Embed Size (px)
Citation preview

In!. J. Radiation Oncology Biol. Phys., Vol. IS, pp. 81 S-822 0360-3016/88 $3.00 + .LKJ
Printed in the U.S.A. All rights reserved. Copyright 0 I988 Pergamon Press plc
??Original Contribution
PERITONEAL FLUID CYTOLOGY IN ENDOMETRIAL CANCER: ITS SIGNIFICANCE AND THE ROLE OF CHROMIC PHOSPHATE (32P) THERAPY
ROBERT HEATH, M.D.,* JULIAN ROSENMAN, PH.D., M.D.,* MAHESH VARIA, M.D.*
AND LESLIE WALTON, M.D.t
University of North Carolina at Chapel Hill, N.C.
Between 1978 and 1986,243 patients (all stages) had peritoneal fluid cytology performed while undergoing total abdominal hysterectomy for endometrial carcinoma; 39 (16%) were found be positive. At 3 years (median follow- up of 30 months) the disease-free survival (DFS) for the 165 negative cytology clinical Stage I patients was 91% compared to only 56% for the 25 positive cytology patients (p < .OOl). Of the 25 Stage I positive cytology patients, 14 with greater than one-third myometrial invasion had a DFS of 30% at 3 years as compared to 87% for negative cytology patients with comparable depth of invasion (p < .OOl). There was no difference in DFS between the negative and positive cytology Stage I patients who had one-third or less myometrial invasion. Stage I patients with histologic Grade 2 and 3 had a lower 3 year DFS when cytology positive, 49% and 22%, versus 92% and 79% when cytology negative (p < .OOl andp = .03 respectively). In clinical Stage II patients the 3-year DFS was 21% for those with a positive cytology and 59% with a negative cytology. Fourteen of the 25 clinical Stage I positive cytology patients received 15 mCi of intraperitoneal 32P. At 3 years they had a 68% DFS as compared to 27% for those not receiving 32P (p = 0.01). All 11 patients with superficial myometrial invasion (9 received 32P) remained disease-free. The 4 Stage I patients with deep invasion who received 32P therapy had an improvement in abdomi- nal/pelvic control and DFS when compared to 9 similar patients who did not receive ‘*P (p = .02). For histologic Grade 2 and 3 patients, there was a 64% 3-year DFS in the 32P treated group and 16% for those not receiving 32P (p = 0.02). Although ‘*P therapy improved DFS in Stage I positive cytology patients its use along with pelvic radiation therapy can lead to complications. Of 9 Stage I patients receiving ‘*P as well as pelvic irradiation, 4 experienced serious bowel complications requiring surgery. None of the 5 patients receiving 32P only had a complication.
Positive peritoneal fluid cytology, Endometrial cancer, Intraperitoneal 32P.
INTRODUCTION with a positive cytology. However, Konski et al.” and Yazigi et a1.26 found no significant difference in disease-
Although early stage endometrial carcinoma is usually curable,16 several factors are known to be predictive for treatment failure. These include advanced stage, high histologic tumor grade, deep myometrial invasion, lower uterine segment involvement, and nodal and adnexal metastases.8 Whereas patients with good prognostic fac- tors do uniformly well, patients with poor prognostic fac- tors have a more varied course. This suggests that further prognostic variables wait to be determined. Increasingly recognized in various gynecologic cancers as having ad- verse prognostic significance, is the presence of malig- nant cells in the peritoneal fluid (positive cytology).4,*4,‘7
The significance of a positive cytology in endometrial cancer patients is controversial. Creasman et al3 found an increased recurrence rate in clinical Stage I patients
free survival (DFS) between positive and negative cytol- ogy patients. Similarly the need to alter treatment in patients with positive cytology remains unclear. The successful use of intraperitoneal radioactive chromic phosphate (32P) in ovarian cancer patients with malig- nant cytologies’x’ 1,‘2,25 led Creasman et aL4 to use intra- peritoneal 32P in a group of positive cytology patients with Stage I endometrial cancer. These investigators re- ported a significantly decreased recurrence rate in these patients as compared to historical controls.4 On the other hand, Konski et al. I5 did not find any significant im- provement in recurrence rates or survival in positive cy- tology patients who received whole abdominal irradia- tion as compared to those who received only pelvic irra- diation.
Presented at the 29th Annual Scientific Meeting ofthe Amer- ican Society for Therapeutic Radiology and Oncology, Boston, MA, October 20, 1987.
* Department of Radiation Oncology. t Division of Gynecologic Oncology.
815
Reprint requests to: Robert Heath, M.D., Department of Ra- diation Oncology, The University of North Carolina, Chapel Hill, NC 275 14.
