Embed Size (px)
Citation preview

© 1999 by the American Society for Dermatologic Surgery, Inc. • Published by Blackwell Science, Inc.ISSN: 1076-0521/99/ • Dermatol Surg 1999;25:1–9
Periorbital Rejuvenation: A Review ofDermatologic Treatments
Rhesa May P. Manaloto, Md and Tina S. Alster, Md
Washington Institute of Dermatologic Laser Surgery, Washington, DC
background.
The periorbital region serves as a barometer ofchronologic and environmental age and, as such, patients oftenseek its cosmetic rejuvenation.
objective.
The purpose of this article was to review the derma-tologic treatments available for periorbital skin rejuvenation.
methods.
Topical retinoic and glycolic acid preparations, chemi-cal peels, botulinum and collagen injections, dermabrasion, andlaser resurfacing procedures for periorbital skin rejuvenationwere reviewed. The relative benefits and risks of each treatmentwere detailed.
results.
Minimal photodamage with mild rhytides should beresponsibe to topical acid therapy and superficial peels, whereasmoderate wrinkling and photodamage generally require me-dium-depth peels, collagen injections, or erbium:YAG laser re-surfacing. Deeper rhytides and more extensive cutaneous photo-
damage usually necessitate CO
2
laser resurfacing and botulinuminjections.
conclusions.
Proper patient selection and assessment of agingseverity are critical to determine the best therapeutic option.
THE ONGOING quest for a youthful image has notdiminished in this era of aging “baby boomers.” Thisis exemplified by the different therapies that are cur-rently available for use or are undergoing clinical in-vestigation. The face and, in particular, the eyes areoften used as an immediate gauge of chronologic age.Consequently, most rejuvenative treatments are directedto the improvement, if not elimination, of rhytides in theperiorbital area. This article reviews dermatologic treat-ments currently in use for periorbital skin rejuvenation.
Background
Clinically, photoaged skin appears wrinkled, blotchy,and leathery. Histologically, dyskeratotic keratinocytesare present with evidence of epidermal atrophy and
flattening of the dermo-epidermal junction.
1
The periorbital region is a difficult area to treat be-cause of its delicate nature and important function.Eyelid skin is the thinnest in the body with the epider-mis measuring a mere 0.04 mm thick.
2
Careful alter-ation of the anatomic eyelid structure is crucial in orderto avoid any compromise of function. Because of theprotective role of the eyelids, ocular complications mayoccur if the lids are unable to close completely.
Periorbital wrinkles (“crow’s feet”) are primarily theresult of cumulative ultraviolet light-induced “photoag-ing” and muscle movement. The orbicularis oculi mus-cle fibers are arranged in a concentric fashion around
each eye. Upon muscle contraction, folding or wrin-kling of the overlying skin occurs, accentuating the cu-mulative sun damage in this area. Thus, the ideal treat-ment for periorbital aging should address both intrinsic(muscle movement) and extrinsic (ultraviolet light ex-posure) processes. For optimal results, two or moretherapeutic modalities may be necessary.
Topical Therapy
Tretinoin (Retinoic Acid)
Topical retinoic acid or tretinoin (Retin-A, Ortho-Pharmaceutical, Raritan, NJ) is one of the few topicaltreatments available in which the beneficial effect onphotoaging has been documented by several authors,beginning with Kligman’s observation of improvedskin texture and wrinkling in a post-adolescent acnepatient placed on long-term tretinoin therapy.
3–5
Thefeatures showing the most consistent and significantimprovement within 4–10 months of therapy are skintexture, mottled hyperpigmentation, and fine wrin-kles.
6,7
The use of 0.05% and 0.1% tretinoin creamfor six months leads to an increase in epidermal andgranular layer thickness.
8
The improvement seen inskin texture is attributed to hyaluronic acid depositionand compaction of the stratum corneum.
6
A limiting factor of tretinoin therapy is its tendencyto cause skin dryness. In order to counteract this ef-fect, new emollient formulations have been produced(Renova, Ortho). Long-term studies of tretinoin emol-lient cream using skin textural analysis have showncontinued clinical improvement of fine wrinkling, dys-pigmentation, and roughness after 48 weeks of use.
Address correspondence and reprint requests to: Tina S. Alster, MD,2311 M Street, NW Suite 200, Washington, DC 20037

2
manaloto and alster: periorbital rejuvenation
Dermatol Surg 25:1:January 1999
Histologically, reversal of stratum corneum compactionand epidermal and granular layer thickness is observedafter 24 weeks of therapy. Melanin content decreasesand epidermal mucin increases after 48 weeks.
9
Another retinoid, retinol (all-trans-retinol or vita-min A
1
) has been discovered to possess similar activityas retinoic acid without the irritative effects. Retinolapplication of up to a 1.6% concentration producesmuch less erythema when compared to retinoic acid0.025% while inducing epidermal thickening and in-creasing expression of cellular retinoic acid-bindingprotein (CRABP-II mRNA) and cellular retinol bind-ing protein (CRBP mRNA) similar to that of retinoicacid.
10
Alpha Hydroxy Acids (AHAs)
Over the past few years, AHAs have become popular-ized and incorporated in the skin care maintenance regi-mens of thousands of individuals. AHAs are linear or-ganic carboxylic acids with an attached hydroxyl groupand can be derived in natural foods; hence the com-mon name, fruit acids. Included in this class of acidsare glycolic acid found in sugar cane, lactic acid fromsour milk, malic acid from apples, citric acid from citrusfruits, and tartaric acid derived from grapes. Glycolicacid, the simplest of the alpha hydroxy acids, is the mostpopular fruit acid and is available in concentrationsranging from 5% to 15%. Higher concentrations of thisacid are used for chemical peels.
