Embed Size (px)
Citation preview

Peritoneal Dialysis Access Current Recommendations
Reusz GS
First Department of Pediatrics
Semmelweis University, Budapest

Etiology of RRT
2 Data from US Renal Data System, 2014.

Modality of first RRT according to age
3
Data from US Renal Data Systems, 2008.

2016.11.11. 4
Patient with VACTERL
association

2014

Technique – and beyond?
PD as a complex procedure
• Detailed discussion with family before decision • Inspection of the patient’s physical and social
environment • Technical issues of catheter placement and care • Comprehensive PD course and timed re-
education for caregivers and the patient • Periodical courses for nurses and staff
(recapitulation and eventual novel guide-lines)

GUIDELINE 1 – TRAINING
1.1 We suggest that PD training be performed by an experienced PD nurse with pediatric training, using a formalized teaching program that has clear objectives and criteria, and that incorporates adult-learning principles (2C).
1.2 We suggest that retraining be provided to all caregivers periodically. We also suggest that re-evaluation of the PD technique be conducted after development of a peritonitis episode (2C).

Content of training curriculum
1. Theory
Functions of the kidney
Overview of PD (osmosis and diffusion)
Fluid balance (relate to weight and blood pressure)
Use of different strengths and types of dialysis fluid
Prevention of infection
2. Practical
Handwashing
Aseptic technique
Dialysis therapy—machine or manual exchanges (step-by-step procedure guide)
Emergency measures for contamination
Troubleshooting or problem-solving alarms on the cycler
Blood pressure monitoring and recording
Weight monitoring and recording
Exit-site care
3. Complications
Signs, symptoms, and treatment of peritonitis
Signs, symptoms, and treatment of exit-site and tunnel infections
Drain problems (constipation, fibrin)
Fluid balance (hypertension, hypotension)
Other (leaks, pain)
4. Other
Record-keeping
Administration of medications
Dietary management
Ordering and managing supplies
Managing life with PD (school, sport, holidays)
Contacting the hospital, making clinic visits, having home visits

Content of training curriculum
1. Theory
Functions of the kidney
Overview of PD (osmosis and diffusion)
Fluid balance (relate to weight and blood pressure)
Use of different strengths and types of dialysis fluid
Prevention of infection
2. Practical
Handwashing
Aseptic technique
Dialysis therapy—machine or manual exchanges (step-by-step procedure guide)
Emergency measures for contamination
Troubleshooting or problem-solving alarms on the cycler
Blood pressure monitoring and recording
Weight monitoring and recording
Exit-site care
3. Complications
Signs, symptoms, and treatment of peritonitis
Signs, symptoms, and treatment of exit-site and tunnel infections
Drain problems (constipation, fibrin)
Fluid balance (hypertension, hypotension)
Other (leaks, pain)
4. Other
Record-keeping
Administration of medications
Dietary management
Ordering and managing supplies
Managing life with PD (school, sport, holidays)
Contacting the hospital, making clinic visits, having home visits

Training • Peritonitis rates significantly lower in PD programs with
longer training • Having nursing experience does not mean teaching exercise
• Need for continuous education
• Retraining periodically and after peritonitis episodes
• Root-cause analysis to establish the causes of ES infection or peritonitis • Specific examples
• Handwashing
• Domestic animals
Holloway Met al. Pediatric peritoneal dialysis training: characteristics and impact on peritonitis rates. Perit Dial Int 2001; 21:401–4. Gunasekara WD, et al: Specialist pediatric dialysis nursing improves outcomes in children on chronic peritoneal dialysis. Pediatr Nephrol 2010; 25:2141–7.

http://www.chp.gov.hk/en/wapdf/30879/1.html

GUIDELINE 2 – CATHETER TYPE AND PLACEMENT
2.1 We suggest the use of a double-cuff Tenckhoff catheter with a downward or lateral subcutaneous tunnel configuration that is placed by a surgeon or nephrologist experienced in PD catheter placement (2B).
• Nephrol Dial Transplant 1997; 12:2664–6 • Am Soc Nephrol 2004; 15:2735–46. • Clin J Am Soc Nephrol 2010; 5:1041–6. • Etc…

