Embed Size (px)
Citation preview

www.thelancet.com/neurology Vol 12 October 2013 1011
Review
Peripheral neuropathy in mitochondrial disordersDavide Pareyson, Giuseppe Piscosquito, Isabella Moroni, Ettore Salsano, Massimo Zeviani
Why is peripheral neuropathy common but mild in many mitochondrial disorders, and why is it, in some cases, the predominant or only manifestation? Although this question remains largely unanswered, recent advances in cellular and molecular biology have begun to clarify the importance of mitochondrial functioning and distribution in the peripheral nerve. Mutations in proteins involved in mitochondrial dynamics (ie, fusion and fi ssion) frequently result in a Charcot-Marie-Tooth phenotype. Peripheral neuropathies with diff erent phenotypic presentations occur in mitochondrial diseases associated with abnormalities in mitochondrial DNA replication and maintenance, or associated with defects in mitochondrial respiratory chain complex V. Our knowledge of mitochondrial disorders is rapidly growing as new nuclear genes are identifi ed and new phenotypes described. Early diagnosis of mitochondrial disorders, essential to provide appropriate genetic counselling, has become crucial in a few treatable conditions. Recognising and diagnosing an underlying mitochondrial defect in patients presenting with peripheral neuropathy is therefore of paramount importance.
IntroductionPeripheral nerves are highly dependent on energy metabolism, since they have long axons that are wrapped by myelin lamellae provided by Schwann cells. Thus, it is not surprising that a third of patients with mitochondrial disorders develop peripheral neuro-pathy.1–3 Although often mild or subclinical, peripheral neuropathy can be severe and might be the main or only feature of a mitochondrial disorder. Identifi cation and characterisation of peripheral neuropathy can be fundamental in diagnosing mitochondrial disorders. Peripheral neuropathy often occurs in mitochondrial disorders associated with defects in mitochondrial DNA (mtDNA) maintenance and replication or defects in respiratory chain complex V. The distribution of mitochondria along peripheral axons is regulated by a continuous process of mitochondrial fusion and fi ssion (this is termed mitochondrial dynamics and is fundamental for regulating number, shape, and transport of these organelles), and abnormalities in mitochondrial dynamics are increasingly understood to be a cause of peripheral nerve dysfunction. Additionally, nuclear genes associated with mitochondrial disorders are continuously being identifi ed, and new phenotypes are expanding the list of atypical presentations of known mitochondrial disorders.
This Review addresses peripheral neuropathy in mitochondrial disorders, particularly when it is the key or only feature. Peripheral neuropathy as a unique or predominant manifestation of a mitochondrial disorder is rare, and is restricted to disorders of mitochondrial dynamics associated with MFN2 and GDAP1 mutations;4–9 a few mitochondrial disorders related to defects in mtDNA replication and maintenance, caused by mutations in nuclear genes such as POLG1, C10ORF2, TYMP, and MPV17; or respiratory chain complex V defects associated with MTATP6 mutations leading to decreased ATP synthesis.1–3,10–14 Whereas disorders of mitochondrial dynamics usually present with a Charcot-Marie-Tooth neuropathy (CMT), disorders of mtDNA replication and maintenance and respiratory chain
complex V abnormalities are associated with a range of neuropathic phenotypes (panel). Peripheral neuropathy can occur in mitochondrial disorders other than those due to disorders of mitochondrial dynamics or mtDNA replication and maintenance, but it is usually mild or subclinical.
Chronic sensorimotor axonal polyneuropathy is the pattern most often seen in cases of peripheral neuropathy associated with mitochondrial disorders.3,10,15–17 De-myelinating neuropathy is less common,1–3,10,15,16 but is often associated with mitochondrial neurogastro-intestinal encephalomyopathy (MNGIE; related to TYMP mutations)13 and occasionally with Leber hereditary optic neuropathy,18 Leigh syndrome,19 myoclonic epilepsy and ragged-red fi bres (MERRF) syndrome,16 and mito-chondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS) syndrome.20 Sensory ataxic neuropathy is another syndrome associated with mitochondrial disorders, particularly ataxia neuropathy spectrum related to POLG1 mutations, and neuropathy, ataxia, and retinitis pigmentosa (NARP) syndrome associated with MTATP6 mutations.1-3,10,11
In most mitochondrial disorders, peripheral neuropathy occurs in the setting of multisystem neurological impairment as a minor manifestation that is useful for diagnosis but with little eff ect on patient disability. A small proportion of patients develop moderate-to-severe peripheral neuropathy in the context of multisystem diseases such as MELAS and MERRF syndromes, Leigh syndrome, and Kearns-Sayre syndrome.1–3,10 In these cases, peripheral neuropathy might be the fi rst manifestation, subsequently complicated by involvement of other neurological systems and extraneurological organs.
It is important for neurologists to know when a mitochondrial disorder might be the underlying cause of peripheral neuropathy—ie, they should know the clinical presentations, diagnostic clues, examinations to be performed, diff erential diagnoses, and disorders amenable to treatment. This Review aims to provide an update on peripheral neuropathy in mitochondrial disorders with a practical diagnostic approach.
Lancet Neurol 2013; 12: 1011–24
Clinic of Central and Peripheral Degenerative Neuropathies Unit, Department of Clinical Neurosciences (D Pareyson MD, G Piscosquito MD, E Salsano MD), Child Neurology Unit, Department of Child Neurology (I Moroni MD), and Molecular Neurogenetics Unit, Department of Diagnostic and Applied Technology (M Zeviani MD), IRCCS Foundation, C Besta Neurological Institute, Milan, Italy; and MRC Mitochondrial Biology Unit, Cambridge, UK (M Zeviani)
Correspondence to:Dr Davide Pareyson, Clinic of Central and Peripheral Degenerative Neuropathies Unit, Department of Clinical Neurosciences, IRCCS Foundation, C Besta Neurological Institute, via Celoria 11, 20133 Milan, [email protected]

1012 www.thelancet.com/neurology Vol 12 October 2013
Review
Mitochondrial CMTCMT is a heterogeneous group of hereditary neuropathies characterised by distal limb muscle wasting and weakness, with sensory loss, reduced or absent deep tendon refl exes, and foot deformities. Subdivision into demyelinating (CMT1 if autosomal dominant and CMT4 if autosomal recessive) and axonal forms (CMT2, which is typically dominant but can be recessive) is based on nerve conduction velocities (demyelinating if ≤38 m/s in upper limb motor nerves vs axonal if >38 m/s). Intermediate forms between CMT1 and CMT2 include X-linked CMT (CMTX1), and dominant and recessive intermediate CMT types. Pure motor forms are labelled as distal hereditary motor neuropathies. Rare subtypes include hereditary motor and sensory neuropathy type V, which indicates CMT plus corticospinal tract involvement (CMT5), and type VI, which is CMT with optic atrophy
(CMT6). More than 50 genes (eg, MFN2 and GDAP1) have been associated with CMT or distal hereditary motor neuropathies and contribute to their further subclassifi cation.21,22
CMT might be the presenting phenotype of disorders of mitochondrial dynamics and other mitochondrial dysfunctions, including respiratory chain complex V defi cit. The main forms of mitochondrial CMT are listed in table 1. Pure autosomal dominant CMT2 of varying severity, sometimes complicated by pyramidal involvement or optic atrophy, is associated with mutations in MFN2, whereas GDAP1 mutations usually result in autosomal recessive CMT with normal or decreased nerve conduction velocities.
MFN2 and GDAP1 are involved in the fusion and fi ssion of mitochondria (mitochondrial dynamics), processes that are fundamental in regulating mitochondrial shape, size, number, and transport along the cell (fi gure 1).4,5 Fusion is governed by dynamin-like GTPases located in the outer membrane (MFN1 and MFN2) and inner membrane (OPA1).4,5 MFN1 and MFN2 form homotypic and heterotypic oligomers, tethering mitochondria during fusion. OPA1 is important for inner membrane fusion and cristae shaping. GDAP1, located in the outer membrane, has a role in mitochondrial fi ssion.4,6 At least three proteins involved in mitochondrial dynamics are associated with peripheral neuropathy—ie, mutations aff ecting MFN2 and GDAP1 can cause CMT,7–9,21,22 and OPA1 mutation carriers can develop neuropathy.23–25 So far, no phenotype has been associated with MFN1 mutations.
MFN2-related CMT and more complex phenotypesMFN2 is a 19-exon gene on chromosome 1p36.22 that encodes a 757-aminoacid protein containing a GTPase domain, two transmembrane domains, and two coiled-coil regions that mediate binding with other mitofusin molecules.7,26 MFN2 tethers mitochondria to the endoplasmic reticulum and might have a role in calcium release and infl ux to mitochondria.26 MFN2 is also involved in increasing permeability of the outer membrane, oxidative phosphorylation and gradient coupling, and mitochondrial transport along neurons through the microtubule system.5,26,27 This is a crucial process that allows proper distribution of mitochondria in the cell, including concentration in particular regions of peripheral neurons (eg, Ranvier’s nodes and synaptic terminations).27 Although MFN2 is ubiquitously expressed, mutations in this protein have been associated only with neurological dysfunction, particularly CMT. Low levels of MFN1 in neurons, which are not suffi cient to compensate the MFN2 defect, are postulated to contribute to the organ specifi city of the disease.4,26
Clinical characteristics and presentationMFN2 mutations are usually associated with autosomal dominant axonal CMT2 (CMT2A), and MFN2 is the most frequently mutated gene in CMT2 (in up to about 20% of
Panel: Mitochondrial disorders with peripheral neuropathy
Neuropathy as the only or predominant feature• MFN2-related disorders : autosomal dominant CMT2A, autosomal recessive CMT2, CMT5
(HMSN type V), CMT6 (HMSN type VI), complex phenotypes• GDAP1-related disorders: autosomal recessive CMT2K, CMT4A, recessive intermediate
CMT, autosomal dominant CMT2K• MTATP6-related disorders: CMT2 and dHMN• DHTKD1-related disorder: CMT2Q • AIFM1-related disorder: CMTX4 (Cowchock syndrome)• PDK3-related disorder: CMTX6
Neuropathy as a key feature• MTATP6-related disorders: NARP, MILS• POLG1-related disorders: ataxia neuropathy spectrum , SANDO, MNGIE-like syndrome• C10ORF2-related disorder: SANDO, IOSCA (MTDPS7), complex phenotypes• TYMP-related disorder: MNGIE (MTDPS1)• RRM2B-related disorder: MNGIE-like syndrome (MTDPS8B)• MPV17-related disorder: Navajo neurohepatopathy (MTDPS6)• SLC25A19-related disorder: neuropathy and bilateral striatal necrosis
Neuropathy as a minor feature• OPA1-related disorder: DOA plus syndrome• POLG1-related disorders: MIRAS, Alpers-Huttenlocher syndrome, MEMSA, complex
phenotypes• ND1-related, ND4-related, and ND6-related disorders and other mtDNA mutations:
LHON• SURF1-related disorder and other gene mutations: Leigh syndrome• MTTL1 3243A→G and other mtDNA mutations: MELAS syndrome• MTTK 8344A→G and other mtDNA mutations: MERRF syndrome• Single mtDNA deletion-related disorder: Kearns-Sayre syndrome• ADCK3-related disorder: primary coenzyme Q10 defi ciency syndrome• Non-syndromic respiratory chain disorders
CMT=Charcot-Marie-Tooth neuropathy. HMSN=hereditary motor and sensory neuropathy. dHMN=distal hereditary motor neuropathy. NARP=neuropathy, ataxia, and retinitis pigmentosa. MILS=maternally inherited Leigh syndrome. SANDO=sensory ataxia, neuropathy, dysarthria, and ophthalmoplegia. MNGIE=mitochondrial neurogastrointestinal encephalopathy. IOSCA=infantile-onset spinocerebellar ataxia. MTDPS=mitochondrial DNA depletion syndrome. DOA=autosomal dominant optic atrophy. MIRAS=mitochondrial recessive ataxia syndrome. MEMSA=myoclonic epilepsy, myopathy, and sensory ataxia. LHON=Leber hereditary optic neuropathy. MELAS=mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes. MERRF=myoclonus epilepsy with ragged-red fi bres. mtDNA=mitochondrial DNA.