Accepted for publication 2 1 April 1988.

816 I. J. Radiation Oncology 0 Biology 0 Physics October 1988, Volume 15, Number 4
At the University of North Carolina assessment of peritoneal fluid cytology was studied in endometrial can- cer patients since 1978. Intraperitoneal 32P has been given to selected positive cytology patients since 1980. We report on the prognostic significance of positive peri- toneal cytology and the results of the use of intraperito- neal 32P as a therapeutic modality in these patients.
METHODS AND MATERIALS
From January 1978 through December 1986, 237 patients with endometrial carcinoma underwent total abdominal hysterectomy, bilateral salpingo-oophorec- tomy, selected pelvic and para-aortic lymph node biop- sies, and collection of peritoneal fluid for cytologic evalu- ation at the University of North Carolina. In addition six patients, having undergone a similar operation at an outside hospital and found to have malignant cells in the peritoneal fluid, were referred for further therapy. The material for cytology was collected by aspiration of peri- toneal fluid, if there was sufficient quantity, or by pelvic washings with 100-200 cc’s of normal saline or Hespan@ upon opening the abdomen before further exploration. All cytologic and pathologic materials were reviewed by the pathologists at the University of North Carolina.
Patients with malignant cells in the peritoneal fluid (positive cytology) received intraperitoneal 32P using a standardized procedure. Intraperitoneal 32P was admin- istered only to those positive cytology patients who had no gross residual disease after total abdominal hysterec- tomy. A peritoneal dialysis catheter was inserted under local anesthesia and 150-200 cc’s of normal saline in- stilled. A tracer dose of 1 mCi of 99Tc was injected to image the fluid distribution in the peritoneal cavity. The patient was then maneuvered and scanned to determine if adequate distribution within the pelvis as well as the upper abdomen was possible. If the distribution was ade- quate, 15 mCi of chromic 32P was mixed with 500 cc’s of normal saline and infused into the peritoneal cavity. This was followed by an additional 500- 1000 cc’s of nor- mal saline. The catheter was then removed and the entry site closed with one or two purse-string sutures. During the next 3-4 hr the patient was rotated every 15 minutes into multiple positions (supine, prone, right and left de- cubitus, Trendelenberg and reverse Trendelenberg) to ensure a good distribution of the 32P. Appropriate radia- tion safety precautions were observed and the patient monitored for any spill or leakage.
Sixteen of the 39 patients with positive cytologies re- ceived 32P. Ten of the 16 patients also received pelvic irradiation. Twenty-three patients with positive cytolo- gies did not receive 32P for various reasons. Reasons in- cluded extensive tumor found at laparotomy (11 pa- tients), a positive cytology found prior to the implemen- tation of 32P therapy in 1980 (4 patients), whole abdominal radiation instead (2 patients), the inability to perform the intraperitoneal therapy safely (2 patients)
and uncertain reasons (4 patients). Nine patients re- ceived radiation only and 14 received a progestational agent only. In the negative cytology group, 95 of 204 pa- tients received intracavitary and/or external beam pelvic irradiation.
Information on patient follow-up was obtained through a retrospective hospital chart review. Disease- free survival (DFS) was calculated using Kaplan-Meier13 survival curves. Statistical significance between survival curves was determined by the log rank method.20
RESULTS
All stages Thirty-nine of the 243 patients (16%) were found to
have positive cytologies. Table 1 summarizes the inci- dence of positive cytology for each clinical stage. At pres- ent, 202 patients are alive and 4 1 have died. The median follow-up for the entire population was 30 months. The actuarial survival for the entire 243 patients was 80% at 3 years with a DFS of 77%.
Clinical stage I Survival by peritoneal cytology. Twenty-five ( 13%) of
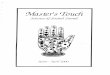
190 clinical Stage I patients had positive cytologies. As seen in Figure 1, the 3-year DFS of the negative cytology patients was 9 1% and 56% for the positive cytology pa- tients (p < .OOl).
Survival by peritoneal cytology and depth of myome- trial invasion. Of the 190 clinical Stage I patients, 134 had myometrial invasion of f or less (superficial inva- sion) and 55 had myometrial invasion of more than f (deep invasion). In one patient treated with 32P the depth of invasion was not recorded. The 3-year disease-free sur- vivals were, respectively, 92% and 74% (p < .OO 1).
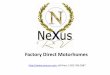
The 3-year DFS for the 11 patients with superficial in- vasion and positive cytology was 89% versus 92% for the 123 patients with superficial invasion and negative cytol- ogy (p = .7 1). Nine of the 11 patients received 32P. How- ever, the 3-year DFS for the 13 patients with deep inva- sion and positive cytology was 30% versus 87% (p < .OO 1) for the 42 patients with deep invasion and negative cytol- ogy (Fig. 2). Ten of the 13 patients had received pelvic irradiation.
