Embed Size (px)
Citation preview

Transfus. Sci. 1993; 14:65-69 09X%3886/93 $6.00+0.00 Printed in Great Britain Perzamon Press Ltd
Peripheral Blood Stem Cell Transplantation for Breast Cancer
Patients With Bone Marrow Metastases Using GM-CSF
Priming Jeane P. Hester, MD
Ralph 0. Wallerstein, MD*
H Twenty-seven patients with metas- tastic breast cancer to the bone marrow underwent successful collection of peripheral blood progenitor cells (PBPC) following GM-CSF cytokine priming and were engrafted following courses of high- dose chemotherapy. Myeloid engraft- ment was observed in a median of 12 days, with a range of 8-29 days. The cell dose infused correlated, although weakly, with days to engraftment, although assays of CFU-GM and CD34+ cells did not, suggesting refinement in such assays is needed. The failure to observe complete remission of the tumor suggests alternative chemotherapy reg- iments should be investigated. n
INTRODUCTION
High-dose chemotherapy/autologous transplantation protocols have demons- trated efficacy of using progenitor cell- rich mononuclear cell fractions collected from peripheral blood as the source of transplant material. It has not been clearly established, however, whether a transplantable quantity of peripheral
Section of Aphcresis, Department of Hematology, Divi- sion of Medicine, The University of Texas, M. D. Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX 77030, and ‘Department of Internal Medicine, Kaiser Pennanente Co
‘t’p ration,
ster, CO 80234, .S.A. 11245 Huron Street, Westmin-
65
blood progenitor cells (PBPC) can be collected from patients with tumor infiltration of the bone marrow and whether there is, or is not, any inhibition of engraftment when these cells are returned to a compromized marrow environment.
The study reports the hematopoietic response to rhGM-CSF of 27 breast can- cer patients with bone marrow metas- tases, the subsequent collection and re- infusion of PBPC following high-dose chemotherapy.
METHODS
Patient Population
Thirty-four female patients, who were candidates for high-dose chemotherapy/ transplantation protocols were referred for collection of PBPC, as the presence of bone marrow metastases precluded har- vesting pelvic bone marrow. All patients had received a course of chemotherapy within 3-8 weeks of collection of PBPC. The median age of these patients was 42 years, with a range of 31-58 years.
Cytokine Priming for PBPC Collections
Recombinant granulocyte-macrophage colony stimulating factor (rhGM-CSF) was infused intravenously over a 4 h period, at a dose of 0.5 mg/mVday, begin-

66 7’runsfus. Sci. Vol. 14, No. 1
ning 3 days prior to PBPC collection and continuing until the end of PBPC collec- tion.
PBPC Collection
A Quinton double-lumen catheter was placed in one subclavian vein prior to PBPC collection. Patient blood volume (BV) were calculated from height, weight, sex,’ and two times the BV was processed per collection. Acid Citrate Dextrose-A (ACD-A) was used at a 1: 10 AC:WB ratio for patients with platelet counts below lx lO”/liter; 1:9 for platelet counts between 1 and 3x loll/L, and 1:8 for platelet counts 3x loll/L. ACD-A was infused at flow rates of 1.4xBV so that the procedure time could be restricted to 3 h or less. Because this ACD-A flow rate was 40% greater than standard, con- tinuous calcium replacement was given in a peripheral vein. PBPC collections were performed daily on continuous flow cell separation devices (COBE Spectra or Fenwal CS3000) until 4x108 small mononuclear (S-MNC) cells/kg had been collected. S-MNC were defined by Wright stained differentials and were roughly equivalent to the peripheral blood lymphocyte population.
Progenitor Cell Assays
Ahquots of MNC concentrates were monocyte-depleted by adherence, and non-adherent cells were plated at 1 x 105 viable cells/soft agar + conditioned media, incubated x 14 days at 37°C in a 5% CO, chamber (Queue), then exami- ned for colonies. Calculations of total CFU-GM were made from the number of colonies/105 plated cells x total number of S-MNC collected. Aliquots were also submitted for immunophenotyping for CD34+ cells by flow cytometry methods.
