Embed Size (px)
Citation preview

Peritonsillar Abscess in Emergency Medicine
BackgroundPeritonsillar abscesses (PTAs) are common infections of the head and neck region and comprise approximately 30% of soft tissue head and neck abscesses.[1] Physicians must be aware of the typical clinical presentation and diagnostic strategies in order to quickly diagnose and appropriately treat these patients to prevent complications and further propagation of the infectious process.
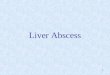
A peritonsillar abscess is shown in the image below.
Right peritonsillar abscess. The soft palate, which is erythematous and edematous, is displaced anteriorly. The patient has a "hot potato–sounding" voice.
PathophysiologyThe 2 palatine tonsils are on the lateral walls of the oropharynx in the depression between the anterior and posterior tonsillar pillars. Each pillar is composed primarily of the glossopalatine and the pharyngopalatine muscles.
During embryonic development, the tonsils arise from the second pharyngeal pouch as buds of endodermal cells.[2] The tonsils then grow irregularly and reach their ultimate size and shape at approximately age 6-7 years.
Each tonsil is surrounded by a capsule, a specialized portion of the intrapharyngeal aponeurosis that covers the medial portion of the tonsils and provides a path for blood vessels and nerves.[2] It is within this potential space between the tonsil and capsule that peritonsillar abscesses form.[3] Note that the peritonsillar space is anatomically contiguous with several deeper spaces, and infections can potentially involve the parapharyngeal and retropharyngeal spaces.[4]
Peritonsillar abscesses usually progress from tonsillitis to cellulitis and ultimately to abscess formation. Weber glands are thought to also play a key role in the etiology of the infection. These mucous salivary glands are located superior to the tonsil in the soft palate and clear the tonsillar area of debris. If these glands become inflamed, local cellulitis develops. As the infection progresses, inflammation worsens and results in tissue necrosis and pus formation, most commonly just above the superior pole of the tonsil where the glands are located.[3]
EpidemiologyFrequency
United States

In the United States, the incidence of peritonsillar abscess has been estimated at 30 cases per 100,000 persons per year, accounting for approximately 45,000 cases annually.It has also been estimated to result in at least $150 million a year in health care expenditures.[5] Most infections occur during November to December and April to May, which coincide with the highest incidence rates of streptococcal pharyngitis and exudative tonsillitis.[3]
InternationalA higher rate due to recurrence and antibiotic resistance is reported internationally.
Mortality/Morbidity
Mortality of peritonsillar abscess is unknown.
Morbidity of peritonsillar abscess is due mostly to pain, cost of treatment, lost time from work and school, and complications.
Race
No racial predilection of peritonsillar abscess is noted.
Sex
The male-to-female ratio of peritonsillar abscess is equal.
Age
Peritonsillar abscess can occur in anyone aged 10-60 years according to one source, although peritonsillar abscess is most commonly seen in those aged 20-40 years.[6] The younger children who get peritonsillar abscess are often immunocompromised.
HistorySymptoms of peritonsillar abscess usually begin 3-5 days prior to evaluation.
Fever Malaise Headache Neck pain Throat pain markedly more severe on the affected side and occasionally referred to
the ipsilateral ear Dysphagia Change in voice Otalgia Odynophagia
PhysicalPhysical findings of peritonsillar abscess include the following:
Mild/moderate distress Fever Tachycardia Dehydration Drooling, salivation, trouble handling oral secretions