Survival by peritoneal cytology and tumor grade. At 3 years the DFS for the 89 patients with negative cytology and grade I histology was 95%. This did not differ sig-
Table 1. Patient population by stage and cytology
Stage Positive cytology/Total patients
I 25/190(13%) II 7/40 (18%)
III 3/8 (38%) IV 4/5 (80%)
Total 39/243 ( 16%)

Peritoneal fluid cytology in endometrial cancer 0 R. HEATH et al. 817
_ _ _!83) S1ogeI Negative Cytology (40) -_______ ___________ L______!!T’
(p<.OOi)
l- 5 20 -
1 3 I I 1 I I 0 12 48 60
Fig. 1. Clinical Stage I disease-free survival by cytology status.
nificantly from the survival of the 5 positive cytology, grade I patients none of whom suffered a recurrence. Stage I patients with histologic grade II had a significantly lower (p < .OOl) 3-year DFS with a positive cytology (49%) as compared with a negative cytology (92%). This trend continued for patients with grade III histology as those with a positive cytology had a DFS of 22% at 17 months as compared to 79% at 3 years for negative cytol- ogy patients (p = .03).
Relationship of peritoneal cytology to other prognostic factors. As shown in Table 2 there were small numbers of Stage I patients with other adverse prognostic factors. In each case the percentage of patients with the adverse factor was higher in the positive cytology patients. How- ever, the total number of patients in each category is too small for a useful analysis.
stage I
(26) Negolive Cytology
--_____--- ,_ _ _ _ _ _@e ~y_ometriol Invasion (7) ___-- _________
(P<.OOl)
-
MONTHS
Fig. 2. Clinical Stage I disease-free survival for deep invasion by cytology status.
Table 2. Prognostic factors of Clinical Stage I patients by peritoneal cytology
Positive Negative WologY WologY
Prognostic factor n = 25 n= 165
Myometrial invasion* 4 or less 11 (44%) 123 (75%) Greater than f 13 (52%) 42 (25%)
Histologic grade 1 5 (20%) 83 (50%) 2 12 (48%) 57 (35%) 3 8 (32%) 25 (15%)
Involvement of the lower uterine segment 10 (40%) 31(19%)
Cervical involvement 9 (36%) 7 (4%) Adnexal metastases 7 (28%) 5 (3%) Nodal metastases 5 (25%) 3 (2%)
* In one patient the depth of myometrial invasion was not recorded.
“P Intraperitoneal therapy. As seen in Table 3, only 4/l 3 (3 1%) patients with deep invasion received intra- peritoneal 32P as compared to 9/ 11(82%) with superficial invasion. Therefore, any analysis of the efficacy of 32P therapy must be corrected for depth of myometrial inva- sion. In addition, we corrected for tumor grade even though the imbalance between those treated with 32P and not treated was not as pronounced. There are too few patients to correct for other adverse factors although it should be noted that included in the 32P treated group were three patients who had adnexal metastases and one patient who had pelvic and periaortic node metastases.
The 3-year DFS for the group receiving 32P was 76% versus 27% for the group not receiving 32P (Fig. 3). For those patients with superficial invasion the DFS for the 32P treated group was 86% at 3 years compared to 100% for the two patients with superficial invasion who were not treated with 32P (p = 59). For the four patients with deep invasion treated with 32P had a 3-year DFS of 75%
Table 3. Clinical Stage I, outcome by peritoneal cytology and therapy
Cytology positive
32p* No 32P WhY negative
n= 14 n= 11 n= 165
Recurrences
Myometrial invasion* f of less l/9(11%) O/2(0%) 7/123 (6%) Greater than f l/4 (25%) 7/9 (78%) 4/42 (10%)
Histologic grade
: O/4 (0%) O/l (0%) 4/83 (5%) l/6(17%) 5/6(83%) 3/57 (5%)
3 2/4 (50%) 2/4 (50%) 4/25 (16%)
* In one 32P treated patient the depth of myometrial invasion was not recorded.

818 1. J. Radiation Oncology 0 Biology 0 Physics October 1988, Volume 15, Number 4
5 -_____-_ 1
’ 80
I
I stogc I 32~ Traoted
07 ; (IO) (5) Positive Cytology (I) --__-- -_-________ -_---
(p=.OOl)
_
01'1"'1'1'1 0 12 24 36 48 60
MONTHS
Fig. 3. Clinical Stage I, positive cytology disease-free survival by 32P treatment status.
versus 2 1% at 8 months for the 9 patients with positive cytologies not treated with 32P (p = .02, see Fig. 4).
