Embed Size (px)
Citation preview
Perioperative Pain Management
Dr. Mahmoud Abdel-Khalek
What is pain?
An unpleasant sensory and emotional
experience associated with actual or
potential tissue damage, or described
in terms of such damage
IASP Pain Definition (1994, 2008)IASP: International Association for the study of Pain

Introduction: Nociception

Introduction: NociceptionRefers to the detection, transduction and transmission of
noxious stimuliSubstances generated from thermal, mechanical or
chemical tissue damage, activate free nerve endings, which we refer to as nociceptors
These afferent fibers have their cell body located in the dorsal root ganglion
From DRG axons go into dorsal horn of the spinal cord where axons synapse with the second order neuron as well as with regulatory interneuron. In addition synapses occur with the cell bodies of the sympathetic nervous system and ventral motor nuclei, either directly or through the internuncial neurons

The cell body of the second order neuron lies in the dorsal horn. Axonal projections of this neuron cross to the contralateral hemisphere of the spinal cord and ascend to the level of the thalamus
In the thalamus, the second order neuron synapses with a third order afferent neuron, which sends axonal projections into the sensory cortex
Postoperative Pain
Postoperative pain can be divided into acute pain and chronic pain:
Acute pain is experienced immediately after surgery (up to 7 days);
Pain which lasts more than 3 months after the injury is considered to be chronic.
Why Treat Pain?Basic human right!↓ pain and suffering↓ complications – next slide↓ likelihood of chronic pain development↑ patient satisfaction↑ speed of recovery → ↓ length of stay → ↓ cost
↑ productivity and quality of life

Adverse Effects of Poor Pain ControlCVS: MI, dysrhythmiasRespiratory: atelectasis, pneumoniaGI: ileus, anastomotic failureEndocrine: “stress hormones”Hypercoagulable state: DVT, PEImpaired immunological state:Infection, cancer, delayed wound healing
Psychological:Anxiety, Depression, Fatigue

PathophysiologyInadequately treated pain following chest& abdominal incisions → diaphragmatic muscle splinting → ↓ ability to cough& clear secretions → atelectasis, hypoxemia& pneumonia
Nociceptive stimuli reaching the spinal cord → sympathetic stimulation → hypertension, tachycardia → ↑ heart work load → ↑ oxygen demand → myocardial ischemia in vulnerable patients& myocardial infarction
PathophysiologyAlso increased sympathetic tone → ↑ intestinal secretions& slows gut motility& ↑ smooth muscle tone → gastric stasis, nausea and vomiting, ileus and urinary retention
Poorly controlled acute pain → initiation and maintenance of stress response seen with the trauma of major surgery → hypercoagulability → DVT, p. embolism, MI, ↓ immunity, hypermetabolism, Hyperglycemia, protein catabolism and delayed wound healing

Pain Assessment
Pain HistoryO – Onset P – Provoking / Palliating factorsQ – Quality / QuantityR – RadiationS – Severity T – Timing

Pain Assessment Severity: Visual Analogue Scale

Severity of postoperative pain

Pain Assessment Current Pain Medications
Accuracy and detail are very important: Name, dose, frequency, route i.e. Oxycontin 10mg PO TID
Co-existing conditions Renal disease: avoid morphine, NSAID’s Vomiting: avoid oral forms of medication
Drug allergies Document drug, adverse reaction and severity
Intolerances
Nausea / vomiting, hallucinations, disorientation, etc.

Methods to Treat Pain
Pharmacologic Medications (po, iv, im, sc, pr, transdermal)
Acetaminophen NSAIDs e.g. Aspirin, diclofenac, ibuprofen.. etc. Opioids e.g. Morphine, pethidine, fentanyl, codeine.. etc. Gabapentin NMDA antagonists e.g. ketamine Alpha-2 agonists
Procedures Regional Anesthesia LA infiltration at incision site
Surgical InterventionRemoval of cause of pain e.g. distended urinary bladder
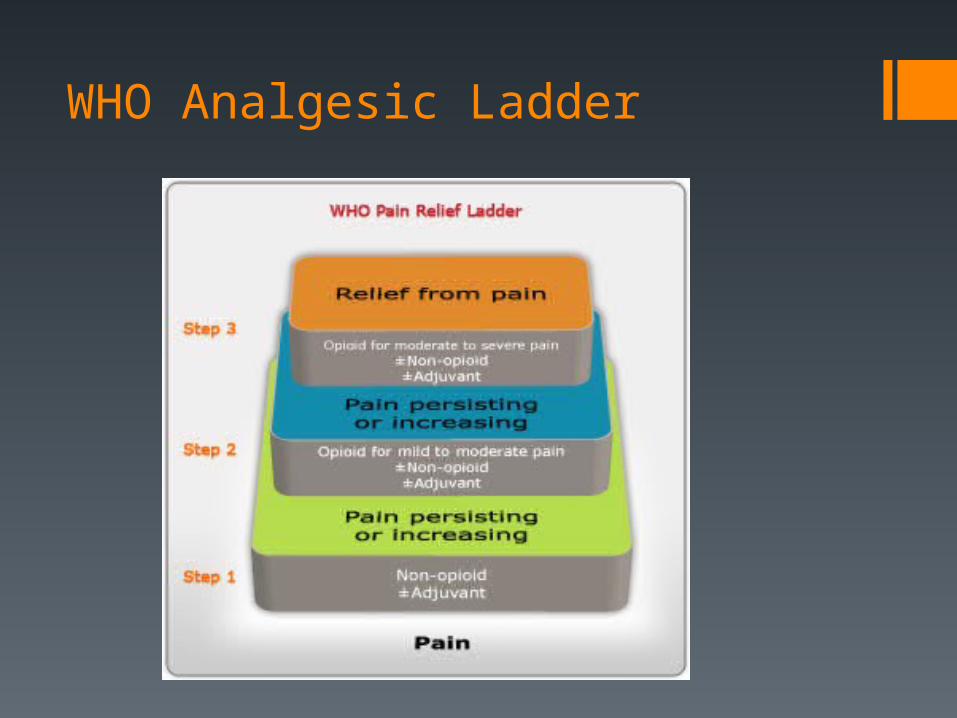
WHO Analgesic Ladder