Trismus resulting from pain from inflammation and spasm of masticator muscles Hot potato/muffled voice Rancid or fetor breath Cervical lymphadenitis in the anterior chain Asymmetric tonsillar hypertrophy Localized fluctuance Inferior and medial displacement of the tonsil Contralateral deviation of the uvula Erythema of the tonsil Exudates on the tonsil
CausesPeritonsillar abscesses are usually polymicrobial. A recent prospective study carried out to elucidate significant pathogens involved in peritonsillar abscesses demonstrated that the most prominent aerobic pathogen was Streptococcus pyogenes. Other aerobic pathogens isolated included Staphylococcus aureus,Neisseria species, and Corynebacterium species. In the same study, the most common anaerobic species found was Fusobacterium necrophorum, an obligate, anaerobic, Gram-negative rod. Other Fusobacterium species andPrevotella species were also isolated. Though the study was carried out in Denmark, studies within the United States have demonstrated similar results.[3, 7, 2, 8]
Differential Diagnoses Dental, Infections
Laboratory Studies No definitive studies are required for the diagnosis of peritonsillar abscess, although
one might consider obtaining CBC count and electrolyte evaluations if the patient had significant comorbidities.
Monospot test/heterophile antibody test can be performed to rule out infectious mononucleosis if the etiology is unclear.
Culture of fluid from needle aspiration may be performed. Blood cultures may be indicated if the clinical presentation is severe. Imaging Studies Lateral soft tissue neck radiographs may help rule out other causes. The
anteroposterior (AP) view of the neck may demonstrate distortion of soft tissue. Intraoral ultrasonography (US) has a sensitivity of 95.2% and specificity of 78.5%.
This method is cost-effective and fast, although it does require a cooperative patient. A recent study carried out at an academic level I emergency department included 43 patients who received intraoral US for suspected peritonsillar abscess. Thirty-five were diagnosed with an abscess on US, and these patients subsequently received needle aspiration using US guidance. There was one false positive, but no patients returned unexpectedly after drainage, and, on reexamination, there was no evidence of persistent or recurrent peritonsillar abscess or cellulitis. This study supports the use of US for both the diagnosis and treatment of peritonsillar abscesses.[9] Prior studies of US use have shown similar successful results.
Head and neck CT scanning with intravenous (IV) contrast is useful if incision and drainage fails, if the patient cannot open his or her mouth, or if the patient is young (< 7 y) and uncooperative. A hypodense fluid collection with rim enhancement may

be seen in the affected tonsil. Foreign bodies, such as fish or chicken bones, may also be found as an inciting factor.
Procedures Three options are available for acute surgical management of peritonsillar abscess:
needle aspiration, incision and drainage, and quinsy tonsillectomy (eg, simultaneous tonsillectomy with open abscess drainage).
A systematic review by Johnson et al attempted to determine the best technique for acute surgical management. Forty-two articles were analyzed. Five level I clinical studies indicated that all 3 techniques were equally effective for initial management.[10]
Needle aspiration
The main advantage of needle aspiration is ease of the procedure, decreased pain for the patient, and cost-effectiveness.[5, 10]
The patient should be sitting upright. Lidocaine with epinephrine should be used to anesthetize the area. A 16- to 18-gauge needle with a 10-mL syringe should be used to aspirate from the
area that is most fluctuant. A needle guard may be used to prevent accidental carotid artery puncture due to the
tip of the needle migrating too far posteriorly. Only 0.5 cm of the needle needs to be exposed. If a needle guard is unavailable, a curved clamp can be used to expose a small portion of the needle before inserting it into the area for aspiration.
Aspirate at the superior pole initially, as this is the most common place for abscess development. Aspiration of the middle one third and then the lower one third should then be attempted if pus is not returned from the superior pole. Also, see Drainage, Peritonsillar Abscess.
Pus is aspirated through a wide-bore needle from the right peritonsillar abscess. An additional incision will be made to drain any other pus pockets.
Abscess incision and drainage [11]
The patient should be sitting upright with a pan available to spit out any blood or pus. A tongue depressor is used to retract the tongue. After local infiltration with lidocaine with epinephrine, a No. 11 blade scalpel is used
to make a small incision 0.5 cm long and no more than 1 cm deep. Be certain that the incision is not extended laterally as the carotid artery lies in that vicinity.
Use a small hemostat to probe the abscess and release the pus. To prevent the risk of aspiration, allow the patient to hold the Yankauer catheter tip
and to suction the pus. Tonsillectomy
No clear evidence indicates that routine elective tonsillectomy is indicated to prevent future peritonsillar abscesses. However, if the patient has had multiple recurrent

