Embed Size (px)
Citation preview

Clinical Expert Series
Persistent Occiput Posterior
William H. Barth, Jr, MD
Persistent occiput posterior (OP) is associated with increased rates of maternal and newbornmorbidity. Its diagnosis by physical examination is challenging but is improved with bedsideultrasonography. Occiput posterior discovered in the active phase or early second stage of laborusually resolves spontaneously. When it does not, prophylactic manual rotation may decreasepersistent OP and its associated complications. When delivery is indicated for arrest of descentin the setting of persistent OP, a pragmatic approach is suggested. Suspected fetal macrosomia,a biparietal diameter above the pelvic inlet or a maternal pelvis with android features shouldprompt cesarean delivery. Nonrotational operative vaginal delivery is appropriate when thematernal pelvis has a narrow anterior segment but ample room posteriorly, like with anthropoidfeatures. When all other conditions are met and the fetal head arrests in an OP position ina patient with gynecoid pelvic features and ample room anteriorly, options include cesareandelivery, nonrotational operative vaginal delivery, and rotational procedures, either manual orwith the use of rotational forceps. Recent literature suggests that maternal and fetal outcomeswith rotational forceps are better than those reported in older series. Although not withoutsignificant challenges, a role remains for teaching and practicing selected rotational forcepsoperations in contemporary obstetrics.
(Obstet Gynecol 2015;125:695–709)
DOI: 10.1097/AOG.0000000000000647
There are levels of the game to every game, as presumptuous hobby-ists learn to their sorrow. At one time in my life, I fancied myselfpretty good—O.K., maybe even a little better than pretty good—atdoing crossword puzzles. Then I met Stanley Newman.
—James Kaplan, The New York Times, July 10, 2005
I trained in an era and at an institution with facultywho taught operative vaginal delivery including Kiel-
land rotations. By the time I finished residency, I hadaccumulated a fair experience with forceps, includingrotational forceps. I thought I was pretty good, and
better than most in the management of persistent occi-put posterior (OP). Then, I met Lenny Safon.
Dr. Leonard Safon, a Boston obstetrician then inhis mid 60s, seemed to live on Labor and Delivery,often staying late into the night to deliver his patientseven when not on call. He won our teaching award somany times that it was eventually named for him. Lateone night, we began a discussion about persistent OP,and it became obvious to me that I was an amateur, orworse, an overconfident amateur. Lenny used termsand concepts that I had memorized only for in-serviceexaminations. I was certainly not applying them asknowledgably to my practice. Sensing this, Lennymade a generous offer and for the next 2 years, hewould page me to come to Labor and Delivery ifavailable for what became an unofficial apprentice-ship in the management of persistent OP.
Despite this kind of experience and the continu-ous practice of obstetrics for 25 years since that time,there remains a phone call that still provokes in me animmediate and visceral anxiety: “Hi, Bill. Mrs. Jones,who you have not met, has been pushing for 3-1/2hours and we think the fetus may be OP. Can youcome to labor and delivery?” Experiencing somedegree of anxiety with this call is not logical. Why,
From the Department of Obstetrics and Gynecology, Division of Maternal-FetalMedicine, Massachusetts General Hospital, Harvard Medical School, Boston,Massachusetts.
Continuing medical education for this article is available at http://links.lww.com/AOG/A604.
Corresponding author: William H. Barth Jr, MD, Department of Obstetrics andGynecology, Division of Maternal-Fetal Medicine, Massachusetts GeneralHospital, Harvard Medical School, Massachusetts General Hospital/Founders418, 55 Fruit Street, Boston, MA 02114; e-mail: [email protected].
Financial DisclosureThe author did not report any potential conflicts of interest.
© 2015 by The American College of Obstetricians and Gynecologists. Publishedby Wolters Kluwer Health, Inc. All rights reserved.ISSN: 0029-7844/15
VOL. 125, NO. 3, MARCH 2015 OBSTETRICS & GYNECOLOGY 695
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

after my training and experience, does this still causeconcern? Often the patient is exhausted. The nursesare commonly frustrated. The patient’s family is con-cerned, and some may be angry. In a short period oftime I must gain the patient’s confidence and trust. Ihave to review a now abnormal labor course, evalu-ate the patient and her fetus clinically, counsel herabout the nuanced risks and benefits of cesareancompared with vaginal delivery, and, if recommend-ing the latter, recruit the support of the nurses andother health care providers and prepare for and per-form an operative vaginal delivery without harmingthe mother or the fetus. I profess no greater or lesserskill with forceps, including rotational forceps, thanany of my contemporaries. Accordingly, this com-munication is not about the broader topic of opera-tive vaginal delivery covered by Yeomans1 earlier inthis series. Rather, I focus on the problem of persis-tent OP and offer an approach that is appropriate forcontemporary practice. It is centered on Dr. Safon’smost important admonition to me: “Bill, not all OPsare the same.”
DEFINITION
Persistent OP is when the occiput remains in theposterior quadrants of the pelvis until delivery,whether that delivery is spontaneous or indicated fora nonreassuring fetal status or arrest of descent in thesecond stage.
INCIDENCE
The incidence of persistent OP ranges from 5–12%.2–6
Right OP is the most common (60%) followed by leftOP (30%) and direct OP (10%).7,8 Occiput posterior istwice as common among nulliparous women as mul-tiparous women.4,9 Importantly, the incidence of OPvaries depending on the time of ascertainment inlabor. Authors relying on ultrasonograms to assessfetal head position throughout labor report thatapproximately 50% of fetuses engage or begin laborin the occiput transverse position with the remainderdivided equally between occiput anterior (OA) andOP.5,6,10 Among those beginning labor in the OP posi-tion, most (80–90%) will rotate to OA before sponta-neous or assisted delivery.3,6,10 Spontaneous rotationto OA is often a late phenomenon and may not occuruntil well into the second stage of labor. Although OPdiscovered late in labor is more likely to persist,50–80% of those beginning the second stage in anOP position will still rotate spontaneously to OAbefore delivery.5,6,11 Malrotation from OA to OP israre (less than 5%) once the second stage has begun.6
ETIOLOGY
Factors that may influence the risk of persistent OPinclude the shape of the pelvis, epidural analgesia,parity, race, and others. For decades, standard teach-ing in obstetrics suggested that features of the femalebony pelvis were a major determinant of engagementand descent of the fetal head during labor.12–15 Giventhe typical shape of the fetal head, it was assumed thatat each level of the pelvis, there was an optimal posi-tion for the fetal head to pass and that, as a generalrule, the larger fetal occiput tended to rotate to thatportion of the pelvis with the most room. The shape ofthe pelvis does have some influence on the final posi-tion at the time of delivery. This is supported by stud-ies showing a tendency for OP to recur in subsequentpregnancies and radiographic studies showing a higherrate of OP among women with features of an anthro-poid pelvis.8,13,16–18 There are racial differences in pel-vic architecture. Handa and colleagues19 studiedpatients with and without anal sphincter tears fromthe Childbirth and Pelvic Symptoms Study (CAPS)with magnetic resonance imaging. Confirming earlierstudies, these authors demonstrated that white womenhad wider pelvic inlets and outlets, whereas AfricanAmerican women had deeper anteroposterior outlets.This may partially explain the increased prevalence ofpersistent OP seen among African American womenin recent observational studies.20,21
The relationship between the use of epiduralanalgesia and persistent OP is complex. The associ-ation between epidural analgesia and an increasedrate of persistent OP at the time of delivery seen inretrospective cohort studies21,22 has not been con-firmed in randomized trials. A meta-analysis of foursuch trials demonstrated no difference in the rate ofmalposition at the time of delivery among womenwho were randomized to epidural analgesia com-pared with those randomized to other methods orno analgesia (relative risk 1.40, 95% confidence inter-val [CI] 0.98–1.99).23 If the mechanism by whichepidurals are thought to increase the risk of persistentOP is by causing a more relaxed and accommodatinglevator complex, we should see more persistent OPamong multiparous women and that is not the case.Observational studies consistently show that persis-tent OP is more common among nulliparous thanmultiparous women by a factor of more than twoto one.4,8,9 Large retrospective cohort studies suggestthat other factors such as race, nulliparity, body massindex (calculated as weight (kg)/[height (m)]2) higherthan 30, macrosomia, maternal age older than 35years, augmentation of labor, and anterior placental
696 Barth Persistent Occiput Posterior OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