Why is design and surgical technique important?
• Reduce risk for catheter-related complications
• Reduce risk for transfer to HD
Mechanical Complications
• Leaks
• Omental entrapment
Infectious Complications
• Exit-Site
• Tunnel
• Peritonitis


Catheter design issues • A peritoneal dialysis catheter has three functional
segments:
• The external segment – the part that is outside the body
• The tunneled segment – the part that is tunneled through the subcutaneous tissue and the rectus muscle
• The intra-peritoneal segment – the part inside the peritoneal cavity

Catheter types

Key technical issues at placement
• Pre-operative antibiotic prophylaxis
• Location of the catheter tip
• Placement of the deep cuff
• Placement of the exit site: • Location on the abdominal wall
• Direction – downward, lateral, or upward pointing?
• Location of superficial cuff relative to exit site

Importance of careful planning

Principles in Fashioning Exit Site • Should be away from belt-lines, skinfolds
• Should be clearly visible to the patient to perform daily exit site care • Inserted through the abdominal wall with
least tubing stress • The smallest skin incisure • Avoid sutures at the ES
•About 2.5 cm from the superficial cuff •Generally achieved when planned with
patient upright, rather than supine

Where is it relative to the belt-line? determine before patient is sedated

How Should PD Catheters Be Placed? • Not the youngest resident on duty at the end of the daily
surgical program • skillfully by and old roadster
• Methods of placement of PD catheters: • Percutaneous, blind (with/without fluroscopy)
• Direct visualization: • Open, surgical dissection • Laparoscopic (general /or local/ anesthesia /adults/)
• Who should place PD catheters? • Whoever places them, depends on local expertise:
• Surgeons • Nephrologists, including interventional nephrologists in standalone access
centers
• Interventional radiologists

No Sutures or Staples At Exit Site!

Practical measures
• Showering or antiseptic bathing • Perioperative bowel preparation
• Double-cuff, downward directed exit-site – better annualized peritoitis rate and longer time to first peritonitis
• Single cuff catheter >13x increased risk of G- peritonitis
• Straight vs coiled: increased rate of post peritonitis technical failure
• Application of fibrin glue to peritoneal cuff suture to prevent early leakage
Nephrol Dial Transplant 1997; 12:2664–6 Am Soc Nephrol 2004; 15:2735–46. Clin J Am Soc Nephrol 2010; 5:1041–6. Etc…

Timing of Placement of PD Access
• General principle: • Wait two weeks from the placement of PD catheter before
starting PD (“teach-in” period)
• Initial and periodic flushing during break-in
• Break-in period may be longer if wound healing impaired: • Post-transplant failure OR
• Patient on immunosuppressives
• Implant catheter too early: • prolonged need for catheter care before dialysis started
• incremental dialysis?
• Implant catheter too late: • Need early “break-in”

Early Break-In
• Start PD (“break-in”) within 24 hours of placement of PD catheter
•Risks: Peri-catheter leak • Solution: Low-volume, supine dialysis (15-10
ml/kg dwell volume x 6-10 exchanges) • Challenges:
• Inadequate dialysis
• Place where dialysis is performed – home, hospital, or dialysis clinic

Conclusions
• Placement technique and skill of operator is among the most important determinant of catheter outcomes
• Careful planning of exit site placement very important
• Early break-in possible, if needed
• Advanced laparoscopy has advantages, if available
• Aim: to minimize/eliminate need for temporary HD

GUIDELINE 2 – CATHETER TYPE AND PLACEMENT (cont)
• 2.2 We recommend that perioperative antibiotic
prophylaxis be used within 60 minutes before the incision for PD catheter placement to reduce the incidence of early-onset peritonitis (1A).

