Embed Size (px)
Citation preview

Perioperative VTE prophylaxis (ACCP 9th edition Guidelines)
Gamal Marey SUNY Downstate Medical Center
10/16/2014
www.downstatesurgery.org

Case Presentation
• 75 y/o AAM • Rectal bleeding & obstructive symptoms 11/12 • Obstructing mass in the descending colon, s/p
left hemicolectomy, Hartmann’s procedure 11/2012
• Path. complicated diverticulitis • Hospital course complicated by urosepsis and B/L
PEs • Elective Hartmann colostomy reversal on 9/14
www.downstatesurgery.org

Case Presentation
• PMH- HTN, BPH, COPD, cardiomyopathy, PE 11/12 Coumadin x 18 mons.
• PSH- umbilical hernia repair, Hartmann’s procedure
• Medications- Enalopril, Doxazosin, Carvedilol, Iron
• Allergy- NKDA • SH- former smoker • FH- not relevant
www.downstatesurgery.org

Labs
• CBC- 4.3/11.9/38/314 • BMP- 139/4.6/107/27/21/1.15/100 • LFTs- 7.3/4.0/22/13/66/0.4 • Coags- 14.3/40.3/1.4
www.downstatesurgery.org

VTE Risk Factors Assessment • Age 75 3 • Lung dis. 1 • Major surgery > 45 min. 2 • History of PE. 3 • Caprini score : 9 • Operation Type 4 • ASA 2 • Work RUV2 • Wound class 1 • HCT<38 1 • Rogers score : 10
www.downstatesurgery.org

pre-op. 5000 SC heparin (one dose) Intraop. Intermittent pneumatic compression devices Post-op. 40 mg lovenox Daily
www.downstatesurgery.org

Postop. Course
• POD#1- clear liquid diet • POD#2- Regular diet • POD3- Discharged home with VNS
www.downstatesurgery.org

?
www.downstatesurgery.org

Outlines
• Epidemiology • Pathophysiology • Risk factors • Symptoms • Diagnosis • Prevention guidelines • Summary
www.downstatesurgery.org
VTE= DVT+PE
www.downstatesurgery.org

Epidemiology
• 350.000 to 600.000 Americans suffer each year from DVT and PE
• 100.000 death 2ry to PE • most common preventable cause of
hospital death Never events. # 1 priority to improve safety in hospitals
www.downstatesurgery.org

Epidemiology • Incidence of symptomatic VTE after
abdominal surgeries occurs up to 3.1% with risk of fatal perioperative PE 0.8%
• Incidence of asymptomatic DVT 25-30% in General surgery patients 20-30% PTS
• 70 % VTE after hospital discharge (within 90 days). Risk 10-50 times
www.downstatesurgery.org

2003 Nationwide Inpatient Sample
Surgical patients with LOS>2 days 7.8 million 44% low risk 14% moderate risk 24% high risk 17% very high risk Many surgical patients at risk for VTE Anderson et al. Am J Hematol. 2007;82:777-782
www.downstatesurgery.org

Pathophysiology
• Anticoagulants (prostacyclin, thrombomodulin, heparin proteoglycan)
• Flow • Endothelial integrity Procoagulant and proinflammatory conditions involving tissue factor, P-selectin, platelets, monocytes, granulocytes, microparticles
www.downstatesurgery.org

Virchow’s Triade www.downstatesurgery.org

•
www.downstatesurgery.org

Surgical Risk factors • Type and extent of surgery or trauma • Type of anesthesia • Duration of hospital stay • A history of previous VTE or cancer • Immobility/ obesity • Perioperative Sepsis • Malignancy • Central venous access • Hyper-coagulable state • Caucasians and African Americans
www.downstatesurgery.org

Risk of DVT in hospitalized patients No PPx with DVT screening
Patient group DVT incidence
Medical Patients 10-20%
Major GYN/Uro/GS 15-40%
Neurosurgery 15-40%
Stroke 20-50%
Hip/Knee surgery 40-60%
Major trauma 40-80%
Spinal cord injury 60-80%
Critical care patients 15-80%
www.downstatesurgery.org