In photoaging, the skin surface is rough and drydue to the accumulation of corneocytes. AHAs exerttheir epidermal effect at the stratum corneum-stratumgranulosum junction. A thinner stratum corneum witha normal-appearing basket-weave pattern is achievedby diminishing corneocyte cohesion, thus promoting asmoother, more supple skin surface.
11–14
The use of AHAs has been shown to reverse histo-logic signs of photoaging by increasing epidermal thick-ness, reversing basal cell atypia, dispersing melanin pig-mentation, and normalizing the rete pattern of thedermoepidermal junction. The increased skin thicknessis attributed to increased synthesis of glycosaminogly-cans, collagen, and possibly elastic fibers.
15
AHAs have also been used as an adjunct to tretinointherapy without increasing adverse sequelae.
11,13,16
Large-scale controlled studies are still needed in order to verifythe effects and advantages of this combination treatment.
Chemical Peels
Chemical peeling is one of the most common proce-dures performed in dermatologic offices for skin rejuve-nation. The process involves the application of a causticchemical agent on the skin to produce a controlled, par-
tial-thickness injury. Chemical peels are categorizedinto superficial, medium-depth, and deep types.
Superficial peels penetrate the epidermis down tothe dermal-epidermal junction. An example of a su-perficial peeling agent is Jessner’s solution, which is acombination of resorcinol, salicyclic acid, and lacticacid in an alcohol solution. Triple-layer application ofthe combination produces stratum corneum separa-tion with upper intraepithelial and intercellular edema.The dermis is not affected with this solution.
17,18
Glycolic acid at concentrations of 20% to 70% is amore popular agent used for superficial chemical peel-ing. The effect of a glycolic acid peel depends on thelength of time it is left on the skin and, thus, needs to beneutralized either with water or sodium bicarbonate toprevent deeper dermal penetration. Glycolic peels areroutinely performed in a series of 4 to 6 treatments at1 to 6 week time intervals in order to improve skin sal-lowness, dyspigmentation, and fine wrinkles.
19–21
Formild photodamage and wrinkling, an initial applicationof 70% unbuffered glycolic solution is recommendedfor a duration of 4 to 8 minutes.
19
Because of varyingindividual responses, continuous monitoring of the pa-tient is imperative to assess epidermolysis and undueskin color change. Histologic comparison studies of35% trichloroacetic acid (TCA) and 70% glycolic acidrevealed similar findings of thickened collagen fibersand elastic fibers in the papillary dermis at 2 months;however, only TCA demonstrated epidermal necrosis.The histologic changes reversed to pretreatment condi-tions after 19 months.
20
Trichloroacetic acid is a versatile peeling agent be-cause the concentration may be adjusted in order toachieve the desired depth of peel. Concentrations of15% to 35% TCA can be used for superficial peeling.TCA causes necrosis and exfoliation of normal andactinically damaged cells and also precipitates epider-mal proteins. This acid is nontoxic systematically andis neutralized by serum in superficial dermal bloodvessels.
21
Partial epidermal exfoliation occurs with20% TCA, therefore a series of peels may be necessaryin order to optimize the rejuvenating effects of papil-lary dermal remodeling.
22
Application of TCA causestransient frosting and erythema. In the subsequent 24-48 hours, the skin darkens, followed by exfoliation bythe third or fourth day. Acid application may be re-peated after 1 to 2 weeks.
23
To ensure an even application of acid, some manufac-turers add sodium fluorescein to the solutions, renderingthe preparation visible under a Wood’s lamp. This tech-nique helps detect skip areas and avoids overcoating. An-other TCA peel modification is the Obagi “blue peel”which contains a non-ionic blue base with glycerin andsaponins in order to slow the rate of TCA action and togauge the depth of peel.
24
A light blue end point signifies

Dermatol Surg 25:1:January 1999
manaloto and alster: periorbital rejuvenation
3
exfoliation to the stratum corneum, while a dark blueendpoint denotes coagulation to the basal layer of theepidermis. These superficial peels are desirable becauseof the minimal recovery time needed and the reducedlikelihood of serious adverse sequelae. Furthermore, allskin types may be treated with superficial peels.
25
Medium-depth peels pertain to the use of agents or acombination of agents in order to produce an injurydepth down to the upper reticular dermis.
26
These peelsare best used to treat actinic keratoses, dyschromia, andmild wrinkling. Concentrations of TCA ranging from40% to 60% cause epidermal necrosis, edema, and ho-mogenization of the papillary dermis and sparse lym-phocytic infiltration in the midreticular dermis within 3days after application.
17
The use of 60 to 75% TCA isrecommended only for spot treatment of localized kera-toses. 50% TCA may be applied either in a rapid fash-ion over the entire face without overcoating or in aslow, controlled manner to each cosmetic unit. Theeyelids are peeled with 20% to 35% TCA. (Figure 1).Higher concentrations of TCA cause more pain thanthe combination peels discussed below, hence, sedationmay be necessary.
26
Contrary to expectations, tape oc-clusion of TCA decreases its depth of penetration.
27
Transepidermal water loss is hindered upon occlusion,causing a dilution of the acid’s concentration.
