Embed Size (px)
Citation preview

4/28/17
1
PerioperativeFluidManagementinERPs
RobertH.Thiele,M.D.AssistantProfessorUniversityofVirginia
FirstDoNoHarm
• Intravenousfluidsshouldbeconsideredapharmacotherapeutic agent• Justlikeallpharmacotherapeutic agents,theycanbebothbeneficial,andharmful
Brandstrup etal.AnnSurg 238:641,2003

4/28/17
2
FirstDoNoHarm
BellamyMC.BJA97:755,2006
Hypoperfusion Edema
WhatDoesn’tWork?
•MeanArterialPressure• ThereisNOmeaningfulcorrelationbetweenMAPandDO2• WhywouldyouexpectanarbitraryMAPtoimpactclinicaloutcomesintheperioperativeenvironment?

4/28/17
3
WhatDoesn’tWork?
Asfar P.NEJM370:1583,2014
WhatDoesn’tWork?
• CentralVenousPressure
Marik P.Chest134:172,2008

4/28/17
4
WhatDoesn’tWork?
• UrineOutput
AlpertRAetal.Surgery95:707,1984
WhyIsThisSoHard?
ChappellDetal.Anesthesiology109:723,2008

4/28/17
5
WhyIsThisSoHard?
• “Researchsuffersfromalackofstandardization…• Investigatorshavenormallynamedtheirtraditionalregimenthestandardgroupandcompareditwiththeirownrestrictiveideas…• Arestrictiveregimeninonestudyisoftendesignatedasliberalinanothersetup…
• Thisshortcomingpreventsevenpromisingresultsfromimpactingdailyclinicalroutineandmakesanypoolingofthedataimpossible”
ChappellDetal.Anesthesiology109:723,2008
WhyIsThisSoHard?
Gan TJ.Anesthesiology 97:820,2002;Brandstrup etal.AnnSurg 238:641,2003
Hypoperfusion Edema
Gan(Control [4.6L]) Gan
(GDT [5.3L])
Brandstrup(“Restricted”
[3.8L])
Brandstrup(“Liberal”[6.2L])

4/28/17
6
WhyIsThisSoHard?
• Howmuchfluidadministeredmaybelessimportantthanwhenitisgiven• Newfocus:willintravenousfluidimproveDO2?
IntraoperativeFluidManagement
• Paradigmshift• Willintravenousfluidimprovecardiacoutput?• Howdoweknowthis?
• 1)Measure“fluidresponsiveness”
• 2)Measurecardiacoutputcontinuously
ThieleRHetal.CanadianJournalofAnesthesia 62:169,2015

4/28/17
7
TimingisImportant!
• Studiesutilizingfluidresponsivenessdemonstratenoconsistentimpactontotalfluidadministration• Buettner (systolicpressurevariation):
• Nodifferenceinfluidadministrationoroutcome• Benes(strokevolumevariation):
• Morefluidinthegoal-directedtherapy(GDT)group• FewercomplicationsandlowerlactateintheGDTgroup
• Forget(PVI):• 500mLlessfluidintheGDTgroup• Lowerlactateatalltimepoints
Buettner Metal.BJA 101:194,2008;BenesJetal.Crit Care14:R118,2010;Forget Petal.Anesth Analg 111:910,2010
Fluid“Optimization”(SV)
• Premise• MaintainingpatientsatthepeakoftheFrank-Starlingcurve willmaximizedeliveryofoxygenwithoutrequiringinitiationofvasoactivepharmacologicagents
• Process:• Giveasmallamountoffluid• Measurethechangeinstrokevolume• Whenstrokevolumenolongerresponds,theintravascularvolumeis“optimized”
• Disadvantages• Requiresaccuratemeasureofstrokevolume(e.g.esophagealDopplermonitoring[EDM])

