Embed Size (px)
Citation preview
Author's Accepted Manuscript
Peri-Prosthetic Femoral Fractures: What to Do, Whatto Do?
John R. Martin M.D., Robert T. Trousdale M.D.
PII: S1045-4527(14)00079-0DOI: http://dx.doi.org/10.1053/j.sart.2014.04.010Reference: YSART50599
To appear in:Semin Arthro
Cite this article as: John R. Martin M.D., Robert T. Trousdale M.D., Peri-ProstheticFemoral Fractures: What to Do, What to Do?,Semin Arthro , http://dx.doi.org/10.1053/j.sart.2014.04.010
This is a PDF file of an unedited manuscript that has been accepted for publication. As aservice to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting galley proofbefore it is published in its final citable form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers that applyto the journal pertain.
www.elsevier.com/locate/enganabound
1
Peri-Prosthetic Femoral Fractures: What to Do, What to Do? Authors: John R. Martin M.D. (Medical Doctor) Mayo Clinic Department of Orthopedic Surgery [email protected] Robert T. Trousdale M.D. (Medical Doctor) Mayo Clinic Department of Orthopedic Surgery 200 First St. SW Rochester, MN 55905 Phone: (507) 284-2511 [email protected] Abstract:
Post-operative periprosthetic fractures have an incidence of 1.1%(Berry 1999). The peri-prosthetic fracture is
commonly classified by the location of the fracture. The most frequently utilized fracture classification
categorizes patients by the location of the fracture including: peritrochanteric, around the stem, or distal to the
femoral implant. Additional considerations incorporated in this classification include femoral implant stability
and host bone status. We will review the different treatment modalities for each fracture type with consideration
given to stem stability and host bone status.
Introduction:
Fracture of the femur after total hip replacement is an uncommon mechanism of failure and the
incidence has been estimated to be around 1.1%(Berry 1999). There have been several studies that have reviewed
peri-prosthetic femoral fractures. Treatment recommendations for these fractures are based on several factors
that must all be considered prior to surgery. Anatomic considerations include the location of the fracture
including fractures located at the level of the lesser or greater trochanter, fractures around the level of the stem,
and finally fractures distal to the stem. Stem stability is the next consideration for patients that have a peri-
prosthetic fracture. Finally, the host bone status will need to be considered prior to proceeding with treatment.
Peritrochanteric fractures
2
The incidence of greater trochanteric peri-prosthetic fractures have been estimated to be as high as 3%
with some of these occurring intraoperatively and post-operatively(Brun, 2013 #4}. According to the Vancouver
classification, peritrochanteric fractures are denoted as type A fractures with AG being greater trochanteric and
AL being lesser trochanteric fractures(Duncan and Masri 1995). The treatment for peritrochanteric fractures is dependent
on stability of the stem, fracture displacement, and the amount of bone loss. In patients with a stable stem,
minimal fracture displacement, and negligible osteolysis, non-operative treatment is indicated(Berry 2002). If
patients have a markedly displaced peritrochanteric fracture or if the fracture is associated with significant
osteolysis then surgical intervention is warranted.
Displaced fractures in the setting of minimal osteolysis warrant open reduction and internal fixation of
the fracture. However, if there is a displaced fracture in the setting of osteolysis, the amount of displacement
will factor into the surgical recommendations. Occasionally, if there is minimal displacement, it is often
possible to treat the trochanteric fracture non-operatively. After the fracture is healed, the osteolysis generator
can then be revised with bone grafting of the trochanter as needed. If the fracture is greatly displaced and there
is no lysis, these fractures can be managed with a construct that holds the trochanteric fragment in a reduced
position. When revising patients with osteolysis in the setting of a trochanteric fracture, if the trochanter is very
thin, care should be utilized to not further disrupt the abductor mechanism.
The following are two separate examples of peritrochanteric periprosthetic fractures. The first case is a
62 year old male with an uncemented femoral component with a nondisplaced greater trochanteric fracture. The
above x-rays show minimal osteolysis and therefore the patient was treated non-operatively. The patient
required Tylenol for pain control and has no issues healing the injury. Image I. The next case is slightly more
complex and involves a 60 year old female who has a nondisplaced right greater trochanteric fracture with
severe osteolysis. We allowed the greater trochanter time to heal and then revised the acetabulum. During the
revision surgery, allograft bone chips were impacted into areas of osteolysis around the greater trochanter.