VTE Consequences
• Leg swelling and discomfort • Dyspnea, chest pain, hypoxemia • Extended hospital LOS • Fatal PE (34% diagnosed/ 59% undiagnosed) • Complications of prolonged anticoagulation • Postphlebitic syndrome
Chronic pulmonary HTN (PAP>25 mmhg. Persists 6 months after PE
www.downstatesurgery.org

DVT Diagnosis
Physical exam Pain, edema, erythema, tenderness, fever,
prominent superficial veins, Homan’s sign Imaging Duplex ultrasound
The ACCP guidelines recommend against routine
screening for VTE with Doppler ultrasonography before discharge if the patient is asymptomatic.
www.downstatesurgery.org

Perioperative VTE Prevention
• Patient specific factors/ Risk Stratification. using evidence based scoring systems • Procedure Specific factors • prophylaxis Based on RA, risk/benefit, efficacy/safety and
evidence based guidelines
www.downstatesurgery.org

Rogers VTE Risk Assessment Grading System
www.downstatesurgery.org
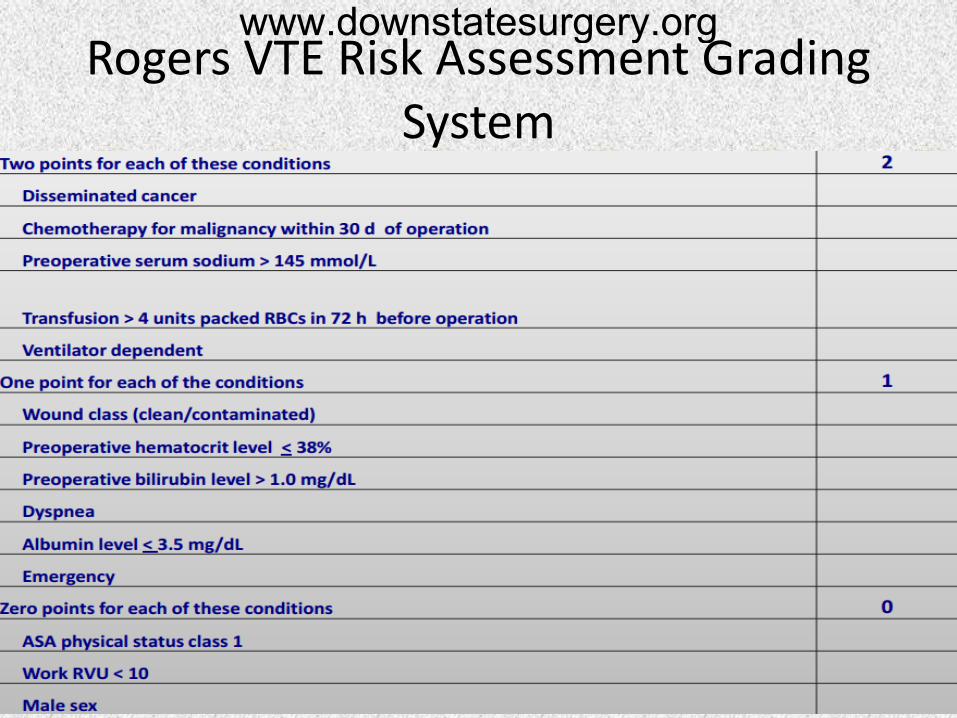
Rogers VTE Risk Assessment Grading System
www.downstatesurgery.org

Caprini VTE Risk Assessment Grading System
www.downstatesurgery.org

Bahl et al. Ann Surg. 2010;251:344-350
www.downstatesurgery.org

Prevention of VTE
Mechanical prophylaxis • Intermittent pneumatic compression therapy • Continous external compression therapy Pharmaco-prophylaxis • Low dose Unfractionated heparin (UFH) • Low molecular weight heparin (LMWH) • Fondparinux • New oral anticoagulants • Warfarin • Aspirin Vena Caval interruption (EAST)
www.downstatesurgery.org