All 5 positive cytology patients with histologic grade I were disease-free at last follow-up irrespective of treat- ment. For the histologic grade II group six patients re- ceived 32P and six did not. The 3-year DFS was 80% for the 32P treated group versus 17% (one patient) alive at 8 months for the non-32P treated group (p = 0.01). For histologic grade III, four patients were treated with 32P and 4 were not. The 3-year DFS for the 32P treated group (38%) versus no survivors in those not treated with 32P (p = .48). Combining grades II and III with 10 patients in each group those patients treated with 32P had a 3-year DFS of 64% compared to 16% for those not treated with 32P (p = .02).
stage I 32p Treated Positive Cytology Deep Myomshial Invasion (3) ________---------- _ _-_
(D=.o2)
Positive Cytology Deep Myomatrial lnvosion
MONTHS
Fig. 4. Clinical Stage I, positive cytology disease-free survival for deep myometrial invasion by 32P treatment status.
Patterns of recurrence. There were 12 recurrences in the 165 (7%) clinical Stage I negative cytology patients. Only 2 ( 16%) ofthe recurrences had an abdominal/pelvic component (Table 4). In the positive cytology group not treated with intraperitoneal 32P (11 patients) there were seven recurrences. Of these 5/7 patients had an abdomi- nal/pelvic component as the site of initial failure. In the 32P treated group ( 14 patients) there were three recur- rences and one was abdominal/pelvic. Thus 5/l 1 pa- tients not receiving 32P had a component of abdominal failure as compared to l/ 14 who received 32P.
Complications. Nine of the 14 patients receiving 32P also received pelvic external beam radiation therapy (ERT) shortly before or after 32P. Four of these 9 patients developed bowel complications requiring corrective sur- gery; one eventually died of complications. Another of the four patients underwent multiple surgeries and de- veloped permanent short bowel syndrome. However, she is without disease at 65 months. A third patient died of a CVA 6 months following surgery; she suffered from short bowel syndrome at the time of death. A fourth patient is alive with mild radiation enteritis. These data are sum- marized in Table 5. There were 5 32P treated patients who did not receive any pelvic ERT or brachytherapy; there were no complications in this group and a11 are alive without disease.
In the 1 1 patients with positive cytology not treated by 32P. 4 patients ec r eived pelvic ERT and 2 patients re- ceived whole abdominal radiation (both whole abdomen irradiated patients are alive and NED at 6 and 8 months respectively). There were no complications in any of the 1 1 patients.
By comparison the negative cytology group had 10 complications (6%). Three patients had partial bowel ob- struction that did not require surgical intervention. Two of these patients were not irradiated and presumably the obstruction was due to post-surgical effects. In addition, there were two patients with bowel obstructions who re- quired surgery. Both patients had been previously irradi- ated. There were two patients with fistulas (one required surgery) both of whom had ERT and pelvic brachyther- apy. One patient who had received both ERT and vagi- nal brachytherapy developed a large vaginal ulcer which
Table 4. Clinical Stage I-Sites of relapse by cytology and therapy
Site of relapse
Positive cytology Negative
32 P No 32P WologY n= 14 n= 11 n= 165
Abdomen/pelvic only 1 5 1 Vagina 3 Pelvic and distant
:, : 1
Distant only 1 1 6 Unspecified 0 1 1
Total relapses 3 (21%) 7 (64%) 12 (7%)

Peritoneal fluid cytology in endometrial cancer ??R. HEATH et al.
Table 5. Complications in patients receiving 32P and pelvic radiation
819
Clinical stage Adjuvant therapy
Time to complication Type of complication Surgical findings
Ultimate outcome
32P 6 days postop 4900 cGy pelvic ERT
IAG~ 32P 11 days postop 5000 cGy pelvic ERT
IBGZ
IAGZ
32P 14 days postop 4590 cGy pelvic ERT
32P 11 days postop 4500 cGy pelvic ERT
11 months Repeated bowel obstruction Adhesions, no tumor
18 months Repeated bowel obstruction Adhesions, no tumor
Between lo- 19 Acute bowel obstruction Unknown months
7 months Repeated bowel obstructions Multiple bowel fistula, peritoneal fluid negative
Postop: postoperative; ERT: external beam radiation therapy.
eventually healed spontaneously. Finally there was a had obvious ascites and a positive cytology; none re- large pelvic lymphocele in a patient treated with ERT ceived intraperitoneal 32P. Three patients are dead from and brachytherapy. She was asymptomatic and did not persistent cancer and two are alive with persistent dis- require surgery. ease.
