Embed Size (px)
Citation preview

Perils of medical tourism
Dr Theo Gouliouris
Microbiology and Infectious Diseases StRAddenbrooke’s Hospital, Cambridge

Case history
• 55 year old man, Pakistani origin• ESRD secondary to hypertensive nephrosclerosis • 2007 Haemodialysis via AV fistula• 2009 Transplant waiting list

Case history
• Summer 2010 Travelled to Pakistan • August 2010 HCV antibody and PCR positive• Removed from transplant waiting list pending antiviral
therapy• September 2010 commenced on ribavirin 200 mg daily• October 2010 travelled to Pakistan against medical advice

Acute presentation• May 2011 Presented to Addenbrooke’s unwell • Living-related kidney transplant in Pakistan Nov 2010
– Donor and HLA match unclear– Recipient CMV positive
• Complications– ARDS, ventilated in ICU for 4 days– Wound dehiscence and infected perinephric
haematoma, treated with imipenem and colistin– Poor graft function: creatinine 477 mol/L
• Medications: Prednisolone 10mg od, Tacrolimus 3mg/4mg, Mycophenolic acid 720mg bd

Examination
• Vomiting• Febrile T 38.9°C• Tachycardia• Widespread vesicular rash consistent with shingles• Open wound in right iliac fossa, packed, discharging pus• Commenced on empirical piperacillin-tazobactam and
aciclovir• Barrier nursed

Baseline investigationsBlood test Result Normal range
Urea 19.9 0.0-7.5 mmol/l
Creatinine 398 35-125 mol/l
Albumin 29 30-51 g/l
ALP 145 30-135 U/l
ALT 6 0-50 U/l
Bilirubin 6 0-17 mol/l
CRP 59 0-6 mg/l
WCC 6.8 4.0-11.0x109/l
Neutrophils 6.3 2.0-8.0x109/l
Lymphocytes 0.26 1.0-4.5x109/l
Haemoglobin 8.8 g/dl
Platelets 258 150-400x109/l
PT 13.4 9.8-12.6 s

CT abdomen and pelvis

Management and progress
• Ultrasound-guided drainage of 3 largest collections• Clinical deterioration
– Ongoing fever– Productive cough– CXR pulmonary infiltrates– Metabolic acidosis– Diarrhoea
• Mycophenolate and tacrolimus stopped • Transplant nephrectomy 12 days post-admission

Microbiology / virology results
• Skin vesicles: VZV DNA detected• Blood: Low-grade CMV viraemia• Stool: Norovirus detected• Wound swabs:
– Multidrug-resistant ESBL-producing Klebsiella pneumoniae and E. coli
– vancomycin-resistant Enterococcus faecium• Peri-nephric abscess aspirates
– Filamentous mould - Aspergillus terreus (amphotericin B resistant)
– Meropenem-resistant Klebsiella pneumoniae

Antimicrobial MIC (mg/l) S/I/R Breakpoint
Ampicillin >64 R 8
Amoxillin/Clavulanate 64 R 8
Cefotaxime >256 R 1-2
Ceftazidime >256 R 1-8
Ertapenem >16 R 0.5-1
Imipenem 16 R 2-8
Meropenem 16 R 2-8
Aztreonam Not done R 2-4
Piperacillin/Tazobactam >64 R 16
Colistin 32 R 2
Ciprofloxacin >8 R 0.5-1
Gentamicin 1 S 8-16
Amikacin 2 S 8-16
Tobramycin 4 I 2-4
Tigecycline 0.5 S 1-2
Fosfomycin 4 S (32)
Klebsiella pneumoniae antibiogram

Cycle5 10 15 20 25 30 35
Norm. Fluoro.
0.6
0.5
0.4
0.3
0.2
0.1
0.0
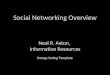
Real-time PCR detection of New Delhi metallo- beta-lactamase
Purple - control NDM positive extract DNAGreen - clinical isolate extract DNABlack/blue - PCR negative control isolates
Courtesy of R. Swayne and M.Ellington, Cambridge HPA

Histopathology results

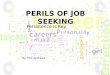
GII.4 – Most prevalentnorovirus in humans
Adapted from Glass et al. Norovirus Gastroenteritis. N Engl J Med 2009;361:1776
GII Cluster
GI Cluster
GIV Cluster
Courtesy of M. Curran, Cambridge HPA

Further management
• Recurrent collections requiring drainage procedures• Antimicrobial therapy complex – renal impairment, drug
interactions and toxicity, multiple MDR organisms, need for prolonged treatment
• Long courses of tigecycline (63d), amikacin (45d) and voriconazole

Transplant tourism
• Common– 5 to 10% of kidney transplants performed worldwide – Pakistan 2006: 2/3 of 2000 transplants for foreign
recipients1
• Ethical issues– Organ trafficking– Transplant commercialism
• Declaration of Istanbul on Organ Trafficking and Transplant Tourism, 2008
1. Naqvi et al, Transpl Int 2007; 20: 934

Literature review of outcomes
• 21 case series between 1990 and 2012• Total no. of patients 1331 (range 5 – 515) • Countries: India (62%), Pakistan (13%), China (12%),
Philippines (3%), Egypt (3%), Iran • Graft 1-yr survival rate 86.9% (range 60-100%)• Patient 1-yr survival rate 91.9% (range 68-100%) • Acute rejection common 23.4% (range 10-50%)

Infective complications
• Infections common, esp. CMV, wound infections• Significant risk of BBV acquisition
– HIV 0.8%– HBV 4%– HCV 16%
• Risk of TB 3%• Malaria reported (1.8%)• Little emphasis on resistant organisms (mainly ESBL
producing Enterobacteriaceae, one panresistant Acinetobacter baumannii)

Aspergillus infections in renal transplants
• 1.3% one-year cumulative incidence of invasive fungal infections in renal transplants1
• 14% of IFI caused by Aspergillus spp. (<5% A. terreus)• Usually pulmonary or disseminated infection• Recognised association with transplant tourism2
• 17 cases identified• Infection in transplanted graft 35%• Graft loss or death 76%
1. Pappas et al, CID 2010; 50: 11012. Shoham et al, Transplant ID 2010; 12: 371

Outcome
• Discharged from hospital on day 82• Last clinical review: wound completely healed, incisional
hernia• HCV RNA negative

Conclusions
• Transplant tourism is associated with significant morbidity and mortality, particularly related to infection
• NDM-1 producers, pose a significant risk to patients who travel to the Indian subcontinent for medical treatment
• Patients returning following hospitalisation in endemic countries should be screened for the presence of resistant bacteria and isolated
• Rapid molecular detection methods for antimicrobial resistance facilitate prompt diagnosis

Acknowledgments
• Dr S.H. Aliyu, Dr S. Ojha, Prof S. J. Peacock, Dr M.E. Török• Renal Transplant team• Microbiology and Infectious Diseases colleagues• Dr Matthew Ellington, Dr Rosie Swayne (Cambridge HPA)• Dr Martin Curran (Cambridge HPA)• Dr Verena Broecker (Histopathology Department)• Dr Winterbottom (Radiology Department)