Cryopreservation and Post-thaw Processing
PBPC were cryopreserved in autologous plasma with a final concentration of
Dimethyl Sulfoxide of 5%, in 100 mL bags (Stericon) in a controlled rate freezer (CryoMed), and stored at - 135°C in a mechanical freezer (Queue). Post-thaw (37°C waterbath x 10min). Cells were pooled into a 3.0 L bag (PL-732 Life Cell Culture), diluted with equal volumes of saline and processed on the CS3000 to remove cell debris (erythrocyte/ leukocyte), DMSO, and excess volume,2 proving a final infusion volume of 20& 400mL. Infusions of PBPC were given 7 days post-chemotherapy.
Chemotherapy/Transplant
Ten patients received two transplants with PBPC. For course no. 1, patients were treated with cytoxan 2 g/m2 daily x 3; VP-16 200mg/m2 every 12 h for 6 doses, and cisplatinum 55 mg/m2 daily x 3. For course no. 2, they received mitox- antrone 50 mg/m2 x 1 dose, and thiotepa 300mg/m2 daily x3 days. Seventeen patients received a single course of high- dose chemotherapy, consisting of cyto- xan 2 g/m2 daily x 3 days, BCNU 150 mg/ m2 daily ~3; and thiotepa 200mg/m2 daily x3. Seven patients received no transplant, as tumor progression occur- red prior to the planned therapy.
RESULTS
A median of 10 leukaphereses were per- formed (range 6-15), yielding a mean of 86x 109+11 total leukocytes (WBC), of which 42x 109+10 were S-MNC and 37+7 were large monocytes or mac- rophages (L-MNC). The capability of the bone marrow to respond to GM-CSF stimulation can be reflected in the changes in peripheral blood WBC and platelets during PBPC collection. As shown in Table 1, the maximum concen- tration of WBC rose to levels approxi- mately three times higher than the ini- tial WBC concentration, but was highly variable. The majority of peripheral blood WBC were granulocytes, metamy- elocytes, eosinophils and monocytes, but a few myelocytes, promyelocytes, and rarely blasts. The S-MNC fraction aver-
PBPC and Breast Cancer 67
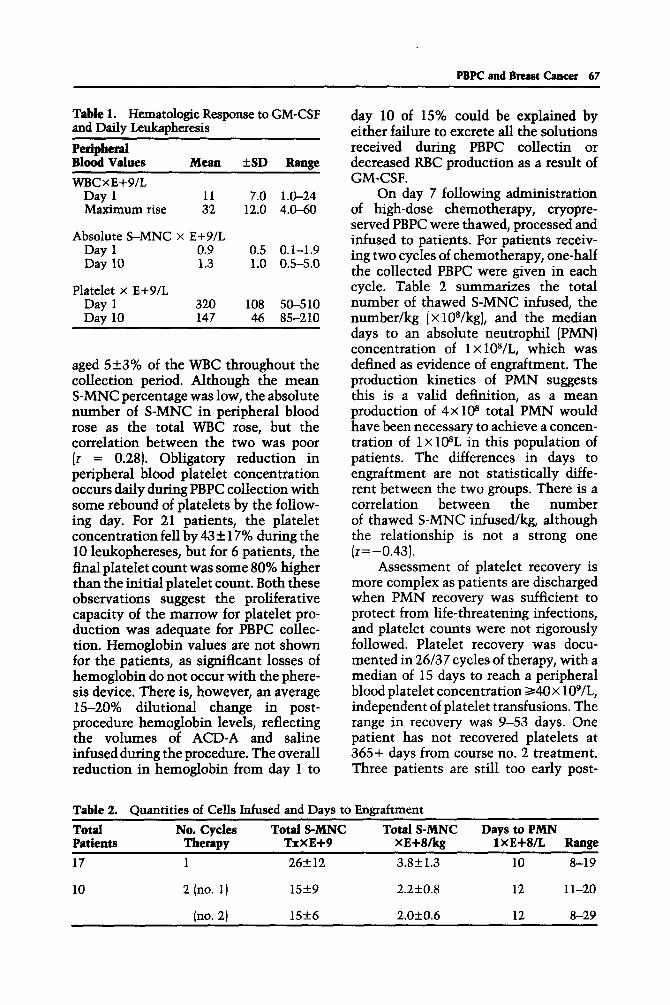
Table 1. Hematologic Response to GM-CSF and Daily Leukapheresis
day 10 of 15% could be explained by either failure to excrete all the solutions
Peripheral received during PBPC collectin or Blood Values MeGUt +SD Range decreased RBC production as a result of WBCxE+9/L GM-CSF.