www.thelancet.com/neurology Vol 12 October 2013 1013
Review
cases).7,28–33 Most patients with CMT2A have disabling neuropathy with early onset (during childhood or adolescence), a progressive course, and motor predominance, sometimes leading to loss of ambulation and severe proximal weakness.7,28,29,31 Other cases show less severe phenotype and later onset.28 De-novo mutations occur with a high frequency in CMT2A.30,31 Almost 100 sequence variants are known, mainly missense mutations in crucial MFN2 protein regions, particularly the GTPase domain and coiled-coil motifs; a few small deletions as well as frameshift and nonsense mutations have also been reported.26,31 Incomplete penetrance with no phenotype in mutation carriers has been reported; additionally, some sequence variations are probably benign polymorphisms.31
In CMT2A, nerve conduction velocities are preserved or slightly slowed, with varying reduction in amplitudes of compound muscle and sensory action potentials, mainly in the lower limbs.29–31 Very rarely, nerve conduction velocity is slowed out of proportion with the reduction in compound muscle action potential amplitude determined by axonal loss, suggesting secondary myelin abnormalities. Nerve biopsies usually show predominant chronic axonal degeneration sometimes with the presence of small onion bulbs (fi gure 2).29,30,34 Some reports described mitochondrial abnormalities with distal accumulation of abnormally shaped mitochondria with cristae alterations.29,34,35
More complex phenotypes that are sometimes seen with CMT2A include the presence of hand tremor and
hearing loss, which are non-specifi c features also observed in other CMT types.7,21,30 About 10–20% of patients with MFN2-related neuropathy develop optic atrophy, showing that MFN2 mutations are a molecular basis for hereditary motor and sensory neuropathy type VI (CMT6).28–30,36 Patients might develop subacute visual loss with subsequent good or incomplete recovery—resembling Leber hereditary optic neuropathy—or insidious and gradually worsening visual impair ment.28,29,36 Mutations in diff erent domains have been associated with hereditary motor and sensory neuropathy type VI, although members of the same CMT2A family might or might not develop optic atrophy.7,28–30 Pyramidal involvement can complicate CMT2A, with increased deep tendon refl exes, Babinski sign, and, rarely, overt spastic paraplegia, suggesting another molecular basis for hereditary motor and sensory neuropathy type V (CMT5).37,38 Discrete T2 hyperintense signals have been reported in brain MRIs of patients with CMT2A;30,39,40 although unspecifi c, the occurrence of this fi nding in several young patients suggests an association with the disease.
A few families have been reported with early-onset axonal neuropathy and homozygous or compound heterozygous MFN2 mutations (some mutations were intragenic deletions), which manifest as recessive or semidominant traits with no or few signs in heterozygous carriers.34,41,42 The phenotype ranged from a severely disabling neuropathy with optic neuropathy, cranial nerve, and respiratory involvement, to typical CMT2.
Gene Inheritance Nerve conduction velocity Neuropathology Frequency
CMT2A MFN2 Autosomal dominant Normal to slightly reduced Axonal changes Around 10–20% of CMT2
Autosomal recessive CMT2A MFN2 Autosomal recessive or semidominant
Normal to slightly reduced Axonal changes A few families reported
CMT5 (HMSN type V) with pyramidal involvement
MFN2* Autosomal dominant Preserved Axonal changes Rare
CMT6 (HMSN type VI) with optic atrophy
MFN2 Autosomal dominant Preserved Axonal changes 10–20% of CMT2A
Autosomal dominant CMT2K GDAP1 Autosomal dominant Normal to slightly reduced Axonal changes Around 5% of CMT2
CMT4A GDAP1 Autosomal recessive Slowed nerve conduction velocity, severely reduced CMAP
Mainly axonal changes, with or without secondary myelin abnormalities
Probably second most common type of recessive CMT
Recessive intermediate CMTA GDAP1 Autosomal recessive Intermediate Mainly axonal changes, with or without secondary myelin abnormalities
Probably second most common type of recessive CMT
Autosomal recessive CMT2K GDAP1 Autosomal recessive Preserved Mainly axonal changes, with or without secondary myelin abnormalities
Probably second most common type of recessive CMT
CMT2 and dHMN MTATP6 Matrilineal Normal to slightly reduced Onion bulbs in one biopsy Rare (<1% of CMT2)
CMT2Q DHTKD1 Autosomal dominant Normal to slightly reduced Not determined One family
CMTX4 (Cowchock syndrome) AIFM1 X-linked Preserved Not determined Deafness and cognitive impairment
CMTX6 PDK3 X-linked Varying, slightly slowed Not determined One family
CMT=Charcot-Marie-Tooth neuropathy. HMSN=hereditary motor and sensory neuropathy. CMAP=compound muscle action potential. dHMN=distal hereditary motor neuropathy. *Other genes are also associated with CMT5.
Table 1: Main forms of mitochondrial CMT

1014 www.thelancet.com/neurology Vol 12 October 2013
Review
The spectrum of MFN2-related phenotypes is rapidly broadening, and complex clinical pictures have been reported. Macrocephaly and mild diff use signal abnormalities in cerebral white matter occurred in two patients with CMT2A.40 Del Bo and colleagues38 reported a family with CMT2A with cognitive and visual impairment and, in one case, spastic paraparesis. Boaretto and colleagues43 studied a family carrying a heterozygous intronic MFN2 mutation, where late-onset, rapidly progressive CMT2 was complicated by subacute, lethal, Wernicke-like encephalopathy in four
individuals; MRI and autopsy showed symmetric vascular–necrotic lesions in the upper brainstem and periaqueductal grey matter.
Recently, a large family harbouring a novel Asp210Val substitution in the GTPase domain of MFN2 showed a very complex phenotype, with the following features present to a varying extent in aff ected individuals: optic atrophy, predominantly sensory axonal neuropathy, hearing loss, pyramidal involvement, cognitive impair-ment, proximal myopathy, cerebellar syndrome, cataracts, supratentorial white matter changes, and muscle
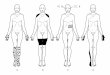
Figure 1: Overview of mechanisms underlying the main mitochondrial peripheral neuropathies(A) MFN2 is located in the outer mitochondrial membrane and interacts with Miro and Milton proteins, which belong to the molecular complex that links mitochondria to kinesin (KHC) motors. (B) MFN2 participates in bringing the outer membranes of two mitochondria into close proximity. Thus, MFN2 mutations can lead to defects in mitochondrial motility along the cytoskeletal microtubular tracks, and to dysfunction in fusion of the outer mitochondrial membranes of opposing mitochondria. Similarly, mutations in OPA1, which is located in the inner mitochondrial membrane, lead to dysfunction in the fusion process of the inner mitochondrial membrane. (C) Loss-of-function mutations in GDAP1, located in the outer mitochondrial membrane, can lead to dysfunction in the mitochondrial fi ssion process, since GDAP1 might be a positive eff ector of assembly of the fi ssion mediator DRP1. Dysfunction is shown by red oblique bars. (D) Dysfunctions in the respiratory chain can be due to the following: direct mutations in mitochondrial protein-coding genes (red segment of circular mtDNA) ND1, ND4, and ND6, which encode for subunits of complex I (NADH dehydrogenase), and MTATP6, which encodes for a subunit of complex V (ATP-synthase); mutations in mitochondrial tRNA-coding genes (light blue segment) MTTL1 and MTTK, which lead to dysfunction in transcription of mitochondrial protein-coding genes; or direct mutations in the nuclear gene SURF1 (in green), which encodes an ancillary protein involved in complex IV (cytochrome c oxidase) assembly. Dysfunction in the corresponding respiratory chain complexes are shown by red, light blue, and green asterisks, respectively. Encircled numbers show the number of subunits encoded by mtDNA. (E) Dysfunctions of the respiratory chain can also occur as a result of changes in mtDNA synthesis (red oblique bar), which lead to mtDNA depletion or multiple mtDNA deletions. mtDNA synthesis might be disturbed by the following: mutations in nuclear genes encoding components of the mitochondrial replisome—ie, polymerase gamma POLG and the helicase C10ORF2 genes; loss-of-function mutations (red oblique bar) in genes involved in the synthesis of nucleotides—ie, RRM2B and TYMP—which lead to nucleotide depletion (red lines show inhibition); or mutations in MPV17, a nuclear gene encoding an inner mitochondrial membrane protein of unknown function. Finally, mitochondrial peripheral neuropathies might result from changes in intermediary metabolism that eventually lead to decreased ATP synthesis. Mutations in SLC25A19 inhibit the passage of TPP from the cytosol to the mitochondrial matrix, thus leading to lactate accumulation and an increase in αKG (an intermediate of the Krebs cycle), since TPP is an essential cofactor of PDH and αKGD (green lines show stimulation); similarly, a gain-of-function mutation (green tick mark) in PDK3 might lock PDH in an inactive state, limiting glucose oxidation and favouring a switch toward anaerobic lactate production. nDNA=nuclear DNA. mtDNA=mitochondrial DNA. NDPs=nucleoside diphosphates. dNDPs=deoxynucleoside diphosphates. dCTD=deoxycytidine. dCMP=deoxycytosine monophosphate. dCTP=deoxycytosine triphosphate. α-KG=α-ketoglutarate. α-KGD=α-ketoglutarate dehydrogenase. SCA=succinyl-CoA. TPP=thiamine pyrophosphate. PDH=pyruvate dehydrogenase.