22
Present trends dictate combining less potent agentsin order to achieve a medium-depth peel. In an at-tempt to decrease the risk of complications, a superfi-cial peeling agent is initially used in order to pretreatthe epidermis followed by TCA application. After de-greasing the skin with acetone, either dry ice or Jess-ner’s solution can be applied to initiate an epidermalinjury. This then enables the 35% TCA to penetratemore readily.
18,26,28
A newer combination is the use of70% unbuffered aqueous glycolic solution to soap-clean skin without prior degreasing with acetone.
26
Left on for 2 minutes, this solution causes epidermoly-sis allowing deeper penetration of subsequent 35%TCA solution application. Histologic examination ofskin treated with each of these three combinationpeels is similar with new collagen formation evident inthe Grenz zone. The deepest medium-depth peel, dryice, and TCA is not recommended for darker skintones due to the risk of hypopigmentation. Approxi-mately an hour following a medium-depth peel, cuta-neous erythema changes to a brownish hue. Edemawith minimal discomfort is typical for the first 48hours. After partial resolution of the edema, crust for-mation ensues, with epidermal separation occurring 4to 8 days after the procedure.
21,28
Deep peels involve the use of chemoexfoliants thatpenetrate to the midreticular dermis. Indications fortheir use include deep rhytides secondary to photo-damage and treatment of severe or extensive actinic
keratoses. Deep chemical peeling entails longer heal-ing times and increased potential for complications.
Baker’s formula is the most commonly used deepchemical peel. It is composed of a mixture containing 3ml 88% phenol USP, 3 drops croton oil, 8 drops Septi-sol, and 2 ml distilled water. Phenol at 80% or higherconcentrations precipitates epidermal proteins, thusforming a barrier hindering deep dermal penetration,while phenol diluted to 50% is keratolytic, allowing in-creased dermal penetration and hence greater dermalinjury. The croton oil is an epidermolytic agent thataugments phenol penetration. Septisol increases surfacetension and is thought to slow the penetration of phe-nol.
23,29
The phenol peel may be applied under occlu-sion using waterproof zinc oxide nonporous tape or leftunoccluded. Occlusion increases the penetration of phe-nol by promoting tissue maceration and prevention ofthe agent’s evaporation.
30,31
Figure 1. Mild to moderately severe periorbital rhytides in a52-year-old woman before (A) and 1 month after two 25% TCAchemical peels at biweekly intervals (B).

4
manaloto and alster: periorbital rejuvenation
Dermatol Surg 25:1:January 1999
The reaction following application of phenol ischaracterized by keratocoagulative necrosis of the epi-dermis extending into the papillary dermis and by amarked inflammatory reaction. Epidermal regenera-tion begins within 48 hours and is completed within 1week. Dermal regeneration takes longer than epider-mal healing and is characterized by rigid, compact col-lagen in the upper dermis replacing the disorganizedcollagen seen in elastosis.
32
Deep phenol peeling may lead to irreversible hypo-pigmentation and, thus, is not advised for darker skintypes. Cardiac arrhythmias may occur with systemicabsorption of phenol, necessitating cardiac monitoringand slow application of the solution.
28
Adverse sequelae following superficial and medium-depth peels are usually minor and reversible, includingprolonged erythema and post-inflammatory hyperpig-mentation. Hypertropic scarring can occur on rare oc-casions and can be managed by the use of any one or acombination of therapies, including topical or intrale-sional steroids, silicone gel sheeting, and pulsed dye la-ser irradiation.
28
Infections such as herpes simplex reac-tivation can occur and could lead to scarring.
33
It is common practice to pretreat patients withtretinoin and/or hydroquinone for 4 to 6 weeks priorto a chemical peel. This regimen decreases the stratumcorneum thickness ensuring a more uniform responsefollowing the application of the peeling solution.
22,23
Botulinum Toxin A Injections
Botulinum type A exotoxin (Botox, Allergan, CA) isnot a new therapeutic agent, having been used for stra-bismus and blepharospasm since 1980.
34,35
Its potentialuse in the cosmetic field was first observed by Carruth-ers in 1986 when a patient treated for blepharospasmdemonstrated marked improvement of frown lines. Aseries of studies were performed to evaluate the safetyand effectiveness of this modality on rhytides.
36,37
Thebotulinum toxin binds to terminal receptors at the pre-synaptic neuron of the motor unit which is then inter-nalized into the nerve cytosol by endocytosis, therebyinhibiting acetylcholine release.
38
Dermatologic use of Botox has traditionally beenlimited to glabellar furrows, but its use has expandedto the treatment of forehead and periorbital rhytides,among others. Since periorbital rhytides result fromboth photoaging and contraction of the orbicularis oc-uli muscles, the treatment goal is muscle weakening,not paralysis.
36,37
Use of this treatment either prior toor after periorbital laser resurfacing augments the ef-fects of the laser and helps maintain the improved ap-pearance of wrinkles.
39
(Figure 2)The toxin is injected periorbitally within 4 hours of
its dilution, usually 1 to 1.5 cm lateral to the lateral
orbital rim with 3 unit injections. Electromyographicguidance may be used during injection in order to lo-calize functioning musculature. Ice compresses are ad-vised after treatment in order to reduce ecchymoses.Patients are advised to keep upright for at least 4hours and to contract the treated muscles in order forthe toxin to be taken up by the involved neural end-plates.
