Embed Size (px)
Citation preview
Letters to Editor
85Neurology India | Jan-Feb 2013 | Vol 61 | Issue 1
usually atherothrombosis of the vertebral or anterior spinal artery.[3]
Kirti Parsi, Raghavendra K. Itgampalli1, Suryanarayana A., Kiran Kumar R.2
Departments of Radiodiagnosis, 2Neurology, Yashoda Hospitals, 1Department of Radiodiagnosis, Vijaya Diagnostics,
Hyderabad, Andhra Pradesh, India E‑mail: [email protected]
References
1. Bassetti C, Bogousslavsky J, Mattle H, Bernasconi A. Medial medullary stroke: Report of seven patients and review of the literature. Neurology 1997;48:882‑90.
2. Thijs RD, Wijman CA, van Dijk GW, van Gijn J. A case of bilateral medial medullary infarction bemonstrated by magnetic resonance imaging with diffusion‑weighted imaging. J Neurol 2001;248:339‑40.
3. Bernasconi A, Bassetti C, Bogousslavsky J. Medial medullary stroke: Clinical‑MRI study of 6 patients. Cerebrovasc Dis 1994;4:253.
Access this article onlineQuick Response Code: Website:
www.neurologyindia.com
PMID: ***
DOI: 10.4103/0028-3886.108023
Received: 08-12-2012 Review completed: 08-12-2012 Accepted: 14-12-2012
Periodic lateralized triphasic waves in an adult with isolated hemimegalencephalySir,Hemimegalencephaly is a rare congenital malformation of brain characterized by hamartomatous enlargement of one cerebral hemisphere imparting extreme asymmetry to brain. It usually presents in infancy with seizures, large asymmetric head, development delay, and mental retardation. Rarely, it is diagnosed in adults with epilepsy with or without dysmorphism and mental sub‑normality. Different types of electroencephalographic (EEG) abnormalities are known in these patients. We present here an adult with isolated hemimegalencephaly and characteristic EEG abnormality.
A 26‑year‑old man presented with generalized
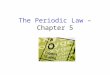
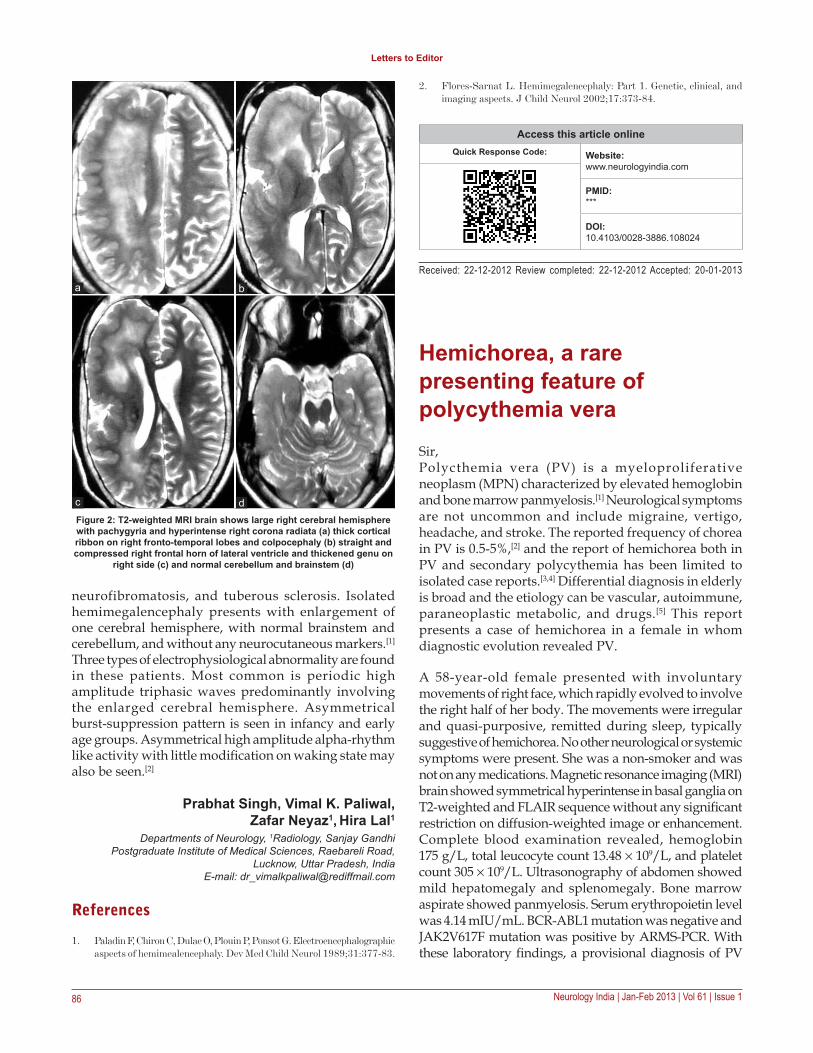
tonic‑clonic seizures since 6 months of age. His seizures remained well controlled on anti‑epileptic drugs and recurred only on drug default. He was born normally, full term at home and cried immediately. Since birth, his parents noted mild weakness of left upper and lower limb. He had delayed motor and mental milestones and achieved sitting, standing, walking, and disyllabic speech at 8 months, 1 year, 2.5 years, and 2 years, respectively. He also had poor scholastic performance. He did not report any family member with seizures, facial dysmorphism, or any neurocutaneous syndrome. On examination, he had normal head size and no skin lesion or dysmorphic facial features. Higher mental functions and cranial nerves were normal. Motor system revealed grade 2 spasticity with grade 4/5 power in left upper and lower limb. All deep tendon jerks on left side were brisk and left planter was extensor. Sensory system examination was normal. His electroencephalogram revealed periodic large amplitude triphasic waves in the right‑sided leads [Figure 1]. Magnetic resonance imaging (MRI) brain revealed large right cerebral hemisphere with pachygyria and hyperintense right corona radiata [Figure 2a], thick cortical ribbon on right fronto‑temporal lobes and colpocephaly [Figure 2b], straight and compressed right frontal horn of lateral ventricle and thickened genu on right side [Figure 2c] and normal cerebellum and brainstem [Figure 2d].