Perioperative antibiotic prophylaxis • Cochrane systematic review (2004) (355 patients, 4 trials):
• perioperative iv antibiotic decreased the risk of early peritonitis [ (RR) 0.35, 95% CI: 0.15–0.80]
• but not the risk of ESI and tunnel infection (RR 0.32, 95% CI: 0.02–4.81).
• ISPD guidelines (2011): vancomycin prophylaxis at catheter placement but weigh the risk of the emergence of resistant organisms
• UK guidelines recommend antibiotic prophylaxis perioperatively but do not stipulate which antibiotic should be used. (VCM resistant enterococcus)
• The Kidney Health Australia (KHA-CARI) guidelines: iv. antibiotic prophylaxis at catheter insertion: vancomycin, cephalosporins or gentamicin are suitable.
• ISPD pediatric guide-line (2012): reiterates the previous guide-lines adding that choice of the antibiotic should take center-specific susceptibility and public health concerns into consideration.
• To summarize, a single dose of intravenous antibiotic given at the time of catheter insertion has been shown to decrease the risk of early peritonitis

GUIDELINE 3 – EARLY EXIT-SITE CARE
3.1 We recommend once-weekly sterile dressing changes to the exit site, performed by experienced health personnel according to a standardized protocol, until the exit site is well healed (2B)
3.2 We recommend catheter immobilization to prevent trauma to the exit-site and to optimize early healing (1B).

The aims of early PD exit-site (ES) care after implantation are
• To prevent bacterial colonization during the healing phase,
• To minimize multiplication of bacteria
• to prevent local trauma through catheter mobilization
• Avoid dressing changes during the first postoperative week, continue once-weekly changes until the ES is well healed. • With each change, the ES may be contaminated even if aseptic
technique is followed
• sterile technique until the site is healed: “when the skin around the exit site looks normal without gaping”
• more frequent changes only if excessive drainage at the exit site or if excessive sweating causes wetness

Early exit-site (ES) care after implantation aseptic technique, using sterile gloves and face mask:
• ES cleaned with a nonirritating, nontoxic agent, clean
around the ES with sterile gauze soaked in sterile cleansing solution • hydrogen peroxide and povidone are cytotoxic • chlorhexidine, normal saline suitable
• ES culture if signs of colonization or infection
• Crusts should not be forcibly removed.
• Use another piece of soaked gauze to clean the tubing.
Start from the exit site and work up the tubing away from the body.
• Use gauze to gently pat the exit site dry, ensuring that it is completely dry.

Early exit-site (ES) care after implantation aseptic technique, using sterile gloves and face mask:
• Application of a topical antibiotic
• Allow the catheter to fall into its natural position from the ES
• Several layers of sterile gauze dressing over the thoroughly dried exit site • to wick away any drainage and to keep the site dry
• Don’t use semipermeable and occlusive dressings • pooling at the exit site of any drainage, provides a good medium
for bacterial growth
• Immobilize the catheter below the ES dressing, anchoring the tube to restrict movement.
• Don’t submerge in water (shower, bathing) until complete healing

GUIDELINE 4 – CHRONIC EXIT-SITE CARE
4.1 We recommend cleansing the exit site with a sterile antiseptic solution and sterile gauze (1C)
4.2 Each program should evaluate the type, frequency, and resistance patterns of organisms causing ESIs and institute a center-specific protocol to diminish such risk (not graded)
4.3 We suggest that a topical antibiotic be applied to the peritoneal catheter exit site as a component of chronic exit-site care (2B).


Healthy exit site without crust and without inflammation
Exit site crust formation and minimal inflammation


Local practice • European Best Practice Guidelines for PD: because of
epithelial toxicity, povidone iodine and hydrogen peroxide should be avoided, especially during the early healing phase
• Chronic exit-site care: • daily in 93% of centers in America and Asia, • in 64% of centers in eastern Europe and Turkey, • but in only 8% of western European centers.
• Large regional differences also exist with respect to the choice of an exit-site cleansing agent and topical antibiotic. • Mupirocin effective against staphylococcus aureus • Gentamycin effective against pseudomonas & staphylococcus, but
possibility of emerging resistant bacteria • Frequency?
• Daily, 3x daily, once monthly
• Intranasal? Local?

Catheter cuff extrusion
• Catheter cuff erodes the skin at the outer abdominal wall
• Secondary to superficial placement or exit site infection with local decubitus
• Incidence up to 7% independentily of catheter type or method of placement
• Treatment: • If no infection: trim the cuff under sterile conditions
• If infected: remove catheter

Where Is It Relative To Superficial Cuff? • Exit site ahould be about 2.5 cm from the superficial cuff

2016.11.11. 40
Exit-site infections

GUIDELINE 7 – OSTOMY PATIENTS 7.1 The PD catheter ES should be placed as far as possible
from an ostomy site (not graded).
7.2 Gastrostomy placement should preferentially take place either before or at the time of PD catheter placement (1C).
7.3 We recommend the preferential use of an open surgical procedure for gastrostomy placement in patients who are already receiving PD. In patients not yet receiving PD, gastrostomy placement can be performed by either open surgical technique or laparoscopically (1C).
7.4 We suggest administration of prophylactic antibiotic and antifungal therapy during gastrostomy placement (2C).
7.5 We suggest withholding PD for 1 or more days after gastrostomy placement (2D).

