Embed Size (px)
Citation preview

Peri-infarct Zone Pacing to Prevent Peri-infarct Zone Pacing to Prevent Adverse Left Ventricular Remodeling in Adverse Left Ventricular Remodeling in
Patients with Large Myocardial InfarctionPatients with Large Myocardial Infarction
Gregg W. Stone, MDGregg W. Stone, MDEugene S. Chung, Branislav Stancak, Eugene S. Chung, Branislav Stancak,
Jesper H. Svendsen, Trent M. Fischer, Fred Kueffer, Jesper H. Svendsen, Trent M. Fischer, Fred Kueffer, Thomas Ryan, Jeroen Bax, and Angel Leon, Thomas Ryan, Jeroen Bax, and Angel Leon, for the Post-Myocardial Infarction Remodeling for the Post-Myocardial Infarction Remodeling
Prevention Therapy (PRomPT) Trial Investigators Prevention Therapy (PRomPT) Trial Investigators
Results from the PRomPT TrialResults from the PRomPT Trial

Presenter DisclosuresPresenter Disclosures
• None

PRomPT: PRomPT: BackgroundBackground
• Patients with large MI have high rates of death and Patients with large MI have high rates of death and hospitalization for heart failure (HF), which markedly hospitalization for heart failure (HF), which markedly affects quality of life (QoL) and increases healthcare affects quality of life (QoL) and increases healthcare costscosts
• Delayed contractile activation in the infarct and peri-Delayed contractile activation in the infarct and peri-infarct regions may increase local wall stress and infarct regions may increase local wall stress and workload, resulting in infarct expansion, wall thinning workload, resulting in infarct expansion, wall thinning and LV remodelingand LV remodeling
• LV pacing in the peri-infarct zone reduces local stroke LV pacing in the peri-infarct zone reduces local stroke work, and may attenuate post-MI increase in LV end-work, and may attenuate post-MI increase in LV end-diastolic volume (LVEDV), preventing ventricular diastolic volume (LVEDV), preventing ventricular remodeling and improving prognosisremodeling and improving prognosis

PRomPT: PRomPT: DesignDesignUp to 250 patients with large first MI (CPK >3000 U/L) and Up to 250 patients with large first MI (CPK >3000 U/L) and
QRS duration <120 msec within 10 days of QRS duration <120 msec within 10 days of symptom onset symptom onset
*Protecta XT or Consulta, with LV leads implanted *Protecta XT or Consulta, with LV leads implanted in the peri-infarct zone with 2D echo guidance in the peri-infarct zone with 2D echo guidance
CRT-D*CRT-D*LV and RV pacingLV and RV pacing
CRT-D*CRT-D*LV pacing onlyLV pacing only
ControlControlNo implantNo implant
Randomized 1:1:1Randomized 1:1:1
BlindedBlinded
Follow-up visits and evaluationsFollow-up visits and evaluations
2D echo, NYHA, MLWHF, EQ-5D, 6MWT at 1, 3, 6, 12, and 18 months2D echo, NYHA, MLWHF, EQ-5D, 6MWT at 1, 3, 6, 12, and 18 months
Baseline 2D echo, NYHA, MLWHF, EQ-5DBaseline 2D echo, NYHA, MLWHF, EQ-5D

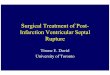
Target (green) and acceptable (yellow) lead implantation sites Target (green) and acceptable (yellow) lead implantation sites
Anterior infarctsAnterior infarcts Inferior and lateral infarctsInferior and lateral infarcts
A lateral (circumflex) infarct generally comprises segments 5, 6, 11, 12, and 16,
while an inferior (right coronary artery) infarct typically comprises segments 3, 4, 9, 10, and 15. A LV lead in this location will be
in the peri-infarct zone of either infarct.
Anterior (i.e. left anterior descending) infarcts generally comprise segments 1, 2, 7, 8, 13, 14, and 17. The target location in green is in the lateral peri-infarct region, segment 12, with other acceptable regions adjacent (yellow).

