Embed Size (px)
Citation preview

Peri-operative Evaluation of
the Cirrhotic Patient
Dr César YAGHIHépato-Gastroentérologue
Hôtel-Dieu de FranceUniversité Saint [email protected]

Introduction
Greater risk for surgical and anesthesia related complications
Risk depends
• Type of liver disease and its severity
• The surgical procedure
• The type of anesthesia.

ESTIMATING SURGICAL RISK
LIVER DISEASE TYPE OF SURGERY MORTALITY PROGNOSTIC FACTORS
Nonlaparoscopic biliary surgery 20% Ascites, prothrombin time, alb
Peptic ulcer surgery 54% Prothrombin time,systolic blo
pressure, hemoglobin
Umbilical herniorrhaphy 13% Urgent surgery
Colectomy 24% Hepatic encephalopathy,
ascites,albumin, hemoglobin
Emergency abdominal surgery 57%
Abdominal surgery for trauma 47% Child Pugh class, urgent surg
Laparoscopic cholecystectomy 0.9%1, 6%
Emergency cardiac surgery 80% Child Pugh class
Elective cardiac surgery 3%–46% Child Pugh score
Knee replacement 0%
Transurethral resection of the prostate 6.7%
Chronic hepatitis Various types 0%
Hepatitis C Laparoscopic cholecystectomy 0%
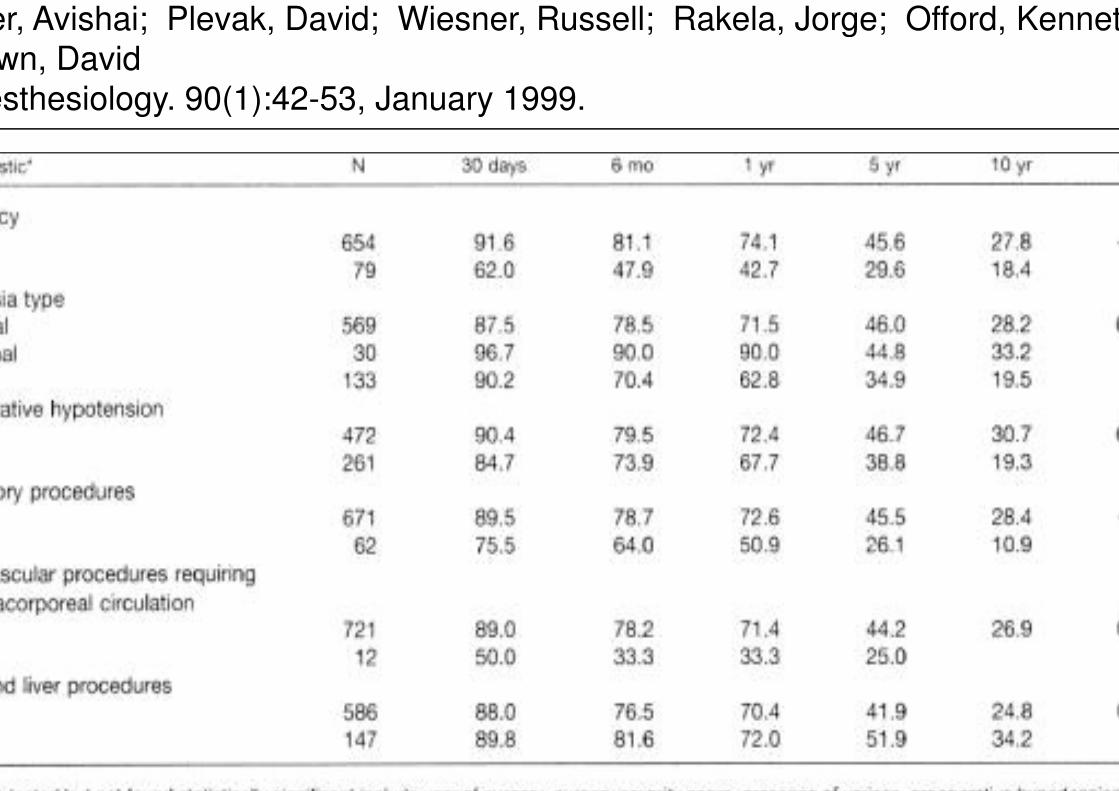
ser, Avishai; Plevak, David; Wiesner, Russell; Rakela, Jorge; Offord, Kenneth
Brown, David
Anesthesiology. 90(1):42-53, January 1999.

