Embed Size (px)
Citation preview

Oxford Inflammatory Bowel Disease MasterClass
Perianal Crohn’s Disease from a
Surgeon’s Perspective
Richard Guy MD FRCS Consultant Colorectal Surgeon
Oxford University Hospitals




Crohn’s Disease: perianal lesions
Type of Lesion No of patients (%)
Skin tag 75 (37)
Anal fissure 38 (19)
Anal fistula 52 (26)
Recto-vaginal fistula 6 (3)
Perianal abscess 32 (16)
Complex abscess 21 (10)
Anorectal stricture 19 (9)
Haemorrhoids 15 (7)
Anal ulcer 12 (6)
Keighley & Allen, Int J Colorect Dis. 1986
•202 consecutive patients •110 (54%) had some perianal involvement

Crohn’s Fistulae
Perianal 55%
Entero-enteric 24%
Recto-vaginal 9%
Other 12%
Schwartz DA Gastroenterology 2002
Cumulative risk for any fistula in CD: 33% after 10 years, 50% after 20 years

Prevalence of anal disease in intestinal Crohn’s
Isolated ileal disease 12%
Ileocolonic disease 15%
Colonic disease (rectal sparing) 41%
Colonic & rectal disease 92%
In 20-36% perianal disease precedes intestinal disease
Hellers et al. Gut 1980;21:525-527

Range of severity of perianal Crohn’s disease
Good prognosis Poor prognosis
Skin tags
Fissures
Fistulae
Strictures
Deep cavitating ulcers

Spectrum of Crohn’s Anal Fistulae

Crohn’s ileoanal pouch

Surgical treatment of Crohn’s fistulae
First aid incision & drainage of sepsis
Bridging treatment convert acute ‘uncontrolled’ situation into potentially ‘curative’ one
seton & immunomodulator
Quality of life based treatment attempt to heal fistula if symptomatic & realistic
consider other options
Proctectomy & permanent stoma

Perianal Sepsis & Fistulae: First Aid Surgery
•adequate drainage •skin-sparing where possible •liberal use of catheters & setons

Bridging treatment
often involves loose seton(s)
short course antibiotics metronidazole
ciprofloxacin
allows patient to be established on immunomodulator
assessment of fistula anatomy

Crohn’s Fistulae: Assessment & Imaging
EUA
90% accuracy
Ultrasound
56-100% accuracy
MRI
76-100% accuracy
Haggett 1995, Orsoni 1999, Sloots 2001, Schwartz 2002
rectal

Fistula “Rules”
Too often broken in Crohn’s!

Simple vs Complex
Bell SJ et al. Aliment Pharmacol Ther 2003;17:1145-51
•Simple •Superficial •intersphincteric
•Complex •Trans-sphincteric •Trans-levator •Supralevator •Extra-sphincteric

Crohn’s fistulae: procedure choice
Fistula size
Length
Anatomical location
Complexity
Disease activity
Concomitant intestinal disease
Undrained sepsis
Bayer & Gordon; DCR 1994

Fistulotomy for low fistulae
60-80% healing
20-40% slow wound healing
10%-20% risk of recurrence
small risk of incontinence
better results if no proctitis
Levien et al. 1989, Williams et al. 1991, Scott & Northover 1996

Find & treat active luminal disease!

Glues & Plugs
Generally disappointing
Not adequately evaluated
Systematic review of plugs in Crohn’s 42 pts only
55% closure
O’Riordan DCR 2012

Insufficient data
Proctitis must be treated
Overall “success” 64%
Incontinence 9.4%
Combination therapy may improve outcome
Endorectal Advancement Flaps
Soltani & Kaiser DCR 2010

Endorectal Advancement Flaps
Soltani & Kaiser DCR 2010

Complex Crohn’s

Complex fistulae: treatment options
Do nothing: long-term setons
Remove setons only
Remove setons and attempt to heal medically
Attempt to heal surgically
Combination medical and surgical treatment
varying patient expectations
varying end-points in studies
uncertain natural history

Crohn’s Fistulae: long-term loose seton
Williams et al. 1991
11 of 23 “good” result
seton usually removed
6 minor incontinence
5 proctectomy
Scott & Northover 1996
23 of 27 “good” result
18 left in situ
3 proctectomy, 1 chronic sepsis/pain

Teamwork!