Acetaminophen (aka Paracetamol)
First-line treatment if no contraindication It is relatively safe It is analgesic and antipyretic Mechanism: thought to inhibit prostaglandin synthesis in
CNS → analgesia, antipyretic It does not cause gastric irritationTypical dose: 650 to 1000 mg PO Q6HMax dose: 4 g / 24 hrs from all sourcesWarning: ↓ dose / avoid in those with liver damage

NSAIDsAlso, first-line treatmentMechanism
Block cyclooxygenase (COX) enzyme → ↓ prostaglandin synthesis
COX-2 → Prostaglandins → pain, inflammation, feverCOX-1 → Prostaglandins → gastric protection, hemostasis

NSAIDs
Warnings: ↓dose / avoid ifGI ulceration Bleeding disorders / CoagulopathyRenal dysfunctionAsthmaAllergy

Opioids
They are highly effective class of analgesics which operates at several levels in the nervous system
Intramuscular morphine or meperidine on prn basis remains the most popular form of acute postoperative pain management at most hospitals

Opioids: mechanism of action
They dampen the transmission of nociceptive stimuli by binding to opioid receptors within substantia gelationsa of the dorsal horn of spinal cord
They release inhibitory neurotransmitters such as noradrenaline, serotonin and GABA
Decrease inflammatory response in the periphery Affect mood and anxiety

Intramuscular opioid administration limitations
Responsibility for management of pain is delegated to the nursing staff, who err on the side of caution in the administration of opioids. They tend to give too small a dose of drug too infrequently because of exaggerated fears of producing ventilatory depression or addiction.
Because the administration of drugs is left entirely to the discretion of the nursing staff, the degree of empathy between nurse and patient affects analgesic administration.
Because the measurement of pain is difficult, it is seldom possible to adjust the dose of drug to match the extent of pain.
There are enormous variations in the extent of analgesic requirements depending upon the type of surgery, pharmacokinetic variability pharmacodynamic variability, etc.

Opioids: Side effects Nausea / Vomiting Sedation Respiratory Depression Pruritus Constipation Urinary Retention Ileus Tolerance
Opioids
MorphineMost commonly prescribed opioid in hospitalMetabolism:
Conjugation with glucuronic acid in liver and kidney Morphine-3-glucuronide (inactive) Morphine-6-glucuronide (active)
Impaired morphine glucuronide elimination in renal failure
Prolonged respiratory depression with small doses Due to metabolite build-up (morphine-6-glucuronide)

Opioids
Hydromorphone (Dilaudid)Better tolerated by elderly, better S/E profilePreferred over morphine for renal disease patientsLow cost, IV and PO forms available
OxycodoneGood S/E profile, but $$PO form onlyPercocet (oxycodone + acetaminophen)
OpioidsCodeine
1/10th Potency of morphineMetabolized into morphine by body Ineffective in 10% of Caucasian patentsChallenge with combination formulations
Meperidine (Demerol)Not very potentDecreases seizure threshold, dystonic reactionsNeurotoxic metabolite (normeperidine)Avoid in renal disease

Opioids - Formulations
Short acting formsNeed to be dosed frequently to maintain consistent
analgesia
Controlled Release formsProvides more consistent steady state levelHelpful for severe pain or chronic pain situationsNever crush / split / chew controlled release pills
Management of Opioid Overdose
Ddx:Seizure, strokeHypoxia, HypercarbiaHypotensionOther medication effectSevere electrolyte or acid base abnormalitiesMISepsis…..etc.

Management of Opioid Overdose
For ↓level of consciousness, somnolent patient:Stimulate patient Vitals/Monitors/LinesAirway BreathingCirculation CODE BLUE?