location may also contribute to persistent OP, butnone of these, either singly or together, reliably pre-dict persistent OP.18,21,22
MATERNAL MORBIDITY
Occiput posterior is associated with higher rates ofdystocia, cesarean delivery, operative vaginal deliv-ery, failed operative vaginal delivery, and severeperineal lacerations (third and fourth degree). Largeretrospective cohort studies consistently demonstratethat OP is associated with longer first and secondstages of labor, prolonged labor, and the need foraugmentation.4,9,21 Senécal and colleagues24 demon-strated that the second stage of labor was approxi-mately 45 minutes longer if the fetus was OPcompared with OA at the onset of the second stagewhether pushing started immediately or was delayed.The likelihood of cesarean delivery increases the laterin labor that OP is noted. It is not associated with anincreased risk of cesarean delivery when noted beforelabor, is associated only weakly in early labor, andbecomes strongly associated with cesarean deliveryif persisting into the second stage.5,24,25 When persist-ing to the point at which delivery is indicated, OP isassociated with a 4- to 10-fold increase in the risk ofcesarean delivery with absolute rates as high as65%.4,6,22 Occiput posterior is associated with a 6- to11-fold increase in the need for operative vaginaldelivery26–28 and a 5- to 10-fold increase in the rateof failed operative vaginal delivery.21,29
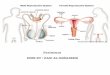
Vaginal delivery from OA is most often associ-ated with a well-flexed fetal head causing the sub-occipitobregmatic diameter (approximately 9.5 cm) topass through the outlet and over the perineal body(Fig. 1). Occiput posterior positions are associatedwith more extended attitudes of the fetal head, prob-ably as a result of forward impingement of the mater-nal sacral promontory on the fetal spine and resultingextension of the neck. With extended attitudes, thediameter that must pass through the outlet is some-where between the occipitofrontal (approximately11.5 cm) and the occipitomental (approximately13.5 cm) (Fig. 1). As such, it is no surprise that OPis associated with substantially higher rates of third-and fourth-degree perineal lacerations.4,9,30 Adjustingfor episiotomy, forceps, vacuum, and other factors,Cheng and colleagues21 reported that delivery in theOP position doubled the risk of third- or fourth-degree extension (relative risk 2.4, 95% CI 2.0–2.8).Modern cohort studies report absolute rates of third-and fourth-degree extensions with operative vaginaldelivery from OP ranging from 33% with a vacuumto as high as 50–70% with forceps.20,29 In a recent
case–control study from the National Institute ofChild Health and Human Development and the Pel-vic Floor Disorders Network, Fitzgerald and col-leagues reported odds ratios (ORs) for sphincterinjury with OP, forceps, or the two combined of 7.0,13.6, and 21.6, respectively. Vacuum deliveries fromOP were associated with an OR of 9.7.31 The highestrisk resulted from the combination of OP, forceps,and episiotomy (OR 33.8, 95% CI 4.8–239.5).
Cesarean delivery in the second stage of labor,especially if the second stage is prolonged, is associ-ated with higher risks of bleeding and surgical injury,such as inadvertent extension of the hysterotomy intothe cervix, vagina, uterine artery, and broad liga-ment.32–37 At least one study has demonstrated a dou-bling of the risk of such extensions when the occiput isposterior.34
NEWBORN OUTCOMES
Older studies reported more abnormal fetal heartpatterns with persistent OP including more variableand late decelerations and more bradycardia.38–40
There are no contemporary studies examining intra-partum fetal heart rate patterns with persistent OPrelying on the newer National Institute of ChildHealth and Human Development classification sys-tem. The neonatal morbidity associated with OP oc-curs primarily among those who require operativevaginal delivery and does not extend to those deliv-ered spontaneously.30,41 Cheng and colleagues41 com-pared the outcomes of 2,591 newborns delivered from
Fig. 1. Anteroposterior diameters of a newborn head. Forocciput anterior delivery, the suboccipitobregmatic diam-eter (green) typically passes through the outlet and over theperineal body. For occiput posterior deliveries, the largeroccipitofrontal (yellow) or occipitomental (red) diameterstypically pass through the outlet as a result of extension ofthe fetal head.
Barth. Persistent Occiput Posterior. Obstet Gynecol 2015.
VOL. 125, NO. 3, MARCH 2015 Barth Persistent Occiput Posterior 697
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

OP to 28,801 delivered from OA. Newborns deliv-ered from OP had higher rates of low Apgar scores(OR 1.5, 95% CI 1.17–1.91), cord gas acidemia (OR2.05, 95% CI 1.52–2.77), meconium (OR 1.29, 95%CI 1.17–1.42), birth trauma (OR 1.77, 95% CI 1.22–2.57), and neonatal intensive care unit admission (OR1.57, 95% CI 1.28–1.92). When the authors adjustedfor other factors that influence newborn outcome andstratified patients by mode of delivery, almost all ofthese associations weakened or disappeared. The onlyoutcome associated with OP that remained significantwith an OR exceeding 2 was birth trauma amongthose with operative vaginal delivery.
DIAGNOSIS
The determination of fetal head position is typicallymade by physical examination. Unfortunately, suchexaminations are notoriously inaccurate before fulldilation of the cervix.10,42,43 The accuracy of physicalexamination improves as labor progresses into thesecond stage, but not as much as one might think.Among five contemporary prospective cohort studiescomparing the accuracy of digital vaginal examinationwith that of ultrasonography for determination ofposition in the second stage, the rate of errors exceed-ing 45° ranged from 30–80%.44–48 In some studies,almost half of the physical examinations that werewrong were off by more 135°.45,48 Clinicians are ableto determine OA positions more accurately (80–85%)than OP positions (50–60%).45,49 Factors such as sta-tion, molding, caput, and experience of the examiner
do not dramatically affect the accuracy of physicalexamination.44,45,48
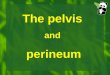
Most studies that use ultrasonography to deter-mine fetal head position show it to be highlyreproducible in experienced hands.50 These examina-tions are typically performed with a portable ultra-sound system with a transducer held in thetransverse position just above the symphysis pubis.Determining position of the fetal occiput depends ondemonstrating the position of the fetal orbits, the falx,and the fetal spine (Fig. 2). Although ultrasonographycan be more accurate than digital vaginal examinationin the second stage of labor, I do not believe it isessential before all operative vaginal deliveries. How-ever, when the physical examination is not clear,more liberal use of ultrasonography before rotationhas the potential to improve the safety of such deliv-eries in contemporary practice.
MANAGEMENT
For purposes of this communication, I consider themanagement of OP as it may be encountered incontemporary practice: 1) before the onset of labor; 2)during active labor before full dilation; 3) early in thesecond stage; and finally, 4) once delivery is indicatedfor arrest of descent or nonreassuring fetal status in thesecond stage. Interventions that have been describedfor the first three are intended to prevent persistentOP and include maternal positioning and prophylac-tic manual rotation. When additional waiting is nolonger an option, interventions in the last scenario
Fig. 2. Transabdominal ultrasounddetermination of the fetal occiput.Direct occiput posterior with bothfetal orbits facing the transducer(A), right occiput posterior withthe fetal orbits facing anteriorly tothe maternal left (B), right occiputanterior with the fetal cerebellumseen anteriorly to the maternalright (C), and occiput anterior bylocalization of the fetal spine inthe sagittal plane (D).
Barth. Persistent Occiput Posterior.Obstet Gynecol 2015.
698 Barth Persistent Occiput Posterior OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