40
Reported adverse effects of Botox injections in thelateral orbital area include worsening of preexistingfat herniations of the lower eyelid, temporary droopof the lateral lower eyelid, and skin redundancy be-neath the lateral lower eyelid. These complicationsmay be avoided by injecting more laterally and, incases of skin redundancy, combining Botox injectionswith cutaneous resurfacing.
36
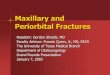
Figure 2. A 41-year-old woman with mild to moderate periorbitalrhytides before (A) and 3 months after lateral canthal injections of18 units of botulinum toxin (9 units per eye). (B). Both photo-graphs were taken when patient was squinting.

Dermatol Surg 25:1:January 1999
manaloto and alster: periorbital rejuvenation
5
Collagen Injections
The aim of any collagen implantation process is to sub-stitute or enhance diminished or altered native collagenin order to elevate skin contour depression. There arethree available formulations of injectable exogenousbovine collagen: Zyderm I, Zyderm II, and Zyplast(Collagen Corporation, CA). These formulations arecomposed of reconstituted bovine collagen suspendedin saline, with the more antigenic telopeptides removedby enzymatic digestion. Zyderm I contains 35 mg/cc ofcollagen while Zyderm II contains 65 mg/cc of collagen,both have 0.3% lidocaine added to reduce pain associ-ated with injection. Zyplast consists of highly purifiedbovine collagen with 0.3% lidocaine and 0.0075% glu-taraldehyde. Crosslinks in the collagen molecule areproduced with the addition of glutaraldehyde to makethe collagen more resistant to degradation by pro-teolytic enzymes and less immunogenic.
41
Zyderm I is the most versatile of the three bovine col-lagens and is used to correct superficial dermal defects.Injection is targeted to the upper dermis. Side by side in-jections are placed in the upper dermis in order to pro-duce an overcorrection of 150% to 200%. Zyplast isused for deeper dermal defects and is best placed in themid-dermis. A layering technique whereby Zyderm I isimmediately implanted over the mid-dermal Zyplast in-jection sites is used to optimize clinical correction.
42
Erythema, temporary overcorrection, wheal forma-tion, edema, and bruising are common after collageninjection. Occasionally, skin lumpiness, hypersensitiv-ity reactions (despite negative skin testing), and reacti-vation of herpes simplex infection may occur. Rareadverse sequelae include recurrent intermittent swell-ing at the treatment site, local necrosis, abscess forma-tion, and loss of vision due to collagen embolus to theophthalmic artery.
42
Collagen implantation offers ex-cellent results. However, repeat injections at 4 to 12month intervals are necessary in order to maintain theclinical effect.
Despite the ease of application and good overallcosmetic effect of collagen implantation, the perior-bital area is the least responsive to collagen injections.This may be related to the thin dermis of periorbitaltissue that contains loose stroma and a relatively highliquid/mucin component. These characteristics makeplacement of dermal filler difficult with their eventualrapid dissolution.
43
The risk of hypersensitivity reactions to bovine col-lagen injection and its relatively short-term efficacystimulated research in the use of human collagen forskin augmentation. Autologous collagen fibers can beprepared from mechanical pulverization of the recipi-ent patient’s own excised skin (Autologen, Collagene-sis, Beverly, MA) or, alternatively, the patient’s fibro-
blasts can be cultured
in vitro
from a small biopsy for4 to 6 weeks (Isolagen, Isolagen Technologies, Para-mus, NJ).
44,45
Ongoing multi-center clinical trials arebeing conducted to evaluate the clinical efficacy andadverse effects of cadaveric human collagen (Dermalo-gen, Collagenesis) compared to bovine collagen. Theuse of human collagen diminishes the possibility of hy-persensitivity reactions and may lead to more pro-longed clinical effects.
44–46
Dermabrasion
Dermabrasion is a process of surgical skin planingwhereby a wire brush or diamond fraise attached to arotary instrument is used to abrade the skin, effectivelyremoving the epidermis and the upper and middle der-mis, including the upper portions of adnexae. Reepithe-lialization and repigmentation occurs from the adjacenthair follicles and residual adnexal structures.
Dermabrasion has been used primarily in the treat-ment of atrophic acne scarring, however, superficialdermabrasions extending only to the level of papillarydermis have been performed on patients with actini-cally damaged skin.
47–49
Histologic studies of pre- and post-dermabraded skindemonstrate reversal of actinic features. Specifically, theepidermis shows eventual return of the rete pattern in 2years and disappearance of dyskeratotic keratinocytes.In the dermis, expansion of the Grenz zone with thick-ened and increased numbers of collagen bundles are ob-served. The resulting skin smoothness and improvedtexture and turgor after dermabrasion have been attrib-uted to these histologic changes.
50
The equipment used for dermabrasion is not expen-sive and large areas may be treated in short periods oftime; however, fine control is difficult due to the instru-ment’s bulkiness. Because it is best to have an immobileand relatively rigid skin surface on which to work, eye-lids and periorbital regions are almost impossible totreat with dermabrasion. Moreover, the procedure isbloody, rendering intraoperative visualization of theskin difficult. Other concerns include infectious poten-tial of aerosolized particles such as HIV and hepatitis Band risk of complications such as permanent dyspig-mentation and scarring.
50,51
Laser Resurfacing
Carbon Dioxide (CO
2
) Laser
Dermatologic surgery has been revolutionized with thedevelopment and clinical expansion of laser technology.Cutaneous laser resurfacing involves the vaporizationof the entire epidermis as well as a variable thickness ofthe dermis. Water-containing cells of the epidermis and

6
manaloto and alster: periorbital rejuvenation
Dermatol Surg 25:1:January 1999
dermis can be preferentially targeted by laser light usingthe principles of selective photothermolysis.