Clinical Stages II, III and IV The 3-year DFS for all clinical Stage II patients was
52%. For the negative cytology patients the DFS was 59% compared to 2 1% for positive cytology patients (Fig. 5). Only two Stage II positive cytology patients received 32P. Despite the fact that neither of these 32P treated patients had adnexal or nodal metastases, one died of disease at 14 months and the other recurred at 18 months.
The 3-year DFS for clinical Stage III patients was 42%. For the negative cytology patients it was 53%, and none of the positive cytology patients survived past 22 months.
All five Stage IV patients went to surgery for what was thought to be ovarian cancer. Four of these five patients
--- - _ i-_
L I
slog0 II ----:(13) Negative Cytokqy (51 _--___-________
(p <.OOl)
stage II Positive Cytology 101
_
OO'--1 36 60
MONTHS
Fig. 5. Clinical Stage II disease-free survival by cytology status.
Died of CVA at 6 months; short bowel syndrome
NED at 65 mo with short bowel syndrome
NEDat 19mo
Died of sepsis related to fistula
DISCUSSION
In one of the original papers on the subject, Marcus” reported on 15 endometrial cancer patients of whom 3 had positive cytology. All 3 patients had deep (> 4) myo- metrial invasion and 2 died within 14 months. In a later study Keettel et al. I4 found 5 of 39 ( 13%) Stage I patients had positive cytologies. The authors did not describe a correlation of positive cytology with other known ad- verse prognostic factors.
Many modes of spread have been postulated to ex- plain the presence of malignant cells in the peritoneal cavity. The most obvious would be by direct extension through the myometrium and serosa into the peritoneal cavity. In our Stage 1 patients, 13/24 (54%) with positive cytology had deep myometrial invasion as compared to only 42/ 165 (25%) with negative cytology. Another route of metastatic spread may be through vascular/lymphatic pathways to the ovary2 and shedding of cells at that site. Direct intraperitoneal spread, from microscopic lymph node deposits, is unlikely as these structures are extra- peritoneal. In our positive cytology clinical Stage I pa- tients adnexal involvement occurred in 7/25 (28%) of positive cytology patients as compared to only 5/165 (3%) of the negative cytology patients. Yet another route of spread can be iatrogenic dislodgment of cells during biopsy, dilatation and curettage, or placement of intra- uterine radiation sources. These cells can then migrate through the fallopian tubes into the peritoneal cavity. In this case the finding of positive cytology may not be bio- logically important which may explain why our patients with superficial myometrial invasion and positive cytol- ogy did so well. Also, in the Yazigi series26 8/ 10 positive

820 1. J. Radiation Oncology 0 Biology 0 Physics October 1988. Volume 15, Number 4
cytology patients had had preoperative intrauterine ra- dium therapy. For ovarian cancer, pluripotential perito- neal cells have been cited as a possible cause of malignant cytologies, but endometrial cancer has a different embry- onic origin making this an unlikely possibility. Finally, the possibility of interpretation difficulties by the review- ing cytologist may lead to a false positive or negative reading.
In the first large series evaluating the significance of peritoneal fluid cytology in endometrial cancer, Creas- man et ~1.~‘~ found 26/ 167 clinical Stage I patients had positive cytologies. This group also reported a correla- tion between positive cytology and the other adverse prognostic factors. Positive cytologies were seen in 11/35 (3 1%) of patients with deep myometrial invasion versus 15/l 32 (8%) with superficial invasion. The discovery of extrauterine disease at laparotomy was also correlated with increased rates of positive cytology. The rates were 46, 60, 65, and 72% respectively for cervical, adnexal, pelvic and para-aortic node involvement. Finally, posi- tive cytologies were seen in 9, 22, and 16% respectively for tumor grades 1,2, and 3.
In a more recent study, Yazigi et r~/.~’ reported on 93 clinical Stage I patients of whom 10 had positive cytology (7/ 10 had superficial disease). The incidence of positive cytology by depth of myometrial invasion was not statis- tically different for patients with superficial and deep in- vasion. The distribution of patients with positive cytol- ogy for tumor grades 1, 2, and 3 were 11, 7, and 17%’ respectively. The authors did not report that any patients had cervical or extra-uterine disease.
The positive cytology rate in our study ( 13%) was com- parable to the previous studies. As in the Creasman and associates3.4 series we found an increased rate of positive cytologies in patients with deep (24%) versus superficial (8%) myometrial invasion (Table 2). We also found that positive cytology patients had higher rates of cervical, lower uterine segment, adnexal, and lymph node in- volvement (Table 2). Positive cytologies were seen in 6, 17, and 24% of our patients for tumor grades 1, 2 and 3 respectively.