include cesarean delivery and operative vaginal deliv-ery with or without rotation. For this last situation, Ipropose an ordered approach that I have foundhelpful when called to assist in the second stage inthe setting of persistent OP.
Before the Onset of Labor
If asked to consult before labor, I would not alterrecommendations for standard obstetric management.First, the majority of fetuses will rotate to an anteriorposition during labor, even late in labor. Occiputposterior before labor predicts neither an increasedrisk of cesarean delivery nor the final position at thetime of delivery.10,51 Second, there are no interven-tions before labor that are effective in decreasing per-sistent OP. Karimina and colleagues52 randomized2,500 women with singleton pregnancies to handsand knees position with pelvic rocking from 37 weeksof gestation until delivery. The rate of persistent OP inthe treatment group (105/1,298 [8.1%]) was no differ-ent than that in the control group (98/1,255 [7.8%]).
During the First Stage of Labor
If consulted about an OP position in the first stage oflabor, my response is similar. At most, such informationmight heighten my vigilance regarding fetal position inthe second stage, but there is no evidence to supportmaternal positioning to encourage rotation of the occiputin the active phase.53 Stremler and colleagues54 random-ized 147 women with ultrasonography-confirmed OPpositions in labor to as much time as possible in theknee–chest position or to a control group instructed toassume any position other than knee–chest. Women inthe treatment group had no significant increase in theproportion that was OA 1 hour after the intervention orat delivery. In another clinical trial, Desbriere and col-leagues55 randomized women in active labor confirmedby ultrasonography to be in the OP position to eithera dorsal recumbent position or to purposeful maternalpositioning that was intended to encourage rotation. Theauthors noted no differences in any important clinicaloutcomes, including fetal head position at delivery, dura-tion of the first or second stage of labor, length of push-ing, rates of operative vaginal delivery, cesareandelivery, or perineal tears. Consequently, if consultedfor arrest of dilation or a protraction disorder associatedwith OP before full dilation, I would recommend stan-dard management with oxytocin unless otherwise con-traindicated and I would move to cesarean delivery ifthis did not solve the problem. Importantly, I wouldavoid and recommend against any attempt to rotatethe fetal head before full dilation of the cervix. Beforefull dilation, the failure rate of manual rotation is high,
and at least one group has reported cord prolapse, cer-vical lacerations, and nonreassuring fetal heart rate pat-terns with such attempts.56,57
Early in the Second Stage
If the fetal status is reassuring and labor is progressing,there is no immediate need to intervene simply for OPat the beginning of the second stage. In this setting,conservative management without intervention hasbeen advocated for decades.8,58–60 Because spontane-ous rotation to OA is so common, if performed tooearly, any manual rotations or complications arisingfrom them are likely to have been unnecessary. Thedilemma arises as OP persists longer into the secondstage. As it does, the probability of spontaneous rota-tion decreases and the likelihood of adverse outcomesassociated with delivery from OP increases (cesareandelivery, operative vaginal delivery, maternal perineallacerations, and fetal effects of operative vaginal deliv-ery). Compounding this dynamic, manual rotation ismore likely to be successful if performed early than ifit is attempted once an arrest of labor has occurred.56
In light of this, recent authors have advocated“prophylactic manual rotation” earlier in the secondstage as a means of preventing persistent OP. Retro-spective cohort studies demonstrate significantlylower rates of cesarean delivery when manual rota-tions are successful and high rates of success when itis attempted.56,61–63 In the only prospective study todate, Reichman and colleagues64 enrolled womenwith a fetus in the OP position halfway into the secondstage (1 hour for nulliparous women, 30 minutes formultiparous women, +30 minutes if laboring with anepidural). Compared with the expectant managementgroup, those who underwent prophylactic rotationwere more commonly OA at delivery (93% comparedwith 15%, P,.001), more likely to have a spontaneousvaginal delivery (77% compared with 27%, P,.001),and less likely to require operative vaginal delivery(23% compared with 50%, P,.001) or cesarean deliv-ery (0 compared with 23%, P,.001). Although noneof these studies are without limitations, this approachappears to have few downsides for the mother orfetus. The only adverse maternal outcome of note inthese reports is the possibility of a slight increase inthe risk of cervical lacerations but with an absoluterisk that remains low (approximately 2%). Newbornoutcomes are generally the same or better amongthose undergoing manual rotation.62,64 The risk ofemergency cesarean delivery for an abnormal fetalheart rate tracing precipitated by a prophylactic man-ual rotation is approximately 1%.56,64 Given the lowrisks of prophylactic manual rotation and the potential
VOL. 125, NO. 3, MARCH 2015 Barth Persistent Occiput Posterior 699
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

for significant reductions in cesarean delivery andother adverse outcomes associated with delivery fromOP, my current practice is to wait for some period oftime—approximately 1 hour for nulliparous womenand 30 minutes for multiparous women, possibly lon-ger with an epidural—and then evaluate the patient fora prophylactic manual or digital rotation. If my pelvicexamination suggests crowding in the anterior seg-ment and ample room posterior, like with an anthro-poid pelvis, OP may be the most optimal position,and I do not attempt a prophylactic manual rotation.
Technique for Manual or Digital Rotation
Numerous variations of manual and digital rotation ofthe fetal occiput have been described previously.65–68
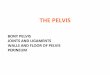
The main difference between the two is that with man-ual rotations, the whole hand is placed in the vagina tograsp the fetal head, whereas with digital rotations,only two fingers are inserted to apply rotational force.For manual rotations from left OP, the operator’s righthand is placed in the vagina palm up with four fingersspread evenly across the left side of the fetal headfrom occiput to chin with the thumb gently heldacross the opposite side (Fig. 3A). The fetal head isslightly destationed, flexed, and rotated counterclock-wise to left OA or OA by pronation of the operator’sright hand. The operator’s left hand can be used toreach across the maternal abdomen and pull the rightfetal shoulder from the maternal left to right side con-current with the rotation. For manual rotations fromright OP, the hands and directions are exactly
reversed. The operator’s left hand is placed in thevagina, palm up, with four fingers spread across theright side of the fetal head and the thumb gently heldacross the opposite side. Again, the fetal head isslightly elevated, flexed, and rotated clockwise toa right OA position. Although guidance varies in priorreports, I have found manual rotations more easilyaccomplished between contractions and in those pa-tients with an epidural in place. I have also found thatbreaking down the labor bed and placing the patientin a dorsal lithotomy position with the hips flexed andlegs supported before the attempt allows me to com-plete the rotation more easily as my elbow dropstoward the floor and below the patient’s buttocks asI complete pronation while maintaining flexion of thefetal head. I generally withdraw my thumb and keepmy four fingers in position, applying gentle pressureuntil the head settles into position, sometimes imme-diately, sometimes only with the next contraction.Digital rotations are similar, but with only two fingersinserted into the vagina to find and hold the posterioredge of the upper parietal bone near the junction ofthe lambdoid suture and posterior fontanel (Fig. 3B).With either type of rotation, if gentle force does notaffect rotation, there are only two maneuvers to con-sider before abandoning the attempt, flexing the headmore or elevating slightly to a higher station. Flexingthe fetal head will decrease the diameter that must berotated, and elevating may find a more favorable levelof the pelvis to allow rotation, especially if moldinghas taken place. The two techniques, manual and
Fig. 3. A. Manual rotation of left occiput posterior to left occiput anterior. With the right hand facing palm up, four fingersare placed inferiorly and spread across the left side of the fetal head with the thumb on the right side. While flexing the fetalhead, the operator rotates the occiput counterclockwise into the anterior segment of the pelvis. B. Digital rotation leftocciput posterior to left occiput anterior. The index and middle fingers are used to locate and apply counterclockwisepressure in a dialing motion on the posterior margin of the right parietal bone at the right lambdoidal suture. A is reprintedand B is modified from Hale RW, editor. Posterior presentations of the occiput. In: American College of Obstetricians andGynecologists. Dennen’s forceps deliveries. 4th ed. Washington, DC: American College of Obstetricians and Gynecologists;2001.
Barth. Persistent Occiput Posterior. Obstet Gynecol 2015.
700 Barth Persistent Occiput Posterior OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