episodes of peritonsillar abscessor has other clear indications such as sleep-disordered breathing, elective tonsillectomy should be considered.[5]
Additionally, if general anesthesia is required because of the patient's age or lack of cooperation, tonsillectomy should be considered, as the complication rate is low and although the data do not support this, consideration for the most definitive procedure should be made.[5, 10]
Prehospital CarePrehospital care for peritonsillar abscess includes transport with supplemental oxygen.
Emergency Department CareABCs, paying attention to the patient's airway, should be evaluated. If the patient's airway is compromised, he or she needs immediate endotracheal intubation. If this cannot be completed, a cricothyroidotomy or a tracheotomy may be required. Alternatively, if the resources are available, one study concluded that awake fiberoptic bronchoscopy was the method of choice for intubating patients with significant pharyngeal edema.[5]
These patients are often dehydrated because of their avoidance of food and liquid and may need fluid resuscitation.
Antipyretics should be administered for elevated temperature, and adequate analgesia should be provided for pain.
Acute surgical management should be carried out as discussed above.
Empiric antibiotics should be administered.
Steroids are often used as adjunctive treatment. In the systematic review carried out by Johnson et al, no published studies on the use of steroids in peritonsillar abscess were found, but the authors did identify a randomized controlled trial that demonstrated a benefit for steroids for severe, acute pharyngitis. It is likely that the use of steroids for PTA derived from this management strategy
Patients can be managed in an outpatient setting unless they show signs of toxicity, sepsis, airway compromise, inability to swallow, or other complications.
ConsultationsAn otolaryngologist may be required if the patient's presentation is severe. An anesthesiologist or surgeon may be required for management of a difficult airway
Medication SummaryAntibiotics are the main component of therapy.
Begin antibiotic therapy prior to needle aspiration and report of culture results.
Though several studies have shown intravenous penicillin alone is clinically effective (provided the abscess is adequately drained), other studies have reported that greater than 50% of cultures grow beta-lactamase – producing anaerobes, leading to the tendency to

use broader-spectrum antibiotics such as clindamycin or a second- or third-generation oral cephalosporin.
In those patients allergic to penicillin, clindamycin is a good choice.
Analgesics and throat washes are recommended.
As mentioned above, some physicians report using adjunctive steroids to decrease edema and pain.
AntibioticsClass Summary
Empiric antimicrobial therapy must be comprehensive and should cover all likely pathogens in the context of the clinical setting.
View full drug informationClindamycin (Cleocin)
Semisynthetic antibiotic produced by 7(S)-chloro-substitution of 7(R)-hydroxyl group of parent compound lincomycin. Inhibits bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing RNA-dependent protein synthesis to arrest. Widely distributes in the body without penetration of CNS. Protein bound and excreted by the liver and kidneys.
Oral or parenteral antibiotic for anaerobic or susceptible streptococcal, pneumococcal, or staphylococcal species. Considered to have good absorption into bloodstream in both oral and parental forms.
View full drug informationPenicillin G benzathine (Bicillin L-A)
DOC in combination with metronidazole. Effective in approximately 98% of patients. Interferes with synthesis of cell wall mucopeptide during active multiplication, resulting in bactericidal activity against susceptible microorganisms.
View full drug informationMetronidazole (Flagyl)
DOC in combination with penicillin. Effective in approximately 98% of treated patients.
Imidazole ring-based antibiotic active against various anaerobic bacteria and protozoa. Appears to be absorbed into the cells of microorganisms that contain nitroreductase. Unstable intermediate compounds are formed that bind DNA and inhibit synthesis, causing cell death.
View full drug informationNafcillin (Unipen)
Initial therapy for suspected penicillin G-resistant streptococcal or staphylococcal infections.

