Embed Size (px)
Citation preview

Pericardiocentesis practice in the United Kingdom
S. Balmain,1 N. M. Hawkins,2 M. R. MacDonald,3 F. G. Dunn,2 M. C. Petrie3
Introduction
In individual centres pericardiocentesis is a relatively
infrequent procedure. Whether or not to drain an
effusion is often a difficult clinical decision (1,2).
Methods of drainage depend on individual physi-
cian’s experience and preference, as well as available
facilities. Assessment of ‘real-life’ practice is limited.
Who performs pericardiocentesis, their procedural
preferences, and the perceived indications for drain-
age are unknown. We performed a survey to evaluate
the practice of pericardiocentesis among UK cardiol-
ogists.
Methods
In March 2003, 640 questionnaires (Appendix 1) were
sent to all cardiology consultants, specialist registrars
and staff grades in the UK Directory of Cardiology
(2003 edition). District general hospitals (DGHs) and
tertiary referral centres (TRCs) received similar num-
bers of questionnaires (344 vs. 296 respectively). Car-
diologists were asked to report their pericardiocentesis
experience within the preceding 2 years, focussing
particularly on indications for pericardiocentesis and
procedural preferences. We also asked respondents to
report any procedure-related complications and to
provide details of the aetiology of pericardial effusion
if available. Data were collated and analysed using
Access and Excel software (Windows XP Professional;
Microsoft Corporation, Seattle, WA).
Results
RespondentsA total of 274 (43%) completed questionnaires were
returned: 88% consultants, 9% specialist registrars
and 3% staff grades. Respondents were equally dis-
tributed between TRCs and DGHs (49% and 51%
respectively). A maximum of three questionnaires
SUMMARY
Background: Pericardial effusions frequently present challenging clinical dilem-
mas. Whether or not to drain an effusion, and if so by what method, are two
common decisions facing cardiologists. We performed a survey to evaluate pericar-
diocentesis practice in the United Kingdom (UK). Methods: A total of 640 ques-
tionnaires were sent to all cardiologists in the UK Directory of Cardiology in March
2003. Results: A total of 274 (43%) completed questionnaires were returned,
88% from consultants, equally distributed between tertiary referral centres and dis-
trict general hospitals. More than 1500 procedures were performed, largely using
a paraxiphoid approach (89%). Clinical tamponade was the commonest indication
for pericardiocentesis (83%). However, the majority of respondents (69%) consid-
ered echocardiographic features alone an indication for pericardiocentesis, even in
the absence of clinical tamponade. The commonest perceived indications for drain-
age were right ventricular diastolic collapse and right atrial collapse (69% and
33% of respondents respectively). For guidance, 82% use echocardiography, either
alone or with fluoroscopy or the electrocardiogram (ECG) injury trace. 11% employ
fluoroscopy alone or with the ECG injury trace. The remaining 11% stated that
they would use the ECG injury trace alone or use no guidance. Using the ECG
injury trace alone is said by the European Society of Cardiology (ESC) guidelines to
offer an inadequate safeguard. Reported complications included ventricular punc-
ture (n ¼ 12, 0.8%) and hepatic damage (n ¼ 4, 0.3%). Conclusion: Pericardio-
centesis practice varies substantially in the UK. Many cardiologists would perform
pericardiocentesis based on echocardiographic features alone. 11% of cardiologists
use guidance that is considered inadequate by the ESC guidelines.
What’s knownVery little is known about this topic. Although
there are ESC guidelines on the management of
pericardial disease, there are no published data on
pericardiocentesis practice in the UK.
What’s newThis article adds insight into the variability of
current pericardiocentesis practice in the UK, and
that available practice guidelines are not adhered
to.
1Department of Cardiology,
New Royal Infirmary of
Edinburgh, Edinburgh, UK2Department of Cardiology,
Stobhill Hospital, Glasgow, UK3Department of Cardiology,
Royal Infirmary, Glasgow, UK
Correspondence to:
Dr Sean Balmain,
Department of Cardiology, New
Royal Infirmary of Edinburgh,
51 Little France Crescent,
Edinburgh EH16 4SA, UK
Tel.: + 447811113015
Fax: + 448717142621
Email:
Disclosures
The authors have stated that
they have no interests that
might be perceived as posing a
conflict or bias.
doi: 10.1111/j.1742-1241.2007.01536.x
OR IG INAL PAPER
ª 2007 The AuthorsJournal compilation ª 2007 Blackwell Publishing Ltd Int J Clin Pract, October 2008, 62, 10, 1515–1519 1515

were returned from any single centre, reflecting the
large number of hospitals which responded.