52
The CO
2
laser emits monochromatic 10,600 nmlight which is preferentially absorbed by water-con-taining tissues. In order to minimize the thermal dam-age to surrounding skin, it is also important to deliversufficient energy to the target chromophore at a pulseduration shorter than the time it takes for the lased tis-sue to lose 50% of its heat (thermal relaxation time).With the newer pulsed and scanned CO
2
laser sys-tems, high energies can be delivered above the skin ab-lation threshold of 5 J/cm
2
at a tissue dwell time of lessthan 1 ms, which is the thermal relaxation time of theepidermis.
53–55
Histological comparisons of differentCO
2
laser systems have demonstrated variable depthsof tissue ablation and residual thermal damage; how-ever, clinical efficacy is comparable when proper tech-nique is used.
56–58
In general, with each laser pass, in-creased residual thermal necrosis is observed due toextensive heat absorption of partially desiccated tissueand decreased vaporization upon delivery of each sub-sequent laser pass.
56–58
Of all facial regions, rhytides in the periorbital area re-spond best to CO
2
laser resurfacing with up to 90% clin-ical improvement observed from baseline.
59
In addition,infraorbital hyperpigmentation improves after CO
2
laserresurfacing.
60
Typically, only a couple of non-overlap-ping laser passes using any of the CO
2
laser systems arenecessary to achieve significant clinical improvement.
A study comparing the CO
2
laser resurfacing with amedium-depth peel (Jessner’s followed by 35% TCA) inthe treatment of periorbital rhytides demonstrated betterwrinkle scores after laser resurfacing.
61
However, post-operative erythema was more prolonged after laser treat-ment than after chemical peeling. In a comparison studyof two high-energy pulsed CO
2
lasers in the treatment ofperiorbital wrinkles, the “ultrapulse” CO
2
laser pro-vided a slightly better clinical response (82% mean im-provement) and required fewer laser passes than did the“surgipulse” CO
2
system (63% mean improvement).
62
Healing times were equivocal for the two systems.In addition to the layer-by-layer vaporization of
skin that occurs with CO
2
laser resurfacing, collagenshrinkage also results from thermal denaturation oftype I collagen. The laser-induced dermal injury isthought to promote collagen deposition, with a widerzone of fibroplasia.
63
The combination of vaporiza-tion, collagen shrinkage, and collagen deposition ac-counts for the clinical improvement seen.
64
(Figure 3)Adverse effects observed after CO
2
laser resurfacinginclude prolonged erythema, hyperpigmentation, milia,infections, hypersensitivity, scarring, and ectropion.
65–71
Post-treatment erythema, which is an expected side ef-fect, is seen in all patients and can persist for severalmonths.
66
Hyperpigmentation has been reported to
occur in 2.8% to 36% of cases, with the highest inci-dence in patients with darker skin tones. Some authorsrecommend the use of hydroquinone and retinoic acidtwo to six weeks prior to laser resurfacing and postop-eratively in order to decrease the risk of hyperpigmen-tation.
65,67
Alternatively, post-laser hyperpigmentationmay also be managed with a series of superficial gly-colic acid peels in order to hasten the resolution of dys-pigmentation.
54,66
Reactivation of latent herpes simplexvirus can occur and is typically observed in the firstpostoperative week.
66,68
Bacterial and candidal infec-tions have also been documented.
54,65,66,69,70
A severecomplication associated with periorbital laser resur-facing is the development of lower lid ectropion. Thisoccurs more often in patients with prior eyelid surgeryor concurrent resurfacing with blepharoplasty and of-
Figure 3. Facial photodamage with prominent periorbital rhytidesand dermatochalasis in a 53-year-old woman before (A) and 5months after (B) periorbital CO2 laser resurfacing using a 5-mmscanning handpiece at 300-mJ energy, 60-watt power, density of6. Two passes were delivered with complete removal of partially-desiccated tissue after each pass.

Dermatol Surg 25:1:January 1999
manaloto and alster: periorbital rejuvenation
7
ten necessitates surgical correction.
54,66,71
It is impera-tive that proper assessment of eyelid elasticity be madepreoperatively in order to determine the appropriateadjustments in laser protocol.
In a continuous mode, the CO
2
laser may be used toassist blepharoplasty in conjunction with laser resurfac-ing.72 (Figure 4) The main advantage of incisional lasersurgery over conventional cold steel and electrocauteryis its improved intraoperative hemostasis, with subse-quent decreased ecchymoses and edema.73 The contin-uous wave CO2 laser is capable of photocoagulatingblood vessels up to 0.5 mm in diameter and sealingsmall lymphatic vessels and nerve endings, thereby alsoleading to decreased postoperative pain.74 Combininglaser blepharoplasty and cutaneous resurfacing has ad-ditional advantages, including improved clinical effi-cacy and a single, rather than double, healing process.