Creasman et al. and others3*4.23,24 were the first to find that conventionally treated positive cytology, clinical Stage I patients recurred more frequently (38% at 31 months) than negative cytology patients of comparable Stage (10% at 48 months). On the other hand. Konski et al. I5 found no statistical difference in recurrence or sur- vival rates between 114 negative and I 8 positive cytology clinical Stage I endometrial carcinoma patients (10% and 16% recurrences respectively). Likewise, Yazigi et ~1.~~ could not find a difference in DFS at 10 years between negative and positive cytology patients, 65 and 60% re- spectively. In none of these three studies were recurrence and survival rates for patients with positive cytologies correlated with depth of invasion or tumor grade.
Our results were again similar to those of Creasman et ~1.~‘~ In our clinical Stage I patients recurrences were seen
in 40% with positive cytology (at 30 months) versus 7% with negative cytology. However, in our patients with su- perficial invasion, no difference was seen in DFS between the positive and negative cytology groups. Only our posi- tive cytology patients with deep invasion had a worse DFS. Therefore, our results are not inconsistent with those of Yazigi et a1.26 as most of the patients in their series had good prognostic features (superficial invasion). For the higher histologic grade patients the adverse effect on prognosis of a positive cytology is again seen but is not as pronounced.
Radioactive chromic phosphate is available as a sus- pension consisting of particles 0.05- 1 .O microns in size22 which forms a biochemically inert precipitate that pre- cludes intravascular absorption. 32P is a pure beta emitter with an average energy of 0.69 MeV and a half life of 14.3 days. Because of the low electron energy the radia- tion effects are essentially limited to the first few millime- ters of exposed tissue making chromic 32P suitable for treating microscopic surface tumor deposits. These prop- erties also make chromic 32P safe to handle: also a patient injected with 32P poses no hazard to others as the radia- tion is barely detectable outside the peritoneal cavity.
In dog experiments, Currie et aL5 found that 5 mCi of ‘?P suspension delivered 3,000-40,000 cGy at serosal and diaphragmatic surfaces and that thoracic lymph nodes received high doses (average-8700 cGy) whereas para-aortic, pelvic and mesenteric nodes received sub- therapeutic doses (25 to 300 cGy). It was suggested this occurred because the main pathway for clearance of peri- toneal fluid and the chromic 32P is via the diaphragmatic lymph channels and the thoracic lymph nodes. In addi- tion it was noted that the serosal surfaces and the bowel tolerated the intraperitoneal 32P extremely well.’
These properties have led a number of different insti- tutions to use intraperitoneal 32P in the treatment of early ovarian carcinoma. For example, Hester et al. ” ob- tained a 89% survival rate in 9 Stage I ovarian carcinoma patients and Hilaris and Clark’* reported a 93% 5-year survival in 28 patients treated with 32P. Varia et aI.25 pre- sented data which suggest that intraperitoneal 32P may reduce relapses after a negative second-look laparotomy for ovarian cancer. The success of intraperitoneal 32P therapy in ovarian cancer has led to its use in other ma- lignant cytologic conditions such as endometrial cancer.
Creasman et al. and Soper et ~1.~3~~ found that the use of intraperitoneal 32P reduced recurrences in positive cy- tology, clinical Stage I endometrial cancer patients from 38% to 8%. Furthermore, only l/53 32P treated patients had an intra-abdominal recurrence as compared to 6/26 patients not receiving 32P. The authors also reported an 89% 2-year DFS for all 32P treated patients. They did not report their 32P results by depth of invasion or tumor grade.
In our series of clinical Stage I positive cytology pa- tients receiving 32P there was a 3-year DFS of 68% versus 24% for those who did not receive 32P (p = .OO 1). Only

Peritoneal fluid cytology in endometrial cancer 0 R. HEATH et al. 821
l/ 14 (7%) of those treated with 32P recurred with disease in the abdomen compared to 5/l 1 (45%) in the group not treated with 32P. Only one relapse was seen in the patients with superficial invasion and positive cytology; because of the small numbers no conclusions can be drawn as to the value of 32P therapy in this group. 32P therapy appeared to improve survival and abdominal- pelvic control in our patients with positive cytology and deep myometrial invasion (Fig. 4). There was also im- proved abdominal control and survival for histologic grade 2 patients. No benefit from 32P therapy was dem- onstrated in histologic grade 3 patients (Table 3).