Colorectal Dis 2011;14:331-335

Medical therapy in combination with surgery
Consensus
Antibiotics
metronidazole &/or ciprofloxacin
short-term use only
lack of clinical trials
Azathioprine/mercaptopurine
appear to be effective in closure & maintenance
lack of clinical trials
In combination with surgical therapy
Van Assche et al. (ECCO); J Crohn’s Colitis 2010;4:63-101

0
10
20
30
40
50
60
% of patients
with complete
closure of
fistulae
placebo
5mg/kg
10mg/kg
infliximab
*
* *
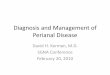
Infliximab-induced closure of fistulae
Present et al. N Eng J Med 1999;340:1399-1405

ACCENT II
•At 14 weeks •69% response
•RCT 5mg/kg IFX every 8 weeks vs placebo •At 54 weeks
•36% closure IFX vs 19% placebo
•14.9% new abscess formation
Sands et al. N Engl J Med 2004;350:1398-1405, Sands et al. Clin Gastroenterol Hepatol 2004;2:912-920


Biologicals:Monitoring Therapeutic Response
Problem of “end-points”
Clinical assessment (decreased drainage)
MRI
Perianal Crohn’s Disease Activity Index (PCDAI)
Irvine et al. J Clin Gastro 1995, Present et al. N Engl J Med 1999

Irvine EJ. J Clin Gastroenterol 1995;20:27-32
PCDAI

There are known, knowns. There are known unknowns. There are unknown unknowns

Immunomodulation & Surgery
Immunomodulation may not be enough
Combined approach generally more effective
Some controversy & confusion
No consensus on ideal combination
Definitive surgery possible
Worries about second malignancies
Topstad 2003, Van der Hagen 2005, Van der Hagen 2006, Hyder 2006, Gaertner 2007, Tozer 2012


Luminal Disease
Perianal Disease
Perianal Crohn’s: relapse post-Infliximab
Domenech et al. Aliment Pharmacol Ther 2005

Combined seton, infliximab and
maintenance immunosuppression
Topstad et al. Dis Colon Rectum 2003;46:577-583
•Setons removed after second infusion •67% complete healing at follow-up (mean 9 mths)

Multistep Strategy: IFX induction & surgery
Van der Hagen DCR 2005

Combination Therapy: Oxford
Hyder et al. DCR 2006

MDT discussion!

Combination Therapy: IFX vs IFX/Surgery
32 patients
IFX vs IFX + EUA/seton
IFX IFX+Surg P
Initial response (%) 82.6 100 0.014
Recurrence rate (%) 79 44 0.001
Time to recurrence (m) 3.62 13.5 0.0001
Regueiro & Mardini; Inflamm Bowel Dis 2003

Combination Therapy: Minnnesota 1991-2005
•Overall healing rates similar •For IFX + Surgery patients
•shorter healing time (12.1 vs 6.5 mths) •better healing of TS fistulae
Gaertner et al. DCR 2007

Combination Therapy: Cleveland Clinic 1999-2009
El-Gazzazz et al; Colorectal Dis 2012

Combination therapy: Leeds, UK
•52 patients, median follow-up 66 mths •73% EUA +/- seton •22 (42.3%) complete response
•13 (59%) no recurrence at 40 mths
Duff et al. Colorectal Dis 2012

Rectovaginal Fistula
Affects up to 10% of women with CD
Reported healing rates 40-60%
ACCENT II trial
72.2% healing at 14 weeks
44.4% healing at 54 weeks
Higher healing rates with combination therapy?
Hull & Fazio 1997, Morrison et al. 1989, O’Leary et al. 1998, Pennincx et al. 2001, Sands et al. 2004

Rectovaginal Fistula:Cleveland Clinic 1997-2007
El-Gazzazz et al. J Gastrointest Surg 2010

Rectovaginal Fistula: Cleveland Clinic 1997-2007
El-Gazzazz et al. J Gastrointest Surg 2010

What if bridging treatment is going badly?
Check that sepsis adequately drained
Consider defunctioning stoma
Consider proctectomy


Defunctioning ileostomy for perianal Crohn’s
• 18 patients defunctioned for severe perianal Crohn’s
• 15 acute remission
• 2 reversed with satisfactory function
Edwards et al. Br J Surg 2000
We’re still not really sure who to defunction!

Predictors of permanent diversion
•356 consecutive CD patients •86 (24%) perianal CD •20 RVF •344 operations •53 (62%) pts diverted •42 (49%) permanent stoma
Galandiuk et al. Ann Surg 2005

Operate when conditions as favourable as possible preliminary ileostomy
nutrition
setons/anti-TNF
Primary myocutaneous flap
Proctectomy


VRAM flap

Perineal Wound Failure

Perineal Wound Failure
Early failure
VAC dressing
Late failure
re-investigate for active small bowel Crohn’s
re-do flaps
hyperbaric oxygen

13 papers for CD, 9 for perianal disease
Improvements for 31/40 (78%) patients
Promising for chronic sinus/unhealed perineum in combination with flap surgery (Oxford)
Hyperbaric Oxygen

Complex Fistulating Crohn’s: Conclusions
Surgery must achieve adequate drainage
Surgery & biologics combination improves fistula healing
Diversion can assist disease stabilisation
Proctectomy is not usually a happy day out!

Benefits of Team Working