Image II.
Fractures Around the Stem
3
Fractures about the stem are categorized according to the Vancouver classification as Type B fractures.
They are further categorized as B1 if the stem is stable, B2 if the stem is loose, or B3 if the stem is loose and the
proximal bone is non supportive(Duncan and Masri 1995). Fractures around the stem are by far the most common
periprosthetic femur fracture associated with total hip replacement(Berry 1999). The treatment algorithm is almost
always surgical intervention in this patient population because there is a high incidence of malunion and
nonunion with non-operative management(Bethea, DeAndrade et al. 1982). Additionally, non-operative management
would require immobilization and/or bedrest which would not be an attractive option in this elderly patient
population.
B1 Fractures
B1 fractures are fractures about the stem with no loosening of the femoral component. These fractures
are most commonly treated by open reduction and internal fixation with a variety of fixation techniques. One of
the unique technical points when treating these fractures is how to obtain proximal fixation. Distal fixation can
be easily achieved with several bicortical screws below the level of the stem. However, the proximal fragment
is often much shorter than the distal fragment and the stem often precludes the use of bicortical screws. The
available options for treatment include either nonlocking or locking plates with unicortical screws and or
cerclage wires, strut allograft, or a combination of these two techniques(Buttaro, Farfalli et al. 2007). In the setting of a
cemented component, disruption of the cement mantle when placing screws should be avoided to prevent
loosening of the otherwise stable component.
The following example is a 72 year old female with an uncemented proximally coated femoral stem.
The stem appears stable radiographically, and was confirmed at the time of surgery. The patient underwent an
open reduction internal fixation with a locking plate. We utilized bicortical nonlocking screws distally.
Proximally there is a combination of unicortical locking screws and cerclage wires to bolster fixation in this
area. The patient did great after surgery and was discharged four days post-operatively. The final x-rays at two
years post-operative show complete union of the fracture, continued stem stability, and no hardware failure.
Image III.
B2 Fractures
4
Periprosthetic femoral fractures with loosening of the stem are treated very differently than the B1
fracture where the stem is stable. These fractures most commonly require revision of the femoral component in
order to obtain a stable and well-functioning hip. Revision in the setting of fracture is associated with a
relatively high risk of both complications (18%) and reoperations (23%) according to the Swedish Joint
Registry(Lindahl, Malchau et al. 2005). Treatment options for this fracture pattern include revision to a fully porous
coated diaphyseal fixation femoral stem or to revision to a fluted tapered modular femoral stem (Lewallen and Berry
1998).
The goals of revision surgery include a stable femoral component, healing of the fracture, a quick return
to pre-injury functional level while minimizing complications associated with the injury and the surgery.
Surgical considerations include obtaining adequate exposure, avoiding fracture propagation and properly
preparing the remaining bone stock for the new hip prosthesis. We commonly utilize an ETO for exposure and
removal of the femoral component. This allows excellent visualization of both the femoral and acetabular
components and allows the stem to be removed easily. Prior to preparing the femoral canal a cerclage wire
should be placed around the femur just distal to the level of the fracture to prevent fracture propagation during
preparation of the femoral canal. After the stem is placed, the ETO can be repaired with cerclage wires as well.
Levine et. al. found a 100% union rate of the ETO and radiographic fracture union approximately 13.1 weeks
post-operatively utilizing this same strategy(Levine, Della Valle et al. 2008).
A couple of cases that illustrate the above principles are shown below. This is an 71 y.o. male with an
uncemented stem with a type B2 fracture. The stem is clearly loose on the pre-operative photographs. An ETO
was utilized for exposure on this patient. A fully coated porous stem was inserted at the time of revision
surgery. The ETO and fracture were held together with wires and the patient united approximately 3 months
post-operatively. Image IV. The patient has an excellent Harris Hip Score and has fully returned to his previous
functional activity level. Our current workhorse for implants is a fluted tapered modular stem, as seen in the
following case. These stems give great axial and rotational stability and therefore proximal femur fixation is not
as important for construct stability. The following patient had a transfemoral approach to the hip. The soft
tissues around the fracture fragments were not violated. A fluted tapered modular stem was inserted and served
5
as a scaffold for fixation of the proximal fragments. Image V. The patient was able to WBAT following surgery
and the post-operative radiographs once again show that the fracture has united and the stem is stable.