The benefit of intraperitoneal 32P therapy must be weighed against the risk of complications. Creasman’s group23 had a 29% (5/ 17 patients) rate of serious compli- cations in those who received 32P and pelvic irradiation. They had no complications in those who received 32P only. Thirty percent (4/14-excluding one patient with bowel obstruction due to cancer recurrence) of our clini- cal Stage I patients who had 32P encountered serious bowel complications requiring surgery. All of these pa- tients had had adjuvant pelvic radiation (Table 5). These findings suggest that there is a combination of effects from surgery, pelvic irradiation and intraperitoneal 32P that predisposes to a significant risk of serious bowel complications. However, the risk of treatment-related complications must be compared to the more serious consequences of cancer recurrence that would occur in approximately 40% of these patients had they not re- ceived intraperitoneal therapy.
Based on the experience with ovarian cancer,6,7 whole abdominal radiation has also been evaluated for the treatment of endometrial carcinoma. Martinez et al.19 reported a 76% disease-free rate at 12 months in high risk patients (Stages II-IV) using abdomino-pelvic radiation. In his series of 24 patients, 69% of patients had positive cytologies. However, Konski et al. I5 found no improve- ment in abdominal recurrences or disease-free survival in 7 of 18 clinical Stage I positive cytology patients re- ceiving whole abdominal radiation.
Other possible therapies for positive cytology, endo- metrial cancer patients include intraperitoneal chemo- therapy’*s2’ as has been tried in ovarian cancer. The use of systemic chemotherapy, however, has been disap- pointing in endometrial cancer. Finally, biologic re-
sponse modifiers such as interferon and monoclonal an- tibodies that may be used in an intraperitoneal infusion remain to be explored.
It is difficult to make specific recommendations for the treatment of endometrial cancer patients with positive cytology. More experience in the management of posi- tive cytology patients is needed. Until such time we sug- gest the following: For Stage I patients with superficial invasion, low histologic grade and no other extra-uterine disease we suggest intraperitoneal 32P infusion only. The conventional approach for higher risk patients is to rec- ommend postoperative pelvic radiation therapy.’ Our experience suggests that intraperitoneal 32P treatment of the entire abdomen improves abdominal/pelvic control and DFS but is associated with an increased rate of com- plications in patients receiving both pelvic irradiation and 32P. This concern of complications necessitates a better modality to treat the entire abdomen and pelvis. Currently, we are exploring the use of whole abdominal radiation with a pelvic boost in positive cytology pa- tients. To minimize the risk for small bowel complica- tions the pelvic irradiation should be performed using techniques to minimize small bowel dose. This could be done by the method described by Gunderson and Tep- per” for postoperative rectal cancer patients.
CONCLUSIONS
In our series of endometrial cancer patients a positive peritoneal fluid cytology adversely affected disease-free survival beyond that for the depth of myometrial inva- sion and histologic grade. Intraperitoneal 32P therapy produced a significant improvement in abdominal/pel- vic control and DFS in Stage I patients with deep inva- sion. We also found an increased risk for serious bowel complications in those patients receiving a combination of intraperitoneal 32P and pelvic irradiation. Because we feel the risk of treatment related complications is signifi- cant with 32P and ERT we currently suggest whole ab- dominal irradiation with pelvic boost for positive cytol- ogy patients with deep invasion, high tumor grade or ex- tra-uterine disease. The Stage I patients with superficial invasion and positive cytology treated with 32P therapy only had one relapse and no complications.
REFERENCES
Alderman, S.J., Dillon, T.F.: Postoperative use of radioac- tive phosphorus in stage I ovarian carcinoma. Obstet. Gy- necol. 49: 659-662, 1977. Barber, H.R., Sommers, S.C.: Carcinoma of the Endome- trium. New York, Masson. 198 1, pp. 20-2 1. Creasman, W.T., DiSaia, P.J., Blessing, J., Wilkinson, R.H., Johnston, W., Weed, J.C.: Prognostic significance of peritoneal cytology in patients with endometrial cancer and preliminary data concerning therapy with intraperito-
4.
5.
neal radiopharmaceuticals. Am. J. Obstet. Gynecol. 141: 921-929,198l.
Creasman, W.T., Rutledge, F.: The prognostic value of peritoneal cytology in gynecologic malignant disease. Am. J. Obstet. Gynecol. 110: 773-781, 1971.
Cunie, J.L., Bagne, F., Harris, C., Sullivan, D.L., Surwitt, M.D., Wilkinson, R.H., Creasman, W.T.: Radioactive chromic phosphate suspension: studies on distribution,

822 1. J. Radiation Oncology 0 Biology 0 Physics October 1988, Volume 15, Number 4
6.
dose absorption and effective radiation in phantoms, dogs and patients. Gynecol. Oncol. 12: 193-2 18, 198 1. Delctos, L.: Malignant tumours ofthe ovary managed with pos?operative megavoltage irradiation. Radiology 93: 659, 1959.