digital rotation, have not been compared with eachother with regard to ease, safety, or efficacy, but thereare some important differences. First, manual rota-tions tend to be more uncomfortable for the patient,because the operator’s whole hand is inserted androtated within the vagina along with the fetal head.Second, because the head must generally be elevatedslightly more to place the fingers correctly around thefetal head with manual rotation, care must be takennot to disengage the head because cord prolapse ispossible with the rush of amniotic fluid that often ac-companies this maneuver. Finally, the ultimate choicemay be health care provider-dependent. Because myhands are larger, I generally prefer to attempt a digitalrotation first, especially if the rotation is performedprophylactically to prevent persistent OP.
Persistent Occiput Posterior With Arrest ofDescent or Nonreassuring Fetal Status
This, by far, is the most challenging situation for theclinician, especially if called on to consult or assumecare for the patient late in the course of labor oncepersistent OP has become a problem that must beaddressed. In this situation, I believe there are fivecritical questions that must be answered to guide themethod of delivery (Box 1).
Is Delivery Indicated at This Time?Because OP is associated with longer second stages, itis especially important to distinguish between a pro-longed second stage and arrest of descent. Since 1988,the American College of Obstetricians and Gynecol-ogists has defined a prolonged second stage as greaterthan 2 hours for nulliparous women and greater than1 hour for multiparous women unless an epidural is inplace, in which case these times are 3 hours and 2hours, respectively.69 An arrest of descent need notcoincide with these times and occurs when there hasbeen no descent of the fetal vertex in 1 hour despiteadequate maternal expulsive efforts. If the fetal statusis reassuring, maternal efforts are strong, and progressin descent is being made, an additional amount of
time to allow spontaneous vaginal delivery of the per-sistent OP may be perfectly appropriate. On the otherhand, if arrest of descent has occurred in the OP posi-tion despite adequate maternal efforts, it is unlikelythat additional time without intervention will be suc-cessful and some form of operative intervention isindicated, whether abdominal or vaginal. Typically,if consulted for arrest of descent in the second stagewith persistent OP, my experience is that the patientwill usually have been pushing beyond the typicaldefinitions of a prolonged second stage and interven-tion is almost invariably warranted.
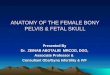
Is Vaginal Delivery Contraindicated?There are three contraindications to operative vaginaldelivery that are especially important in arrest ofdescent with persistent OP. These are suspected fetalmacrosomia, a high station, or a pelvis with markedandroid features, raising the possibility of dangerousoutlet obstruction. To avoid these pitfalls when calledto consult for a patient I have not previously seen, Ihave found it helpful to follow a standard approach(Fig. 4). I begin by confirming or ascertaining theestimated fetal weight by reviewing any recent ultra-sound reports and performing Leopold’s maneuversmyself. If macrosomia is suspected, operative vaginaldelivery for arrest of descent in the second stage iscontraindicated whether the fetus is OP or not.70
The second contraindication is more unique to persis-tent OP. For decades, authors have warned of theoccurrence of extreme molding and caput formationwith persistent OP such that the biparietal diametermay remain deceptively higher than suspected withvaginal examination.58,68 Indeed, with persistent OPand a prolonged second stage, the biparietal diametermay be above the ischial spines and possibly still nearthe inlet, although the scalp may be visible at thevaginal introitus. Therefore, if I can palpate the bipar-ietal diameter abdominally with Leopold’s third orfourth maneuvers (Fig. 5A and B) in the setting ofan arrest of descent in the OP position, I know thestation is high and delivery must be by cesarean, evenif the scalp is visible on the perineum.
In the absence of suspected macrosomia andprovided I do not feel the biparietal diameter abdom-inally, I move on to a careful pelvic examination withattention to the fetal position and specific features ofthe maternal bony pelvis. Like many obstetricians, Imemorized the Caldwell Moloy pelvic types asa resident, primarily for test-taking purposes. How-ever, it is in this setting that an understanding of thepelvic types and their features remains extremelyhelpful. In my opinion, the third contraindication to
Box 1. Questions That Must Be Answered toGuide the Method of Delivery for PersistentOcciput Posterior
1. Is delivery indicated at this time?2. Is vaginal delivery contraindicated?3. What is the true position of the fetal head?4. Should rotation be considered before vaginal
delivery?5. If rotating, which method is preferred?
VOL. 125, NO. 3, MARCH 2015 Barth Persistent Occiput Posterior 701
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

proceeding with operative vaginal delivery in thesetting of persistent OP is a pelvis with markedandroid features, suggesting the possibility of a dan-gerous outlet obstruction described even by theearliest writers in this area.12,58 This occurs as a resultof the narrow or crowded anterior segment forcing thevertex posterior combined with the forward sacrumand short posterior segment producing the potentiallydangerous bony obstruction. With this in mind, I con-tinue with the maneuvers shown in Figure 5. Ifandroid features are noted at this point (narrow sub-pubic arch, narrow retropubic angle, a short sacrospi-nous ligament, or palpably forward lower third of thesacrum) in the setting of arrest of descent with persis-tent OP (and OA in my own practice), cesarean deliv-ery is indicated to avoid the potential for fetal andmaternal morbidity. If, on the other hand, I do notget the sense of android features, I proceed to the nextstep.
What is the True Position of the Fetal Head?Concurrent with the careful examination of the pelvis,I try to confirm OP by palpation of the anteriorfontanel, sometimes aided by palpation of an ear ifpossible. If I have any doubt at all, I rely onultrasonography to confirm the position of the
occiput. For direct OP positions, I have also foundthat ultrasound detection of the fetal spine helps me indetermining the proper direction of rotation.Although unusual, the direction of the fetal occiputand spine at the level of the thorax is not alwaysconcordant (Fig. 6) and suggests to this author thatrotation in what appears to be the short arc is notalways the correct route.
If Vaginal Delivery Is Not Contraindicated,Should Rotation Be Considered?If on pelvic examination the anterior segment iscrowded (narrow retropubic angle and subpubic arch),but there is ample room in the posterior segment typicalof an anthropoid pelvis, there is no benefit to rotatingthe larger fetal occiput into a narrow or crowdedanterior segment. Indeed, anterior rotation of the largerocciput in the setting of an acute subpubic arch withlonger inferior pubic rami and a narrow transverseoutlet will necessarily force the vertex posterior andincrease risk to the perineum and rectal sphinctermuscles. In this setting, I would recommend anoperative vaginal delivery from OP without rotation.Because forceps fail less often than vacuum in thesetting of persistent OP, I prefer them. Also, becausearrest of descent with persistent OP is invariably
Is the fetus >4,500 grams?
No
Is the biparietal diameter palpable abdominally?
No
Are basic requirements for operative vaginal delivery met?
Yes
Careful examination of the pelvis
Anthropoid features Gynecoid features
Deliver as occiput posterior
Consider rotation to occiput anterior
and delivery
Android features
Cesarean deliveryYes
Yes
No
Fig. 4. Suggested approach to arrest ofdescent in the second stage with per-sistent occiput posterior.
Barth. Persistent Occiput Posterior. ObstetGynecol 2015.
702 Barth Persistent Occiput Posterior OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

associated with significant molding, I prefer Simpsonforceps because of the shallower and longer cephaliccurve. Elliot-style forceps with their more roundedcephalic curve are not recommended in this settingbecause they tend to apply pressure at the heel and toeof the blades. I generally use a Bill’s axis of traction barto help identify the correct line of traction, which maybe difficult to find with what is often a higher stationthan anticipated and the need to continue downwardtraction until the brow clears the symphysis pubisbefore flexion should begin. Finally, because of the highrate of sphincter injury with the combination of OP anda forceps delivery, in this setting only, I perform a me-diolateral episiotomy near completion of the deliveryand remove the forceps before complete expulsion to
protect the external anal sphincter. Although uncom-mon in the United States, recent cohort studies fromThe Netherlands demonstrate profound reductions inrectal sphincter injury with mediolateral episiotomy inthe setting of forceps-assisted vaginal delivery.71,72 Fora review of the performance and repair of mediolateralepisiotomy, readers are referred to the illustrated man-ual published by the American College of Obstetriciansand Gynecologists.73
Should Rotation to Occiput Anterior andOperative Vaginal Delivery Be Performed?From a purely pragmatic perspective, if delivery isindicated for a category 3 fetal heart rate tracing in thesetting of persistent OP, the decision is usually
Fig. 5. Physical examination of the pelvis to aid decision-making with arrest of descent in the second stage with persistentocciput posterior. Step 1: Leopold’s third (A) and fourth (B) maneuvers to determine whether the biparietal diameter can bepalpated abdominally. Step 2: Examination of the retropubic angle (C) and pubic arch (D) to assess capacity of the anteriorsegment of the pelvis from inlet to outlet, respectively. Step 3: The relative capacity of the posterior segment is aided bypalpating the length of the sacrospinous ligament (E). A short ligament (F) suggests a crowded posterior segment withprominent spines and a forward sacrum and coccyx. This finding raises the possibility of a dangerous outlet obstruction andis an indication for cesarean delivery in the setting of an arrest of descent with persistent occiput posterior.
Barth. Persistent Occiput Posterior. Obstet Gynecol 2015.
Fig. 6. Ultrasonogram showingdiscordant positions of the fetalspine. A. The fetal spine to thematernal right. B. The fetal orbitsalso directed anterior to thematernal right, implying a leftocciput posterior position.
Barth. Persistent Occiput Posterior.Obstet Gynecol 2015.
VOL. 125, NO. 3, MARCH 2015 Barth Persistent Occiput Posterior 703
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

