and Psychological
Symptoms of Dementia (BPSD)
• Definition: Symptoms of disturbed perception, thought content, mood or behavior that frequently occur in patients with dementia (Finkel & Burns, 1999)
• Challenging behaviors such as screaming, wandering, aggression, agitation, and physical violence
• Seriously effects quality of life
• A major cause of distress, burden and physical trauma in staff, other residents and family members
• Psychotropic medications/antipsychotic agents (suppression of symptoms) remain the most common form of management
• Associated with increased health care costs due to greater supervision, medical practitioner call-out, staff turn-over and absenteeism

There is growing international recognition that many BPSD are not
simply part of the dementing process but rather represent behavioral
symptoms of an unmet need
• Instead of normal
verbal communication, people with moderate
–advanced dementia
express their needs via
non-typical and often challenging behavioral
symptoms
• Understanding and
targeting the cause of the behavior provides a
better alternative than
trying to suppress the
behavioral symptom via chemical or physical
restraints

Resident Outcomes
“Yes I am regularly asked about the pain by all members
of staff. Different levels of staff ask about pain.”
“It’s surprising the amount of relief I get from just the wheat pack.
The heated wheat pack is marvellous. It is a really consoling
sort of treatment.”
“I’m quite happy with it [the TENS machine]… I’ve been told it won’t
cure it but it takes away a lot of that pain… there’s nothing more
that I can do as far as I am concerned because that has more or less
fixed me up for what I wanted.”