Day 1 11 7.0 l&24 Maximum rise 32 12.0 4.0-60
Absolute 8-MNC x E+9/L Day 1 Day 10
Platelet x E+9/L
0.9 0.5 0.1-1.9 1.3 1.0 0.5-5.0
Day 1 320 108 50-510 Day 10 147 46 85-210
aged 5+3% of the WBC throughout the collection period. Although the mean S-MNC percentage was low, the absolute number of S-MNC in peripheral blood rose as the total WBC rose, but the correlation between the two was poor (r = 0.28). Obligatory reduction in peripheral blood platelet concentration occurs daily during PBPC collection with some rebound of platelets by the follow- ing day. For 21 patients, the platelet concentration fell by 43 + 17% during the 10 leukophereses, but for 6 patients, the final platelet count was some 80% higher than the initial platelet count. Both these observations suggest the proliferative capacity of the marrow for platelet pro- duction was adequate for PBPC collec- tion. Hemoglobin values are not shown for the patients, as significant losses of hemoglobin do not occur with the phere- sis device. There is, however, an average E-20% dilutional change in post- procedure hemoglobin levels, reflecting the volumes of ACD-A and saline infused during the procedure. The overall reduction in hemoglobin from day 1 to
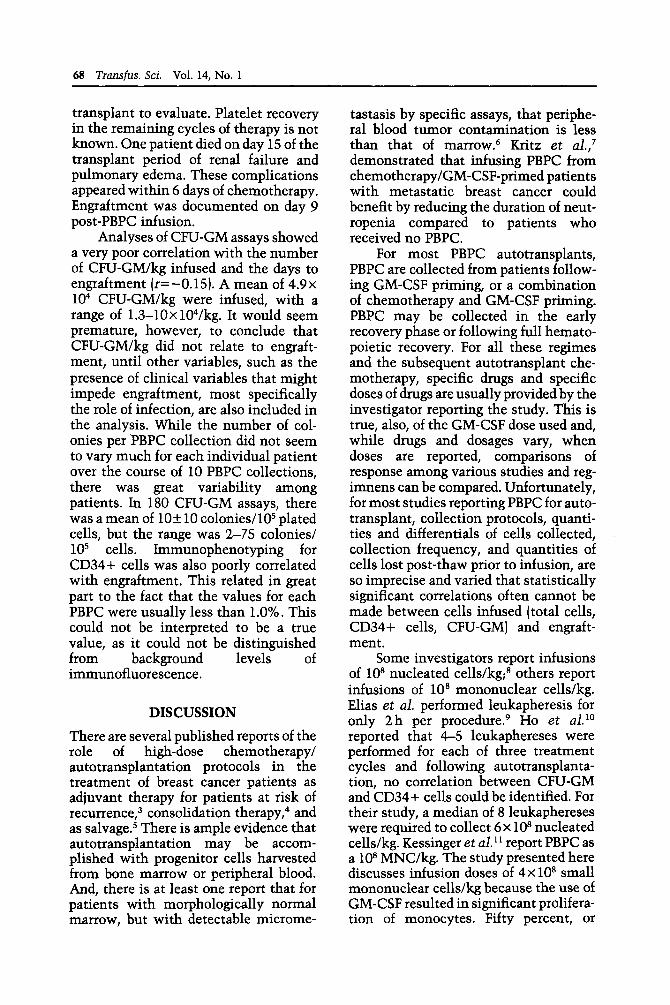
On day 7 following administration of high-dose chemotherapy, cryopre- served PBPC were thawed, processed and infused to patients. For patients receiv- ing two cycles of chemotherapy, one-half the collected PBPC were given in each cycle. Table 2 summarizes the total number of thawed S-MNC infused, the number/kg (X lO*/kg), and the median days to an absolute neutrophil (PMN) concentration of lx 108/L, which was defined as evidence of engraftment. The production kinetics of PMN suggests this is a valid definition, as a mean production of 4x10* total PMN would have been necessary to achieve a concen- tration of 1 X 108L in this population of patients. The differences in days to engraftment are not statistically diffe- rent between the two groups. There is a correlation between the number of thawed S-MNC infused/kg, although the relationship is not a strong one (r=-0.43).