4/28/17
8
Fluid“Optimization”(Resp.Var.)
• Premise• Optimizing“recruitable”strokevolumebasedonrespiratoryvariation
• Arteriallinescommon(16%ofpatients)• Masimo PVIrelativelyinexpensiveandnon-invasive(canbeusedonalmostanypatient)
• Disadvantages• DoesnotactuallymeasurechangeinSV• MeaningconfoundedinpatientswithelevatedPVRorRVfailure• Onlyusefulinmechanicallyventilatedpatients• DoesnothavetheevidencebaseenjoyedbyEDM(yet)
EsophagealDopplercontinuouslymonitorscardiacoutputandtheresponsetovolumeadministration
“Pleth VariabilityIndex”monitors“fluidresponsiveness”continuouslybasedonthepulseoximeter waveform
ThieleRHetal.CanadianJournalofAnesthesia 62:169,2015

4/28/17
9
ThieleRHetal.PerioperativeMedicine 5:24,2016
EDMandHospitalStay(RCTs)
RANDOMIZEDCONTROLLEDTRIALS
NineRCTsincluding945Subjects,weightedaverage3.2dayreductioninLOS
Year Author Patients n Outcome
1997 Sinclair Orthopedicsurgery 40 Reducedmeanstay9days
2002 Gan Majorelectivesurgery 100 Reducedmeanstay2days
2002 Venn Orthopedic 90 Reducedmeanstay6days
2005 Wakening Colorectal 128 Decreasedhospitalstay1.5days
2006 Noblett Colorectal 108 Reducedmeanstay2days
2007 Chytra Trauma 162 Reducedmeanstay5days
2011 Pillai RadicalCystectomy 66 Reducedmeanstay4days*(*NS)
2013 Jones LiverResection 91 Reducedmeanstay3days
2013 Li LiverResection 160 Reducedmeanstay1.1days

4/28/17
10
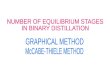
SchematicofEnhancedRecoveryAfterSurgery(Source:NHSEnhancedRecoveryPartnership)
DoYouNeed WantADevice?
“150patientsundergoingelectivecolorectalsurgerywererandomizedtoreceivefluidtherapyaftereitherthegoal
ofnear- maximalSVguidedbyEDorthegoalofzerobalanceandnormalBW”

4/28/17
11
DoYouNeed WantADevice?
SrinivasaBJS100:66,2013
“NotknownwhetherGDFTisofvaluewithinanERprotocolincorporatingfluidrestriction…electivecolectomy…85
patientswererandomized…”
DoYouNeed WantADevice?
• IsGDTsuperiortoa“restrictive”or“zerobalance”approach?• GDT(EDM)v.“zerobalance”(B,S)or“restrictive”(P)• Randomizedtrialsofcolorectalsurgicalpatients• Results(335patientsin3studies)• Nodifferencesincomplications• Nodifferenceinlengthofstay
BrandstrupBJA109:191,2012;SrinivasaBJS100:66,2013;PhanTDAnaesthIntCare42:752,2014

4/28/17
12
DoYouNeed WantADevice?
Pearse RMetal.JAMA 311:2181,2014
Whichgroupwouldyouchoosetobein?
DoYouNeed WantADevice?
Pearse RMetal.JAMA 311:2181,2014

4/28/17
13
DoYouNeed WantADevice?
• ManyindividualshavedemonstratedreducedLOSwithoutadvancedmonitoring• However,thedataonGDT(prospectiveRCTs)ismorecompellingthantheERASdata• Advancedmonitoringallowsyoutocomfortablyadoptafluidrestrictivestrategywithamarginofsafety• Youaremorelikelytodetecttherarepatientwhoisprofoundlyfluidresponsive• Thiswillnotbedetectedina100patientcase-controlstudy
Conclusions
• Intravenousfluidcancauseharm• Traditional(“static”)fluidmanagementstrategiesarebasedonflawedlogicandnotsupportedbymeaningfuloutcomesdata• Advancedhemodynamicmonitoring(“dynamic”indicatorsofvolume)havebeenshowntoimproveoutcomesinGDTstudies• WhetherornotthisholdstrueinthecontextofERASstudiesissomewhatcontroversial
• Fluidresponsivenessmonitorswillallowyoutodetecthypovolemia andprovideamarginofsafety• Ultimatelythedecisionabouthowtomanageintraoperativefluidsisbasedonanindividualizedcost-benefitratio

4/28/17
14
Conclusions
ThieleRHetal.PerioperativeMedicine 5:24,2016