Embed Size (px)
Citation preview

Peripheral T-cell lymphomas (PTCL)Specified and Unspecified
Eric Van Den Neste
Cliniques universitaires Saint-Luc
Bruxelles
BHS seminar 12, 07 March 2015

Peripheral T-cell lymphomas (PTCL)Specified and Unspecified
1. Physiopathology, epidemiology, diagnosis, prognosis – key points summary
2. Treatment – general recommendations
3. Treatment – disease-adapted recommendations

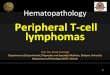
T-cell ontogenesis
Cellular differentiation
Self-Ag recognition
MHC recognition
Pos- & neg-selection
TCR() receptor
Immature T-cell malignancies
(Thymic, TdT+)
T-ALL
T-LBL
Fetal liver
BM
Thymus Peripheral lymphoid organs
CD4+
CD8+
Malignant counterpart
Mature T-cell malignancies
(Post-Thymic, TdT-)
PTCL
Lymphoid
progenitors
NK
T

APC
PTCL: pathophysiology of T-cell subsets
T/NK T
Innate immune system Adaptive immune system
Apoptotic/necrotic cell death
(not MHC restricted or limited
repertoire)
cytokines
chemokines
complement
CD4+ cells: regulatory
CD8+ cells: cytotoxic
(MHC restricted, greater specificity)
antigen
recognition
Pediatric/young T-cell lymphoma
Extranodal, CD4-/CD8-
Cytokine storm, HS
Ex: NK-cell lymphoma, ETTCL
Post-thymic
lymphocytes
Adult T-cell lymphoma
Nodal, predominantly CD4+
Ex: PTCL-NOS

Simplified classification of PTCL10-15% of all lymphomas, 23 entities
• Common category
– Peripheral T-cell lymphoma, unspecified (PTCL-U/NOS) 34%
– Angioimmunoblastic T-cell lymphoma (AILT) 29%
– Extranodal NK/T-cell lymphoma, nasal type (NKTCL) 4%
– Enteropathy-type T-cell lymphoma (ETTCL) 9%
– Hepatosplenic T-cell lymphoma 2%
– Subcutaneous panniculitis-like T-cell lymphoma <1%
• Anaplastic large-cell lymphoma category
– ALK(-), systemic 9%
– ALK(+), systemic 6%
– cutaneous CD30+ 1%
For a complete classification, see WHO 2008 and Vose et al, JCO 2008
Europe

Diagnosis of PTCL
• Multiparametric approach (clinical picture, phenotype, morphology, genetics), no specific markers
• Phenotypic profile:
– CD4/CD8 stain may indicate clonal restriction BUT double-neg and double-pos
– Frequent antigenic loss (« antigen-aberrancy »), ie CD5 and CD7
– TCR rearrangement pivotal, but germline in NK subtypes!
• Other markers
– Cytotoxic profile: granzyme, perforin
– NK markers
– CD30+: ALCL
– ALK+, t(2;5)
– EBV: nasal forms, aggressive behaviour

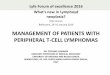
PTCLPrognosis
Overall survival of 288 PTCL patients compared with 1,595
DLBCL patients
Gisselbrecht, Blood 1998
PTCL is a poor prognosis disease, except for some specific
entities (ie, ALCL ALK+, primary cutaneous ALCL, MF)

PTCL, NOSPoor prognosis also explained by high IPI
Most PTCL patients
are advanced:
0/1: 28%
2-5: 72%
Weisenburgerr, Blood 2011
Factors included:
Age (<60y vs >60)
LDH (<NL vs >Nl)
ECOG PS (0-1 vs 2-4)
Stage (I/II vs III/IV)
EN involvement (<1 site vs >1)

PTCLClinical characteristics
• Age > 50y, male, aggressive behavior, EN sites
• Potential association with hemophagocytic syndrome (HS)
• More « specific » clinical features
– AILT: fever, rash, polyclonal gammapathy, auto-immunity
– NKTCL: EBV-related, local nasal destruction, extensive necrosis
– Hepatosplenic : young men, liver/spleen, immune suppression, chronic antigen stimulation (SLE), i(7)(q10)
– ETTCL: jejunum/ileum, closely associated with celiac disease
– Panniculitis-like: subcutaneous nodules, HS often fatal