Assessment of platelet recovery is more complex as patients are discharged when PMN recovery was sufficient to protect from life-threatening infections, and platelet counts were not rigorously followed. Platelet recovery was docu- mented in 26/37 cycles of therapy, with a median of 15 days to reach a peripheral blood platelet concentration ~40~ 109/L, independent of platelet transfusions. The range in recovery was 9-53 days. One patient has not recovered platelets at 365+ days from course no. 2 treatment. Three patients are still too early post-
Table 2. Quantities of Cells Infused and Days to Engraftment
Total No. Cycles Total S-MNC Total S-MNC Days to PMN Patients maPY TxxE+9 xE+8/kg 1 xE+8/L Range 17 1 26f12 3.8f1.3 10 8-19
10 2 (no. 1) 15f9 2.2kO.8 12 1 l-20
Ino. 2) 15+6 2.OkO.6 12 8-29
68 Transfus. Sci. Vol. 14, No. 1
transplant to evaluate. Platelet recovery in the remaining cycles of therapy is not known. One patient died on day 15 of the transplant period of renal failure and pulmonary edema. These complications appeared within 6 days of chemotherapy. Engraftment was documented on day 9 post-PBPC infusion.
Analyses of CFU-GM assays showed a very poor correlation with the number of CFU-GM/kg infused and the days to engraftment (r=-0.15). A mean of 4.9x lo4 CFU-GM/kg were infused, with a range of 1.3-lOxlV/kg. It would seem premature, however, to conclude that CFU-GM/kg did not relate to engraft- ment, until other variables, such as the presence of clinical variables that might impede engraftment, most specifically the role of infection, are also included in the analysis. While the number of col- onies per PBPC collection did not seem to vary much for each individual patient over the course of 10 PBPC collections, there was great variability among patients. In 180 CFU-GM assays, there was a mean of 10f 10 colonies/105 plated cells, but the range was 2-75 colonies/ lo5 cells. Immunophenotyping for CD34+ cells was also poorly correlated with engraftment. This related in great part to the fact that the values for each PBPC were usually less than 1 .O% . This could not be interpreted to be a true value, as it could not be distinguished from background levels of immunofluorescence.
DISCUSSION
There are several published reports of the role of high-dose chemotherapy/ autotransplantation protocols in the treatment of breast cancer patients as adjuvant therapy for patients at risk of recurrence,3 consolidation therapy,4 and as salvage.5 There is ample evidence that autotransplantation may be accom- plished with progenitor cells harvested from bone marrow or peripheral blood. And, there is at least one report that for patients with morphologically normal marrow, but with detectable microme-
tastasis by specific assays, that periphe- ral blood tumor contamination is less than that of marrow.6 Kritz et ul.,’ demonstrated that infusing PBPC from chemotherapy/GM-CSF-primed patients with metastatic breast cancer could benefit by reducing the duration of neut- ropenia compared to patients who received no PBPC.
For most PBPC autotransplants, PBPC are collected from patients follow- ing GM-CSF priming, or a combination of chemotherapy and GM-CSF priming. PBPC may be collected in the early recovery phase or following full hemato- poietic recovery. For all these regimes and the subsequent autotransplant che- motherapy, specific drugs and specific doses of drugs are usually provided by the investigator reporting the study. This is true, also, of the GM-CSF dose used and, while drugs and dosages vary, when doses are reported, comparisons of response among various studies and reg- imnens can be compared. Unfortunately, for most studies reporting PBPC for auto- transplant, collection protocols, quanti- ties and differentials of cells collected, collection frequency, and quantities of cells lost post-thaw prior to infusion, are so imprecise and varied that statistically significant correlations often cannot be made between cells infused (total cells, CD34+ cells, CFU-GM) and engraft- ment.
Some investigators report infusions of lo8 nucleated cells/kg;* others report infusions of lOa mononuclear cells/kg. Elias et al. performed leukapheresis for only 2 h per procedure.9 Ho et aI.” reported that 4-5 leukaphereses were performed for each of three treatment cycles and following autotransplanta- tion, no correlation between CFU-GM and CD34+ cells could be identified. For their study, a median of 8 leukaphereses were required to collect 6 x lo* nucleated cells/kg. Kessinger et al. l1 report PBPC as a lo8 MNC/kg. The study presented here discusses infusion doses of 4~ lo8 small mononuclear cells/kg because the use of GM-CSF resulted in significant prolifera- tion of monocytes. Fifty percent, or

PBPC and Breast Cancer 69
more, of each PBPC collection was often monocytes, not the small mononucle- ated population thought to contain prog- enitor cells.