whether to proceed with emergent cesarean deliveryor an operative vaginal delivery, either with forceps orvacuum, without rotation. One of the faculty physi-cians who taught me how to perform Kiellandrotations (Gary D. V. Hankins) has suggested thatbecause a successful rotation cannot be guaranteedand because a cesarean delivery can usually beperformed just as quickly, the latter is generallypreferred.74 If operative vaginal delivery is consideredin this setting, I would choose forceps over a vacuum,again because they are less likely to fail.75
In the setting of an arrest of descent withpersistent OP with a more reassuring fetal heart ratetracing (category 1 or 2), if my clinical evaluation ofthe pelvis suggests an ample anterior segment likewith a gynecoid pelvis, and assuming that the otherrequirements of operative vaginal delivery are met,my usual recommendation is for a trial of rotation,with or without forceps, followed immediately byforceps-assisted vaginal delivery. Although it is lesslikely to be successful in the setting of arrest ofdescent, I usually begin with an attempt at manualor digital rotation (usually in the labor room) aspreviously described, because there are no reports offetal injuries associated with such attempts. If thisrotation is successful, asking the patient to push fora few contractions to determine if spontaneousdelivery is imminent is an option, but in the settingof an already prolonged second stage, I usuallyproceed with traction forceps (Simpsons) to completethe delivery.
If the manual or digital rotation is unsuccessful,the remaining options include cesarean delivery,forceps or vacuum delivery without rotation, rota-tional vacuum, and finally, rotational forceps followedby nonrotational forceps. My own preference is tocounsel the patient about the relative risks andbenefits of a trial of rotational forceps compared witha cesarean delivery or nonrotational forceps for arrestof descent with persistent OP in the second stage, inthat order. Although there are advocates of rotationalor nonrotational vacuum for persistent OP, I have lessconfidence in these procedures once the fetal head ismolded and impacted deep in the pelvis in the OPposition. The failure rate of nonrotational vacuumfrom OP is high29 and the only correction that can beimparted with rotational vacuum is to improve flexionof the fetal head and hope that autorotation occurswith traction and descent. Torque on a vacuumextractor to effect rotation is contraindicated as a resultof the risk of scalp lacerations and more serious inju-ries. In their guidelines for operative vaginal delivery,at least one professional organization lists the need for
rotation of more than 45° as a relative contraindica-tion to vacuum delivery.67
Although there are a few randomized clinicaltrials comparing forceps with vacuum for operativevaginal delivery, there are no such trials comparingrotational forceps for persistent OP with the alter-natives and such trials are unlikely to be forthcoming.Furthermore, almost all cohort studies comparingthese options are inevitably confounded by indication.Nonetheless, there are some common themes regard-ing one approach compared with another.
Rotational Forceps Deliveries
The relative risks, benefits, and safety of rotationalforceps deliveries have been debated for decades.Those suggesting that such procedures should beabandoned usually cite one of three reasons: 1) anunacceptably high rate of serious fetal morbidity suchas skull fracture, tentorial tears, intracranial hemor-rhage, or spinal cord injury; 2) a growing lack ofexperienced health care providers willing to performand teach the procedure; and finally 3) an insufficientvolume to maintain competence.
Concern for higher rates of fetal injury stems fromolder case series and retrospective cohort studies.76–82
Newer cohort studies demonstrate more favorable fetaloutcomes, fewer maternal third- and fourth-degree lac-erations, and avoidance of the complications associatedwith cesarean delivery in the second stage.74,75,83–89
Burke and colleagues86 prospectively collected dataon all attempted Kielland forceps deliveries from1997 to 2011 at Galway University Hospital in Ireland.The authors described 144 attempted Kielland rota-tional forceps operations, 129 (90%) of which weresuccessful. The authors reported no cases of neonataltrauma among the 129 successful procedures and onlyone third- or fourth-degree tear. Bahl and colleagues75
report a success rate higher than 90% (355/381) andfew instances of neonatal morbidity among 381 mid-cavity rotational operative vaginal deliveries largelyperformed by residents under the supervision of thefaculty at two university hospitals in the United King-dom. This group demonstrated similar maternal andfetal outcomes among three planned approaches: man-ual rotation followed by nonrotational forceps, rota-tional vacuum, and Kielland rotations followed byforceps. However, the failure rate of the primarymethod requiring a second instrument was much high-er with planned vacuum rotation (36.9%) when com-pared with manual (1%) or Kielland (0%) rotations.Bradley and colleagues87 compared the maternal andfetal outcomes of 91 rotational operative vaginal deliv-eries (31 forceps rotations, 60 manual rotations
704 Barth Persistent Occiput Posterior OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

followed by forceps) with 57 nonrotational forceps withdelivery in the OP position. Similar to other studies,maternal and newborn outcomes were similar, butdelivering with forceps in the OP position without rota-tion was associated with a significantly increased risk ofthird- or fourth-degree laceration (43% compared with24%, adjusted OR 3.67, 95% CI 1.42–9.47). In a largecohort study, Stock and colleagues88 described thematernal and newborn outcomes associated with873 successful Kielland rotations between 1995 and2008 in a single institution where such proceduresare still practiced and taught. Neonatal complicationswere rare, including admission to the neonatal inten-sive care unit (4.7%), Apgar score less than 7 at 5 mi-nutes (3.8%), cephalohematoma (1.4%), transient nervepalsy (1.5%), permanent nerve palsy (0%), and sub-dural hematoma (0.1%). In this study, the rate of hem-orrhage greater than 1 L was three times higher withcesarean delivery than with a successful Kielland rota-tional delivery. Finally, Tempest and colleagues89 com-pared the maternal and newborn outcomes of 1,038Kielland rotational forceps with 107 vacuum-assisteddeliveries and 146 second-stage cesarean deliveries.Improving on prior cohort studies by relying on anintention-to-treat analysis and adjusting for indicationfor delivery and experience of the operator, these au-thors noted no differences in the rates of maternal hem-orrhage or neonatal admission to a special care unit.Importantly, not a single case of spinal cord injury wasreported in these five contemporary series described(0/2,966 [0%]; 95% CI 0.0–0.16%). Although I mentionthis complication when counseling patients, I stress thatit is extraordinarily rare and is probably associatedonly with ill-advised persistence through a difficult pro-cedure, which I will not do. In light of such favorableneonatal outcomes and with an awareness that cesareandelivery late in the second stage with arrest of descentin the OP position can be a morbid procedure for themother,32–37 it is this author’s opinion that rotationalforceps should remain an option in contemporaryobstetrics.
If rotational forceps operations are to continue,the procedure must be taught during residency andfellowship. In programs that have abandoned rota-tional forceps and no longer have faculty memberswilling to perform or teach rotations, this is aninsurmountable challenge. In teaching programs thatdo have faculty trained in rotational forceps, clini-cians not comfortable with the procedure must bewilling to consult in the setting of an arrest of descentin the OP position. Similarly, those who are con-sulted must make themselves available if at allpossible, a task that may require creative plans for
coverage when assigned to duties away from thelabor floor. Illustrating the importance of suchsupervision, among the 36 deaths resulting fromintracranial injury reported by O’Mahoney82 in theConfidential Enquiries into Stillbirths and Deaths inInfancy, only two were performed or supervised byattending physicians.
That there are too few procedures to trainresidents and fellows, and too few to maintaincompetence, is an unfortunate self-perpetuatingdynamic. At present, many graduating residents arenot comfortable with forceps operations of any type,much less Kielland rotations.90,91 With the rate ofoperative delivery in many hospitals now less than5%, I would argue that such training should be selec-tive and that there is no point in diluting the experi-ence of some by training those who will never practicerotational forceps. Next, although there is no substi-tute for the experience gained by the feel and real-time feedback in performing rotational forceps undersupervision, a rational argument can be made for sim-ulation training with realistic pelvic models beforereal-time application in hopes of gaining more whenthe rare occasion does arise.
Conduct of Kielland Rotational Delivery
With a gynecoid pelvis and no contraindication tovaginal delivery, if the patient is willing to attemptsuch a delivery, I move the patient to the operatingroom. In my hands, such deliveries are always a trialof rotational forceps. After informed consent, Igenerally write a preoperative note explaining myrationale and the critical components of the decision-making and recommendation as noted in Figure 4.With adequate anesthesia, I position the patient inthe dorsal lithotomy position with the buttocksslightly overhanging the end of the bed, and I takecare to make sure the hips are flexed only slightlysuch that the knees are approximately 30° off of thevertical and toward me. If I have not done so pre-viously, I rely on ultrasonography to ensure that theocciput and spine are concurrent and that my at-tempted rotation is in the correct direction. Afteremptying the bladder and lubricating the Kiellandforceps, I place them using a cephalic applicationwith the indicator buttons directed anteriorly towardthe face. I do this because my practice is to rotatewith the Kiellands and, if successful, replace themwith Simpson-type forceps for traction and delivery.After checking the position, I correct for any asyn-clitism by comparing the correspondent length of thehandles and using the sliding lock to assure that theknobs are closely related. Next, I hold the handles in
VOL. 125, NO. 3, MARCH 2015 Barth Persistent Occiput Posterior 705
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