Hemimegalencephaly is classified as isolated, syndromic, or total. Total hemimegalencephaly involves enlargement of ipsilateral cerebellum and brainstem in addition to the cerebral hemisphere. Syndromic hemimegancephaly includes number of neurocutaneous syndromes, where hemimegancephaly exists in addition to several other features. These syndromes include epidermal nevus syndrome, Klippel–Trenaunay–Weber syndrome, Proteus syndrome, hypomelanosis of Ito,
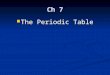
Figure 1: Electroencephalograph obtained by 10‑20 international system of electrode placement reveals periodic large amplitude triphasic waves
occupying predominantly over right cerebral hemisphere
Letters to Editor
86 Neurology India | Jan-Feb 2013 | Vol 61 | Issue 1
2. Flores‑Sarnat L. Hemimegalencephaly: Part 1. Genetic, clinical, and imaging aspects. J Child Neurol 2002;17:373‑84.
neurofibromatosis, and tuberous sclerosis. Isolated hemimegalencephaly presents with enlargement of one cerebral hemisphere, with normal brainstem and cerebellum, and without any neurocutaneous markers.[1] Three types of electrophysiological abnormality are found in these patients. Most common is periodic high amplitude triphasic waves predominantly involving the enlarged cerebral hemisphere. Asymmetrical burst‑suppression pattern is seen in infancy and early age groups. Asymmetrical high amplitude alpha‑rhythm like activity with little modification on waking state may also be seen.[2]
Prabhat Singh, Vimal K. Paliwal, Zafar Neyaz1, Hira Lal1
Departments of Neurology, 1Radiology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Raebareli Road,
Lucknow, Uttar Pradesh, India E‑mail: [email protected]
References
1. Paladin F, Chiron C, Dulac O, Plouin P, Ponsot G. Electroencephalographic aspects of hemimealencephaly. Dev Med Child Neurol 1989;31:377‑83.
Access this article onlineQuick Response Code: Website:
www.neurologyindia.com
PMID: ***
DOI: 10.4103/0028-3886.108024
Received: 22-12-2012 Review completed: 22-12-2012 Accepted: 20-01-2013
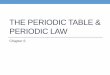
Figure 2: T2‑weighted MRI brain shows large right cerebral hemisphere with pachygyria and hyperintense right corona radiata (a) thick cortical ribbon on right fronto‑temporal lobes and colpocephaly (b) straight and compressed right frontal horn of lateral ventricle and thickened genu on
right side (c) and normal cerebellum and brainstem (d)
dc
ba
Hemichorea, a rare presenting feature of polycythemia veraSir,Polycthemia vera (PV) is a myeloproliferative neoplasm (MPN) characterized by elevated hemoglobin and bone marrow panmyelosis.[1] Neurological symptoms are not uncommon and include migraine, vertigo, headache, and stroke. The reported frequency of chorea in PV is 0.5‑5%,[2] and the report of hemichorea both in PV and secondary polycythemia has been limited to isolated case reports.[3,4] Differential diagnosis in elderly is broad and the etiology can be vascular, autoimmune, paraneoplastic metabolic, and drugs.[5] This report presents a case of hemichorea in a female in whom diagnostic evolution revealed PV.
A 58‑year‑old female presented with involuntary movements of right face, which rapidly evolved to involve the right half of her body. The movements were irregular and quasi‑purposive, remitted during sleep, typically suggestive of hemichorea. No other neurological or systemic symptoms were present. She was a non‑smoker and was not on any medications. Magnetic resonance imaging (MRI) brain showed symmetrical hyperintense in basal ganglia on T2‑weighted and FLAIR sequence without any significant restriction on diffusion‑weighted image or enhancement. Complete blood examination revealed, hemoglobin 175 g/L, total leucocyte count 13.48 × 109/L, and platelet count 305 × 109/L. Ultrasonography of abdomen showed mild hepatomegaly and splenomegaly. Bone marrow aspirate showed panmyelosis. Serum erythropoietin level was 4.14 mIU/mL. BCR‑ABL1 mutation was negative and JAK2V617F mutation was positive by ARMS‑PCR. With these laboratory findings, a provisional diagnosis of PV
Copyright of Neurology India is the property of Medknow Publications & Media Pvt. Ltd. and its content may
not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written
permission. However, users may print, download, or email articles for individual use.