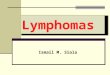
PTCL – TreatmentCHOP is standard
Reviewed in Foss, Semin Hematol 2010
≈ 30%

Weisenburger, Blood 2011
OS and FFS of 340 patients with PTCL-NOS (retrospective)
PTCL – TreatmentCHOP is disappointing

PTCL - TreatmentHow to do better than CHOP? What has been tried?
• Consolidation with upfront ASCT
• Consolidation with upfront allogeneic transplantation
• Addition of etoposide: CHOEP
• New CHOP-X combinations
No proof of superiority, sometimes looks better but not demonstrated in randomized trials

PTCLRole of high-dose therapy and ASCT in consolidation
Rodriguez, Ann Oncol 2004
BUT
-median age 46y
-Only 14% PIT 3-4
-ALCL included (ALK
status not known)

Le Gouill, JCO 2008
Patient characteristics (n=77):
18-60 years, LDH ≤ UNV
35% ALCL, 35% PTCL-NOS, 14% AITL
All pretreated (25% ASCT)
74% myeloablative, TBI 66%, RIC 26%
PTCLRole of allogeneic translantation
BUT
-Survivals given AFTER
transplantation
-Many patients do not achieve
transplant eligibility at any time!

PTCLRole of addition of etoposide (retrospective)
Schmitz et al, Blood 2010
ALCL, ALK-positive Other subtypes
Benefit in young mainly, risk of toxicity in elderly

PTCL – TreatmentNew CHOP-X combinations
• CHOP-alemtuzumab (closed study)
• CHOP-rhomidepsin (ongoing study)
• CHOP alternating with BV (brentuximab vedotin) or CHP-BV for CD30+ malignancies
• Maintenance pralatrexate after CHOP

PTCLTreatment recommendations
• Start with an anthracyclin-containing regimen
• CHOP21/14, CHOEP…
• If NO/SLOW response (role of Pet?), try to convert into CR
• ESHAP, DHAP, IFE (IFO-VP16), gemcitabine-containing…
• Consider upfront HDT and ASCT
• in young patients with initial int/high IPI (majority)
• and/or with HS
• and chemosensitive (in 1st CR)
• HDT and ASCT (or allogenic Tx?) in relapse
• if not transplanted upfront
• and chemosensitive (in 2nd or higher CR)

PTCLBelgian treatment recommendations (van Obbergh et al, BJH 2013)
Overallrecommendations Category*
· Inclusioninaclinicaltrialisadvisedgiventhedisappointingresultsofstandardmanagement
· CHOP-basedtreatments1remainstandard
· 4-6cyclesconsolidatedbylocoregionalRTinlocalizeddisease(stagesIorII)withIPI0or1
· 6-8cycles+/-RTinadvanceddisease(stagesIII,IV)orlocalizeddiseasewithIPI2or3
2A
· ConsiderconsolidationwithHDT/ASCTinfirstlineifrespondingpatientsandinthepresenceofriskfactors2
2B
· In refractory/relapsing patients, use non cross-resistant (mainlyplatinum-orgemcitabine-based)regimens3andconsiderpatientforASCTifnotperformedpreviously,orallogeneictransplantation,ornewdrug
2A
· Incaseofallogeneictransplantation,considerRICbecauseofthetoxicityofmyeloablativeconditionings
2B
· CNSprophylaxisasinDLBCL 2B
* Grade of recommendation based on NCCN categories of evidence and consensus1 Potential regimens: CHOP-21, CHOP-14, CHOEP-21, CHOEP-14…2 IPI 2 or 3, presence of HPS3 DHAP, ESHAP, gemcitabine-containing (GDP, GemOX), ICE, pralatrexate, romidepsin, alemtuzumab, bortezomib…

Low-IPI PTCLs: more conservative approach?
18/02/2014 19/06/201422/08/2014
08/10/2014
IPI=0 Metabolic CR?
6xCHOP, planned for RT
Facial palsy Systemic relapse
MTX IT and systemic

PTCLTreatment recommendations by NCCN version 1.2015

PTCLTreatment recommendations by NCCN version 1.2015

PTCLTreatment recommendations by ESMO 2013

PTCL« How I treat the PTCLs » by Moskowitz et al, Blood 2014
• General approach
– « Outside of a clinical trial, we most frequently use the treatment approach evaluated in the Nordic study with 6 cycles of CHOEP-14 followed by consolidation with ASCT as this is the largest dataset with the best phase II outcomes »
• Is there a favorable risk PTCL who should be treated differently?
– Low IPI patients: « Clearly, even for these more favorable patients, reduced therapy is not validated »
– ALK-positive: « We generally treat these patients as we treat the less favorable diseases with induction chemotherapy and ASCT consolidation »