Use parenteral therapy initially in severe infections. Change to PO therapy as condition warrants.
Because of thrombophlebitis, particularly in elderly persons, administer parenterally only for short term (1-2 d); change to PO route as clinically indicated.
View full drug informationErythromycin (E.E.S, Ery-Tab, Erythrocin)
Inhibits bacterial growth, possibly by blocking dissociation of peptidyl tRNA from ribosomes, causing RNA-dependent protein synthesis to arrest. For treatment of staphylococcal (including S aureus) and streptococcal infections.
Indicated if patient is allergic to penicillin.
Further Inpatient CareObservation, imaging studies, airway management, and intravenous hydration may be required.
Other methods of operative management strategy may be indicated and should be performed by an otolaryngologist.
Recurrence obviates the need for a second hospitalization for interval tonsillectomy after needle decompression or incision and drainage.
To prevent recurrence, interval tonsillectomy may be considered 3-4 weeks after resolution of edema and symptoms.
Further Outpatient CareIf outpatient care is used, the patient can be discharged on an appropriate regimen of antibiotics and pain medications.
Relative indications for elective tonsillectomy can be identified in almost a third of all patients who present with paratonsillar abscess (eg, recurrent tonsillitis).
ComplicationsComplications of peritonsillar abscess may include the following:
Necrotizing soft tissue infection of the neck and chest wall[12]
Recurrence Aspiration, which may lead to pneumonia or pneumonitis Cervical abscess Mediastinitis Meningitis Sepsis Cerebral abscess Jugular vein thrombosis Carotid artery rupture/necrosis Carotid artery injury (from I&D or needle aspiration)

PrognosisUncomplicated, treated peritonsillar abscess has a resolution rate of 94%. In the United States, the recurrence rate is 10%, although this rate jumps to 15% internationally.
Patient EducationFor patient education resources, see the Ear, Nose, and Throat Center, as well asPeritonsillar Abscess, Tonsillitis, and Antibiotics.
ABSES PERITONSIL
Diposkan oleh Taufik Abidinoleh: Taufik Abidin
PENDAHULUAN
Abses peritonsiler dapat terjadi pada umur 10-60 tahun, namun paling sering terjadi pada
umur 20-40 tahun. Pada anak-anak jarang terjadi kecuali pada mereka yang menurun sistem
immunnya, tapi infeksi bisa menyebabkan obstruksi jalan napas yang signifikan pada anak-anak.
Infeksi ini memiliki proporsi yang sama antara laki-laki dan perempuan. Bukti menunjukkan
bahwa tonsilitis kronik atau percobaan multipel penggunaan antibiotik oral untuk tonsilitis akut
merupakan predisposisi pada orang untuk berkembangnya abses peritonsiler. Di Amerika insiden
tersebut kadang-kadang berkisar 30 kasus per 100.000 orang per tahun, dipertimbangkan hampir
45.000 kasus setiap tahun4.
Abses leher dalam terbentuk dalam ruang potensial diantara fasia leher dalam sebagai
akibat dari penjalaran infeksi dari berbagai sumber, seperti gigi, mulut, tenggorok, sinus
paranasal, telinga tengah dan leher tergantung ruang mana yang terlibat. Gejala dan tanda klinik
dapat berupa nyeri dan pembengkakan. Abses peritonsiler (Quinsy) merupakan salah satu dari
Abses leher dalam dimana selain itu abses leher dalam dapat juga abses retrofaring, abses
parafaring, abses submanidibula dan angina ludovici (Ludwig Angina) 3.
Abses peritonsiler adalah penyakit infeksi yang paling sering terjadi pada bagian kepala
dan leher. Gabungan dari bakteri aerobic dan anaerobic di daerah peritonsilar. Tempat yang bisa
berpotensi terjadinya abses adalah adalah didaerah pillar tonsil anteroposterior, fossa piriform
inferior, dan palatum superior4.
Abses peritonsil terbentuk oleh karena penyebaran organisme bakteri penginfeksi
tenggorokan kesalah satu ruangan aereolar yang longgar disekitar faring menyebabkan