11/11/2016 42
We are already there!
I’m feeling the first
rain drops...

Adequacy of dialysis
Reusz GS
First Department of Pediatrics
Semmelweis University, Budapest

Adequacy of
solute remouval Adequacy of
ultrafiltration Well-being of
the patient
Nutrition
Growth
Aim:
• to decrease morbidity and mortality and
• to ensure an acceptable QOL
• By delivering an optimum dialysis dose
MAJOR GOALS FOR PD ARE
Flessner M. Contrib Nephrol 163:7, 2009

Outline
1. Principles of water and solute transport
2. Individual variability of transport properties
3. „Dosing” goals in dialysis
4. Individual techniques for the individual patient to achieve dialysis adequacy
Flessner M. Contrib Nephrol 163:7, 2009

Outline
1. Principles of water and solute transport
2. Individual variability of transport properties
3. „Dosing” goals in dialysis
4. Individual techniques for the individual patient to achieve dialysis adequacy
Flessner M. Contrib Nephrol 163:7, 2009

Structure of the Peritoneal Membrane
• Serous membrane lining the abdominal cavity • Single layer of
mesothelial cells supported by connective tissue
• Capillaries, lymphatics, and nerves are found within connective tissue
Flessner M. Contrib Nephrol 163:7, 2009 Image adapted from Baxter

http://www.kbdialysis.com/peritoneal-dialysis/

The driving forces of equilibration
diffusion: solutes
blood abdominal space
(P) (D)
osmosis: glucose + H2O
blood abdominal
space
H2O (Do)
(D)

Flessner M. Contrib Nephrol 163:7, 2009

Distribution of AQP1 in the peritoneal membrane
AQP1 in the endothelium lining peritoneal capillaries, venules, and small veins.
esothelium
AQP1 in the plasma membrane of capillary endothelial cells.
Ni J et al; Kidney Int 69: 1518–1525, 2006

Role of AQP1 in the peritoneal membrane
mice lacking AQP1 show a complete loss of sodium sieving and significantly lower initial UF rates
Ni J et al; Kidney Int 69: 1518–1525, 2006

Dialysate-to-plasma concentration ratios for urea, creatinine, inulin, and protein
Popovich RP et al: Ann Intern Med 1978; 88:449.

Intr
ape
rito
ne
al vo
lum
e,
ml
0 100 200 300 400 500 600 700
2800 2600 2400
2200 2000 1800
1600
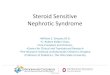
4.25% Dextrose 1.5% Dextrose
Time, min
Ultrafiltration with Different Strengths of Dialysate

Sodium mmol/L
135 130 125 120 115 110
0 30 60 90 120 150 180 210 240
Dwell time (min)
2.5% D 4.25% D
Heimburger et al. Kid Int 38: 495, 1990
Changes in dialysate sodium during dwell in function
of the dialysate glucose concentration
(Sodium sieving)

Outline
1. Principles of water and solute transport
2. Individual variability of transport properties
3. „Dosing” goals in dialysis
4. Individual techniques for the individual patient to achieve dialysis adequacy

Standard PET test A tool to characterize the transport properties
The tool to evaluate the
• individual properties of the peritoneal membrane
• adequacy of dialysis
Timing:
• 4 weeks after catheter insertion
• every 6 month thereafter
• after peritonitis (4-6 weeks following the acute phase)
• In the case of clinical signs of inadequacy

The standard PET test
• standardized parameters
– Long overnight SINGLE exchange of usual volume and solution
– FULL drain and very fast instillation of 1000-1100 ml/m2 of 2.5% standard PD fluid
– 4 hour test time with
• PD fluid samples drawn at Time Zero/ 120 and 240 minutes [Urea/ Creatinine/ Glucose + Na or PO4]
• Blood sample drawn at Time 120 and 240 minutes