PTCL« How I treat the PTCLs » by Moskowitz et al, Blood 2014
• Relapsed/refractory (R/R) disease
– « We typically aim for allogeneic stem cell transplant (alloSCT) in fit patients, as in our experience this has been more reliably curative than ASCT in the relapsed setting »
• Categories of R/R patients
– Transplant soon: fit, donor+
Multiagent chemotherapies (IFO, CARBO or CDDP) before Tx
– Transplant never: age, co-morbidities, lack of donor, choice…
– Transplant unclear: to be valuated for Tx
Experimental or single-drug more tolerable

PTCL – TreatmentRecommendations by disease subtypes
• ALCL ALK+, systemic
• Primary cutaneous ALCL
• Extranodal NK/T, nasal type
• Enteropathy-type (EATL)

PTCL - ALCL category (CD30+)ALK+ systemic vs ALK- systemic
ALK+
ALK-
PTCL vs DLBCL ALCL ALK+ vs ALK-
ALK+ (ALKoma) systemic ALCL:
Men, < 35y
Chromosome translocation t(2;5), resulting in the fusion protein NPM-ALK
CHOP-type treatment, no upfront HDC-SCT (at relapse)

PTCL - ALCL category (CD30+)ALK+ systemic, ALK- systemic, Cutaneous
Features
ALK+ systemic
ALCL
ALK-systemic
ALCL
Primary cutaneous
ALCL
T-cell phenotype CD4 CD4 CD4
ALK protein + - -
CD30 + + +
Median age <30 >50 >50
5-y OS 65-90% 30-40% >90%
Treatment Chemo Chemo conservative
Transplantation NO (2A) YES (2B) NO

PTCL - ALCL category (CD30+)ALK+ systemic, ALK- systemic, Cutaneous
Cutaneous ALCLPrimary cutaneous ALCL:
Localized nodules, spontaneous regression 25%
Spot radiation, surgical excision, interferon + bexarotene
CHOP-type treatment only advanced cases

Extranodal NK/TCL, nasal typeClinical presentation

Extranodal NK/TCL, nasal typeMainstays of treatment
• Avoidance of anthracyclins
• Radiotherapy (> 50 Gy)
• L-asparaginase

Extranodal NK/TCL, nasal typeMainstays of treatment
Localized disease*
* Definition: stage IE disease, potentially stage IIE
Radiotherapy (concurrent, sequential, or in sandwich at > 50 Gy) combined with chemotherapy (L-asparaginase-containing)
Advanced disease
AspaMetDex followed by BEAM and ASCT
(Jaccard, Blood 2011)
SMILE followed by BEAM/ASCT or allogenic Tx
(Yamaguchi, JCO 2011)
See also « How I treat NK/T-cell lymphomas », Tse & Kwong, Blood 2013

Smile1 Smile2 BEAM+
ASCT
Extranodal NK/TCL, nasal typeSMILE regimen

PTCLNew drugs
• Pralatrexate
– Novel antifolate, ORR 29%
– In combination? Maintenance?
• Romidepsin
– HDACi, ORR 30%
• Bendamustine
• Brentuximab vedotin
– Anti-CD30 antibody-drug conjugate
– ALCL (ALK+ and ALK-): ORR 87%, 57% CR
– Active in systemic CD30+ PTCLs: 33-54% ORR

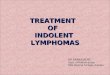
New drugs: alisertib (Aurora-kinase inhibitor)
07/08/14 07/10/2014 02/12/2014 10/02/2015
Courtesy by Dr Philippe d’Abadie, nuclear medicine, UCL Saint-Luc
PTCL NOSRelapse 6 months
after 6xCHOP14
Alisertib2 months
Alisertib4 months
Alisertib6 months

PTCLConclusions
• CHOP remains the (poor) platform to build on, but beware of additional toxicity of CHOP-X
• Limited number of patients who can be treated less intensively must be identified, but beware of under-treatment
• More targeted approaches eagerly awaited