Management of Opioid Overdose
Opioid Reversal Naloxone - opioid antagonistReverses effects of opioid overdose (for 30-45min)MUST BE diluted before use: 0.4mg ampule Dilute: 1mL Naloxone + 9mL Saline = 0.04 mg/mL
Give 0.04 to 0.08 mg (1 to 2 mL) IV q3-5 minutes If no change after 0.2mg, consider other causes
Opioids: PCAPatient-controlled analgesia (PCA) permits the patient to
administer the delivery of his own analgesic by activating a button, which then triggers the intravenous delivery of a predetermined dose of an opioid such as morphine.
Limits are set on the number of doses per four-hour period and on the minimum time that must elapse between doses (lockout interval).
The pharmacokinetic advantage of PCA is that by self administering frequent, small doses, the patient is able to come closer to achieving a steady state analgesic level in the blood, avoiding the high peaks and low troughs that can be found with intermittent (intramuscular) opioid administration.
Benefits of PCAPCA has been shown to provide equivalent analgesia with
less total drug dose, less sedation, fewer nocturnal disturbances and more rapid return to physical activity.
In addition, patient acceptance is high since patients have a significant level of control over their pain management.
PCA analgesia is not without side effects, the most common of which is nausea and vomiting, Excessive sedation and pruritus
Standardized orders provide “as needed” orders for medications to counteract both nausea and pruritus.

Benefits of PCAAlthough it does not obviate the need for close monitoring,
PCA frees nursing personnel from administering analgesic medication.
Since patients titrate their own therapy with PCA, they must be capable of understanding the principle, willing to participate and physically able to activate the trigger. Consequently, use is prohibited at the extremes of age as well as in very ill or debilitated patients
Typically, the PCA modality is used for 24-72 hours. The patient must be capable of oral (fluid) intake prior to
converting from PCA to oral analgesics

Opioids – PCA

Management of Opioid Side Effects
Nausea / VomitingOndansetron (Zofran)Dimenhydrinate (Gravol)Metoclopramide (Maxeran)Changing medication(s) / ↓ dose
PruritusDiphenhydramine (Benadryl)Changing medication(s) / ↓ dose
Gabapentin
Anti-epileptic drug, also useful in:Neuropathic pain, Postherpetic neuralgia, CRPS
Blocks voltage-gated Ca channels in CNSAdditive effect with NSAIDsReduces opioid consumption by 16-67%Reduces opioid related side effectsDrowsiness if dose increased too fast

Regional Anesthesia
Involves blockade of nerve impulses using local anesthetics (LA)
LA bind sodium channels preventing propagation of action potentials along nerves
Wide variety of LA with different characteristics: i.e. Lidocaine – fast onset, short duration of action i.e. Bupivacaine (Marcaine) – slow onset, longer
duration

Central neuraxial analgesiaCentral neuraxial analgesia involves the delivery of local anesthetics and/or opioids to either the intrathecal (spinal) space or the epidural space.
Opioids added to the (spinal) local anesthetic solution provide long-lasting analgesia after a single injection, lasting well into the post-operative period
The duration of effect is directly proportional to the water-solubility of the compound, with hydrophilic compounds such as morphine providing the longest relief
Epidural catheters are safe and easy to insert

Epidural Analgesia
Epidural analgesia can be used to provide pain relief for days through the infusion of a solution containing local anesthetic, opioid or both. The infusion is usually delivered continuously
Continuous epidural infusions provide a steady level of analgesia while reducing the side-effects associated with bolus administration
Overall, epidural analgesia can provide highly effective management of post-operative pain
Benefits of Epidural AnalgesiaSuperior analgesia to IV, PCA in open abdominal procedures & specifically in colorectal surgery
Reduce incidence of paralytic ileusBlunt surgical stress responseImproves dynamic pain reliefReduces systemic opiate requirements

Regional AnesthesiaPeripheral Nerve Blocks
Upper Limb: Brachial plexusLower Limb: Femoral, sciatic, popliteal, ankleAbdomen: TAP blocksThoracic: Paravertebral, intercostal blocks
Use of Ultrasound Imaging has revolutionized peripheral nerve blockadeSafety?Accuracy / Improved SuccessEfficiency
Contraindications to Neuraxial BlockadeAbsolute:
Pt refusal or allergy to LA Uncorrected hypovolemia Infection at insertion site Raised ICP Coagulopathy
Relative: Uncooperative patient Fixed cardiac output states Systemic infection/sepsis Unstable neurological disease Significant spine abnormalities or surgery

Peripheral Nerve Blocks Almost any peripheral nerve that can be reached with a needle
can be blocked with local anesthetics The brachial plexus, intercostal and femoral nerves are examples
of nerves which are commonly blocked to provide post-operative analgesia
A block may be used as the sole method of post-operative analgesia or it may be useful as an adjunct to decrease the required dose of systemic opioids
The major drawback of this method of post-operative analgesia is that the duration of effect of a single block is limited, usually to less than 18 hours
A typical example of the use of a peripheral nerve block for post-operative pain would be the use of a femoral/sciatic nerve block for a patient undergoing total knee arthroplasty. The block would be augmented with oral opioids and other adjuncts

Summary
Accurate pain assessmentUse Multimodal pain managementSuperior analgesia, ↓ side effects means:
Improved patient satisfactionBetter rehabilitationEarlier functional returnEarlier discharge from hospital↓ likelihood of chronic painReduced health care costs

Thank you