Erbium:Yttrium-Aluminum-Garnet (Er:YAG) Laser
The erbium:YAG laser is one of the latest additions tothe armamentarium of resurfacing treatments for rhy-tides. The laser light is emitted in the mid-infrared elec-tromagnetic spectrum at 2,940 nm which is highly ab-sorbed by water. Thus, water-containing cutaneoustissues can be vaporized, much like the CO2 laser sys-tem.74,75 In contrast, however, insignificant residualthermal damage is produced in the dermis due to thebrief pulse width with minimal heat conduction.76,77 Sig-nificant clinical improvement of periorbital and otherfacial rhytides has been reported with remarkablyspeedy recovery times.77–80 Minimal, if any, collagencontraction occurs; however, erbium:YAG laser resur-facing is less desirable than CO2 laser resurfacing or ble-pharoplasty for dermatochalasis or moderate to severeperiorbital rhytides.79,80 In addition, the reduced hemo-static effect of the erbium:YAG laser compared withthat of the CO2 laser may impair intraoperative visibilitydue to bleeding.
The major advantage of cutaneous laser resurfacingis the control of skin vaporization layer-by-layer in arelatively clear field. When proper laser technique andpostoperative management is used, the risk of scarringor other complications is minimized and clinical re-sults are equal to, if not better than, that obtainedwith chemical peels or dermabrasion. The major dis-advantages of using this advanced laser technology arethe technical skill learning curve required of surgeonsand the monetary expense and postoperative timecommitment required of patients.
Conclusion
It is evident that there are several dermatologic therapiesfrom which to choose for periorbital skin rejuvenation.
Proper patient selection and assessment of aging severityis important in order to determine the best therapeuticoption. Minimal photodamage with mild rhytides shouldbe responsive to topical acid therapy and superficialpeels, whereas moderate wrinkling and photodamagemay necessitate medium-depth peels, collagen injections,or erbium laser resurfacing. Deeper rhytides and moreextensive cutaneous photodamage are better managedwith CO2 laser resurfacing and Botox injections. Ofequal importance are the patient’s expectations from thetherapy, necessitating a proper preoperative consultationto discuss the anticipated results and possible side effectsfrom each of the aforementioned procedures. Lastly,maintenance of the newly rejuvenated skin through sunprotection and a good skin care regimen is important toprolong the clinical results.
Figure 4. Dermatochalasis and herniated orbital fat of lower eye-lids in a 53-year-old woman before (A) and 1 month after laser-assisted upper and lower blepharoplasties (B).

8 manaloto and alster: periorbital rejuvenation Dermatol Surg 25:1:January 1999
References1. Lavker RM. Cutaneous aging: chronologic versus photoaging. In:
Gilchrest BA, ed. Photodamage. Cambridge: Blackwell Science Inc.,1995:123–31.
2. Ackerman AB. Embryologic, histologic and anatomic aspects. In:Ackerman AB, ed. Histologic Diagnosis of Inflammatory Skin Dis-ease, 2nd ed. Baltimore: Williams and Wilkins, 1997:3–56.
3. Kligman AM, Grove GL, Hirose R, et al. Topical tretinoin for pho-todamaged skin. J Am Acad Dermatol 1986;15:836–59.
4. Weiss J, Ellis CN, Headington JT, et al. Topical tretinoin improvesphotoaged skin: a double blind vehicle controlled study. JAMA1988;259:527–32.
5. Weinstein GD, Nigra TP, Pochi PE, et al. Topical tretinoin fortreatment of photodamaged skin: a double-blind, vehicle-controlledstudy. Arch Dermatol 1991;127:659–65.
6. Kang S, Fisher GJ, Voorhees JJ. Photoaging and topical tretinoin:therapy, pathogenesis, and prevention. Arch Dermatol 1997;133:1280–4.
7. Kligman AM, Grove GL, Hirose R, Leyden JJ. Topical tretinoin forphotoaged skin. J Am Acad Dermatol 1986;15:836–59.
8. Bwanan J, Gonzalez-Serva A, Nehal K, et al. Effects of tretinoin onphotodamaged skin: a histologic study. Arch Dermatol 1991;127:666–72.
9. Olsen EA, Katz IH, Levine N, et al. Tretinoin emollient cream forphotodamaged skin: results of 48-week, multicenter, double-blindstudies. J Am Acad Dermatol 1997;37:217–26.
10. Kang S, Duell EA, Fisher GJ, Datta SC, et al. Application of retinolto human skin in vivo induces epidermal hyperplasia and cellularretinoid binding proteins characteristic of retinoic acid but withoutmeasurable retinoic acid levels or irritation. J Invest Dermatol1995;105:549–56.
11. Kligman AM. The compatibility of combinations of glycolic acidand tretinoin in acne and photoaged facial skin. J Geriatr Dermatol1995;3(Suppl A):25A–9A.
12. Rendon-Pellarno MI, Bernstein EF. The use of glycolic acids in themanagement of xerosis and photoaging. J Geriatr Dermatol 1996;4(Suppl B):112b–16B.
13. Leyden JJ, Lavker RM, Grove G, Kaidbey K. Alpha hydroxy acids aremore than moisturizers. J Geratr Dermatol 1995;3(Suppl A):33A–7A.
14. Van Scott EJ, Yu RJ. Actions of alpha hydroxy acids on skin com-partments. J Geriatr Dermatol 1995;3(Suppl A):19A–25A.
15. Ditre CM, Griffin TD, Murphy GF, et al. Effects of alpha-hydroxyacids on photoaged skin: a pilot clinical, histologic and ultrastruc-tural study. J Am Acad Dermatol 1996;34:187–95.
16. Draelos ZD. Therapeutic skin care in the mature patient. Clin PlastSurg 1997;24:369–77.
17. Brody HJ. Histology and classification. In: Brody HJ. ChemicalPeeling and Resurfacing, 2nd ed. St. Louis: Mosby, 1997:7–28.