A B
D E
C
– +
MiroMiltonMFN2
Microtubules
KHC
MFN
2 MFN
2
OPA1 OPA1OPA1
OPA1
MFN2
MFN2
GDAP1
GDAP1DRP1
↑Thymidine
Thymine
mRNA
mRNA
GDAP1
GDAP1
↑Thymidine
TYMP↓dNDPs
dCTD
α-KG SCA
mtDNAsynthesis
TPP
↓dCMP → ↓dCTP
→
↓
NDPs
RRM2B
↓ATP
C10ORF2TK2
PDH
α-KGDPDK3
SLC25A19
POLG1
*Respiratory chain
↓dNTPsMPV17
IntermembranespaceInnermitochondrialmembraneMatrix
III
* * * * ** *
III IV V
mtDNA
ND6ND1 ND4 MTATP6
MTTK
SURF
1
MTTL1
7 21 3 ü

www.thelancet.com/neurology Vol 12 October 2013 1015
Review
mitochondrial abnormalities (including ragged red fi bres and multiple mtDNA deletions).44 A de-novo Asp210Tyr substitution was also reported in a girl aff ected by a severe multisystem disorder with psychomotor retardation, microcephaly, chorea, neuropathy, optic atrophy, hearing loss, and mtDNA depletion.45
Diagnosis of CMT related to MFN2 mutationsMFN2-related neuropathy should be suspected in all cases of axonal CMT, particularly if autosomal dominant, whatever the age of onset. Sporadic axonal CMT of early onset and severe course is a typical presentation related to the frequency of de-novo mutations. The co-occurrence of optic atrophy (CMT6) strongly points to MFN2 as a causative gene, and the presence of pyramidal involvement (CMT5) is another feature that warrants MFN2 mutation screening. The frequency with which mutated MFN2 causes very complex phenotypes is still unknown.
Pathological mechanismsHow MFN2 mutations result in CMT2 or more complex phenotypes is unclear. In cellular studies, some MFN2 mutations aff ect mitochondrial fusion, whereas others do not.5,26,27 Abnormal mitochondrial transport leading to distal axonal degeneration probably explains peripheral neuropathy and pyramidal involvement in CMT2A and CMT5, with the longest axons preferentially aff ected.27 The occurrence of optic atrophy in patients with CMT6 links MFN2 dysfunction to OPA1, since mutations in this gene are associated with dominant optic atrophy, a syndrome sometimes complicated by a multisystem neurological disorder with multiple mtDNA deletions or even depletion. Dominant optic atrophy is probably due to impaired mitochondrial fusion and not to abnormal mitochondrial transport.5,23–27 MFN2-related optic atrophy and more complex phenotypes could be the result of changes in MFN2 functions other than mitochondrial transport—eg, mitochondrial fusion or oxidative phosphorylation coupling, as seen with OPA1 mutations. Such dysfunction might lead to altered maintenance, instability, and secondary abnormalities of mtDNA, the ultimate patho-physiological basis for complex phenotypes.44
GDAP1-related CMTGDAP1 is encoded by a six-exon gene on chromosome 8q21.11 and contains two glutathione S-transferase domains, one transmembrane domain, one hydrophobic domain, and an alpha4–alpha5 loop important for protein interaction.8,9,46 GDAP1 is involved in mitochondrial fi ssion, although the mechanism is unknown. It is debated whether it is exclusively localised in axons or is also expressed in myelinating Schwann cells.4–6,9,47
Clinical characteristics and presentationGDAP1 mutations are usually associated with severe, early-onset, autosomal recessive CMT. Axonal (auto-somal recessive CMT2K), demyelinating (CMT4A), and
intermediate recessive (RI-CMT) forms have been described, leading to uncertainty about whether the primary defect is in the myelin or axon.8,9,48,49 Neuropathy is characterised by a severe course, with onset in infancy and rapid progression to loss of distal movements, proximal weakness, and wheel-chair dependence typically by age 20–30 years.46,49–51 Hoarseness of voice due to vocal cord palsy occurs in a high proportion of cases, and diaphragm involvement can also be observed.46,50
Nerve conduction velocity is often preserved; however, when reduced (sometimes substantially), it is accompanied by marked decrease in compound muscle action potential amplitude, suggesting concomitant severe axonal loss.46,49,51 Nerve biopsy shows constant and predominant chronic axonal degeneration, with preferential loss of large myelinated fi bres; demyelination features depend on the extent of axonal damage, in keeping with a primary axonal neuropathy, with secondary myelin changes ensuing with disease progression (fi gure 3).46,48,49
More than 40 mutations associated with GDAP1-related CMT have been described, with either compound heterozygosity or homozygosity. Most of these are mis-sense mutations involving the glutathione S transferase domains or the alpha4–alpha5 loop, but several frameshift, nonsense, and splicing mutations have also been reported.46,51 Recessive truncating mutations might
Figure 2: Nerve biopsy fi ndings in patients with CMT2A who carry MFN2 mutationsLight microscopy of transverse semithin sections stained with Toluidine blue, showing sural nerve biopsy in two patients with CMT2A, a 6-year-old girl with heterozygous Arg94Gln mutation (A, C), and a 68-year-old-woman with heterozygous Met376Ile mutation (B, D). (A, B) Nerve fascicles showing reduced myelinated fi bre density are more evident in the adult (B) case. (C, D) Higher magnifi cation of both cases showing myelin fi bre loss and occasional regeneration clusters (asterisks). In the aff ected child (C), some fi bres with thin myelin sheaths with respect to the axonal calibre are present (arrows). Image courtesy of Tiziana Cavallaro and Gian Maria Fabrizi.
A B
C D
10 µm
100 µm100 µm
10 µm

1016 www.thelancet.com/neurology Vol 12 October 2013
Review
be associated with more severe disease, suggesting that the C-terminal portion is necessary for protein targeting to mitochondria, and related mutations lead to a complete loss of function. Missense mutations might produce a protein that is still targeted to the outer membrane but has reduced or altered function, resulting in less severe consequences.46,49 Ten diff erent heterozygous GDAP1 mutations have been reported to cause autosomal dominant CMT2K, a form of CMT with later onset and less severe phenotype than recessive forms related to GDAP1, slowly progressive course, and only rarely leading to severe impairment; these patients show preserved or slightly slowed nerve conduction velocity, without evidence of relevant myelin derangement.51–53
Diagnosis of GDAP1-related CMTMutations in GDAP1 frequently cause recessive CMT and should be screened for in all patients with early-onset and severe CMT, irrespective of nerve conduction velocities, and particularly if electrophysiology or nerve biopsy show prominent loss of axons. Vocal cord palsy is another feature suggesting GDAP1-related neuropathy. The frequency of GDAP1 mutations in autosomal dominant CMT2 is undetermined, but might be high in regions with founder mutations (ie, Spain).32,53 Diff erential diagnoses include acquired and inherited causes of severe neuropathy with onset in infancy and childhood (table 2).
Pathological mechanismsA few GDAP1 mutations cause neuropathy in heterozygotes, whereas many others are associated with disease only when both alleles are mutated. Niemann and colleagues6 showed that recessive mutations behave as loss-of-function mutations and are associated with decreased mitochondrial fi ssion, whereas dominant mutations can cause a gain of abnormal function resulting in impaired fusion (as with MFN2 mutations), increased production of reactive oxygen species, and enhanced apoptosis. In both cases, changes in mitochondrial dynamics might lead to altered transport of mitochondria and the distal axonal degeneration typical of CMT, albeit with diff erent degrees of severity. Decreased activity of respiratory chain complex I was reported in muscle and fi broblasts from patients with dominant GDAP1-associated CMT.51 Two families with CMT had combined mutations in MFN2 and GDAP1.54,55 These individuals had severe neuropathy and substantial mitochondrial functional abnormalities (ie, reduced respiratory chain complex I activity and energy uncoupling in fi broblasts, and enlarged mitochondria with distorted cristae seen on nerve biopsy), because of the combined eff ect of the mutations on diff erent parts of the same pathway in mitochondrial dynamics.
MTATP6-related CMTMaternally-inherited mutations in the mitochondrial ATP-synthase subunit 6, encoded by MTATP6, usually present with NARP syndrome or Leigh syndrome; rarely, isolated peripheral neuropathy was reported in association with 9185T→C or 8993T→C mutations.56–60 Screening for the 8993T→C mutation in 96 clinically diagnosed (genetically undiagnosed) cases of CMT did not show any cases with the mutation;61 however, Pitceathly and colleagues62 recently found the 9185T→C mutation in 1∙1% of 270 patients with genetically undiagnosed CMT2. Three families and one sporadic patient presented with a phenotype that included pure motor or predominantly motor neuropathy (CMT2 and distal hereditary motor neuropathy); associated features were learning disabilities, pyramidal involvement, sensorineural hearing loss, retinitis pigmentosa, proximal neurogenic weakness, and illness with symptoms similar to those of Leigh syndrome. In another family, CMT2 was associated with the 9176T→C mutation.63 Therefore, diff erential diagnosis of CMT2 now includes MTATP6 mutations, particularly when there are mild associated features and transmission is compatible with matrilineal inheritance.
Other CMT typesRecently, a large Chinese family with autosomal dominant CMT2 was shown to carry a nonsense mutation in DHTKD1, which is involved in mitochondrial energy production;64 additionally, CMTX465 and CMTX666 have been associated with mutations in two genes involved in mitochondrial metabolism (table 1).
Figure 3: Nerve biopsy fi ndings in a patient with early-onset, severe, GDAP1-related neuropathySural nerve biopsy of a 3·5-year-old child with recessive CMT2K due to GDAP1 mutations (Arg125stop and Leu239Phe).49 (A, B) Light microscopy of transverse semithin sections stained with Toluidine blue. (A) A nerve fascicle showing reduced myelinated fi bre density. (B) Occasional Wallerian-like degenerations (arrow), cluster of regeneration (asterix), and Schwann cell hyperplasia (arrowheads) are seen. (C) Teased fi bres showing internodal and paranodal remyelination (arrows), short internodes as sign of regeneration (arrowheads), and fi bres with rosary-like morphology, expression of Wallerian-like degeneration (asterisk). (D–F) Electron microscopy ultrathin section (treated with uranyl acetate and lead citrate). (D) Normally myelinated fi bre surrounded by Schwann cell nuclei (asterisks) and cell processes containing amyelinated fi bres (arrows). (E) Several collagen pockets (arrows) as sign of unmyelinated fi bre loss. (F) Higher magnifi cation shows that mitochondrial morphology is unaff ected (arrowheads).