As a number of cells collected per procedure will be a function of the quan- tity and type of available mononuclear cells to be collected (a biological variable over which there is little control even with cytokine priming), device efficiency and procedural variables such as the volume of blood processed and the num- ber of non-mononuclear cells collected, then targetting specific mononuclear cell populations and specific doses of these cells for autotransplant protocols would seem more appropriate than specifying the number of leukapheresis or reporting simply total nucleated cells infused. Fai- lure of progenitor assays to correlate more strongly with engraftment suggests the need to re-evaluate existing assays and investigate new ones.
REFERENCES
Nadler SB, Hidalgo JR, Block T: Predic- tion of blood volume in normal human adults. Surgery 1962; 51:224. Hester JP: Apheresis processing (A-P) of thawed peripheral blood progenitor cells (PBPC) compared to standard processing (S-P): a comparative study. Proc Am Sot Apheresis, p. 47, 1991. Peters WP, Davis R, Shpall EJ: Adjuvant chemotherapy involving high-dose com- bination cyclophosphamide, cisplatin and carmustine (CPA/CCDP/BCNU) and autologous bone marrow support (ABMS) for stage II/III breast cancer involving ten or more lymph nodes: a preliminary report. Proc Am Sot Clin Oncol, 1990; 9:22. Bitran JD, Kaminer LA, Williams SF: High-dose chemotherapy with auto- logous hematopoietic stem cell rescue in stage IV breast cancer. The University of Chicago experience. PTO, in autologous bone marrow transplantation, Dicke KA, Spitzer G, Jaganath S (eds): Autologous
5.
6.
7.
8.
9.
10.
11
Bone Marrow Transplantation, Proc 4th Int Symp, 1989; pp. 367370. Dour 0, Champlin R, Ho W: High-dose combined-modality therapy and auto- logous bone marrow transplantation in resistant cancer.Am IMed 1981; 17:973- 976. Sharp JG, Vaughan WP, Kessinger A, Mann SL, DeBoer JM, Sanger WG, Weisenburger DD: Significance of detec- tion of tumor cells in hematopoietic stem cell harvests of patients with breast cancer, in Dicke KA, Arm&age JO, Dicke- Evinger MJ (eds): Autologous Bone Mar- row Transplantation, Proc 5th Int Symp 1990; pp. 385-391. Kritz A, Crown, Motzer R, Gulati S, Reich L, Moore M, Michaelvicz R, Schneider JG, Hamilton N, Bellettieri R, Dougherty M, Heller G, Heelan R, Alfrey L, Moore MAS, O’Reilly R, Norton L: Superiority of peripheral blood progeni- tors (PBP) and GM-CSF alone in a pros- pective randomized trial following high dose chemotherapy (HDC) for metastatic breast cancer (MBC). Blood 1991; 78( 10): 19. Lasky LC, Hurd DD, Smith JA, Haake R: Peripheral blood stem cell collection and use in Hodgkin’s disease: comparison with marrow in autologous transplanta- tion. Transfusion 1989; 29:323-327. Elias A, Ayash L, Anderson K, Wheeler C, Mazanet R, Schwartz G, Teppler L, Reich E, Hunt M, Pap S, Pelaez J, Lynch C, S&nipper L, Griffin J, Frei E III, Antman K: GM-CSF-mobilized peripheral blood progenitor cells (PBPC) support after high dose chemotherapy for breast cancer: effect of GM-CSF post re-infusion. Blood 1991; 78( 10): 1590. Ho AD, Dietz M, Dietz G, Germond C, Sinoff C: Hematopoietic progenitors and lymphocyte subsets in peripheral blood and leukapheresis products after induc- tion chemotherapy combined with rhGM-CSF in patients with breast can- cer. Blood 1991; 78(10):57. Kessinger A, et al. : Autologous peripheral hematopoietic stem cell transplantation restores hematopoietic function follow- ing marrow ablative therapy. Blood 1988; 71: 723-727.





