pembentukan abses, dimana infeksi telah menembus kapsul tonsil tetapi tetap dalam batas otot
konstriktor faring5.Peritonsillar abscess (PTA) merupakan kumpulan/timbunan (accumulation) pus (nanah) yang terlokalisir/terbatas (localized) pada jaringan peritonsillar yang terbentuk sebagai hasil dari suppurative tonsillitis.
ETIOLOGI
Abses peritonsil terjadi sebagai akibat komplikasi tonsilitis akut atau infeksi yang
bersumber dari kelenjar mucus Weber di kutub atas tonsil. Biasanya kuman penyebabnya sama
dengan kuman penyebab tonsilitis. Biasanya unilateral dan lebih sering pada anak-anak yang
lebih tua dan dewasa muda2.
Abses peritonsiler disebabkan oleh organisme yang bersifat aerob maupun yang bersifat
anaerob. Organisme aerob yang paling sering menyebabkan abses peritonsiler
adalah Streptococcus pyogenes(Group A Beta-hemolitik streptoccus), Staphylococcus aureus,
danHaemophilus influenzae. Sedangkan organisme anaerob yang berperan
adalah Fusobacterium. Prevotella, Porphyromonas, Fusobacterium,dan Peptostreptococcus
spp. Untuk kebanyakan abses peritonsiler diduga disebabkan karena kombinasi antara organisme
aerobik dan anaerobik6.
PATOLOGI
Patofisiologi PTA belum diketahui sepenuhnya. Namun, teori yang paling banyak
diterima adalah kemajuan (progression) episode tonsillitis eksudatif pertama menjadi
peritonsillitis dan kemudian terjadi pembentukan abses yang sebenarnya (frank abscess
formation).
Daerah superior dan lateral fosa tonsilaris merupakan jaringan ikat longgar, oleh karena
itu infiltrasi supurasi ke ruang potensial peritonsil tersering menempati daerah ini, sehingga
tampak palatum mole membengkak. Abses peritonsil juga dapat terbentuk di bagian inferior,
namun jarang.
Pada stadium permulaan, (stadium infiltrat), selain pembengkakan tampak juga
permukaan yang hiperemis. Bila proses berlanjut, daerah tersebut lebih lunak dan berwarna
kekuning-kuningan. Tonsil terdorong ke tengah, depan, dan bawah, uvula bengkak dan terdorong
ke sisi kontra lateral.

Bila proses terus berlanjut, peradangan jaringan di sekitarnya akan menyebabkan iritasi
pada m.pterigoid interna, sehingga timbul trismus. Abses dapat pecah spontan, sehingga dapat
terjadi aspirasi ke paru.
Selain itu, PTA terbukti dapat timbul de novo tanpa ada riwayat tonsillitis kronis atau
berulang (recurrent) sebelumnya. PTA dapat juga merupakan suatu gambaran (presentation) dari
infeksi virus Epstein-Barr (yaitu: mononucleosis).
GEJALA KLINIS DAN DIAGNOSIS
Selain gejala dan tanda tonsilitis akut, terdapat juga odinofagia (nyeru menelan) yang
hebat, biasanya pada sisi yang sama juga dan nyeri telinga (otalgia), muntah (regurgitasi), mulut
berbau (foetor ex ore), banyak ludah (hipersalivasi), suara sengau (rinolalia), dan kadang-kadang
sukar membuka mulut (trismus), serta pembengkakan kelenjar submandibula dengan nyeri tekan.
Bila ada nyeri di leher (neck pain) dan atau terbatasnya gerakan leher (limitation in neck
mobility), maka ini dikarenakan lymphadenopathy dan peradangan otot tengkuk (cervical muscle
inflammation)1.
Prosedur diagnosis dengan melakukan Aspirasi jarum (needle aspiration). Tempat
aspiration dibius / dianestesi menggunakan lidocaine dengan epinephrine dan jarum besar
(berukuran 16–18) yang biasa menempel pada syringe berukuran 10cc. Aspirasi material yang
bernanah (purulent) merupakan tanda khas, dan material dapat dikirim untuk dibiakkan.
Pada penderita PTA perlu dilakukan pemeriksaan7:

1. Hitung darah lengkap (complete blood count), pengukuran kadar elektrolit (electrolyte
level measurement), dan kultur darah (blood cultures).
2. Tes Monospot (antibodi heterophile) perlu dilakukan pada pasien dengan tonsillitis dan
bilateral cervical lymphadenopathy. Jika hasilnya positif, penderita memerlukan
evaluasi/penilaian hepatosplenomegaly. Liver function tests perlu dilakukan pada
penderita dengan hepatomegaly.
3. “Throat culture” atau “throat swab and culture”: diperlukan untuk identifikasi organisme
yang infeksius. Hasilnya dapat digunakan untuk pemilihan antibiotik yang tepat dan
efektif, untuk mencegah timbulnya resistensi antibiotik.
4. Plain radiographs: pandangan jaringan lunak lateral (Lateral soft tissue views) dari
nasopharynx dan oropharynx dapat membantu dokter dalam menyingkirkan diagnosis
abses retropharyngeal.
5. Computerized tomography (CT scan): biasanya tampak kumpulan cairan hypodense di
apex tonsil yang terinfeksi (the affected tonsil), dengan “peripheral rim enhancement”.
6. Ultrasound, contohnya: intraoral ultrasonography.
KOMPLIKASI
Komplikasi yang mungkin terjadi ialah2:
1. Abses pecah spontan, mengakibatkan perdarahanm aspirasi paru, atau piema.
2. Penjalaran infeksi dan abses ke daerah parafaring, sehingga terjadi abses parafaring.
Kemudian dapat terjadi penjalaran ke mediastinum menimbulkan mediastinitis.
3. Bila terjadi penjalaran ke daerah intracranial, dapat mengakibatkan thrombus sinus
kavernosus, meningitis, dan abses otak.
Sejumlah komplikasi klinis lainnya dapat terjadi jika diagnosis PTA diabaikan. Beratnya
komplikasi tergantung dari kecepatan progression penyakit. Untuk itulah diperlukan penanganan
dan intervensi sejak dini.
DIAGNOSIS BANDING
Infiltrat peritonsil, tumor, abses retrofaring, abses parafaring, aneurisma arteri karotis
interna, infeksi mastoid, mononucleosis, infeksi kelenjar liur, infeksi gigi, dan adenitis tonsil2,8,9.