A B C
D E F
50 µm
400 nm1·5 µm2 µm
100 µm 10 µm

www.thelancet.com/neurology Vol 12 October 2013 1017
Review
Peripheral neuropathy with visual impairmentVisual loss due to optic atrophy or pigmentary retinopathy in combination with polyneuropathy is a phenotype highly suggestive of mitochondrial dysfunction, as in dominant optic atrophy plus syndrome (OPA1 mutations), Leber hereditary optic neuropathy (ND1, ND4, ND6), CMT6 (MFN2), and NARP syndrome (MTATP6). In CMT6, peripheral neuropathy precedes optic involvement and both might be prominent. In dominant optic atrophy plus syndrome, visual loss is almost always a predominant feature and peripheral neuropathy is a possible subsequent fi nding, often of minor importance. Leber hereditary optic neuropathy is only rarely complicated by peripheral neuropathy. Neuropathy and retinopathy are both typical of NARP syndrome and can be severely disabling.
Dominant optic atrophy plus syndrome and OPA1OPA1 is a 690-aminoacid protein encoded by a 30-exon gene on chromosome 3q29, and is involved in mitochondrial fusion, cristae organisation, oxidative phosphorylation, and maintenance of mitochondrial membrane potential. Heterozygous mutations lead to early-onset and progressive dominant optic atrophy.5 About 20% of patients develop subsequent hearing loss and further neurological abnormalities, such as progressive external ophthalmoplegia, peripheral neuropathy, proximal myopathy, and cerebellar ataxia (dominant optic atrophy plus syndrome); this multisystem disorder is associated with missense mutations in the GTPase domain.23–25 Muscle biopsy often shows multiple mtDNA deletions and sometimes depletion, ragged red fi bres, and COX-defi cient fi bres. Neuropathy is usually mild, sensorimotor or mostly sensory, and axonal, manifesting as reduced-to-absent deep tendon refl exes, sensory loss, varying ataxia (sensory and cerebellar), and distal muscle wasting and weakness. Pes cavus can be seen. Nerve conduction studies show preserved nerve conduction velocity but reduced compound muscle action potential and sensory action potential amplitudes. Most OPA1 sequence alterations are loss-of-function mutations, but some can have a dominant-negative eff ect, since OPA1 forms homo-oligomers. As with other proteins that cause peripheral neuropathy, OPA1 and MFN2 seem to be associated with mtDNA stability (table 3).
Defects of ATP synthesisNARP syndrome is usually characterised by neuropathy, neurogenic proximal weakness, cerebellar ataxia, and retinitis pigmentosa, with varying extent of supratentorial involvement. MTATP6 mutations, by causing defi cits in ATP produced by complex V of the respiratory chain, cause a range of phenotypes of diff erent severity, including maternally inherited Leigh syndrome.56–60 8993T→G is the most common mutation seen in MTATP6, but other missense changes have been reported, including 8993T→C and 9185T→C. Neuropathy is axonal, mainly sensory, and can manifest as pes cavus, decreased or
absent deep tendon refl exes, distal wasting and weakness, distal sensory loss, and sensory ataxia.57–59 Electrophysiology shows chronic axonal degeneration and reduced sensory action potential amplitudes.10,17,58,59 MTATP6 mutations can manifest as a pure neuropathy. Mild-to-moderate neuropathy was the only manifestation in four individuals from three unrelated families harbouring 9185T→C or 8993T→C mutations;56,59,60 one individual had a previous diagnosis of CMT with ataxia.60 Another family carrying the 8993T→C mutation showed adult-onset, slowly progressive ataxia and polyneuropathy.67 Diagnosis is diffi cult when the clinical picture is incomplete. Furthermore, plasma lactic acid concentrations are not increased and muscle biopsy usually does not show mitochondrial histochemical abnormalities, since MTATP6 is involved in the fi nal step of ATP production in energy coupling.
Leber hereditary optic neuropathy and Kearns-Sayre syndromeLeber hereditary optic neuropathy is associated with mutations in the mitochondrial genes ND1, ND4, and ND6, which encode respiratory chain complex I subunits, and is only very rarely complicated by severe neuropathy that can be demyelinating.18 Peripheral neuropathy can occur in Kearns-Sayre syndrome, which is due to single mtDNA macrodeletions and is characterised by pigmentary retinopathy.10
Gene Diff erential diagnoses
Disorders of mitochondrial dynamics
CMT2 MFN2 Other axonal CMT, other inherited and acquired axonal neuropathies
CMT5 MFN2 Other causes of CMT5 (mutations in BSCL2, GJB1, HSPB1, SETX), complicated hereditary spastic paraplegia, adrenomyeloneuropathy
CMT6 MFN2 LHON, DOA plus
Recessive CMT GDAP1 Other CMT with early onset, CIDP
Dominant CMT GDAP1 Other mild-to-moderate axonal CMT, other inherited and acquired axonal neuropathies
DOA plus OPA1 LHON, CMT6, Wolfram syndrome
Disorders of mtDNA replication and maintenance, and of complex V
NARP MTATP6 Acquired sensory ataxias, AVED, abetalipoproteinaemia, peroxisomal disorders (Refsum and Refsum-like diseases)
CMT2 and dHMN MTATP6 Other axonal CMT and dHMN
SANDO POLG1 Inherited ataxias (Friedreich’s ataxia, AVED, SCA28, etc), CMT, abetalipoproteinaemia, acquired chronic progressive sensory ataxias (ie, Sjoegren syndrome)
SANDO, IOSCA C10ORF2 Inherited ataxias (Friedreich’s ataxia, AVED, SCA28, etc), CMT, abetalipoproteinaemia, acquired chronic progressive sensory ataxias (ie, Sjoegren syndrome)
MNGIE TYMP Leukodystrophies, CIDP, demyelinating CMT
CMT=Charcot-Marie-Tooth neuropathy. LHON=Leber hereditary optic neuropathy. DOA plus=autosomal dominant optic atrophy plus syndrome. CIDP=chronic infl ammatory demyelinating polyradiculoneuropathy. mtDNA=mitochondrial DNA. NARP=neuropathy, ataxia, and retinitis pigmentosa. AVED=ataxia with vitamin E defi ciency. dHMN=distal hereditary motor neuropathy. SCA28=spinocerebellar ataxia type 28. SANDO=sensory ataxia, neuropathy, dysarthria, and ophthalmoplegia. IOSCA=infantile-onset spinocerebellar ataxia. MNGIE=mitochondrial neurogastrointestinal encephalopathy. MILS=maternally inherited Leigh syndrome.
Table 2: Diff erential diagnoses of the main mitochondrial disorders presenting with peripheral neuropathy

1018 www.thelancet.com/neurology Vol 12 October 2013
Review
Sensory ataxic neuropathiesSensory ataxia as an isolated manifestation or, more commonly, in the setting of a more widespread neurological disorder is another possible presentation of a mitochondrial disorder caused by respiratory chain complex V defi cit, as in NARP syndrome, or by defects in mtDNA replication and maintenance, as with mutations in POLG1 and C10ORF2.
POLG1 and C10ORF2 mutationsMutations in the nuclear gene POLG1, which encodes the catalytic subunit of mitochondrial gamma-polymerase involved in mtDNA replication, lead to complex phenotypes that often include peripheral neuropathy, particularly when onset occurs in adolescents or adults.1–3,11 Ataxia neuropathy spectrum encompasses a range of phenotypes associated with
Inheritance Phenotype Pathophysiology Neuropathy
Type Nerve conduction velocities
Severity range Relevance
MFN2 Autosomal dominant much more frequent than recessive
CMT2A, HMSN type V, HMSN type VI
Mitochondrial dynamics
Sensory-motor axonal Normal or slightly decreased
Mild to severe Usually the only feature
GDAP1 Autosomal recessive more frequent than dominant
CMT4A, CMT2K, recessive intermediate CMT
Mitochondrial dynamics
Sensory-motor axonal (with or without secondary demyelinating changes)
Normal or decreased
Autosomal recessive is severe; autosomal dominant is mild to moderate
Usually the only feature
OPA1 Autosomal dominant
DOA plus Mitochondrial dynamics
Sensory-motor axonal Normal or slightly decreased
Subclinical to mild Occurs with other features
MTATP6 Mitochondrial NARP and MILS, CMT2-like and dHMN-like
Oxidative phosphorylation coupling, ATP synthesis
Predominantly sensory axonal; predominantly motor in CMT2-like
Normal or slightly decreased
Moderate to severe Can be the sole or presenting feature
POLG1 Autosomal recessive more frequent than dominant
Alpers-Huttenlocher syndrome, SANDO, MIRAS, MEMSA, MNGIE-like
mtDNA replication and maintenance
Sensory axonal; hypomyelinating when early onset
Normal or slightly decreased
Moderate to severe Can be the sole or presenting feature
C10ORF2 Autosomal dominant or recessive
SANDO, IOSCA, progressive external ophthalmoplegia
mtDNA replication and maintenance
Usually sensory axonal Normal or slightly decreased
Mild or subclinical, rarely severe
Prominent
TYMP Autosomal recessive
MNGIE mtDNA replication and maintenance
Sensory-motor demyelinating Decreased Subclinical to severe
Can be the presenting feature
RRM2B Autosomal recessive
MNGIE-like mtDNA replication and maintenance
Sensory-motor demyelinating Decreased Only one case reported
Occurs with other features
MPV17 Autosomal recessive
Navajo neurohepatopathy mtDNA maintenance
Sensory-motor axonal or demyelinating
Normal or slightly decreased
Severe Substantial feature
MTTL1 3243A→G (and other mitochondrial mutations)
Mitochondrial MELAS Respiratory chain disorder
Sensory-motor predominantly axonal
Normal or decreased
Varies, usually mild Frequently occurs with other fi ndings, rarely severe
MTTK 8344A→G (and other mitochondrial mutations)
Mitochondrial MERRF Respiratory chain disorder
Sensory-motor usually mixed Varies, often decreased
Varies, usually mild, only rarely severe
Frequent but mild and with other fi ndings
mtDNA ND1, ND4, ND6
Mitochondrial LHON Respiratory chain disorder
Sensory-motor and predominantly demyelinating
Slightly decreased Varies, rarely severe
Infrequent
mtDNA large deletion
Mitochondrial Kearns-Sayre syndrome Respiratory chain disorder
Sensory-motor axonal Normal Varies, usually mild Infrequent
SURF1, PDHA1 Autosomal recessive
Leigh syndrome Respiratory chain disorder
Sensory-motor demyelinating Decreased Varies, rarely severe
Infrequent
SLC25A19 Autosomal recessive
Bilateral striatal necrosis mtDNA replication and maintenance
Motor or sensory-motor axonal
Normal Moderate to severe One report
CMT=Charcot-Marie-Tooth neuropathy. HMSN=hereditary motor and sensory neuropathy. DOA plus=autosomal dominant optic atrophy plus syndrome. NARP=neuropathy, ataxia, and retinitis pigmentosa. MILS=maternally inherited Leigh syndrome. dHMN=distal hereditary motor neuropathy. SANDO=sensory ataxia, neuropathy, dysarthria, and ophthalmoplegia. MIRAS=mitochondrial recessive ataxia syndrome. MEMSA=myoclonic epilepsy myopathy sensory ataxia. MNGIE=mitochondrial neurogastrointestinal encephalopathy. mtDNA=mitochondrial DNA. IOSCA=infantile-onset spinocerebellar ataxia. MELAS=mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes. MERRF=myoclonus epilepsy with ragged-red fi bres. LHON=Leber hereditary optic neuropathy.