my right hand and use my left hand fingers to followthe rotation. Then, when the patient is not contract-ing, I slightly elevate and flex the fetal head, thenapply gentle rotational force in the direction movingthe fetal spine in the short arc from posterior to ante-rior (left OP to left OA, right OP to right OA). If Imeet with resistance, the only two maneuvers are toelevate the head to a more favorable plane or to flexthe head to achieve a more favorable diameter. Flex-ing the head may require a slight adjustment of theforceps to a more occipitally oriented position. Addi-tional rotational force is to be avoided. If the rotationis successful, often heralded by a sucking sound asthe fetal head disengages and easily rotates, I gentlyreseat the head with the Kiellands. At this point Iremove one blade and replace it with the corre-sponding side of a pair of Simpson forceps to holdthe position. After removing the other Kielland, Iplace the remaining Simpson blade and completethe delivery, this time without an episiotomy.
Cesarean Delivery for Arrest of Descent WithOcciput Posterior
As described earlier, cesarean delivery in the secondstage is a more morbid procedure for the motherthan cesarean delivery before labor or during theactive phase and this is especially so with OP. Thefetal vertex is often deeply impacted and difficult toextract. Several authors have proposed techniques tofacilitate delivery and minimize inadvertent hyster-otomy extensions in this situation by elevating thefetal vertex with a vaginal hand (pushing frombelow), by reverse breech delivery (pulling fromabove as a breech), or by using various devices orspecialized forceps to assist with disengagement ofthe fetal head. A recent meta-analysis of six pro-spective and four retrospective studies comparing thepush with the pull method found that pushing frombelow was associated with a significant increase inthe risk of hysterotomy extension (OR 7.8, 95% CI5.01–12.25), more infectious morbidity for themother, and more blood transfusions but fewer fetalbirth injuries.92 My own approach is to try to deliverthe head in a standard fashion with my abdominalhand while trying not to back my wrist as a fulcruminto the lower uterine segment toward the cervix. Ifthat is unsuccessful, and until further research settlesthe issue comparing outcomes between the push andpull methods for a deeply impacted fetal head, I usu-ally ask for assistance with a hand from below and,then, if still unsuccessful, proceed with delivery ofthe feet and complete the delivery as a breech extrac-tion from above.
CONCLUSIONS
Persistent OP need not be the bête noir of intrapartumobstetrics some believe it to be. When encountered inearly labor, OP positions usually resolve spontaneouslyand a conservative approach is best. On the otherhand, if rotation has not occurred after some periodof observation in the second stage, more liberal useof prophylactic manual rotation may decrease maternalmorbidity by preventing both cesarean deliveries andvaginal deliveries in the OP position. Once an arrest ofdescent has occurred in the second stage, an apprecia-tion that not all OPs are the same is paramount indetermining the safest route of delivery. Some shouldbe delivered abdominally; among these are macroso-mia, the deceptively high station common in OP, orandroid pelvic features with the potential for dangerousoutlet obstruction. Some should be delivered from theOP position without rotation, like with anthropoid pel-vic features and ample room in the posterior pelvis.Even today, some should be rotated, whether manuallyor with forceps, and delivered from an anterior posi-tion. Kielland forceps rotations still have a place inmodern obstetrics. The challenges posed by a decreas-ing number of clinicians willing to perform or teach theprocedure are substantial. Those of us trained in theprocedure must be willing to perform them and teachthem acknowledging that opportunities to do so maycome at the most inopportune times. Simulation train-ing offers promise and I hope that models and techni-ques will get closer to the invaluable feedback gainedwhen real rotations are and are not proceeding well.Lastly, I am of the firm opinion that we cannot con-tinue to train all residents to be proficient in all proce-dures. Training in complicated operative vaginaldelivery should be limited to those who will be per-forming such procedures after residency.
REFERENCES1. Yeomans ER. Operative vaginal delivery. Obstet Gynecol
2010;115:645–53.
2. Gardberg M, Tuppurainen M. Persistent occiput posterior posi-tion—a clinical problem. Acta Obstet Gynecol Scand 1994;73:45–7.
3. Gardberg M, Laakonen E, Sälevaara M. Intrapartum sonogra-phy and persistent occiput posterior position: a study of 408deliveries. Obstet Gynecol 1998;91:746–9.
4. Ponkey SE, Cohen AP, Heffner LJ, Lieberman E. Persistentfetal occiput posterior position: obstetric outcomes. Obstet Gy-necol 2003;101:915–20.
5. Akmal S, Tsoi E, Howard R, Osei E, Nicholaides KH. Investi-gation of occiput posterior delivery by ultrasonography. Ultra-sound Obstet Gynecol 2004;24:425–8.
6. Lieberman E, Davidson K, Lee-Paritz A, Shearer E. Changes infetal position during labor and their association with epiduralanalgesia. Obstet Gynecol 2005;105:974–82.
706 Barth Persistent Occiput Posterior OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