B3 Fractures
Periprosthetic fractures in which the stem is loose and there is significant osteolysis represent the most
challenging periprosthetic reconstruction. Similar to type B2 fractures, the complication rates and revision rates
are high(Lindahl, Malchau et al. 2005). Proximal fixation is nonexistent in this patient population due to the significant
osteolysis or severe comminution of the injury itself. Surgical options for this patient population include options
that replace the proximal bone loss such as allograft prosthetic composite or proximal femoral tumor prostheses
or implants that are rotationally and axially stable such as fluted tapered modular implants(Levine, Della Valle et al. 2008).
Both methods of fixation are commonly employed in managing this patient population.
The following patient is a good example of a patient with a B3 fracture. There is significant proximal
bone loss. The stem is grossly loose. A posterior approach with an ETO was utilized. We specifically avoided
stripping the soft tissues off of the proximal bone. A cerclage wire was placed just distal to the fracture site
before preparing for the femoral stem. A fluted tapered modular stem was utilized to bypass the site of the
fracture by several cortical diameters. The proximal bone was then reconstructed to envelope the prosthesis and
was then fixed with wires. Image VI. At final follow-up much of the proximal bone has reconstituted, the stem
is stable with no evidence of loosening, and the patient has returned to their previous functional level.
Fractures distal to the stem
According to the Vancouver classification, fractures distal to the stem of the femoral component are
categorized at type C fractures(Duncan and Masri 1995). Fractures distal to the stem behave similar to midshaft femoral
fractures in patients that do not have a prosthesis. For this reason they are often treated in a similar fashion.
Most surgeons advocate treatment with open reduction internal fixation with plate or wire fixation or with a
retrograde intramedullary device(Berry 2002). Depending on the proximity of the fracture to the stem and the length
of the plate used for fixation, cerclage wires and unicortical screws are typically required for fixation overlaps
the femoral stem, similar to treatment with B1 fractures. If the patient has an ipsilateral total knee replacement, a
laterally placed locking plate construct with or without additional fixation with wires should be utilized. Finally,
6
when utilizing a retrograde intramedullary device, a stress riser can occur between the femoral stem of the
intramedullary nail and the total hip stem. This may lead to subsequent fracture between the two constructs and
can be avoided with the use of a plate construct.
Our final example is an 73 y.o. male who fell on ice and sustained a fracture well below a solidly
ingrown total hip replacement. The patient had a well-functioning total hip replacement prior to the injury. The
fracture was reduced and a lateral locking plate was placed with minimal disruption of the soft tissues
surrounding the fracture. Screws were inserted percutaneously with the use of an external guide and
fluoroscopy. Intraoperatively, rotational alignment was assessed by comparing the rotation of the knee and
ankle of the operative leg to the contralateral leg. Additionally, we assesed that we have restored the
mechanical axis of the knee by ensuring that an alignment rod held from the center of the femoral head to the
center of the ankle passes through the center of the knee. This is most commonly confirmed utilizing
fluoroscopy. The patient did well after the surgery, he was maintained on PWB for 4 weeks post-operatively.
Our final x-rays show excellent restoration of the mechanical axis, union of the fracture, and the stem remains
well fixed. Image VII.
Summary:
Post-operative periprosthetic fractures around total hip arthroplasties are a unique mechanism of failure.
It is likely that there will be increasing numbers of these fracture patterns with rising numbers of total hip
arthroplasties being performed annually. The treatment of these fractures is not complex but requires evaluating
i) the location of the fracture (peritrochanteric, around the stem, or distal) ii) whether the stem is loose and iii)
the status of the host bone. Our preferred method of treatment for Type A fractures is most commonly non-
operative management. For type B1 fractures we utilize a locking plate with unicortical screws and cerclage
wires, B2 and B3 fractures we prefer a fluted tapered modular femoral stem. Finally, for type C fractures a
lateral locking plate is our most common treatment. Each patient offers unique reconstructive challenges and
this algorithm must be adjusted to meet the specific demands on a case by case basis.