Evidence: anticoagulant thrombo-
prophylaxis in general surgery • Unfractionated heparin (UFH) reduces risk of
fatal PE by 66% • Low-molecular weight heparin (LMWH)
reduces risk of symptomatic VTE by 80% in patients undergoing abdominal surgery
• Prophylactic anticoagulants reduce the risk of silent DVT by 30-70%
www.downstatesurgery.org

UFH vs. LMWH Non-randomized prospective- laparoscopic gastric bypass 238 –UFH 5,000 units TID; 238 enoxaparin 40mg BID 1 PE in UFH Postop transfusion: enoxaparin vs UFH: 6% vs 1% Conclusion Equivalent efficacy for VTE prophylaxis LMWH- better Biovability and more predictable effect Singh, Podolsky et al. Obesity Surgery (2012). 22:4
www.downstatesurgery.org

UFH vs. LMWH
LMWH UFH More expensive Less expensive less frequent dosing More dosing Longer half life Shorter half life Contraindicated in renal failure Greater safety in pts with
epidural catheters
Lower risk of HIT Higher risk of HIT
www.downstatesurgery.org

www.downstatesurgery.org

ACCP 9th Edition Guidelines General and abdominal-pelvic surgery
• Caprini = 0 / Rogers Score: < 7 ( very low VTE risk <0.5%)
• Ambulation • No pharmacological (1B) or mechanical ppx
(2C) is needed Harms > benefits (4-10 bleeds/1000 pts vs. 0-3
nonfatal VTE)
www.downstatesurgery.org

ACCP 9th Edition Guidelines General and abdominal-pelvic surgery
• Caprini=1-2/ Rogers Score: 7-10 ( Low VTE risk ~ 1.5%) • Use mechanical ppx (IPC) over nothing (2C) • Harms = benefits with pharmacologic ppx
(19/1000 vs. 13/1000)
www.downstatesurgery.org

ACCP 9th Edition Guidelines General and abdominal-pelvic surgery
• Caprini=3-4/ Rogers Score: >10 (moderate VTE risk ~ 3%)
• Not at high bleeding risk, use LMWH (2B), UFH (2B), or mechanical ppx (IPC)(2C) over none
– 2 fold more VTE prevented than bleeding events • High bleeding risk, use mechanical ppx (2C)
www.downstatesurgery.org

ACCP 9th Edition Guidelines General and abdominal-pelvic surgery
• Caprini >5 (high VTE risk ~ 6%)
• Not at high bleeding risk, use LMWH (1B), UFH (1B), and add mechanical ppx (2C)
• High bleeding risk, use mechanical ppx (2C) until bleeding risk less; then start pharmaco-ppx.
www.downstatesurgery.org

ACCP 9th Edition Guidelines General and abdominal-pelvic surgery
• Abdominal or pelvic surgery for cancer • History of VTE • Spinal cord injury Extended Duration thrombo-ppx Recommend LMWH x 4 weeks (1B)
www.downstatesurgery.org

• Cardiac: similar, but IPC for non complicated po course; add pharmacologic for complicated po course (2C)
• Thoracic: pharmacologic (2B) and IPC (2C) • Trauma: IPC + pharmacologic prophylaxis (2B)
IVC filter should NOT be used for primary prevention (2C)
www.downstatesurgery.org

ACCP 9th Edition Guidelines (Critically ill medical patients)
• At High risk of thrombosis, use LMWH, LDUH, or fondaparinux (1B)
• At High risk for bleeding, Mechanical ppx (IPC) (2C)
www.downstatesurgery.org
Pharmacologic Thrombo-prophylaxis Considerations
• UFH – Initiate 1-2 hours prior to induction of general anesthesia – TID dosing superior to BID dosing • If pharmacologic thrombo-prophylaxis is
indicated, continue until hospital discharge or at least 7 days postoperatively
www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

www.downstatesurgery.org

Relative Contraindications to pharmacologic prophylaxis
• Severe head injuries • Nonoperatively managed liver or spleen injuries • Renal failure • Spinal column fracture with epidural hematoma • Severe thrombocytopenia and coagulopathy Chest. 2012; 141;e227S-e277S
www.downstatesurgery.org