7. Randal JH. The persistent occiput posterior. J Iowa State MedSoc 1952;42:148–51.
8. Kutcipal RA. The persistent occiput posterior position: a reviewof 498 cases. Obstet Gynecol 1959;14:296–304.
9. Fitzpatrick M, McQuillan K, O’Herlihy C. Influence of persis-tent occiput posterior position on delivery outcome. ObstetGynecol 2001;98:1027–31.
10. Peregrine E, O’Brien P, Jauniaux E. Impact on delivery out-come of ultrasonographic fetal head position prior to inductionof labor. Obstet Gynecol 2007;109:618–25.
11. Peregrine E, O’Brien P, Jauniaux E. Impact on delivery out-come of ultrasonographic fetal head position prior to inductionof labor. Obstet Gynecol 1932;23:360–6.
12. Caldwell WE, Moloy HC. Anatomical variations in the femalepelvis and the effect in labour with a suggested classification.Am J Obstet Gynecol 1933;26:479–505.
13. Caldwell WE, Moloy HC, D’Esopo DA. A roentgenologicstudy of the mechanism of engagement of the fetal head. AmJ Obstet Gynecol 1934;28:824–41.
14. D’Esopo DA. The occipitoposterior position: its mechanismand treatment. Am J Obstet Gynecol 1941;42:937.
15. Danforth DN, Ellis AH. Midforceps delivery—a vanishing art?Am J Obstet Gynecol 1963;86:29–37.
16. Holmberg NG, Liljeqvist B, Magnusson S, Segerbrand E. Theinfluence of the bony pelvis in persistent occiput posterior posi-tion. Acta Obstet Gynecol Scand Suppl 1977;66:49–54.
17. Floberg J, Belfrage P, Ohlsén H. Influence of the pelvic outletcapacity on fetal head presentation at delivery. Acta ObstetGynecol Scand 1987;66:127–30.
18. Gardberg M, Stenwall O, Laakonen E. Recurrent persistentoccipito-posterior position in subsequent deliveries. BJOG2004;111:170–1.
19. Handa VL, Lockhart ME, Fielding JR, Bradley CS, Brubaker L,Cundiff GW, et al. Racial differences in pelvic anatomy by mag-netic resonance imaging. Obstet Gynecol 2008;111:914–20.
20. Benavides L, Wu JM, Hundley AF, Ivester TS, Visco AG. Theimpact of occiput posterior fetal head position on the risk ofanal sphincter injury in forceps-assisted vaginal deliveries. Am JObstet Gynecol 2005;192:1702–6.
21. Cheng YW, Shaffer BL, Caughey AB. Associated factors andoutcomes of persistent occiput posterior position: a retrospectivecohort study from 1976 to 2001. J Matern Fetal Neonatal Med2006;19:563–8.
22. Sizer AR, Nirmal DM. Occipitoposterior position: associatedfactors and obstetric outcome in nulliparas. Obstet Gynecol2000;96:749–52.
23. Anim-Somuah M, Smyth RMD, Jones L. Epidural versus non-epidural or no analgesia in labour. The Cochrane Database ofSystematic Reviews 2011, Issue 12. Art. No.: CD000331. DOI:10.1002/14651858.CD000331.pub3.
24. Senécal J, Xiong X, Fraser WD; Pushing Early Or Pushing Latewith Epidural Study Group. Effect of fetal position on secondstage duration and labor outcome. Obstet Gynecol 2005;105:763–72.
25. Peregrine E, O’Brien P, Omar R, Janiaux E. Clinical and ultra-sound parameters to predict the risk of cesarean delivery afterinduction of labor. Obstet Gynecol 2006;107:227–33.
26. Fraser WD, Cayer M, Soeder BM, Turcot L, Marcoux S; PEO-PLE (Pushing Early or Pushing Late with Epidural) StudyGroup. Risk factors for difficult delivery in nulliparas with epi-dural analgesia in second stage of labor. Obstet Gynecol 2002;99:409–18.
27. Hawkins JL, Hess KR, Kubicek MA, Joyce TH III,Morrow DH. A reevaluation of the association betweeninstrument delivery and epidural analgesia. Reg Anesth1995;20:50–6.
28. Mazouni C, Porcu G, Bretelle F, Loundou A, Heckenroth H,Gamerre M. Risk factors for forceps delivery in nulliparouspatients. Acta Obstet Gynaecol 2006;85:298–301.
29. Damron DP, Capeless EL. Operative vaginal delivery: a com-parison of forceps and vacuum for success rate and risk of rectalsphincter injury. Am J Obstet Gynecol 2004;191:907–10.
30. Pearl ML, Roberts JM, Laros RK, Hurd WH. Vaginal deliveryfrom the persistent occiput posterior position: influence on mater-nal and neonatal morbidity. J Reprod Med 1993;38:955–61.
31. Fitzgerald MP, Weber AM, Howden N, Cundiff GW,Brown MB; Pelvic Floor Disorders Network. Risk factors foranal sphincter tear during vaginal delivery. Obstet Gynecol2007;109:29–34.
32. Murphy DJ, Liebling RE, Verity L, Swingler R, Patel R. Earlymaternal and neonatal morbidity associated with operativedelivery in the second stage of labour: a cohort study. Lancet2001;358:1203–7.
33. Allen VM, O’Connell CM, Baskett TF. Maternal and perinatalmorbidity of caesarean delivery at full cervical dilatation com-pared with caesarean delivery in the first stage of labour. BJOG2005;112:986–90.
34. de la Torre L, González-Quintero VH, Mayor-Lynn K,Smarkusky L, Hoffman C, Saab A, et al. Significance of acci-dental extensions in the lower uterine segment during cesareandelivery. Am J Obstet Gynecol 2006;194:e4–6.
35. Alexander JM, Leveno KJ, Rouse DJ, Landon MB, Gilbert S,Spong CY, et al. Comparison of maternal and infant outcomesfrom primary cesarean delivery during the second comparedwith the first stage of labor. Obstet Gynecol 2007;109:917–21.
36. Sung JF, Daniels KI, Brodzinsky L, El-Sayed YY, Caughey AB,Lyell DJ. Cesarean delivery outcomes after a prolonged secondstage of labor. Am J Obstet Gynecol 2007;197:306.e1–5.
37. Pergialiotis V, Vlachos DG, Rodolakis A, Haidopoulos D,Thomakos N, Vlachos GD. First versus second stage C/S mater-nal and neonatal morbidity: a systematic review and meta-anal-ysis. Eur J Obstet Gynecol Repro Biol 2014;175:15–24.
38. Ingamarssen E, Ingamarsen I, Solum T, Westgren M. Influenceof occiput posterior position on the fetal heart rate pattern.Obstet Gynecol 1980;55:301–4.
39. Sokol RJ, Roux JF, McCarthy S. Computer diagnosis of laborprogression. Am J Obstet Gynecol 1975;122:253–60.
40. Sokol RJ. Occipitoposterior position and FHR patterns. ObstetGynecol 1981;57:266–7.
41. Cheng YW, Shaffer BL, Caughey AB. The association betweenpersistent occiput posterior position and neonatal outcomes.Obstet Gynecol 2006;107:837–44.
42. Sherer DM, Miodovnik M, Bradley KS, Langer O. Intrapartumfetal head position I: comparison between transvaginal digitalexamination and transabdominal ultrasound assessment duringthe active stage of labor. Ultrasound Obstet Gynecol 2002;19:258–63.
43. Kawabata I, Nagase A, Oya A, Hayashi M, Miyake H, Nakai A,et al. Factors influencing the accuracy of digital examination fordetermining fetal head position during the first stage of labor.J Nippon Med Sch 2010;77:290–5.
44. Sherer DM, Miodovnik M, Bradley KS, Langer O. Intrapartumfetal head position II: comparison between transvaginal digitalexamination and transabdominal ultrasound assessment during
VOL. 125, NO. 3, MARCH 2015 Barth Persistent Occiput Posterior 707
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