7
Bibliography:
Berry, D. J. (1999). "Epidemiology: hip and knee." The Orthopedic clinics of North America 30(2): 183-190. Berry, D. J. (2002). "Management of periprosthetic fractures: the hip." The Journal of arthroplasty 17(4 Suppl 1): 11-13. Bethea, J. S., 3rd, J. R. DeAndrade, et al. (1982). "Proximal femoral fractures following total hip arthroplasty." Clinical orthopaedics and related research(170): 95-106. Buttaro, M. A., G. Farfalli, et al. (2007). "Locking compression plate fixation of Vancouver type-B1 periprosthetic femoral fractures." The Journal of bone and joint surgery. American volume 89(9): 1964-1969. Duncan, C. P. and B. A. Masri (1995). "Fractures of the femur after hip replacement." Instructional course lectures 44: 293-304. Levine, B. R., C. J. Della Valle, et al. (2008). "Extended trochanteric osteotomy for the treatment of vancouver B2/B3 periprosthetic fractures of the femur." The Journal of arthroplasty 23(4): 527-533. Lewallen, D. G. and D. J. Berry (1998). "Periprosthetic fracture of the femur after total hip arthroplasty: treatment and results to date." Instructional course lectures 47: 243-249. Lindahl, H., H. Malchau, et al. (2005). "Periprosthetic femoral fractures classification and demographics of 1049 periprosthetic femoral fractures from the Swedish National Hip Arthroplasty Register." The Journal of arthroplasty 20(7): 857-865.

8
Images:
Image I: The image on the left demonstrates a mildly displaced greater trochanteric fracture. This was treated non-operatively and has healed at final follow-up approximately 3 years after the fracture.
Image II: The presenting films are shown above with a nondisplaced greater trochanteric fracture with significant osteolysis. The fracture had healed prior to revising the acetabulum. The three month follow-up x-ray shows bone grafting of the greater trochanter, good fracture healing, and the acetabulum has been revised.
9
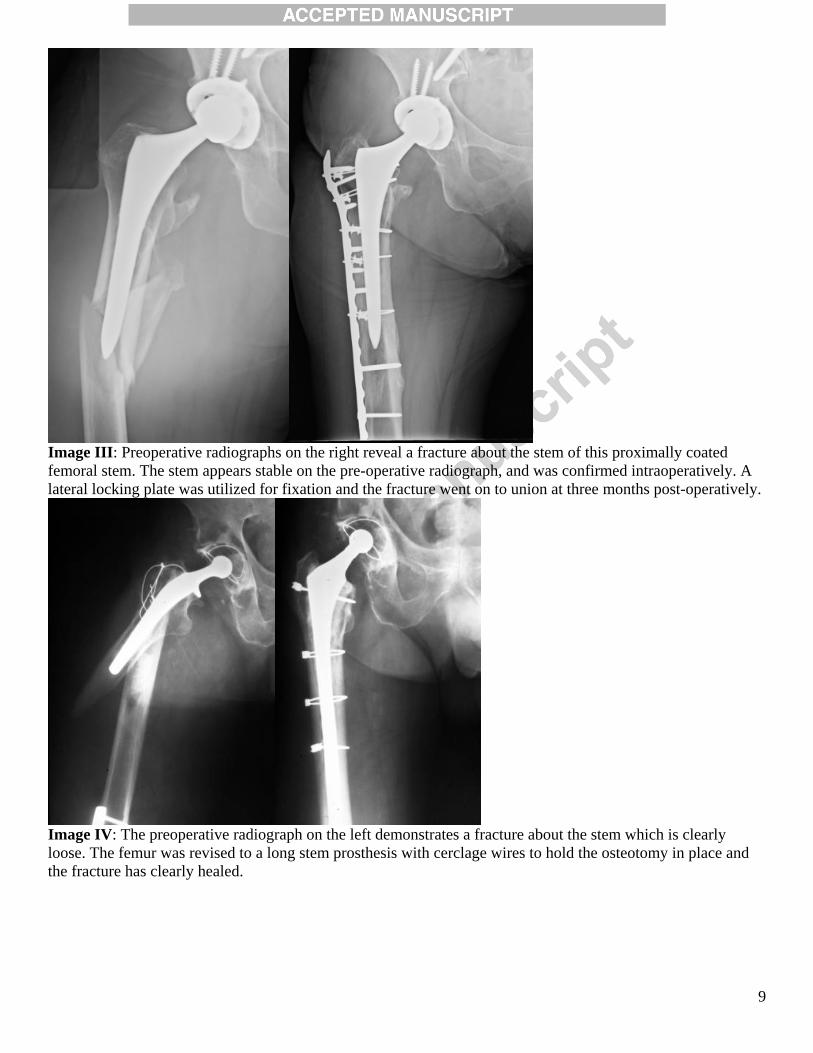
Image III: Preoperative radiographs on the right reveal a fracture about the stem of this proximally coated femoral stem. The stem appears stable on the pre-operative radiograph, and was confirmed intraoperatively. A lateral locking plate was utilized for fixation and the fracture went on to union at three months post-operatively.