Table 3: Genetic causes and characteristics of mitochondrial neuropathies in mitochondrial disorders with peripheral nerve involvement

www.thelancet.com/neurology Vol 12 October 2013 1019
Review
POLG1 mutations, including cerebellar and sensory ataxia.11 Sensory ataxic neuropathy, dysarthria, and ophthalmoparesis (SANDO), by defi nition characterised by peripheral neuropathy, is usually inherited as an autosomal recessive trait with juvenile-to-adult onset.11,68,69 The neuropathy is mainly sensory, with ataxia, loss of proprioception and vibration sense, touch and pinprick sensory changes (to a lesser extent), and a varying degree of distal muscle wasting and weakness; pes cavus is sometimes reported. Nerve conduction studies show decreased or absent sensory action potentials and varying motor involvement. Only a few pathology reports are available, showing axonal and dorsal column degeneration, suggesting involvement of dorsal root ganglia.69,70 Hypomyelinating or demyelinating neuropathy are rarely reported and are usually associated with early-onset phenotypes.11,71 Diagnosis can be challenging when onset occurs late, such as in an 80-year-old man who presented with a 7-year history of neurological dysfunction,72 or when neuropathy is the only manifestation for a long period, mimicking CMT, as reported in one family where individuals developed other SANDO features much later.73 Muscle biopsy can show ragged red fi bres, COX-defi cient fi bres, and multiple mtDNA deletions or depletion in the most severe cases; however, in some cases, no mitochondrial abnormalities are found.
Neuropathy can also occur as the result of mutations in another gene involved in mtDNA replication—ie, C10ORF2, which encodes twinkle helicase.12 Aff ected individuals present with dominant or recessive phenotypes that can include progressive external ophthalmoplegia, myopathy, dysarthria, dysphagia, parkinsonism, hearing loss, seizures, dementia, diabetes, and liver damage.2,3,12 Neuropathy is often mild or subclinical. In a few patients it was prominent, with predominant motor involvement in one family,12 and sensory ataxic presentation in other instances,74 including a family with SANDO associated with a heterozygous mutation.75 Multiple mtDNA deletions, ragged red fi bres, and COX-defi cient fi bres are often present and might help to guide diagnosis.
Sensory ataxic neuropathy caused by degeneration of dorsal root ganglia is a key feature of infantile onset spinocerebellar ataxia with sensory neuropathy (IOSCA), a rare autosomal recessive spinocerebellar ataxia of the Finnish population that is associated with C10ORF2 mutations.76 IOSCA is an mtDNA depletion syndrome (hepatocerebral form of MTDPS7), with mtDNA depletion aff ecting the brain and liver.77
Peripheral neuropathy and gastrointestinal manifestationsPeripheral neuropathy has been associated with disrupted gastrointestinal motility in MNGIE13 and with liver disease in Navajo neuro hepatopathy;14 both disorders also show brain white matter abnormalities on MRI.
MNGIE and TYMP mutationsMNGIE is a rare autosomal recessive disease associated with mutations in TYMP, which encodes thymidine phosphorylase, a cytosolic transferase that catalyses the breakdown of thymidine into thymine and deoxyribose-1-phosphate and is involved in mitochondrial nucleotide pool homoeostasis.78 MNGIE combines mtDNA depletion syndrome (MTDPS1) with accumulation of multiple deletions and point mutations. Clinical diagnosis is based on the presence of severe gastrointestinal dysmotility (with pseudo-obstructions), cachexia, ptosis and ophthalmoparesis, demyelinating peripheral neuropathy, and diff use (though generally asymptomatic) leuko-encephalopathy.13,79 Age at onset ranges between 0·5–52 years, although the disease often starts during childhood or adolescence.13,79,80 Progression varies, sometimes with rapid course and often proving lethal between ages 20 and 40 years;13 however, some patients live into their sixties.80 Diagnosis is based on demonstrating substantial decrease in thymidine phosphorylase activity in leucocytes or platelets, increase in thymidine and deoxyuridine urinary excretion and plasma concentrations, and defi nitively by TYMP mutations.13,78,81 Muscle biopsy shows ragged red fi bres and COX-defi cient fi bres in most patients, together with multiple mtDNA deletions, depletion, and point mutations.13,79,81
Peripheral neuropathy is almost always found in MNGIE, and is typically demyelinating with slowed nerve conduction velocities presenting as weakness and wasting that preferentially aff ect distal muscles and as sensory loss. Neuropathy ranges in severity from asymptomatic involvement detected only on nerve conduction studies to rapidly progressive and devastating course.13,79,81–84 Nerve biopsy shows axonal degeneration together with segmental demyelination and remyelination, thinly myelinated internodes, few onion bulbs, and tomacula-like myelin irregularity.81–84 Dystrophic mitochondria, loss of cristae, and occasional paracrystallin inclusions have been seen with electron microscopy.83
Peripheral neuropathy was the onset manifestation in 12% of patients with MNGIE in a large series, and eight of 102 patients were initially misdiagnosed as having chronic infl ammatory demyelinating polyradiculo-neuropathy or CMT.13 Other investigators have also reported a presentation similar to chronic infl ammatory demye linating polyradiculoneuropathy in patients with MNGIE.81,82 Conduction blocks and symptom fl uctuations occur82 and, together with frequent CSF protein increase, contribute to misdiagnosis. In another fi ve cases, the clinical presentation mimicked CMT, with initial (predominantly) sensorimotor demyelinating neuropathy with pes cavus.83,84
The symptoms of MNGIE are an example of a mitochondrial syndrome caused by an mtDNA replication dysfunction that results from an imbalance in the mitochondrial nucleotide pool. Indeed, there is an overload of thymidine and deoxythymidine triphosphate

1020 www.thelancet.com/neurology Vol 12 October 2013
Review
caused by loss-of-function mutations in TYMP. However, mtDNA replication dysfunction is probably due to both thymidine and deoxythymidine triphosphate overload and secondary depletion of deoxycytidine triphosphate. It has been proposed that thymidine and deoxythymidine triphosphate overload might inhibit mitochondrial thymidine kinase 2 thus leading to limited mitochondrial deoxycytidine triphos phate availability—thymidine kinase 2 is a deoxy ribonucleoside kinase that catalyses phosphorylation of intramitochondrial pyrimidine nucleosides, including deoxycytidine, to monophosphate nucleotides (fi gure 1).85
MNGIE-like disordersMNGIE-like phenotypes have occurred in association with recessive POLG186,87 or RRM2B88 mutations; leukoencephalopathy was either absent (POLG1) or patchy (RRM2B), unlike the diff use white matter changes of TYMP-related MNGIE. Neuropathy was demyelinating in a patient carrying RRM2B mutations, whereas patients with POLG1 mutations had mainly sensorimotor axonal87 or sensory ataxic axonal86 neuropathy.
Navajo neurohepatopathy and MPV17Peripheral neuropathy is a main feature of Navajo neurohepatopathy, a rare mtDNA depletion syndrome (MTDPS6) associated with a homozygous recessive mutation (Arg50Trp) in MPV17.14,89 The disease begins in infancy or childhood, and is characterised by liver disease, corneal ulcerations, leukoencephalopathy, and recurrent metabolic acidosis. Aff ected patients develop severe sensorimotor neuropathy with progressive muscle wasting and weakness, loss of deep tendon refl exes, marked sensory defi cit leading to acro mutilations, and corneal anaesthesia. Nerve conduction velocities are slowed. Nerve biopsy shows myelinated fi bre depletion and degenerative changes in unmyelinated fi bres.14 This unusual neuropathic phenotype seems to be limited to the Navajo population of the southwestern USA.14,90 A 21-year-old Pakistani man and a 65-year-old man of European origin carrying other MPV17 recessive mutations developed axonal sensorimotor neuropathy in the context of a multisystem disorder, with multiple mtDNA deletions seen in muscle biopsy.91,92
Peripheral neuropathy in other mitochondrial disordersPeripheral neuropathy occurs in many other syndromic and non-syndromic mitochondrial disorders; however, it only rarely manifests as a predominant feature. Peripheral nerve involvement is common but often subclinical in MELAS syndrome, where it is frequently axonal and predominantly sensory.1–3,10,15 A Guillain-Barrè-syndrome-like neuropathy was reported in one patient with MELAS syndrome.15 Although common, neuropathy is rarely relevant in MERRF syndrome, particularly in patients with multiple lipomas, and is usually demyelinating and
sensorimotor.16 Occasionally prominent neuropathy has been reported in Leber hereditary optic neuropathy,18 Kearns-Sayre syndrome,10 and Leigh syndrome,19 and in primary coenzyme Q10 defi ciency due to ADCK3 mutations, which is usually characterised by cerebellar ataxia sometimes associated with mental retardation, seizures, and peripheral neuropathy.93
Moderate-to-severe progressive motor or sensorimotor axonal neuropathy with foot deformities was reported in four siblings aff ected by bilateral striatal necrosis with recurrent episodes of fl accid paralysis and encepha-lopathy. CSF lactate concentration was elevated but respiratory chain complex activity was normal. Homozygosity mapping led to the identifi cation of a homozygous mutation in SLC25A19, encoding the mitochondrial thiamine pyrophosphate transporter.94
Diagnosis of peripheral neuropathies associated with respiratory chain dysfunctionPeripheral neuropathy in individuals with disrupted mitochondrial dynamics typically presents as CMT, and MTATP6 mutations should be considered in patients with CMT2 or distal hereditary motor neuropathy, particularly when there are mild associated features and inheritance might be matrilineal. Not all patients presenting with pes cavus and sensorimotor neuropathy have CMT, thus MNGIE (when peripheral neuropathy is demyelinating) or POLG1-related disorders (when peripheral neuropathy is axonal) should be considered. Similarly, MNGIE should not be misdiagnosed as chronic infl ammatory demyelinating polyradiculoneuropathy. Sensory ataxia is a possible presentation in mitochondrial disorders and might suggest POLG1-related neuropathy or NARP syndrome. The diff erential diagnosis includes Friedreich’s ataxia and vitamin E defi ciency (table 2).