18. Monheit GD. The Jessner’s-trichloroacetic acid peel. Dermatol Clin1995;13:277–83.
19. Moy LS, Murad H, Moy RL. Glycolic acid peels for the treatment ofwrinkles and photoaging. J Dermatol Surg Oncol 1993;19:243–46.
20. Murad H, Shamban AT, Premo PS. The use of glycolic acid as apeeling agent. Dermatol Clin 1995;13:285–306.
21. Brody HJ. Superficial peeling. In: Brody HJ. Chemical Peeling andResurfacing, 2nd ed. St. Louis: Mosby, 1997:73–108.
22. Roenigk RK, Brodland DG. A primer of facial chemical peel. Der-matol Clin 1993;11:349–59.
23. Glogau RG, Matarasso SL. Chemical peels: trichloroaceetic acidand phenol. Dermatol Clin 1995;13:263–75.
24. Johnson JB, Ichinose H, Obagi ZE. Obagi’s modified trichloroa-ceetic acid (TCA)-controlled variable-depth peel: a study of clinicalsigns correlating with histological findings. Ann Plast Surg 1996;36:225–37.
25. Ditre CM, Nini KT, Vagley RT. Practical use of glycolic acid as achemical peeling agent. J Geriatr Dermatol 1996;4(Suppl B):2–7.
26. Brody HJ. Medium-depth peeling. In: Brody HJ. Chemical Peelingand Resurfacing, 2nd ed. St. Louis: Mosby, 1997:109–36.
27. Brodland DG, Cullimore KC, Roenigk RK, et al. Depths ofchemexfoliation induced by various concentrations and applicationtechniques of trichloroacetic acid in a porcine model. J DermatolSurg Oncol 1989;15:967–71.
28. Coleman WP, Brody HJ. Advances in chemical peeling. DermatolClin 1997;15:19–26.
29. Matarasso SL, Brody HJ. Deep chemical peeling. Semin Cutan MedSurg 1996;15:155–61.
30. Spira M, Freeman R, Arfai P, et al. A comparison of chemical peel-ing, dermabrasion and 5-fluorouracil in cancer prophylaxis. J SurgOncol 1971;3:367–8.
31. Brody HJ. Deep peeling. In: Brody HJ. Chemical Peeling and Resur-facing, 2nd ed. St. Louis: Mosby, 1997:137–59.
32. Stuzin JM, Baker TJ, Gordon HL. Treatment of photoaging facialchemical peeling (phenol and trichloroacetic acid) and dermabra-sion. Clin Plast Surg 1993;20:9–25.
33. Resnik SS, Resnik BI. Complications of chemical peeling. DermatolClin 1995;13:309–12.
34. Scott AB. Botulinum toxin injection of eye muscles to correct stra-bismus. Trans Am Ophthalmol Soc 1981;79:734–70.
35. Elton JS. Botulinum toxin treatment of blepharospasm. Adv Neurol1988;50:579–81.
36. Carruthers A, Caruthers J. Cosmetic uses of botulinum A exotoxin.Adv Dermatol 1997;12:325–53.
37. Guerrissi J, Sarkissian P. Local injection into mimetic muscles ofbotulinum toxin A for the treatment of facial lines. Ann Plast Surg1997;39:447–53.
38. Carruthers A, Kiene K, Carruthers J. Botulinium A exotoxin use inclinical dermatology. J Am Acad Dermatol 1996;34:788–97.
39. West TB, Alster TS. Effect of botulinum toxin type A on move-ment-associated rhytides following cutaneous CO2 laser resurfac-ing. Lasers Surg Med 1998;Suppl 10:7.
40. Klein AW. Cosmetic therapy with Botulinum toxin. Dermatol Surg1996;22:757–9.
41. Klein AW. Indications and implantation techniques for the variousformulations of injectable collagen. J Dermatol Surg Oncol 1988;14(Suppl 1):27–30.
42. Drake LA, Dinehart SM, Farmer ER, et al. Guidelines of care forsoft tissue augmentation: collagen implants. J Am Acad Dermatol1996;34:698–702.
43. Bailin PL, Bailin MD. Collagen implantation: clinical applicationsand lesion selection. J Dermatol Surg Oncol 1988;14(Suppl 1):21–6.
44. DeVore DT, Kelman CD, Fagien S, et al. Autologen: autologous,injectable dermal collagen. In: Bosniak S, ed. Principles and Prac-tice of Ophthalmic Plastic and Reconstructive Surgery, Vol I. Phila-delphia: W.B. Saunders, 1996:670–75.
45. West TB, Alster TS. Autologous human collagen and dermal fibro-blasts for soft tissue augmentation. Dermatol Surg 1998;24:510–2.
46. Elson ML. Soft tissue augmentation: a review. Dermatol Surg1995;21:491–500.
47. Nelson BR, Majmudar G, Griffiths CEM, et al. Clinical improve-ment following dermabrasion of photoaged skin correlates withsynthesis of collagen. Arch Dermatol 1994;130:1136–42.
48. Fulton JE. Dermabrasion, chemabrasion and laserbrasion. Derma-tol Surg 1996;22:619–28.
49. Orentreich N, Orentreich DS. Dermabrasion. Dermatol Clin 1995;13:313–27.
50. Benedetto AV, Griffith TD, Benedetto EA, Humeniuk HM. Derm-abrasion: therapy and prophylaxis of the photoaged face. J AmAcad Dermatol 1992;27:439–47.