Who performs pericardiocentesis?More than 1500 pericardiocentesis procedures were
performed over the 2-year audit period, 56% in
TRCs and 44% in DGHs. Procedures were more fre-
quently performed by a trainee under supervision in
TRCs than DGHs (47% vs. 33% respectively). Most
cardiologists (81%) do not believe that on-site car-
diothoracic surgical support is necessary. Of those
not requiring surgical support, 42% work in TRCs
and 58% in DGHs.
Indications for pericardiocentesisThe commonest reason for pericardiocentesis was
clinical tamponade (83% of procedures). 10% were
undertaken for diagnostic purposes. Only 7% were
performed based on echocardiographic appearances
alone. However, the majority of respondents (69%)
regarded echocardiographic features an indication for
pericardiocentesis, even in the absence of clinical
tamponade. Features considered an indication for
drainage were: right ventricular diastolic collapse
(69% of respondents); right atrial collapse (33%);
respiratory variation of transvalvular Doppler flow
(7%) and large effusion size (3%).
Procedural preferencesA paraxiphoid approach was most popular (89%),
with the remaining operators preferring an apical
approach. For guidance (Table 1), 78% routinely use
echocardiography alone or in conjunction with fluo-
roscopy, the electrocardiogram (ECG) injury trace or
both. 11% of respondents employ fluoroscopy alone
or in combination with the ECG injury trace. The
remaining 11% use the ECG injury trace alone, or
use no guidance. 10% routinely inject contrast into
the pericardial space.
ComplicationsThe most commonly reported complications were
ventricular puncture [n ¼ 12 (0.8%), nine right ven-
tricular, one left ventricular and two unspecified]
and hepatic damage (n ¼ 4, 0.3%). Right coronary
artery laceration was reported once, as was subphren-
ic haematoma and splenic vein perforation. One
peri-procedure death was reported, but related to
progressive cardiogenic shock rather than pericardio-
centesis. Few procedures resulted in failed drainage
(n ¼ 10, 0.7%).
Aetiology of pericardial effusionAetiology was ascertained in only 26% of cases.
Malignancy predominated (45%), followed by car-
diac surgery (21%), viral infection (13%), autoim-
mune disorders (7%), myocardial infarction (5%),
uraemia (5%) and tuberculous infection (3%).
Discussion
This is the first national survey of pericardiocentesis.
The European Society of Cardiology (ESC) has since
published guidelines on the diagnosis and manage-
ment of pericardial disease, including pericardiocen-
tesis (3).
Indications for pericardiocentesisClinical tamponade was the primary indication for
pericardiocentesis. This is a consistent finding
worldwide (4–6). The ESC guidelines state that
pericardiocentesis is mandatory in tamponade (class
I indication). The guidelines are less clear when
considering whether or not large effusions should
be drained. They initially state that pericardiocente-
sis is optional in large or recurrent effusions, or if
previous tests are inconclusive (class IIa indication),
or in small effusions (class IIb indication) (all level
of evidence B) (3). The guidelines subsequently
contradict this statement, recommending pericardio-
centesis for effusions > 20 mm in diameter by echo-
cardiography (class IIa indication). The latter
recommendation cites a report by Sagrista-Sauleda
et al. (7) of 28 patients with large idiopathic
chronic pericardial effusion. However, this subgroup
represented just 2.2% of patients with pericardial
disease (7). The same authors do not advocate peri-
cardial drainage in the initial management of
patients with large pericardial effusion without clini-
cal tamponade (2). The ESC guidelines do not dis-
tinguish between different indications for
pericardiocentesis in acute and chronic effusions
(3). Clarification of this issue (i.e. whether or not
to drain large effusions) would be welcome when
the ESC revises the guidelines.