In patients presenting with peripheral neuropathy, a mitochondrial disorder should be suspected when there are other features, which are sometimes subtle, suggesting mitochondrial dysfunction—eg, ptosis, ophthalmoplegia, gastrointestinal dismotility, cerebellar ataxia, decreased visual acuity, pigmentary retinopathy, hearing loss, and white matter changes on MRI. Lactic acid assay and muscle biopsy to detect ragged red fi bres, COX-defi cient fi bres, respiratory chain complex defi ciency, and mtDNA depletion and deletions can aid diagnosis. Histochemical and biochemical evidence of a mitochondrial disorder are sometimes absent; therefore, physicians must rely on clinical suspicion and look for mutations in common mtDNA hotspots, such as MTATP6, or in nuclear genes, such as POLG1 and OPA1 (table 4).
TreatmentEff ective therapy for mitochondrial diseases is very limited, as noted in a recent Cochrane review.95 Current treatment for mitochondrial diseases is largely supportive and mainly includes vitamins and cofactors supplements—ie, antioxidants (coenzyme Q10,

www.thelancet.com/neurology Vol 12 October 2013 1021
Review
idebenone, vitamin C, vitamin E), respiratory chain cofactors (thiamine, ribofl avin, coenzyme Q10), and compounds that correct secondary biochemical defi ciencies (carnitine, creatine) or improve lactic acidosis (dichloroacetate).3,95
Specifi c treatment is available for only a few diseases. Supplementation can successfully treat primary coenzyme Q10 defi ciency and often improve secondary defi ciencies.96 Platelet infusion transiently restores circulating thymidine phosphorylase and reduces plasma thymidine and deoxyuridine concentrations in patients with MNGIE.96 Allogeneic haemopoietic stem-cell transplantation can potentially halt MNGIE progression, although morbidity and mortality rates are high if general conditions are compromised, thus timely diagnosis is necessary.97 Enzyme replacement therapy (encapsulated in red cell ghosts) might be suitable for patients whose general condition precludes allogenic haemopoietic stem cell transplantation.98 Early and prolonged treatment with idebenone in patients with Leber hereditary optic neuropathy improved the frequency of visual recovery and possibly changed the natural history;99 a small pilot trial of idebenone for dominant optic atrophy reported some improvement in visual function.100 Gene therapies (gene insertion or shifting, and nuclear transfer) are being tested in cellular and animal models of hereditary optic neuropathies and other mitochondrial disorders.101,102 An open-label trial with EPI-743 (a third-generation quinone molecule) recently showed possible halting of disease progression in Leigh syndrome and Leber hereditary optic neuropathy.103 L-arginine seems to be a promising treatment for stroke-like episodes in MELAS syndrome.95 Some studies have reported increased muscle strength with aerobic exercise and resistance training in adults with myopathies caused by single, large-scale mtDNA deletions; these results support the hypothesis of exercise-induced mitochondrial gene shifting in muscle-containing satellite cells that have low or absent levels of deleted mtDNA and encourage further investigations in treating sporadic mtDNA diseases.95
Currently, there is no evidence of specifi c eff ects with any treatment for peripheral neuropathy related to a mitochondrial disorder; conversely, peripheral nerve toxicity occurred after dichloroacetate treatment in patients with the 3243A→G mutation in MTTL1.95 In a series of patients with MNGIE, one patient given an allogenic haemopoietic stem cell transplantation showed clinically and electrophysiologically improved neuro-pathy.96 High-dose coenzyme Q10 was administered to improve optic neuropathy in a patient with an MFN2 mutation, but it did not change the course of peripheral neuropathy.104 There are no data on treatment effi cacy on peripheral nerves in patients with coenzyme Q10 defi ciencies.96 Trials with treatment cocktails including coenzyme Q10, creatine, and lipoic acid in patients with MELAS syndrome did not report on effi cacy in peripheral neuropathy, although such treatments attenuated the
decline in ankle dorsifl exion strength.95 There are no data on possible treatments for mitochondrial diseases in which neuropathy represents a major manifestation, such as NARP syndrome, SANDO, and dominant optic atrophy; however, it is common practice to off er treatment with coenzyme Q10, often combined with thiamine, ribofl avin, and vitamin C, mostly to children with a proven diagnosis of a mitochondrial disorder.
Conclusion and future directionsWe reviewed mitochondrial disorders where peripheral neuropathy is a key feature. Peripheral neuropathy as a unique or predominant fi nding is frequent in disorders aff ecting mitochondrial dynamics, where abnormal mitochondrial transport along axons seems to be the main pathological mechanism and neuropathy presents as CMT. Novel MFN2-related phenotypes are emerging and resemble the complex clinical scenarios of dominant optic atrophy plus syndrome and other mitochondrial disorders. Indeed, peripheral neuropathy might be the only or main presenting feature of some disorders of mtDNA replication and maintenance, and of specifi c disorders of the respiratory chain, including ATP-synthase defects. The number of genes and phenotypes associated with mitochondrial disorders is rapidly expanding. The availability of novel genetic techniques, including whole
Associated genes and diagnoses
Axonal CMT MFN2 and CMT2A; GDAP1 and autosomal dominant or autosomal recessive CMT2K; MTATP6 and CMT2 or NARP; POLG1 and SANDO
Demyelinating CMT and neuropathy
GDAP1 and autosomal recessive CMT4A, or recessive intermediate CMT; TYMP (and RRM2B) and MNGIE; MPV17 and Navajo neurohepatopathy; MERRF
Neuropathy plus visual loss
Optic atrophy MFN2 and CMT6; OPA1 and DOA plus; ND1, ND4, ND6 and LHON
Retinopathy MTATP6 and NARP; Kearns-Sayre syndrome
Neuropathy plus pyramidal involvement
MFN2 and CMT5
Pure motor neuropathy with or without other neurological features
MTATP6
Sensory ataxic neuropathy POLG1, C10ORF2 and SANDO, ataxia neuropathy spectrum; C10ORF2 and IOSCA; MTATP6 and NARP
Predominantly sensory neuropathy with acromutilation
MPV17 and Navajo neurohepatopathy
Axonal neuropathy with CNS involvement
MELAS, MERRF, Kearns-Sayre syndrome, Leigh syndrome, MILS
Neuropathy with gastrointestinal manifestations
TYMP (RRM2B, POLG1) and MNGIE; MPV17 and Navajo neurohepatopathy and related disorders
Neuropathy with leukoencephalopathy
TYMP (RRM2B, POLG1) and MNGIE; MPV17 and Navajo neurohepatopathy and related disorders; Kearns-Sayre syndrome, Leigh syndrome, MELAS
CMT=Charcot-Marie-Tooth neuropathy. dHMN=distal hereditary motor neuropathy. NARP=neuropathy, ataxia, and retinitis pigmentosa. SANDO=sensory ataxia, neuropathy, dysarthria, and ophthalmoplegia. MNGIE=mitochondrial neurogastrointestinal encephalopathy. MERRF=myoclonus epilepsy with ragged-red fi bres. DOA plus=autosomal dominant optic atrophy plus syndrome. LHON=Leber hereditary optic neuropathy. IOSCA=infantile-onset spinocerebellar ataxia. MELAS=mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes. MILS=maternally inherited Leigh syndrome.
Table 4: Associated genes and diagnoses according to neuropathic presentation

1022 www.thelancet.com/neurology Vol 12 October 2013
Review
exome sequencing, will allow detection of other diseases characterised by mitochondrial dysfunction and prominent or exclusive peripheral neuropathy. Growing knowledge of the pathological mechanisms is leading to development of treatment options for some mitochondrial disorders. Thus, the list of treatable disorders will increase, as will the need for early diagnosis. Finally, preimplantation genetic testing raises hopes that prevention of human mtDNA disease transmission is feasible;105 however, successful translation to clinical practice requires further research to test safety and effi cacy, and remains controversial for ethical concerns.105
ContributorsDP designed and wrote the Review, did the literature search, and
designed the tables. GP helped to write the Review and do the literature
search, and collaborated on designing and preparing the tables. IM
wrote part of the Review, helped to do the literature search, and
collaborated on designing fi gures and tables. ES helped to write the
Review and collaborated on designing and preparing fi gures and tables.
MZ gave intellectual contribution and reviewed the manuscript.
Confl icts of interestDP received research funding from ACMT-Rete and Pfi zer Italia, and
travel expenses from Kedrion SpA and Pfi zer Italia. GP received travel
expenses from Pfi zer Italia. ES received travel expenses from Actelion
Pharmaceuticals. All other authors reported no confl icts of interest.
AcknowledgmentsOur work was supported by Telethon Italy grants GPP10005 and
GGP11011 (to MZ). DP is a member of the Inherited Neuropathy
Consortium Rare Disease Clinical Research Consortium funded by the
US National Institutes of Health (NINDS/ORD), Muscular Dystrophy
Association, and Charcot-Marie-Tooth Association (CMTA).We thank
Tiziana Cavallaro and Gian Maria Fabrizi for nerve biopsy material and
for preparing fi gure 2, and Michela Morbin for nerve biopsy material
and for help preparing fi gures 2 and 3.
Ref erences1 Finsterer J. Mitochondrial neuropathy. Clin Neurol Neurosurg 2005;
107: 181–86.
2 McFarland R, Taylor RW, Turnbull DM. A neurological perspective on mitochondrial disease. Lancet Neurol 2010; 9: 829–40.
3 Rahman S, Hanna MG. Diagnosis and therapy in neuromuscular disorders: diagnosis and new treatments in mitochondrial diseases. J Neurol Neurosurg Psychiatry 2009; 80: 943–53.
4 Detmer SA, Chan DC. Functions and dysfunctions of mitochondrial dynamics. Nat Rev Mol Cell Biol 2007; 8: 870–79.
5 Milone M, Benarroch EE. Mitochondrial dynamics: general concepts and clinical implications. Neurology 2012; 78: 1612–29.
6 Niemann A, Wagner KM, Ruegg M, Suter U. GDAP1 mutations diff er in their eff ects on mitochondrial dynamics and apoptosis depending on the mode of inheritance. Neurobiol Dis 2009; 36: 509–20.
7 Züchner S, Mersiyanova IV, Muglia M, et al. Mutations in the mitochondrial GTPase mitofusin 2 cause Charcot-Marie-Tooth neuropathy type 2A. Nat Genet 2004; 36: 449–51.
8 Baxter RV, Ben Othmane K, Rochelle JM, et al. Ganglioside-induced diff erentiation-associated protein-1 is mutant in Charcot-Marie-Tooth disease type 4A/8q21. Nat Genet 2002; 30: 21–22.
9 Cuesta A, Pedrola L, Sevilla T, et al. The gene encoding ganglioside-induced diff erentiation-associated protein 1 is mutated in axonal Charcot-Marie-Tooth type 4A disease. Nat Genet 2002; 30: 22–25.
10 Finsterer J. Inherited mitochondrial neuropathies. J Neurol Sci 2011; 304: 9–16.
11 Milone M, Massie R. Polymerase gamma 1 mutations: clinical correlations. Neurologist 2010; 16: 84–91.
12 Martin-Negrier ML, Sole G, Jardel C, Vital C, Ferrer X, Vital A. TWINKLE gene mutation: report of a French family with an autosomal dominant progressive external ophthalmoplegia and literature review. Eur J Neurol 2011; 18: 436–41.