r, Avishai; Plevak, David; Wiesner, Russell; Rakela, Jorge; Offord, Kenneth;
Brown, David
Anesthesiology. 90(1):42-53, January 1999.
By multivariate analys
the risk factors were:
1. Male gender
2. Child-Pugh score
3. Presence of ascite
4. Cryptogenic cirrho
5. Creatinine
6. preoperative infect
7. ASA physical statu
score
8. Surgery on the
respiratory system
risk factors
59 patients had 0
173 had 1 214 had 2

Assessing Liver Function
Equation du score MELD
MELD score = (9.6 loge[creatinin mg/dL]) + (3.8 loge[bilirubin mg/dL]) + (11.2
e[INR]) + 6.4
MELD < 10 - Low risk
MELD = 10 -15 - Intermediate risk

Operative Mortality in Cirrhotics in relation to Child
Score and Type of surgery
Author Surgery Year Child A Child B Child
Garrison Abdominal 1984 10% 31% 76%
Mansour Abdominal elective 1997 10% 30% 82%
Mansour Abdominal emergency 1997 22% 38% 100%
Bizouarn Cardiac 1999 11% 18% 67%
Gervaz Cancer du colon 2003 6% 13% 28%
Hayashida Cardiac 2004 6% 67% 100%
Benmalek Abdominal 2004 5% 10% > 50%
Pre-operative MELD score for predicting
post-operative risk
MELD > 8 identifies risks of morbidity and mortality post
cholecystectomy
800 cirrhotic patients evaluating causes de morbidity and
mortality following major abdominal, orthopedic, or cardiac
surgery
– MELD correlated with short and long term mortality
– Each increase in the score of 1 unit (above 8) was
associated with an increase in mortality of 14% at 30 and
90 days

http://www.uptodate.com/contents/calculator-mortality-risk-in-post-operat



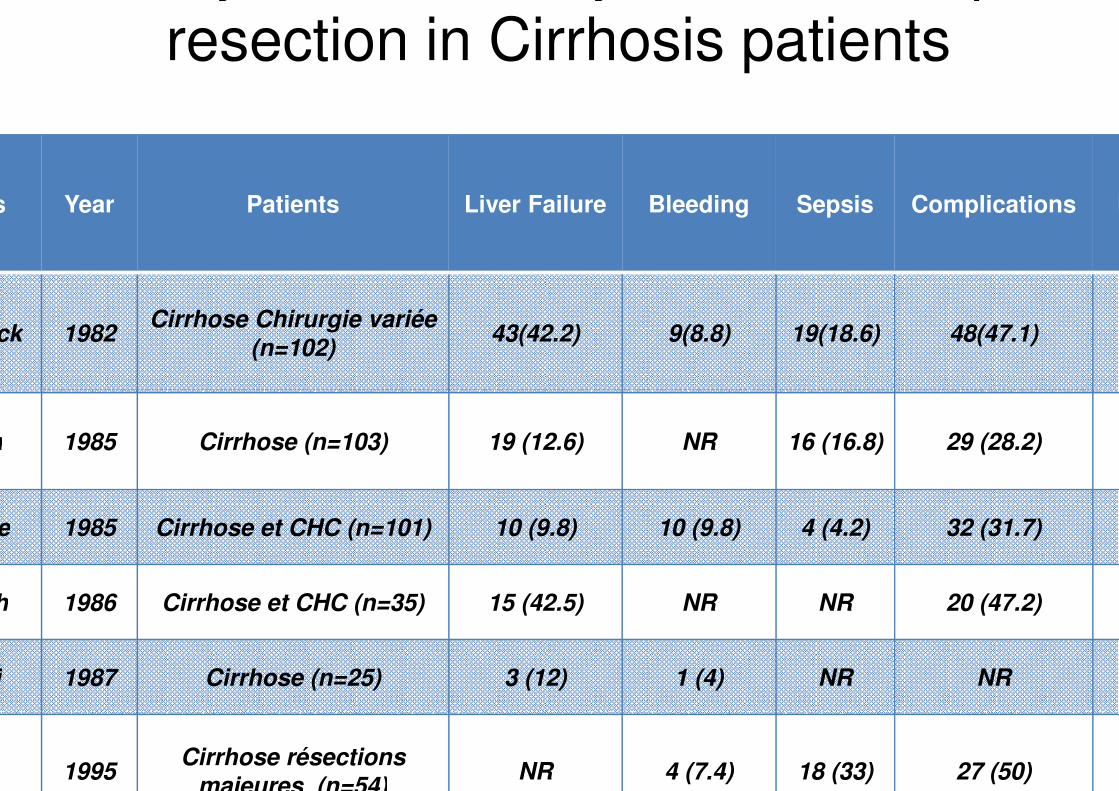
Mortality and Morbidity related to hepatic
resection in Cirrhosis patients
Authors Year Patients Liver Failure Bleeding Sepsis Complications M
Doberneck 1982Cirrhose Chirurgie variée
(n=102)43(42.2) 9(8.8) 19(18.6) 48(47.1)
Yanaga 1985 Cirrhose (n=103) 19 (12.6) NR 16 (16.8) 29 (28.2)
Nagasue 1985 Cirrhose et CHC (n=101) 10 (9.8) 10 (9.8) 4 (4.2) 32 (31.7)
Bismuth 1986 Cirrhose et CHC (n=35) 15 (42.5) NR NR 20 (47.2)
Gozetti 1987 Cirrhose (n=25) 3 (12) 1 (4) NR NR
1995Cirrhose résections
majeures (n=54)NR 4 (7.4) 18 (33) 27 (50)