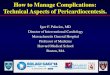
Table 1 Procedural preferences
Guidance method Respondents (%)
Echocardiography alone or in combination 214 (78)
Echocardiography alone 86 (31)
With fluoroscopy 85 (31)
With ECG injury trace 27 (10)
With fluoroscopy and ECG injury trace 16 (6)
Fluoroscopy alone or with ECG injury trace 30 (11)
Fluoroscopy alone 24 (9)
With ECG injury trace 6 (2)
ECG injury trace alone 5 (2)
No guidance 25 (9)
1516 Pericardiocentesis practice in the UK
ª 2007 The AuthorsJournal compilation ª 2007 Blackwell Publishing Ltd Int J Clin Pract, October 2008, 62, 10, 1515–1519

The perceived and actual indications for pericar-
diocentesis differed substantially. The majority of
respondents (69%) considered echocardiographic fea-
tures an indication for drainage, even in the absence
of clinical tamponade. However, few were actually
performed on the basis of echocardiography alone
(7%). The discrepancy likely reflects uncertainty
regarding the indications for drainage, and caution
in ‘real life’ clinical practice. Cardiologists may be
concerned by ‘echocardiographic’ tamponade, but
only commit to an invasive procedure when clinical
compromise dictates.
Although the ESC guidelines list echocardiographic
and clinical criteria for the diagnosis of ‘cardiac
tamponade’, whether or not echocardiographic
appearances alone merit intervention is not discussed
(3). Some have reported strong correlations between
chamber collapse, particularly of the right ventricle
and clinical tamponade (8–14). However, these stud-
ies involved only small numbers of patients, often
with established clinical tamponade (10–14), or
experimental animal models (8,9). Most large series
fail to distinguish between echocardiographic and
clinical tamponade, performing pericardiocentesis in
both (5,15,16). Consequently, the evolution of con-
servatively managed patients with echocardiographic
but not clinical tamponade is uncertain. Pericardio-
centesis is of doubtful benefit in such patients. The
only group to address this question is Merce et al.
(1,17) They found a poor correlation between clinical
tamponade and right-sided chamber collapse (17),
and that clinical outcomes related to underlying aeti-
ology rather than whether or not pericardiocentesis
was performed (1). Indeed, irrespective of chamber
collapse or effusion size, no conservatively managed
patients with nonmalignant effusion developed clini-
cal tamponade, few effusions persisted, and no new
diagnoses occurred during follow-up (1,17). Fewer of
our respondents believed that right atrial (33%)
compared with right ventricular (69%) collapse was
an indication for drainage.
Procedural preferencesA paraxiphoid approach was most popular, as in
many centres (6,15,16). Echocardiography alone, or
in combination with fluoroscopy, was used most fre-
quently to guide pericardiocentesis. 48% of respon-
dents use fluoroscopy and 20% the ECG injury trace
to guide pericardiocentesis. Historically, these meth-
ods were associated with a high complication rate
when used without echo guidance (18). However, in
our survey, the majority of respondents combine
fluoroscopy or the ECG injury trace with echocardi-
ography. Surprisingly, 22% do not use echocardiog-
raphy: 11% prefer fluoroscopy, 2% employ the ECG
injury trace alone, while 9% reported routinely using
no guidance. The ESC guidelines advocate a subxi-
phoid approach guided by either echocardiography
or fluoroscopy, as employed by the majority of
respondents (3). They explicitly state that the ECG
injury trace alone is not an adequate safeguard (3).
19% of respondents consider on-site surgical back up
a necessity.
ComplicationsThe low-reported complication rate is comparable
with large series, including a similar frequency of
ventricular puncture (0.8%) (5,15,16).
AetiologyRespondents reported a low diagnostic yield of peri-
cardiocentesis (< 30%), which is consistent with pre-
vious reports (4,19,20), as is the predominance of
neoplastic aetiology (5,6,15,20,21). The aetiological
spectrum in different series reflects geographical loca-
tion, underlying disease prevalence, hospital charac-
teristics, effusion size and the applied study protocol
(2). Consequently, some series have cited acute idio-
pathic pericarditis (4) and cardiac surgery (5,16) as
the commonest cause. The low-reported frequency of
tuberculous effusion contrasts with studies from
areas with a higher prevalence of tuberculosis infec-
tion (6,15). The relatively low incidence of uraemic
effusion likewise differs from some reports
(20,22,23), reflecting the lower prevalence of end-
stage renal disease and on-site haemodialysis facilities
in many DGHs.
Study limitationsThe modest response rate (43%) may misrepresent
pericardiocentesis practice throughout the UK. In
particular, inexperienced cardiologists or those with
serious complications may not respond. Anonymity
hopefully reduces such bias. The survey methodology
was limited in that we did not telephone or re-send
questionnaires to non-responders, which may have
improved the response rate. Information recalled
from memory is less robust than data from prospec-
tive studies or large registries. Self-reporting of com-
plications is particularly prone to bias.