51. Roenigk HH, Jr. Dermabrasion and aging skin. J Geriatr Dermatol1994;2:24–9.
52. Anderson RR, Parish JA. Selective photothermolysis: precise micro-surgery by selective absorption of pulsed radiation. Science 1983;22:524–7.
53. Weinstein C, Alster TS. High-energy, pulsed carbon dioxide lasertreatment of facial rhytides. In Alster TS, Apfelberg DB, eds. Cos-metic Laser Surgery. New York: Wiley & Sons 1996:9–27.
54. Alster TS. Laser resurfacing of rhytides. In: Alster TS. Manual ofCutaneous Laser Techniques. Philadelphia: Lippincott-Raven; 1997:103–22.
55. Walsh JT, Flotte TJ, Anderson RR, et al. Pulsed CO2 laser tissueablation: effect of tissue type and pulse duration on thermal dam-age. Lasers Surg Med 1988;8:108–18.
56. Kauvar ANB, Waldorf HA, Geronemus RG. A histopathologicalcomparison of “char-free” carbon dioxide lasers. Dermatol Surg1996;22:343–48.

Dermatol Surg 25:1:January 1999 manaloto and alster: periorbital rejuvenation 9
57. Alster TS, Kauvar ANB, Geronemus RG. Histology of high-energypulsed CO2 laser resurfacing. Semin Cutan Med Surg 1996;15:189–93.
58. Alster TS, Nanni CA. Comparison of four carbon dioxide resurfac-ing lasers: a clinical and histopathologic evaluation. Dermatol Surg1999;in press.
59. Alster TS, Garg S. Treatment of facial rhytides with a high-energypulsed carbon dioxide laser. Plast Reconstr Surg 1996;98:791–94.
60. West TB, Alster TS. Improvement of infraorbital hyperpigmentationfollowing CO2 laser resurfacing. Dermatol Surg 1998;24:615–6.
61. Reed JT, Joseph AK, Bridenstine JB. Treatment of periorbital wrin-kles. Dermatol Surg 1997;23:643–8.
62. Alster TS. Comparison of two high-energy pulsed carbon dioxidelasers in the treatment of periorbital rhytides. Dermatol Surg 1996;22:541–5.
63. Ross VE, Grossman MC, Duke D, Grevelkink JM. Long-term re-sults after CO2 laser skin resurfacing: a comparison of scanned andpulsed systems. J Am Acad Dermatol 1997;37:709–18.
64. Alster TS, Rosenbach A, Huband L. Improvement in dermatochala-sis with high-energy, pulsed CO2 laser cutaneous resurfacing. Der-matol Surg 1999;in press.
65. Bernstein LJ, Kauvar ANB, Grossman MC, et al. The short- andlong-term side effects of carbon dioxide laser resurfacing. DermatolSurg 1997;23:519–25.
66. Nanni CA, Alster TS. Complications of cutaneous laser surgery: areview. Dermatol Surg 1998;24:209–19.
67. Ho C, Nguyen Q, Lowe NJ, Griffin ME, et al. Laser resurfacing inpigmented skin. Dermatol Surg 1995;21:1035–7.
68. Monheit GD. Facial resurfacing may trigger the herpes simplex vi-rus. Cosmetic Dermatol 1995;8:9–16.
69. Waldorf HA, Kauvar AN, Geronemus RG. Skin resurfacing of fine
to deep rhytides using the char-free carbon dioxide laser in 47 pa-tients. Dermatol Surg 1995;21:940–6.
70. Sriprachya-Anunt S, Fitzpatrick RE, Goldman MP, et al. Infectionscomplicating pulsed carbon dioxide laser resurfacing for photoagedfacial skin. Dermatol Surg 1997;23:527–36.
71. Weinstein C. Ultrapulse carbon dioxide laser removal of periocularwrinkles in association with laser blepharoplasty. J Clin Laser MedSurg 1994;12:205–9.
72. Biesman BS. Laser-assisted blepharoplasty. In: Alster TS, ApfelbergDB, eds. Cosmetic Laser Surgery, 2nd ed. New York: John Wiley,1998:141–53.
73. David LM. The laser approach to blepharoplasty. J Dermatol SurgOncol 1988;14:741–6.
74. Hruza GJ, Fitzpatrick RE, Dover JS. Laser skin resurfacing. In:Arndt KA, Dover JS, Olbricht SM, eds. Lasers in Cutaneous andAesthetic Surgery. Philadelphia: Lippincott-Raven, 1997:262–85.
75. Drnov ek-Olup B, Vedlin B. Use of Er:YAG laser for benign skindisorders. Lasers Surg Med 1997;21:13–9.
76. Walsh JT, Flotte TJ, Deutsch TF. Erbium:YAG laser ablation of tis-sue: effect of pulse duration and tissue type on thermal damage. La-sers Surg Med 1989;9:314–26.
77. Teikemeier G, Goldberg DJ. Skin resurfacing with the erbium:YAGlaser. Dermatol Surg 1997;23:685–7.
78. Ross VE. The erbium laser in skin resurfacing. In: Alster TS, Apfel-berg DG, eds. Cosmetic Laser Surgery. New York:John Wiley1998;97–84.
79. Alster TS. Comparison of six erbium:YAG lasers for cutaneous re-surfacing: a clinical and histopathological evaluation. Lasers SurgMed 1999;in press.
80. Alster TS. Extended clinical experience with erbium:YAG cutane-ous laser resurfacing. Lasers Surg Med 1998;Suppl. 10:34.
s̆