Estimation des volumes hépatiques
dans la stratégie des hépatectomies
Relationship Between CT Volumetry and Functional Liver Volume Using
Technetium-99m Galactosyl Serum Albumin Scintigraphy
(A) CT scan and (B) 99mTc-GSA scintigraphy

Hepatic volume measured by CT-vol and 99mTc-GSA scintigraphy was significantly
Estimation des volumes hépatiques
dans la stratégie des hépatectomies

Residual Hepatic Volume
An acceptable residual volume in healthy individuals
is around 20% of the initial hepatic voloume, which
should be equivalent to 2 segments at least.
In patients with underlying liver disease:
– The minimal functional liver volume is estimated to
30 - 60% in chronic hepatitis, fatty liver or post-
chemotherapy.
– The residual volume should be 40 - 70% in patients
with cirrhosis

Pre-operative Portal Embolisation
The aim of Pre-operative Portal Embolisation is to
increase the residual hepatic volume and decrease
the incidence of post-operative liver failure.
2-8 weeks after PE, controloateral segment
hypertrophy reported increment of 20-46%
Hemi-hepatectomy was possible in 70-100% of
patients
3 and 5 years-survival respectively 61.2% and 43.7%

Contraindication for PVE
Tumors invading the portal vein
Portal hypertension (blocked to free hepatic vein pressure gradient
over12mm HG)
Coagulation disorders (PT<60%, plateled count <50G/l)
Even if a previous TACE may improve results of PVE , a minimum of
weeks delay between TACE and PVE is recommended.
In patients with cirrhosis,
• The decision is based on liver volumes with or without estimation o
the overall liver function by indocyanin green retention rate at 15
minutes (ICCG 15).
• A residual liver volume of 40% is recommended when the ICCG 15
between 10% and 20%. When the ICCG 15 is above 20%, a volum
of 50% is recommended

Assessing Liver Function
Indocyanine green clearance
– [ICG] plasma > 15% , 15 minutes after injection of 0.5 mg/kg ICG is considered abnormal
– Limited Correlation with Child Pugh score