Image IV: The preoperative radiograph on the left demonstrates a fracture about the stem which is clearly loose. The femur was revised to a long stem prosthesis with cerclage wires to hold the osteotomy in place and the fracture has clearly healed.

10
Image V: The pre-operative film on the left shows a fracture about the stem of a proximally coated femoral stem. Intraoperatively, the stem was confirmed to be grossly loose and the stem was revised to a fluted, tapered, modular stem with interval healing of the fracture on the right at three months post-operative.
Image VI: The pre-operative film on the left shows a fracture about the stem with loosening of the femoral stem and significant osteolysis. The middle image shows a fluted tapered modular stem was utilized to bypass the area of bony deficiency and the greater trochanter was held in place with wires. The final two year post-operative x-rays show that there has been bone reconstituted and the fracture has healed.
11
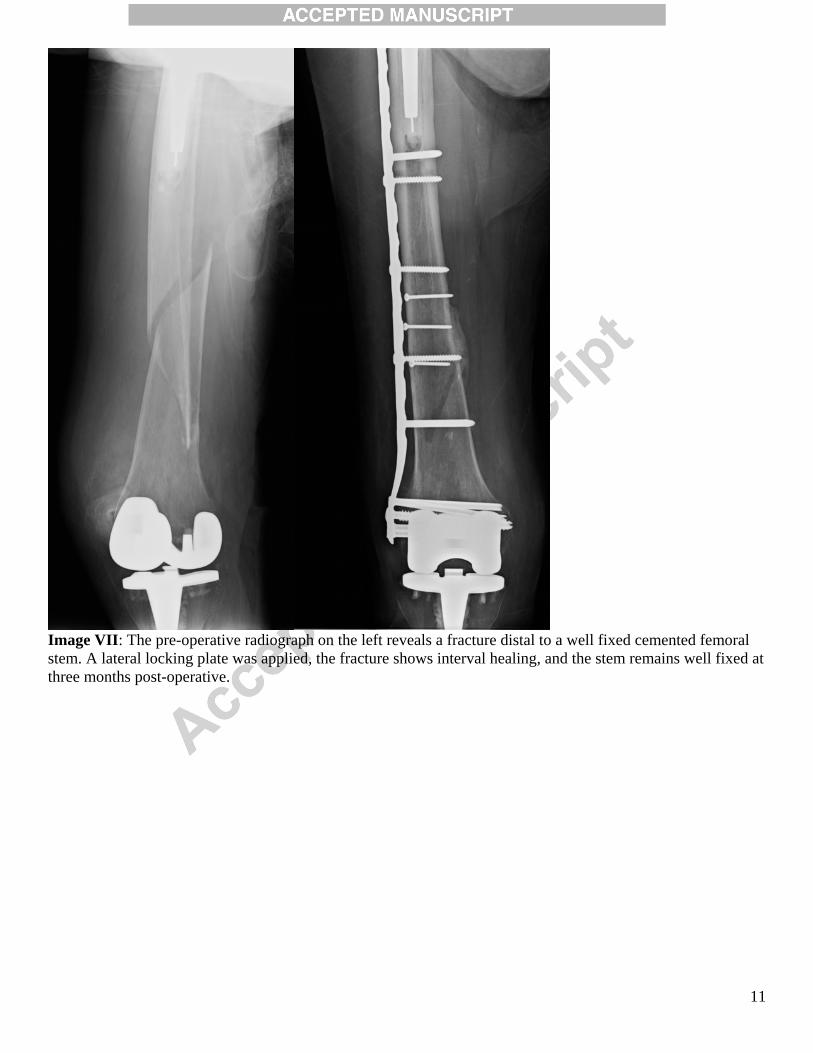
Image VII: The pre-operative radiograph on the left reveals a fracture distal to a well fixed cemented femoral stem. A lateral locking plate was applied, the fracture shows interval healing, and the stem remains well fixed at three months post-operative.





