the second stage of labor. Ultrasound Obstet Gynecol 2002;19:264–8.
45. Akmal S, Kametas N, Tsoi E, Heargraves C, Nicolaides KH.Comparison of transvaginal digital examination with intrapar-tum sonography to determine fetal head position before instru-mental delivery. Ultrasound Obstet Gynecol 2003;21:437–40.
46. Chou MR, Kreiser D, Taslimi MM, Druzin ML, El-Sayed YY.Vaginal ultrasound examination of fetal occiput position duringthe second stage of labor. Am J Obstet Gynecol 2004;191:521–4.
47. Dupuis O, Ruimark S, Corinne D, Simone T, André D, René-Charles R. Fetal head position during the second stage of labor:comparison of digital vaginal examination and transabdominalultrasonographic examination. Eur J Obstet Gynecol ReprodBiol 2005;123:193–7.
48. Zahalka N, Sadan O, Malinger G, Liberati M, Boaz M,Glezerman M, et al. Comparison of transvaginal sonographywith digital examination and transabdominal sonography forthe determination of fetal head position in the second stage oflabor. Am J Obstet Gynecol 2005;193:381–6.
49. Rayburn WF, Siemers KH, Legino LJ, Nabity MR,Anderson JC, Patil KD. Dystocia in late labor: determining fetalposition by clinical and ultrasonic techniques. Am J Perinatol1989;6:316–9.
50. Akmal S, Tsoi E, Nicolaides KH. Intrapartum sonography todetermine fetal occipital position; interobserver agreement.Ultrasound Obstet Gynaecol 2004;24:421–4.
51. Peregrine E, O’Brien P, Omar R, Jauniaux E. Clinical andultrasound parameters to predict the risk of cesarean deliveryafter induction of labor. Obstet Gynecol 2006:107:227–33.
52. Kariminia A, Chamberlain MF, Keogh J, Shea A. Randomizedcontrolled trial of effect of hands and knees posturing on inci-dence of occiput posterior position at birth. BMJ 2004;328:490.
53. Hunter S, Hofmeyr GJ, Kulier R. Hands and knees posture inlate pregnancy or labour for fetal malposition (lateral or poste-rior). The Cochrane Database of Systematic Reviews 2007,Issue 4. Art. No.: CD001063. DOI: 10.1002/14651858.CD001063.pub3.
54. Stremler R, Hodnett E, Petryshen P, Stevens B, Weston J,Willan AR. Randomized controlled trial of hands-and-kneespositioning for occipitoposterior position in labor. Birth 2005;32:243–51.
55. Desbriere R, Blanc J, Le Dû R, Renner JP, Carcopino X,Loundou A, et al. Is maternal posturing during labor efficientin preventing persistent occiput posterior position? A random-ized controlled trial. Am J Obstet Gynecol 2013;208:60.e1–8.
56. Le Ray C, Serres P, Schmitz T, Cabrol D, Goffinett F. Manualrotation in occiput posterior or transverse positions. Obstet Gy-necol 2007;110:873–9.
57. Haddad B, Abirached F, Calvez G, Cabrol D. Manual rotationof vertex presentations in posterior occipital-iliac or transverseposition: technique and value [in French]. J Gynecol ObstetBiol Reprod (Paris) 1995;24:181–8.
58. Gustafson GW. Management of occiput posterior. J Am MedAssoc 1949;139:280–5.
59. Haynes DM. Occiput posterior position: six year’s experienceat Parkland Memorial Hospital. J Am Med Assoc 1954;156:494–6.
60. McKelvey JI, Diefenbach EJ. The obstetric significance of theposterior occiput position. Postgrad Med 1951;9:211–4.
61. Shaffer BL, Cheng YW, Vargas JE, Caughey AB. Manual rota-tion to reduce cesarean delivery in occiput posterior or trans-verse position. J Matern Fetal Neonatal Med 2011;24:65–72.
62. Shaffer BL, Cheng YW, Vargas JE, Laros RK Jr, Caughey AB.Manual rotation of the fetal occiput: predictors of success anddelivery. Am J Obstet Gynecol 2006;194:e7–9.
63. Le Ray C, Deneau-Tharaux C, Khireddine I, Dreyfus M,Vardon D, Goffinett F. Manual rotation to decrease operativedelivery in posterior or transverse positions. Obstet Gynecol2013;122:634–40.
64. Reichman O, Gdansky E, Latinsky B, Labi S, Sameuloff A.Digital rotation from occipito-posterior to occipito-anterior de-creases the need for cesarean section. Eur J Obstet GynecolReprod Biol 2008;136:25–8.
65. Walkowiak RG. Manual rotation of the transverse posteriorocciput. Obset Gynecol 1971;37:464–7.
66. Lowenstein A, Zevin R. Digital rotation of the vertex. ObstetGynecol 1971;37:790–1.
67. Cargill YM, MacKinnon CJ, Arsenault MY, Bartellas E,Daniels S, Gleason T, et al. Guidelines for operative vaginal birth[in English, French]. J Obstet Gynaecol Can 2004;26:747–61.
68. Dennen EH, Dennen PC. Posterior presentations of the occi-put. In: Hale RW, editor. Dennen’s forceps deliveries. 4th ed.Washington, DC: American College of Obstetricians and Gy-necologists; 2001. p. 103–15.
69. Operative vaginal delivery. ACOG Technical Bulletin No. 196.Int J Gynaecol Obstet 1994;47:179–85.
70. Fetal macrosomia. Practice Bulletin No. 22. American Collegeof Obstetricians and Gynecologists. 2000;96:1–11.
71. de Leeuw JW, de Wit C, Kuijken JP, Bruinse HW. Mediolateralepisiotomy reduces the risk for anal sphincter injury duringoperative vaginal delivery. BJOG 2008;115:104–8.
72. de Vogel J, van der Leeuw-van Beek A, Gietelink D,Vujkovic M, de Leeuw JW, van Bavel J, et al. The effect ofa mediolateral episiotomy during operative vaginal deliveryon the risk of developing obstetrical anal sphincter injuries.Am J Obstet Gynecol 2012;206:404.e1–5.
73. Hale RW, Ling FW. Episiotomy: procedure and repair techni-ques. Washington, DC: American College of Obstetricians andGynecologists; 2007.
74. Hankins GD, Leicht T, Van Hook J, Uçkan E. The role offorceps rotation in maternal and fetal injury. Am J Obstet Gy-necol 1999;180:231–4.
75. Bahl R, Van de Venne M, Macleod M, Strachan B, Murphy DJ.Maternal and neonatal morbidity in relation to the instrumentused for mid-cavity rotational operative vaginal delivery: a pro-spective cohort study. BJOG 2013;120:1526–32.
76. Dyack C, Rotational forceps in midforceps delivery. ObstetGynecol 1980;56:123–6.
77. O’Driscoll K, Meager D, MacDonald D, Geohegan F. Trau-matic intracranial hemorrhage in first born infants and deliverywith obstetric forceps. Br J Obstet Gynecol 1981;88:577–81.
78. Singh K, Viegas O, Heng SH, Ratnam SS. An eight year expe-rience with the Kielland forceps in Singapore. Singapore Med J1986;27:225–9.
79. Chiswick ML, James DK. Keilland’s forceps: association withneonatal morbidity and mortality. Br Med J 1979;1:7–9.
80. Hankins GD, Rowe TF. Operative vaginal delivery—year 2000.Am J Obstet Gynecol 1996;175:275–82.
81. Menticoglou SM, Perlman M, Manning FA. High cervical spi-nal cord injury in neonates delivered with forceps: report of 15cases. Obstet Gynecol 1995;86:589–94.
82. O’Mahony F, Settatree R, Platt C, Johanson R. Review of sin-gleton fetal and neonatal deaths associated with cranial trauma
708 Barth Persistent Occiput Posterior OBSTETRICS & GYNECOLOGY
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.

and cephalic delivery during a national intrapartum-relatedconfidential enquiry. BJOG 2005;112:619–26.
83. Krivak TC, Drewes P, Horowitz GM. Kielland vs non-rotational forceps for the second stage of labor. J ReprodMed 1999;44:511–7.
84. Feldman DM, Borgida AF, Sauer F, Rodis JF. Rotational versusnon-rotational forceps: maternal and neonatal outcomes. Am JObstet Gynecol 1999;181:1185–7.
85. Hirsch E, Haney EI, Gordon TE, Silver RK. Reducing high-order perineal laceration during operative vaginal delivery. AmJ Obstet Gynecol 2008;198:668.e1–5.
86. Burke N, Field K, Mujahid F, Morrison JJ. Use and safety ofKielland’s forceps in current obstetric practice. Obstet Gynecol2012;120:766–70.
87. Bradley MS, Kaminski RJ, Streitman DC, Dunn SL, Krans EE.Effect of rotations on perineal lacerations in forceps-assistedvaginal deliveries. Obstet Gynecol 2013;122:132–7.
88. Stock SJ, Josephs K, Farquharson S, Love C, Cooper SE, Kissack C,et al. Maternal and neonatal outcomes of successful Kielland’s rota-tional forceps delivery. Obstet Gynecol 2013;121:1032–9.
89. Tempest N, Hart A, Walkinshaw S, Hapangama D. A re-evaluation of the role of rotational forceps: retrospective com-parison of maternal and perinatal outcomes following differentmethods of birth for malposition in the second stage of labour.BJOG 2013;120:1277–84.
90. Powell J, Gilo N, Foote M, Gil K, Lavin JP. Vacuum and for-ceps training in residency: experience and self-reported compe-tency. J Perinatol 2007;27:343–6.
91. Chinnock M, Robson S. An anonymous survey of registrartraining in the use of Kielland’s forceps in Australia. Aust NZ J Obstet Gynecol 2009;49:515–6.
92. Berhan Y, Berhan A. A meta-analysis of reverse breech extrac-tion to deliver a deeply impacted head during cesarean deliv-ery. Int J Gynecol Obstet 2014;124:99–105.
Earn CME Credits for Your Contribution as a Reviewer to Obstetrics & Gynecology
In recognition of their time, effort, and expertise, reviewers of manuscripts for Obstetrics & Gynecology are eligible to receive continuing medical education credits.
ACCME AccreditationThe American College of Obstetricians and Gynecologists is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians.
AMA PRA Category 1 Credit(s)™The American College of Obstetricians and Gynecologists designates this manuscript review activity for a maximum of 3 AMA PRA Category 1 Credits.™ Physicians should claim only the credit commensurate with the extent of their participation in the activity.
College Cognate Credit(s)The American College of Obstetricians and Gynecologists designates this manuscript review activity for a maximum of 3 Category 1 College Cognate Credits. The College has a reciprocity agreement with the AMA that allows AMA PRA Category 1 Credits™ to be equivalent to College Cognate Credits.
College Fellows will be awarded credit for a maximum of five reviews yearly. Those who are not College Fellows will receive e-mail documentation approximately 1 month after completion of the review, which can be submittedto an accrediting body for credits.
rev 11/2014
VOL. 125, NO. 3, MARCH 2015 Barth Persistent Occiput Posterior 709
Copyright ª by The American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.