Morbidité associée avec:
TP diminué
Une incidence de gestes
chirurgicaux concomitants
Une durée d’ischémie plus
prolongée
Durée opératoire prolongée
Saignement opératoire important
Besoins en transfusion
En analyse multivariée:
TP OR= 0.94
Duree operatoire OR=1.29
Optimizing Medical Therapy
Correction Prothrombin time
• Correction with vitamin K and fresh frozen plasma to achieve a
prothrombin time within three seconds of normal prior to surgery.
• Recombinant factor VIIA, (high cost, transient effect, associated
risk of thromboembolism).
Platelets: 50-100K (100K for cardiovascular and neurosurgery) A
prolonged bleeding time can be treated with diamino-8-D-arginine
vasopressin (DDAVP)
Optimal surgical technique / low central venous pressure may reduc
blood loss
Ascites: to reduce the chance of wound dehiscence and abdominal
wall herniation.
• Electrolyte abnormalities, (hypokalemia, metabolic
alkalosis) to decrease cardiac arrhythmias and hepatic
encephalopathy.
• Renal function
• Gastroesophageal varices : appropriate prophylactic
treatment.
• Malnutrition : Perioperative nutritional support : reduce
postoperative complications and short-term mortality
• calories equal to 1.2 times the estimated resting energ
expenditure and a 1 g/kg per day of protein.
Optimizing Medical Therapy
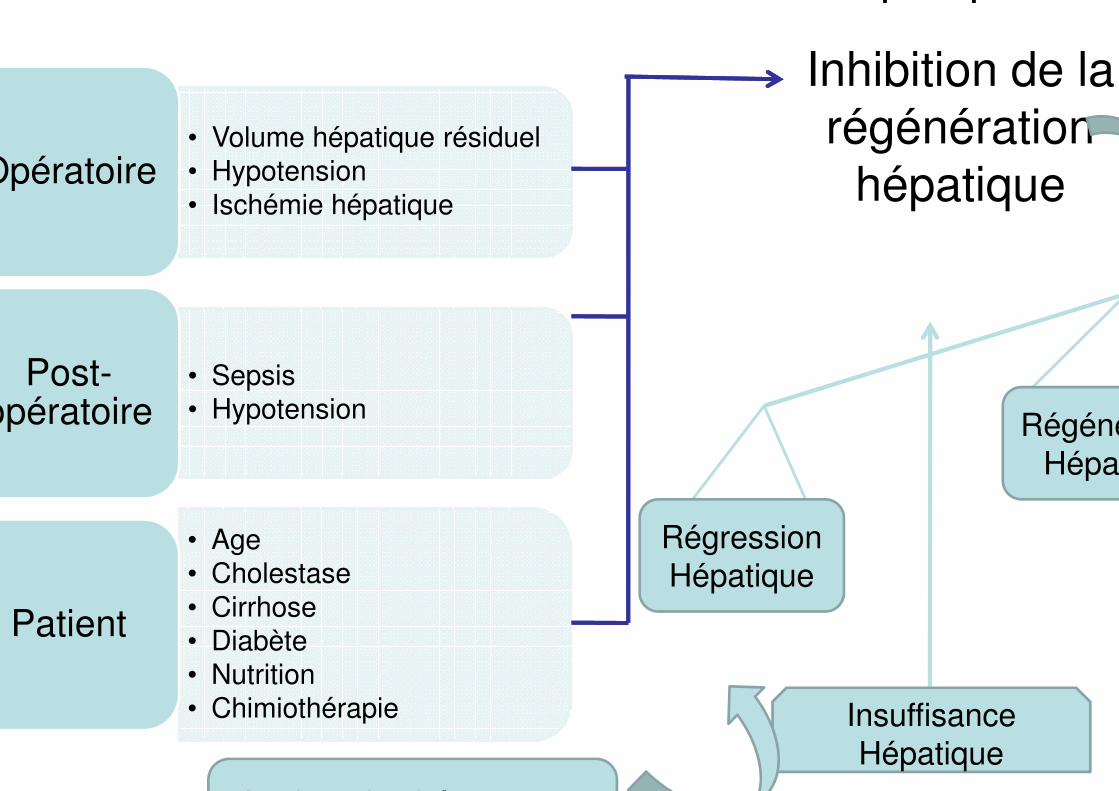
dans la survenue d’une insuffisance hépatique
• Volume hépatique résiduel
• Hypotension
• Ischémie hépatiqueOpératoire
• Sepsis
• HypotensionPost-
opératoire
• Age
• Cholestase
• Cirrhose
• Diabète
• Nutrition
• Chimiothérapie
Patient
Régression
Hépatique
Régéné
Hépat
Insuffisance
Hépatique
Inhibition de la
régénération
hépatique
Atteinte des hépatocytes

Influence des infections sur la régénération
hépatique après hépatectomie
Sepsis
Hypotension Ischémie
Anomalies des Ć de Kupfer
Diminution de la clairance des
bactériesportales
Risque de défaillance
multi-viscérale
Augmentation TNF-α
Apoptose
Regulation TGF-β
Atteintehépatocytaire
directe
Inhibition de la prolifération
hépatocytaire
Atteinte Hépatiquet altération de l
régénération

Conclusion
• Medical therapy should be optimized in all patients
• Operative mortality can be estimated based upon the Child
classification and the MELD score and taking into
consideration other factors such as the patient's age, ASA
score, and additional comorbidities.
• Elective or semi-urgent surgery not be performed in patients
with acute or fulminant hepatitis, alcoholic hepatitis, severe
chronic hepatitis, Child class C or MELD >15 cirrhosis, severe
coagulopathy, or severe extrahepatic manifestations of liver
disease (such as hypoxia, cardiomyopathy, or acute renal
failure)

























![Peri-operative Management of Impacted Third Molars [Autosaved]](https://img.pdfslide.us/doc/110x75/55cf8de3550346703b8c57cd/peri-operative-management-of-impacted-third-molars-autosaved.jpg)