Treatment of Acute VTE
• Delay in initiation of therapeutic anti-coagulation >24 hrs is associated with increased rate of VTE
• Use LMWH or fondaparinux over IV UFH (2C) • Use anticoagulant therapy over systemic
thrombolysis or venous thrombectomy (2C) • Contraindication to anti-coagulation, an IVC
filter is recommended (1B)
www.downstatesurgery.org

Treatment of Acute VTE
Kearon C, et al. Chest 2008; 133 (6 suppl):454S-545S.
Duration Grade
1st VTE 2ry to reversible factor (provoked)
3 mon. 1A
1st VTE unprovoked -At the end of 3 mon. -If no CI -During long term Rx
At least 3 mon. Assess for long term Rx Long term Rx Assess Risk/benefit
1A 1C 1A 1C
Recurrent VTE Long term Rx. 1A
VTE 2ry to cancer Long term Rx. LMWH during 1st 3-6 mon., then anticoagulate as long as the cancer is active
1A 1C
www.downstatesurgery.org

Strategies to improve VTE ppx
• Hospital policy of risk assessment • Electronic alerts to prevent VTE • computer decision-support systems • preprinted orders • Reliable data collection and performance
tracking • periodic audit and feedback
www.downstatesurgery.org

NEW ENGLAND SURGICAL SOCIETY ARTICLES Reducing Postoperative Venous
Thromboembolism Complications with a Standardized Risk-Stratified Prophylaxis Protocol
and Mobilization Program Michael R Cassidy, MD, Pamela Rosenkranz, RN, BSN, MEd, David McAneny, MD, FACS
• Standardized electronic physician orders • Caprini risk stratification. The derived scores
dictate the nature and the duration of VTE ppx • comparing 2 years before and after
implementing trial with NSQIP VTE outcomes • DVT decreased by 84% from 1.9% to 0.3% • PE fell by 55% from 1.1% to 0.5%
www.downstatesurgery.org

Conclusion
• VTE remains a substantial health problem in the US
• prophylaxis remains underutilized • VTE risk factor stratification on admission • Identify contraindications to prophylaxis • Order risk appropriate VTE prophylaxis • Reassess VTE risk factors and contraindications
during hospital stay • IVC filters are not recommended as primary VTE
prophylaxis
www.downstatesurgery.org
References - White RH, Zhou H, Romano PS. Incidence of symptomatic venous thromboembolism after different elective or urgent surgical procedures. Thromb Haemost 2003; 90:446. - Sandler DA, Martin JF. Autopsy proven pulmonary embolism in hospital patients: are we detecting enough deep vein thrombosis? J R Soc Med 1989; 82:203. - Martino MA, Borges E, Williamson E, et al. Pulmonary embolism after major abdominal surgery in gynecologic oncology. Obstet Gynecol 2006; 107:666. - Dismuke SE, Wagner EH. Pulmonary embolism as a cause of death. The changing mortality in hospitalized patients. JAMA 1986; 255:2039 - Bergqvist D et al.Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N. Engl J Med. 2002; 346 (13): 975-980 - Pannucci CJ,et al. Postoperative enoxaparin prevents symptomatic venous thromboembolism in high risk plastic surgery patients. Plast Reconstr Surg. 2011 Nov;128(5):1093-103.
www.downstatesurgery.org

Q- what is the most common inherited thrombophilia ?
A- Antiphospholipid antibodies B- Antithrombin III deficiency C- Protein C/S deficiency D- Factor V Leiden E- Prothrombin gene 20210A mutation F- Hyperhomocystinemia
www.downstatesurgery.org

Q- what is the most common inherited thrombophilia ?
A- Antiphospholipid antibodies B- Antithrombin III deficiency C- Protein C/S deficiency D- Factor V Leiden E- Prothrombin gene 20210A mutation F- Hyperhomocystinemia
www.downstatesurgery.org

Thank you
www.downstatesurgery.org