17.
suits of Treatment of Carcinoma of the Uterus, vagina and ovary, Vol. 16. Stockholm, Radiumhemmet. 1975, FI60. Marcus, C.C.: Cytology of the peritoneal cavity in benign and malignant disease. Obstet. Gynecol. 120: 70 l-7 12, 1962.
7.
8.
9.
18.
19.
10. 20.
21.
11.
12.
Dembo, A.: Radiation Therapy in the Management of Ovarian Cancer. Clin. Obscet. Gynecol. 10: 26 1, 1983. DiSaia, P.J.: Clinical Gynecologic Oncology, 2nd edition. St. Louis, C.V. Mosby. 1984, p. 150. Glassburn, J.R., Brady, L.W.: Cancer ofthe endometrium. In Principles and and Practice of Radiation Oncology, Perez C.C., Brady L.W. (Eds.). Philadelphia, PA, J.B. Lip- pincott. 1987, p. 973. Gunderson, L.L., Russell, A.H.. Llewellyn, H.J., Doppke, K.P., Tepper, J.E.: Treatment planning for colorectal can- cer: radiation and surgical techniques and value of small- bowel films. Inc. J. Radiat. Oncol. Biol. Phys. 11: 1379- 1393, 1985. Hester, L.L., White, L.: Radioactive colloid chromic phos- phate in the treatment ofovarian malignancies. Am. J. Ob- stet. Gynecol. 103: 91 l-14, 1969. Hilaris, B.S., Clark, D.G.: The value ofpostoperative intra- peritoneal injection of radiocolloids in early cancer of the ovary. Am. J. Roentgenol. 112: 749, 197 1. Kaplan, E.L., Meier, P.: Non-parametric estimation from incomplete observations. J. Amer. Stat. Assoc. 53: 457- 481, 1958. Keettel, W.C., Pixley, E.E., Buchsbaum, HI.: Experience with peritoneal cytology in the management of gyneco- logic malignancies. Am. J. Obstet. Gynecol. 120: 174- 182, 1974.
22.
23.
13.
24. 14.
25. 15. Konski, A., Poulter, C., Beecham, J., Keys, H., Rubin, P.:
The influence of positive peritoneal cytology in clinical Stage I endometrial adenocarcinoma and approaches to its treatment (Abstr.). Inc. J. Radial. Oncol. Biol. Phys. lZ(Suppl. 1): 128, 1986.
26.
16. Kottmeir, H., Kolstad, P. (Eds.): Annual Reporl on the Re-
Markman, M., Weiss, R., Howell, S.B., Lucas, W.E.: The intraoperative intraperitoneal administration of CIS-plati- num: A case report. Cancer Drug Deliv. 2: 87-90, 1985. Martinez, A., Schray, M., Podratz, K., Stanhope, R., Schomberg, P., Williams, T., Malkasian, G.: Postoperative whole abdomino-pelvic irradiation for patients with high risk endometrial cancer (Abstr.). Int. J. Radial. Oncol. Biol. Phys. ll(Supp1. 1): 171-172, 1985. Mould, R.F.: Cancer Statistics. Bristol, Adam Hilger Ltd. 1985, pp. 165-179. Roboz, J., Jacobs, H.J., Holland, J.F., Deppe, G., Cohen, C.J.: lntraperitoneal infusion of doxorubicin in the treat- ment ofgynecologic carcinomas. Med. Ped. Oncol. 9: 245- 248, 1981. Rosenshein, N.B.: Radioisotopes in the treatment of ovar- ian cancer. Obstet. Gynecol. 10: 279-280, 1983. Soper, J.T., Creasman, W.T., Pearson, D.L., Sullivan, D.C., Vergado, F., Johnston, W.W.: lntraperitoneal chro- mic phosphate P 32 suspension therapy of malignant cy- tology in endometrial carcinoma. Am. J. Obstet. 153: 19 I- 196, 1985. Szpak, C.A., Creasman. W.T., Vollmer, R.T., Johnston, W.W.: Prognostic value of cytologic examination of peri- toneal washings in patients with endometrial carcinoma. Acta. Cytol. 25: 640-646, 198 1. Varia, M., Rosenman, J., Venkatraman, S., Askin, F., Fowler, W., Walton, L., Halle, J., Currie, J.: Intraperito- neal chromic phosphate therapy following second-look laparotomy for ovarian cancer. Cancer61: 9 19-927, 1988. Yazigi, R., Piver, M.S., Blumenson, L.: Malignant perito- neal cytology as a prognostic indicator in stage I endome- trial cancer. Obstet. Gyn. 62: 359-362, 1983.