Epidemiological data, such as effusion aetiology, is
subject to recall error, and not the focus of the study.
In this respect, the concordance of results with exist-
ing published series is surprising. The main interest
lies in the actual and perceived indications for drain-
age and procedural preferences. Given the relatively
small number of procedures per respondent, this
data may be accurate. We must acknowledge that
objectively reviewing patient records would improve
accuracy.
Pericardiocentesis practice in the UK 1517
ª 2007 The AuthorsJournal compilation ª 2007 Blackwell Publishing Ltd Int J Clin Pract, October 2008, 62, 10, 1515–1519

Reporting subjective clinical decisions through
objective data has limitations. Risks are balanced
against the degree of haemodynamic compromise,
aetiology and anatomical position of the effusion
and potential benefits. Finally, some information that
may have proved interesting was not collected. We
failed to ask where pericardiocentesis was performed,
or whether intrapericardial pressure was routinely
measured.
Conclusion
Pericardiocentesis practice varies considerably in the
UK. Although clinical tamponade is the commonest
indication for pericardiocentesis, 69% of clinicians
would drain an effusion based on echocardiographic
findings alone. The value of this approach is uncer-
tain. 11% of cardiologists use techniques which are
considered unsafe by the ESC. Pericardiocentesis
practice should adhere to the ESC guidelines. This
survey predates these guidelines and should be
repeated to determine whether clinical practice has
changed.
References
1 Merce J, Sagrista-Sauleda J, Permanyer-Miralda G, Soler-Soler J.
Should pericardial drainage be performed routinely in patients
who have a large pericardial effusion without tamponade? Am J
Med 1998; 105: 106–9.
2 Soler-Soler J, Sagrista-Sauleda J, Permanyer-Miralda G. Manage-
ment of pericardial effusion. Heart 2001; 86: 235–40.
3 Maisch B, Seferovic PM, Ristic AD et al. Guidelines on the diagno-
sis and management of pericardial diseases executive summary;
The Task force on the diagnosis and management of pericardial
diseases of the European society of cardiology. Eur Heart J 2004;
25: 587–610.
4 Sagrista-Sauleda J, Merce J, Permanyer-Miralda G, Soler-Soler J.
Clinical clues to the causes of large pericardial effusions. Am J Med
2000; 109: 95–101.
5 Tsang TS, Enriquez-Sarano M, Freeman WK et al. Consecutive
1127 therapeutic echocardiographically guided pericardiocenteses:
clinical profile, practice patterns, and outcomes spanning 21 years.
Mayo Clin Proc 2002; 77: 429–36.
6 Gibbs CR, Watson RD, Singh SP, Lip GY. Management of pericar-
dial effusion by drainage: a survey of 10 years’ experience in a city
centre general hospital serving a multiracial population. Postgrad
Med J 2000; 76: 809–13.
7 Sagrista-Sauleda J, Angel J, Permanyer-Miralda G, Soler-Soler J.
Long-term follow-up of idiopathic chronic pericardial effusion. N
Engl J Med 1999; 341: 2054–9.
8 Leimgruber PP, Klopfenstein HS, Wann LS, Brooks HL. The he-
modynamic derangement associated with right ventricular diastolic
collapse in cardiac tamponade: an experimental echocardiographic
study. Circulation 1983; 68: 612–20.
9 Klopfenstein HS, Schuchard GH, Wann LS et al. The relative
merits of pulsus paradoxus and right ventricular diastolic
collapse in the early detection of cardiac tamponade: an
experimental echocardiographic study. Circulation 1985; 71: 829–
33.
10 Kronzon I, Cohen ML, Winer HE. Diastolic atrial compression: a
sensitive echocardiographic sign of cardiac tamponade. J Am Coll
Cardiol 1983; 2: 770–5.
11 Engel PJ, Hon H, Fowler NO, Plummer S. Echocardiographic
study of right ventricular wall motion in cardiac tamponade. Am J
Cardiol 1982; 50: 1018–21.
12 Armstrong WF, Schilt BF, Helper DJ et al. Diastolic collapse of the
right ventricle with cardiac tamponade: an echocardiographic
study. Circulation 1982; 65: 1491–6.
13 Singh S, Wann LS, Schuchard GH et al. Right ventricular and right
atrial collapse in patients with cardiac tamponade–a combined
echocardiographic and hemodynamic study. Circulation 1984; 70:
966–71.