D/P ratios
From dialysate and serum values calculate a fractional amount of “solute” that appeared the dialysate
– “D/P” ratio or Dialysate/Plasma concentration
– D/P Urea and D/P Creatinine markers of clearance characteristics of membrane
– “D/D0” Glucose a marker of how much glucose absorbed over 0 - 240 minutes – D/P Na and PO4 can also be used, although not part of ‘Classic’ PET... ‘Classic’ PET Test Methodology

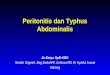
Changes in dialysate glucose and creatinine as a proportion of original dialysate concentration (DO) or
plasma creatinine (P) respectively
Twardowski ZJ.. Blood Purif 1989; 7:95.

PET transport characteristics 2
type D/P (4h) D/Do (4h)
Low tr. 0,34 – 0,49 0,61 – 0,48
Avg low tr 0,50 – 0,64 0,37 – 0,27
Avg high tr 0,65 – 0,80 0,38 – 0,25
High tr. 0,81 – 1,03 0,26 – 0,12

PET results for children
Warady B et al: JASN. 1996; 7:2385-2391

Peritoneal equilibration test in rapid versus slow transporters
Twardowsky ZJ. ASAIO Trans 1990; 36:8.

Optimal dwell time
• Better solute
clearence • Improved ultrafiltration
Dwell time (h)
cre
ati
nin
e c
lea
ran
ce
pe
r e
xc
ha
ng
e (L
)
0
1
2
0 2 4 6 8
Fast transporter
Slow transporter
Optimal dwell time

PET test
allows to plan
dialysis dose and ultrafiltration
Parameters to be determined
- Fluid volume
- dwell time PD type
- number of exchanges
- concentration of glucose

Outline
1. Principles of water and solute transport
2. Individual variability of transport properties
3. „Dosing” goals in dialysis
4. Individual techniques for the individual patient to achieve dialysis adequacy
Flessner M. Contrib Nephrol 163:7, 2009

Adequacy = Quantity of Clearance
„Deliver” a safe quantity of RRT – For the maximum well-being of the patient (CV, QOL) – Time consuming, costs – Deterioration of the peritoneal membreane by the procedure and
the complications
Measured as clearence: UxV/P Quantity of clearance = clearance of small, easily measureable molecules A measure of ‘uremia’ or toxin accumulation Different approaches – UREA reported as Weekly Kt/Vurea – CREATININE reported as Weekly Creatinine Clearance

Kt/Vurea = Fractional Clearance of Body Urea – mathematical “construct” – unitless
urea clearence (Kurea)
renal residual (Kr urea) U x V peritoneal (Kp urea)
P
urine urea (mmol/l) x volume (l) dializate urea x volume (l) plasma urea (mmol/l) plasma urea Weekly KT/Vurea (Kr urea+Kp urea) x t (7 days) volume of urea distribution (=TBW) (l)
“V” urea = volume of distribution for Urea = TBW V: nomograms or formulas
Adequacy defined to reach a Kt/V target

Anthropometric table to predict of Total Body Water (TBW) in children
J Am Soc Nephrol 17: 285–293, 2006.
6.3

The “V” Formula with Ht in cm and Wt in kg
Boys: TBW = 20.75 x BSA - 3.88 Girls: TBW = 16.96 x BSA - 1.57 BSA = HxW/3600 Alternatively: use Gender-Specific Nomograms Extremes not included here – ie very obese or malnourished Anthropometric prediction of total body water in children who are on pediatric peritoneal dialysis. Morgenstern BZ, Wühl E, Nair KS, Warady BA, Schaefer F. J Am Soc Nephrol. 2006 Jan;17(1):285-93.