13 Garone C, Tadesse S, Hirano M. Clinical and genetic spectrum of mitochondrial neurogastrointestinal encephalomyopathy. Brain 2011; 134: 3326–32.
14 Karadimas CL, Vu TH, Holve SA, et al. Navajo neurohepatopathy is caused by a mutation in the MPV17 gene. Am J Hum Genet 2006; 79: 544–48.
15 Hanna MG, Cadia P. Pheripheral nerve diseases associated with mitochondrial respiratory chain dysfunction. In: Dyck PJ, Thomas PK, eds. Peripheral neuropathy, 4th edn. Philadelphia: Elsevier Saunders, 2005: 1937–49.
16 Bouillot S, Martin-Négrier ML, Vital A, et al. Peripheral neuropathy associated with mitochondrial disorders: 8 cases and review of the literature. J Peripher Nerv Syst 2002; 7: 213–20.
17 Menezes MP, Ouvrier RA. Peripheral neuropathy associated with mitochondrial disease in children. Dev Med Child Neurol 2012; 54: 407–14.
18 Gilhuis HJ, Schelhaas HJ, Cruysberg JR, Zwarts MJ. Demyelinating polyneuropathy in Leber hereditary optic neuropathy. Neuromuscul Disord 2006; 16: 394–95.
19 Santoro L, Carrozzo R, Malandrini A, et al. A novel SURF1 mutation results in Leigh syndrome with peripheral neuropathy caused by cytochrome C oxidase defi ciency. Neuromuscul Disord 2000; 10: 450–53.
20 Rusanen H, Majamaa K, Tolonen U, Remes AM, Myllylä R, Hassinen IE. Demyelinating polyneuropathy in a patient with the tRNA (Leu)(UUR) mutation at base pair 3243 of the mitochondrial DNA. Neurology 1995; 45: 1188–92.
21 Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol 2009; 8: 654–67.
22 Reilly MM, Murphy SM, Laurá M. Charcot-Marie-Tooth disease. J Peripher Nerv Syst 2011; 16: 1–14.
23 Yu-Wai-Man P, Griffi ths PG, Gorman GS, et al. Multi-system neurological disease is common in patients with OPA1 mutations. Brain 2010; 133: 771–86.
24 Amati-Bonneau P, Valentino ML, Reynier P, et al. OPA1 mutations induce mitochondrial DNA instability and optic atrophy ‘plus’ phenotypes. Brain 2008; 131: 338–51.
25 Hudson G, Amati-Bonneau P, Blakely EL, et al. Mutation of OPA1 causes dominant optic atrophy with external ophthalmoplegia, ataxia, deafness and multiple mitochondrial DNA deletions: a novel disorder of mtDNA maintenance. Brain 2008; 131: 329–37.
26 Cartoni R, Martinou JC. Role of mitofusin 2 mutations in the physiopathology of Charcot-Marie-Tooth disease type 2A. Exp Neurol 2009; 218: 268–73.
27 Misko AL, Sasaki Y, Tuck E, Milbrandt J, Baloh RH. Mitofusin 2 mutations disrupt axonal mitochondrial positioning and promote axon degeneration. J Neurosci 2012; 32: 4145–55.
28 Züchner S, De Jonghe P, Jordanova A, et al. Axonal neuropathy with optic atrophy is caused by mutations in mitofusin 2. Ann Neurol 2006; 59: 276–81.
29 Verhoeven K, Claeys KG, Züchner S, et al. MFN2 mutation distribution and genotype/phenotype correlation in Charcot-Marie-Tooth type 2. Brain 2006; 129: 2093–102.
30 Chung KW, Kim SB, Park KD, et al. Early onset severe and late-onset mild Charcot-Marie-Tooth disease with mitofusin 2 (MFN2) mutations. Brain 2006; 129: 2103–18.
Search strategy and selection criteria
References for this Review were identifi ed by searches of PubMed from Jan 1, 1989, until May 31, 2013, with the terms “peripheral neuropathy and mitochondria/mitochondrial disease”, “Charcot-Marie-Tooth”, “DOA”, “HMSN”, “HMSN V”, “HMSN VI”, “IOSCA”, “Leber optic atrophy”, “Leigh syndrome”, “LHON”, “MILS”, “MNGIE”, “NARP”, “SANDO”, “C10ORF2”, “GDAP1”, “MFN2”, “MPV17”, “OPA1”, “PEO1”, “POLG1”, “SURF1”, “TYMP”, “Twinkle”, “mitochondrial disease and therapy”. Articles were also identifi ed through searches of the authors’ own fi les. Only reports published in English or French were reviewed. Selection criteria were newness, ease of access, importance, originality, quality, relevance to the scope of this Review, and opportunities for further references.

www.thelancet.com/neurology Vol 12 October 2013 1023
Review
31 Feely SM, Laura M, Siskind CE, et al. MFN2 mutations cause severe phenotypes in most patients with CMT2A. Neurology 2011; 76: 1690–96.
32 Saporta AS, Sottile SL, Miller LJ, Feely SM, Siskind CE, Shy ME. Charcot-Marie-Tooth disease subtypes and genetic testing strategies. Ann Neurol 2011; 69: 22–33.
33 Murphy SM, Laura M, Fawcett K, et al. Charcot-Marie-Tooth disease: frequency of genetic subtypes and guidelines for genetic testing. J Neurol Neurosurg Psychiatry 2012; 83: 706–10.
34 Calvo J, Funalot B, Ouvrier RA, et al. Genotype-phenotype correlations in Charcot-Marie-Tooth disease type 2 caused by mitofusin 2 mutations. Arch Neurol 2009; 66: 1511–16.
35 Vital A, Vital C. Mitochondria and peripheral neuropathies. J Neuropathol Exp Neurol 2012; 71: 1036–46
36 Banchs I, Casasnovas C, Montero J, Martínez-Matos JA, Volpini V. Two Spanish families with Charcot-Marie-Tooth type 2A: clinical, electrophysiological and molecular fi ndings. Neuromuscul Disord 2008; 18: 974–78.
37 Zhu D, Kennerson ML, Walizada G, Züchner S, Vance JM, Nicholson GA. Charcot-Marie-Tooth with pyramidal signs is genetically heterogeneous: families with and without MFN2 mutations. Neurology 2005; 65: 496–97.
38 Del Bo R, Moggio M, Rango M, et al. Mutated mitofusin 2 presents with intrafamilial variability and brain mitochondrial dysfunction. Neurology 2008; 71: 1959–66.
39 Chung KW, Suh BC, Cho SY, et al. Early-onset Charcot-Marie-Tooth patients with mitofusin 2 mutations and brain involvement. J Neurol Neurosurg Psychiatry 2010; 81: 1203–06.
40 Brockmann K, Dreha-Kulaczewski S, Dechent P, et al. Cerebral involvement in axonal Charcot-Marie-Tooth neuropathy caused by mitofusin 2 mutations. J Neurol 2008; 255: 1049–58.
41 Nicholson GA, Magdelaine C, Zhu D, et al. Severe early-onset axonal neuropathy with homozygous and compound heterozygous MFN2 mutations. Neurology 2008; 70: 1678–81.
42 Polke JM, Laurá M, Pareyson D, et al. Recessive axonal Charcot-Marie-Tooth disease due to compound heterozygous mitofusin 2 mutations. Neurology 2011; 77: 168–73.
43 Boaretto F, Vettori A, Casarin A, et al. Severe CMT type 2 with fatal encephalopathy associated with a novel MFN2 splicing mutation. Neurology 2010; 74: 1919–21.
44 Rouzier C, Bannwarth S, Chaussenot A, et al. The MFN2 gene is responsible for mitochondrial DNA instability and optic atrophy ‘plus’ phenotype. Brain 2012; 135: 23–34.
45 Renaldo F, Amati-Bonneau P, Slama A, et al. MFN2, a new gene responsible for mitochondrial DNA depletion. Brain 2012; 135: e223.
46 Cassereau J, Chevrollier A, Gueguen N, et al. Mitochondrial dysfunction and pathophysiology of Charcot-Marie-Tooth disease involving GDAP1 mutations. Exp Neurol 2011; 227: 31–41.
47 Pedrola L, Espert A, Valdés-Sánchez T, et al. Cell expression of GDAP1 in the nervous system and pathogenesis of Charcot-Marie-Tooth type 4A disease. J Cell Mol Med 2008; 12: 679–89.
48 Nelis E, Erdem S, Van Den Bergh PY, et al. Mutations in GDAP1: autosomal recessive CMT with demyelination and axonopathy. Neurology 2002; 59: 1865–72.
49 Moroni I, Morbin M, Milani M, et al. Novel mutations in the GDAP1 gene in patients aff ected with early-onset axonal Charcot-Marie-Tooth type 4A. Neuromuscul Disord 2009; 19: 476–80.
50 Sevilla T, Jaijo T, Nauff al D, et al. Vocal cord paresis and diaphragmatic dysfunction are severe and frequent symptoms of GDAP1-associated neuropathy. Brain 2008; 131: 3051–61.
51 Cassereau J, Chevrollier A, Bonneau D, et al. A locus-specifi c database for mutations in GDAP1 allows analysis of genotype-phenotype correlations in Charcot-Marie-Tooth diseases type 4A and 2K. Orphanet J Rare Dis 2011; 6: 87.
52 Zimoń M, Baets J, Fabrizi GM, et al. Dominant GDAP1 mutations cause predominantly mild CMT phenotypes. Neurology 2011; 77: 540–48.
53 Sivera R, Espinós C, Vílchez JJ, et al. Phenotypical features of the p.R120W mutation in the GDAP1 gene causing autosomal dominant Charcot-Marie-Tooth disease. J Peripher Nerv Syst 2010; 15: 334–44.
54 Cassereau J, Casasnovas C, Gueguen N, et al. Simultaneous MFN2 and GDAP1 mutations cause major mitochondrial defects in a patient with CMT. Neurology 2011; 76: 1524–26.
55 Vital A, Latour P, Sole G, et al. A French family with Charcot-Marie-Tooth disease related to simultaneous heterozygous MFN2 and GDAP1 mutations. Neuromuscul Disord 2012; 22: 735–41.
56 Sciacco M, Prelle A, D’Adda E, et al. Familial mtDNA T8993C transition causing both the NARP and the MILS phenotype in the same generation. A morphological, genetic and spectroscopic study. J Neurol 2003; 250: 1498–500.
57 Uziel G, Moroni I, Lamantea E, et al. Mitochondrial disease associated with the T8993G mutation of the mitochondrial ATPase 6 gene: a clinical, biochemical, and molecular study in six families. J Neurol Neurosurg Psychiatry 1997; 63: 16–22.