14 Singh S, Wann LS, Klopfenstein HS et al. Usefulness of right ven-
tricular diastolic collapse in diagnosing cardiac tamponade and
comparison to pulsus paradoxus. Am J Cardiol 1986; 57: 652–6.
15 Cho BC, Kang SM, Kim DH et al. Clinical and echocardiographic
characteristics of pericardial effusion in patients who underwent
echocardiographically guided pericardiocentesis: Yonsei Cardiovas-
cular Center experience, 1993–2003. Yonsei Med J 2004; 45: 462–8.
16 Lindenberger M, Kjellberg M, Karlsson E, Wranne B. Pericardio-
centesis guided by 2-D echocardiography: the method of choice
for treatment of pericardial effusion. J Intern Med 2003; 253: 411–
7.
17 Merce J, Sagrista-Sauleda J, Permanyer-Miralda G et al. Correla-
tion between clinical and Doppler echocardiographic findings in
patients with moderate and large pericardial effusion: implications
for the diagnosis of cardiac tamponade. Am Heart J 1999; 138:
759–64.
18 Wong B, Murphy J, Chang CJ et al. The risk of pericardiocentesis.
Am J Cardiol 1979; 44: 1110–4.
19 Permanyer-Miralda G, Sagrista-Sauleda J, Soler-Soler J. Primary
acute pericardial disease: a prospective series of 231 consecutive
patients. Am J Cardiol 1985; 56: 623–30.
20 Corey GR, Campbell PT, Van Trigt P et al. Etiology of large peri-
cardial effusions. Am J Med 1993; 95: 209–13.
21 Olsen PS, Sorensen C, Andersen HO. Surgical treatment of large
pericardial effusions. Etiology and long-term survival. Eur J Car-
diothorac Surg 1991; 5: 430–2.
22 Colombo A, Olson HG, Egan J, Gardin JM. Etiology and prognos-
tic implications of a large pericardial effusion in men. Clin Cardiol
1988; 11: 389–94.
23 Levine MJ, Lorell BH, Diver DJ, Come PC. Implications of echo-
cardiographically assisted diagnosis of pericardial tamponade in
contemporary medical patients: detection before hemodynamic
embarrassment. J Am Coll Cardiol 1991; 17: 59–65.
Paper received May 2007, accepted July 2007
Appendix 1: Survey questions
1. What grade are you?
2. Where do you work (district general hospital or
tertiary referral centre)?
3. How many pericardiocentesis procedures have you
performed in the past 2 years?
4. How many pericardiocentesis procedures have you
supervised in the past 2 years?
5. Do you feel that cardiothoracic surgical support is
necessary to perform pericardiocentesis?
6. Regarding the indication for pericardiocentesis,
how many procedures were performed for (a) diag-
nostic purposes, (b) echocardiographic appearances,
(c) clinical tamponade/haemodynamic compromise?
7. How many procedures yielded a diagnosis?
8. Of those procedures which yielded a diagnosis,
how many were due to: (a) trauma, (b) malignancy,
1518 Pericardiocentesis practice in the UK
ª 2007 The AuthorsJournal compilation ª 2007 Blackwell Publishing Ltd Int J Clin Pract, October 2008, 62, 10, 1515–1519

(c) renal disease, (d) viral infection, (e) tuberculosis,
(f) autoimmune disease, (g) postmyocardial infarc-
tion, (h) endocrine disease, (i) other aetiology (please
specify)?
9. Which of the following do you routinely use to
guide pericardiocentesis? (a) echocardiography, (b)
fluoroscopy, (c) injection of contrast into the peri-
cardium, (d) the ECG injury trace, (e) others (please
specify)
10. What size of pericardial effusion (in mm) would
you consider to be unsuitable for drainage?
11. In the absence of clinical tamponade, which of the
following echocardiographic features would you con-
sider to be an indication for pericardiocentesis? (a) right
atrial collapse, (b) right ventricular diastolic collapse,
(c) other echocardiographic feature (please specify)
12. Which anatomical approach do you favour for
pericardiocentesis? (a) subxiphoid, (b) apical, (c)
other approach (please specify)
13. Did you experience any complications of pericar-
diocentesis over the past 2 years? If so please provide
details.
Pericardiocentesis practice in the UK 1519
ª 2007 The AuthorsJournal compilation ª 2007 Blackwell Publishing Ltd Int J Clin Pract, October 2008, 62, 10, 1515–1519