Example
100 cm 20 kg Female BSA = 0.74 m2 she voids 400 ml/day TOTAL dialysate drained/day 800 ml/BSA ~ 600 ml 5 exchanges / day = 3000 ml net ultrafiltration = 350 ml total daily volume drained = 3350 ml Urine urea 9 mmol/L alternatively: 9 plasma urea 17 mmol/L 17 dialysate urea 11 mmol/L 13 Vd_urea (TBW = 16.96 x BSA - 1.57) = 10,9 Weekly Kt/V = 7*[(0.4 x 9/17) + (3.35 x 11/17)] /10,9 = 7*[(0.21 +2.17)/10.9] = 7*[0.42] Weekly Kt/V_urea = 1.53 1.78

http://www.kt-v.net/

PD Prescription Targets
Dosing targets in adults from studies KT/V with morbidity/mortality
– No large scale, prospective studies in children for “adequate” dose of PD
“EXPERT” opinion:
– The minimal delivered dose of total (peritoneal and kidney) small-solute clearance should be a Kt/ Vurea of at least 1.8/wk.

Dialysis dose and survival
Perit Dial Int 1996; 16:457.
J Am Soc Nephrol 1996; 7:198

Outline
1. Principles of water and solute transport
2. Individual variability of transport properties
3. „Dosing” goals in dialysis
4. Individual techniques for the individual patient to achieve dialysis adequacy

Anatomic and physiologic principles for PD prescription
• Peritoneal membrane surface area is proportional to body surface area independent of patient age
• Scale peritoneal dialysis exchange volume to body surface area (and not to weight)

PD Prescription- Fill Volume
Individual differences : • post nephrectomy ARPKD, • nephrotic syndrome etc Flessner M. Contrib Nephrol 163:7, 2009

Dwell volume and pressure
• Excess Volumes may lead to – Raised Intraperitoneal Pressures
– Loss of UF [‘Lymphatics’]
– Pain
– Risk of hernia
– Risk of hydrothorax
– Risk of breathing problems
• Position matters
• Supine<Stand<Sit Maximum ~ 15-18 cmH20

2016.11.11. 79
Pleural effusion

2016.11.11. 80
Hernia inguinalis

High transport
– A larger effective peritoneal surface area
– A higher intrinsic membrane permeability (for the rapid equilibration of small solutes including creatinine and urea
may be the result of structural or functional alterations of the peritoneum
• High transporters: rapid absorption of glucose from the dialysate
– Loss of the osmotic gradient
– Decrease in ultrafiltration capacity
– Greater systemic exposure to glucose
– Efficient clearance.

Low transporters • Achieving ultrafiltration goals
• Difficulty with clearance targets.
Modality • High transporters: frequent short dwells (APD)
maximizing ultrafiltration
• low transporters: longer dwell times
(CAPD) to maximize clearances

Survival on PD according to
transport category
Kidney Int Suppl 2006; 70:S76.


Major Determinants of PD Modality
Choice
• Transport characteristics of the individual patient’s peritoneal Membrane
• Lifestyle
• Financial
• Center preference
• Geography
Flessner M. Contrib Nephrol 163:7, 2009

Infant with with autosomal recessive polycystic kidney disease
Pulmonary hypoplasia in ARPKD
Büscher R et al; Pediatr Nephrol, 2013; DOI 10.1007/s00467-013-2634-1

Case 1
• Patient with ARPKD, • Born at 34 weeks of gestations BW: 2600 g • With signs of IUGR • Difficulties during perinatal adaptation
– Hypoxia, hypoventillation due tu lung hypoplasia and enormous kidneys
– Hypoglycemic episodes – Ventillated for 2 weeks
• Clinical course – Feeding difficulties – Needs parenteral nutrition – Repeated hematogenic infections through CVL

Case 1
• CKD 2-3
– CKD Creatinine 80-110 umol/l depending on hydration and infection
– Diuresis 7-800 ml/day (polyuric)
– Acidosis corrected by NaHCO3
• At the age of 4 month still weighting 3800 g

Case 1
• What should be done? a) Remove one kidney to make more place in the
abdominal cavity b) Bilateral nephrectomy and dialysis?
a) HD trough CVL? b) PD?
One kidney was removed • No improvement of bowel movement • Still on TPN • Repeated infections • Failure to thrive

Case 1
• What to do next? a) Place PD catheter and after break-in remove the second
kidney? b) Place a HD catheter and remove the kidney and continue
HD c) Place a temporary HD catheter, remove the kidney, place
a PD catether
• The second kidney was removed, a PD catheter was placed and HD was initiated through a CV catether,
• 3 weeks later PD was initiated • Enteral feeding could be introduced • Transplanted (living related) at the age of 2