Embed Size (px)
Citation preview

785
EP IMAGE
Permanent Left Atrial Pacing via the Vein of MarshallSUMIT VERMA, M.D.
From the Regional Heart and Vascular Institute, Pensacola, Florida, USA
The patient is a 65-year-old female who was referred forpermanent pacemaker implantation for treatment of sick si-nus syndrome and associated paroxysmal atrial fibrillation.She was found to have severe tricuspid regurgitation andmoderate pulmonary hypertension. ECG revealed sinus ar-rest with a junctional escape rhythm. Right atrial lead place-ment was unsuccessful, due to inability to capture the atriumwith high output pacing (6 V output at a pulse width of1.5 ms) from multiple sites. After coronary sinus cannula-
J Cardiovasc Electrophysiol, Vol. 18, p. 785, July 2007.
Address for correspondence: Sumit Verma, 5151 N. 9th Avenue, Pensacola,FL 32504. Fax: (850) 857-1746; E-mail: [email protected]
doi: 10.1111/j.1540-8167.2007.00797.x
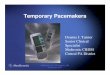
Figure 1. A: Left anterior oblique (LAO)view of coronary sinus venogram B: LAOview. Unipolar lead positioned in the vein ofMarshall (VOM) in a distal location. C: Rightanterior oblique (RAO) view of bipolar leadin VOM. D: LAO view of final lead position.
tion, a unipolar pacing lead (Medtronic Attain� UnipolarOTW Lead- Model 4193- 4 Fr) was initially positioned inthe vein of Marshall (Fig. 1B), but due to poor fixation andnoncapture, this was changed to a bipolar lead (Fig. 1C,D;Medtronic Attain� Bipolar OTW Lead, Model 4194, 6 Fr).A capture threshold of 2.5 V at 0.5 ms pulse width was ob-tained, as confirmed by acceleration of ventricular rate withatrial pacing. After 1 month, the patient had developed fixedatrial fibrillation. Evaluation of the pacing system revealedthat the atrial lead was in a stable position by fluoroscopy,with normal impedance and sensing parameters (sensing offibrillation waves between 0.75 mV–1.5 mV). Due to comor-bidities, a rhythm control strategy for atrial fibrillation wasnot pursued any further. This case illustrates the possibilityof transvenous left atrial pacing via the vein of Marshall inselected patients with suitable indications and anatomy.








![Typical atrioventricular nodal reentrant and orthodromic ......tachycardia [3,14,16-18]. Atrial pacing with extra stimuli at progressively shorter coupling intervals is used for the](https://img.pdfslide.us/doc/110x75/5e522ac39f51e873c016f911/typical-atrioventricular-nodal-reentrant-and-orthodromic-tachycardia-31416-18.jpg)



