58 Rojo A, Campos Y, Sánchez JM, et al. NARP-MILS syndrome caused by 8993 T>G mitochondrial DNA mutation: a clinical, genetic and neuropathological study. Acta Neuropathol 2006; 111: 610–16.
59 Childs AM, Hutchin T, Pysden K, et al. Variable phenotype including Leigh syndrome with a 9185T>C mutation in the MTATP6 gene. Neuropediatrics 2007; 38: 313–16.
60 Castagna AE, Addis J, McInnes RR, et al. Late onset Leigh syndrome and ataxia due to a T to C mutation at bp 9,185 of mitochondrial DNA. Am J Med Genet A 2007; 143: 808–16.
61 Craig K, Elliott HR, Keers SM, et al. Episodic ataxia and hemiplegia caused by the 8993T>C mitochondrial DNA mutation. J Med Genet 2007; 44: 797–99.
62 Pitceathly RD, Murphy SM, Cottenie E, et al. Genetic dysfunction of MT-ATP6 causes axonal Charcot-Marie-Tooth disease. Neurology 2012; 79: 1145–54.
63 Synofzik M, Schicks J, Wilhelm C, Bornemann A, Schöls L. Charcot-Marie-Tooth hereditary neuropathy due to a mitochondrial ATP6 mutation. Eur J Neurol 2012; 19: e114–16.
64 Xu WY, Gu MM, Sun LH, et al. A nonsense mutation in DHTKD1 causes Charcot-Marie-Tooth disease type 2 in a large Chinese pedigree. Am J Hum Genet 2012; 91: 1088–94.
65 Rinaldi C, Grunseich C, Sevrioukova IF, et al. Cowchock syndrome is associated with a mutation in apoptosis-inducing factor. Am J Hum Genet 2012; 91: 1095–102.
66 Kennerson ML, Yiu EM, Chuang DT, et al. A new locus for X-linked dominant Charcot-Marie-Tooth disease (CMTX6) is caused by mutations in the pyruvate dehydrogenase kinase isoenzyme 3 (PDK3) gene. Hum Mol Genet 2013; 22: 1404–16.
67 Rantamäki MT, Soini HK, Finnilä SM, Majamaa K, Udd B. Adult-onset ataxia and polyneuropathy caused by mitochondrial 8993T→C mutation. Ann Neurol 2005; 58: 337–40.
68 Van Goethem G, Mercelis R, Löfgren A, et al. Patient homozygous for a recessive POLG mutation presents with features of MERRF. Neurology 2003; 61: 1811–13.
69 Van Goethem G, Luoma P, Rantamäki M, et al. POLG mutations in neurodegenerative disorders with ataxia but no muscle involvement. Neurology 2004; 63: 1251–57.
70 Hopkins SE, Somoza A, Gilbert DL. Rare autosomal dominant POLG1 mutation in a family with metabolic strokes, posterior column spinal degeneration, and multi-endocrine disease. J Child Neurol 2010; 25: 752–56.
71 Winterthun S, Ferrari G, He L, et al. Autosomal recessive mitochondrial ataxic syndrome due to mitochondrial polymerase gamma mutations. Neurology 2005; 64: 1204–48.
72 Weiss MD, Saneto RP. Sensory ataxic neuropathy with dysarthria and ophthalmoparesis (SANDO) in late life due to compound heterozygous POLG mutations. Muscle Nerve 2010; 41: 882–85.
73 Harrower T, Stewart JD, Hudson G, et al. POLG1 mutations manifesting as autosomal recessive axonal Charcot-Marie-Tooth disease. Arch Neurol 2008; 65: 133–36.
74 Van Hove JL, Cunningham V, Rice C, et al. Finding twinkle in the eyes of a 71-year-old lady: a case report and review of the genotypic and phenotypic spectrum of TWINKLE-related dominant disease. Am J Med Genet A 2009; 149A: 861–67.
75 Hudson G, Deschauer M, Busse K, Zierz S, Chinnery PF. Sensory ataxic neuropathy due to a novel C10Orf2 mutation with probable germline mosaicism. Neurology 2005; 64: 371–73.
76 Nikali K, Suomalainen A, Saharinen J, et al. Infantile onset spinocerebellar ataxia is caused by recessive mutations in mitochondrial proteins Twinkle and Twinky. Hum Mol Genet 2005; 14: 2981–90.

1024 www.thelancet.com/neurology Vol 12 October 2013
Review
77 Hakonen AH, Goff art S, Marjavaara S, et al. Infantile-onset spinocerebellar ataxia and mitochondrial recessive ataxia syndrome are associated with neuronal complex I defect and mtDNA depletion. Hum Molec Genet 2008; 17: 3822–35
78 Nishino I, Spinazzola A, Hirano M. Thymidine phosphorylase gene mutations in MNGIE, a human mitochondrial disorder. Science 1999; 283: 689–92.
79 Nishino I, Spinazzola A, Papadimitriou A, et al. Mitochondrial neurogastrointestinal encephalomyopathy: an autosomal recessive disorder due to thymidine phosphorylase mutations. Ann Neurol 2000; 47: 792–800.
80 Martí R, Verschuuren JJ, Buchman A, et al. Late-onset MNGIE due to partial loss of thymidine phosphorylase activity. Ann Neurol 2005; 58: 649–52.
81 Filosto M, Scarpelli M, Tonin P, et al. Pitfalls in diagnosing mitochondrial neurogastrointestinal encephalomyopathy. J Inherit Metab Dis 2011; 34: 1199–203.
82 Bedlack RS, Vu T, Hammans S, et al. MNGIE neuropathy: fi ve cases mimicking chronic infl ammatory demyelinating polyneuropathy. Muscle Nerve 2004; 29: 364–68.
83 Said G, Lacroix C, Planté-Bordeneuve V, et al. Clinico-pathological aspects of the neuropathy of neurogastrointestinal encephalomyopathy (MNGIE) in four patients including two with a Charcot-Marie-Tooth presentation. J Neurol 2005; 252: 655–62.
84 Needham M, Duley J, Hammond S, Herkes GK, Hirano M, Sue CM. Mitochondrial disease mimicking Charcot-Marie Tooth disease. J Neurol Neurosurg Psychiatry 2007; 78: 99–100.
85 González-Vioque E, Torres-Torronteras J, Andreu AL, et al. Limited dCTP availability accounts for mitochondrial DNA depletion in mitochondrial neurogastrointestinal encephalomyopathy (MNGIE). PLoS Genet 2011; 7: e1002035.
86 Van Goethem G, Schwartz M, Löfgren A, Dermaut B, Van Broeckhoven C, Vissing J. Novel POLG mutations in progressive external ophthalmoplegia mimicking mitochondrial neurogastrointestinal encephalomyopathy. Eur J Hum Genet 2003; 11: 547–49.
87 Tang S, Dimberg EL, Milone M, Wong LJ. Mitochondrial neurogastrointestinal encephalomyopathy (MNGIE)-like phenotype: an expanded clinical spectrum of POLG1 mutations. J Neurol 2012; 259: 862–68.
88 Shaibani A, Shchelochkov OA, Zhang S, et al. Mitochondrial neurogastrointestinal encephalopathy due to mutations in RRM2B. Arch Neurol 2009; 66: 1028–32.
89 Spinazzola A, Viscomi C, Fernandez-Vizarra E, et al. MPV17 encodes an inner mitochondrial membrane protein and is mutated in infantile hepatic mitochondrial DNA depletion. Nat Genet 2006; 38: 570–75.
90 Spinazzola A, Santer R, Akman OH, et al. Hepatocerebral form of mitochondrial DNA depletion syndrome: novel MPV17 mutations. Arch Neurol 2008; 65: 1108–13.
91 Blakely EL, Butterworth A, Hadden RD, et al. MPV17 mutation causes neuropathy and leukoencephalopathy with multiple mtDNA deletions in muscle. Neuromuscul Disord 2012; 22: 587–91.
92 Garone C, Rubio JC, Calvo SE, et al. MPV17 mutations causing adult-onset multisystemic disorder with multiple mitochondrial DNA deletions. Arch Neurol 2012; 69: 1648–51.
93 Emmanuele V, López LC, Berardo A, et al. Heterogeneity of coenzyme Q10 defi ciency: patient study and literature review. Arch Neurol 2012; 69: 978–83.
94 Spiegel R, Shaag A, Edvardson S, et al. SLC25A19 mutation as a cause of neuropathy and bilateral striatal necrosis. Ann Neurol 2009; 66: 419–24.
95 Pfeff er G, Majamaa K, Turnbull DM, Thorburn D, Chinnery PF. Treatment for mitochondrial disorders. Cochrane Database Syst Rev 2012; 4: CD004426.
96 Hirano M, Garone C, Quinzii CM. CoQ10 defi ciencies and MNGIE: two treatable mitochondrial disorders. Biochim Biophys Acta 2012; 1820: 625–31.
97 Halter J, Schüpbach WM, Casali C, et al. Allogeneic hematopoietic SCT as treatment option for patients with mitochondrial neurogastrointestinal encephalomyopathy (MNGIE): a consensus conference proposal for a standardized approach. Bone Marrow Transplant 2011; 46: 330–37.
98 Moran NF, Bain MD, Muqit MM, Bax BE. Carrier erythrocyte entrapped thymidine phosphorylase therapy for MNGIE. Neurology 2008; 71: 686–88.
99 Klopstock T, Metz G, Yu-Wai-Man P, et al. Persistence of the treatment eff ect of idebenone in Leber’s hereditary optic neuropathy. Brain 2013; 136: e230.
100 Barboni P, Valentino ML, La Morgia C, et al. Idebenone treatment in patients with OPA1-mutant dominant optic atrophy. Brain 2013; 136: e231.
101 Carelli V, La Morgia C, Sadun AA. Mitochondrial dysfunction in optic neuropathies: animal models and therapeutic options. Curr Opin Neurol 2013; 26: 52–58.
102 Adhya S, Mahato B, Jash S, Koley S, Dhar G, Chowdhury T. Mitochondrial gene therapy: the tortuous path from bench to bedside. Mitochondrion 2011; 11: 839–44.
103 Martinelli D, Catteruccia M, Piemonte F, et al. EPI-743 reverses the progression of the pediatric mitochondrial disease-genetically defi ned Leigh Syndrome. Mol Gen Metab 2012; 107: 383–88.
104 Takahashi R, Tokuhei I, Hamaguchi A, Iwasa K, Yamada M. Coenzyme Q10 therapy in hereditary motor and sensory neuropathy type VI with novel mitofusin 2 mutation. Intern Med 2012; 51: 791–93.
105 Craven L, Elson JL, Irving L, et al. Mitochondrial DNA disease: new options for prevention. Hum Mol Genet 2011; 20: 168–74.