TERAPI
Pada stadium infiltrasi, diberikan antibiotika dosis tinggi dan obat simtomatik. Juga perlu
kumur-kumur dengan air hangat dan kompres dingin pada leher. Antibiotik yang diberikan ialah
penisilin 600.000-1.200.000 unit atau ampisilin/amoksisilin 3-4 x 250-500 mg atau sefalosporin
3-4 x 250-500 mg, metronidazol 3-4 x 250-500 mg2.
Bila telah terbentuk abses, dilakukan pungsi pada daerah abses, kemudian diinsisi untuk
mengeluarkan nanah. Tempat insisi ialah di daerah yang paling menonjol dan lunak, atau pada
pertengahan garis yang menghubungkan dasar uvula dengan geraham atas terakhir. Intraoral
incision dan drainase dilakukan dengan mengiris mukosa overlying abses, biasanya diletakkan di
lipatan supratonsillar. Drainase atau aspirate yang sukses menyebabkan perbaikan segera gejala-
gejala pasien.
Bila terdapat trismus, maka untuk mengatasi nyeri, diberikan analgesia lokal di ganglion
sfenopalatum.
Kemudian pasien dinjurkan untuk operasi tonsilektomi “a” chaud. Bila tonsilektomi
dilakukan 3-4 hari setelah drainase abses disebut tonsilektomi “a” tiede, dan bila tonsilektomi 4-
6 minggu sesudah drainase abses disebut tonsilektomi “a” froid. Pada umumnya tonsilektomi
dilakukan sesudah infeksi tenang, yaitu 2-3 minggu sesudah drainase abses2.
Tonsilektomi merupakan indikasi absolut pada orang yang menderita abses peritonsilaris
berulang atau abses yang meluas pada ruang jaringan sekitarnya. Abses peritonsil mempunyai
kecenderungan besar untuk kambuh. Sampai saat ini belum ada kesepakatan kapan tonsilektomi
dilakukan pada abses peritonsil. Sebagian penulis menganjurkan tonsilektomi 6–8 minggu
kemudian mengingat kemungkinan terjadi perdarahan atau sepsis, sedangkan sebagian lagi
menganjurkan tonsilektomi segera10.
Penggunaan steroids masih kontroversial. Penelitian terbaru yang dilakukan Ozbek
mengungkapkan bahwa penambahan dosis tunggal intravenous dexamethasone pada antibiotik
parenteral telah terbukti secara signifikan mengurangi waktu opname di rumah sakit (hours
hospitalized), nyeri tenggorokan (throat pain), demam, dan trismus dibandingkan dengan
kelompok yang hanya diberi antibiotik parenteral.

PROGNOSIS
Abses peritonsoler hampir selalu berulang bila tidak diikuti dengan tonsilektomi., maka
difunda sampai 6 minggu berikutnya. Pada saat tersebut peradangan telah mereda, biasanya
terdapat jeringan fibrosa dan granulasi pada saat oprasi.
DAFTAR PUSTAKA
1. Adams, G.L. 1997. Penyakit-Penyakit Nasofaring Dan Orofaring. Dalam: Boies, Buku Ajar
Penyakit THT, hal.333. EGC,Jakarta.
2. Fachruddin, darnila. 2006. Abses Leher Dalam. Dalam: Buku Ajar Ilmu Kesehatan, Telinga-
Hidung-Tenggorokan, hal. 185. Balai Penerbit FKUI, Jakarta.
3. Soepardi,E.A, Iskandar, H.N, Abses Peritonsiler, Buku Ajar Ilmu Kesehatan Telinga,
Hidung dan Tenggorokan, Jakarta: FKUl, 2000; 185-89.
4. Mehta, Ninfa. MD. Peritonsillar Abscess. Available from.www.emedicine.com. Accessed at
Juli 2007.
5. Adrianto, Petrus. 1986. Penyakit Telinga, Hidung dan Tenggorokan, 296, 308-09.
EGC, Jakarta.
6. Bailey, Byron J, MD. Tonsillitis, Tonsillectomy, and Adenoidectomy. In : Head and Neck
Surgey-Otolaryngology 2nd Edition. Lippincott_Raven Publisher. Philadelphia. P :1224,
1233-34.
7. Anurogo, Dito. 2008. Tips Praktis Mengenali Abses Peritonsil.
Accessed: http://www.kabarindonesia.com/berita.php?pil=3&dn=20080125161248.
8. Preston, M. 2008. Peritonsillar Abscess (Quinsy).
accessed:http://www.patient.co.uk/showdoc/40000961/.

9. STEYER, T. E. 2002. Peritonsillar Abscess: Diagnosis and Treatment.
accessed:http://www.aafp.org/afp/20020101/93.html.
10. Hatmansjah. Tonsilektomi. Cermin Dunia Kedokteran Vol. 89, 1993. Fakultas Kedokteran
Universitas Indonesia, hal : 19-21.