PRomPT: PRomPT: Primary endpointPrimary endpoint
• Change in LVEDV in the echocardiographic apical Change in LVEDV in the echocardiographic apical 4-chamber view from baseline to 18 months 4-chamber view from baseline to 18 months between the between the pooledpooled pacing therapy groups and pacing therapy groups and the control group (ΔLVEDV)the control group (ΔLVEDV)
• Primary analysis is performed in the Primary analysis is performed in the as-treated as-treated cohortcohort, including all randomized subjects, but , including all randomized subjects, but requiring successful CRT-D implantation in the requiring successful CRT-D implantation in the device armsdevice arms
• Analyzed by analysis of covariance (ANCOVA) Analyzed by analysis of covariance (ANCOVA) with baseline LVEDV as a covariatewith baseline LVEDV as a covariate

PRomPT: PRomPT: Power analysis / sample sizePower analysis / sample size
• AssumptionsAssumptions
Baseline mean LVEDV 130 mL in each groupBaseline mean LVEDV 130 mL in each group
15% greater increase in mean LVEDV from baseline to 15% greater increase in mean LVEDV from baseline to 18 months in control patients compared to the pooled 18 months in control patients compared to the pooled pacing therapy group (e.g. 19.5 mL vs. 0 mL)pacing therapy group (e.g. 19.5 mL vs. 0 mL)
Standard deviation of ΔLVEDV from baseline to follow-Standard deviation of ΔLVEDV from baseline to follow-up of 35 mL in the randomized groupsup of 35 mL in the randomized groups
• → → 156 evaluable echocardiograms would provide 156 evaluable echocardiograms would provide ~90% power at a 2-sided alpha of 0.05 to ~90% power at a 2-sided alpha of 0.05 to demonstrate superiority of peri-infarct pacingdemonstrate superiority of peri-infarct pacing

PRomPT: PRomPT: Organization / quality controlOrganization / quality control• Principal Investigator: Principal Investigator: Gregg W. Stone, Columbia UniversityGregg W. Stone, Columbia University
• Co-principal Investigator: Co-principal Investigator: Angel Leon, Emory UniversityAngel Leon, Emory University
• Steering Committee: Steering Committee: Eugene S. Chung, Inder S. Anand, Eugene S. Chung, Inder S. Anand, Jeroen J. Bax, Michael R. Gold, Robert Gorman, MD, Jeroen J. Bax, Michael R. Gold, Robert Gorman, MD, Heinz Theres, James Udelson, Mark Pfeffer Heinz Theres, James Udelson, Mark Pfeffer
• Clinical Events Adjudication Committee: Clinical Events Adjudication Committee: John Herre (Chair), John Herre (Chair), Michael Dickinson, Ayesha Hasan, Mark KremersMichael Dickinson, Ayesha Hasan, Mark Kremers
• Echocardiography Core Laboratory: Echocardiography Core Laboratory: Thomas Ryan, Ohio State Thomas Ryan, Ohio State UniversityUniversity
• Implant Lead Adjudication Committee: Implant Lead Adjudication Committee: Jose Dizon, Jagmeet Jose Dizon, Jagmeet Singh, Oussama WazniSingh, Oussama Wazni
• Data Safety and Monitoring Board: Data Safety and Monitoring Board: Dwight W. Reynolds (Chair), Dwight W. Reynolds (Chair), Juan Aranda, Tim ChurchJuan Aranda, Tim Church
• Trial and Site Management, Data Monitoring, Management and Trial and Site Management, Data Monitoring, Management and Analysis and Sponsor: Analysis and Sponsor: Medtronic, plcMedtronic, plc

PRomPT: PRomPT: EnrollmentEnrollment
• Given difficult recruitment and the goal of the present Given difficult recruitment and the goal of the present trial to inform a pivotal trial design, it was determined trial to inform a pivotal trial design, it was determined during enrollment, while the study leadership was still during enrollment, while the study leadership was still blinded, to accept 80% power and an alpha of blinded, to accept 80% power and an alpha of 0.10, requiring 96 evaluable echocardiograms 0.10, requiring 96 evaluable echocardiograms
• Assuming 20% of subjects would not have data Assuming 20% of subjects would not have data available at the 18-month visit due to early study exit, available at the 18-month visit due to early study exit, death, or non-evaluable echocardiograms, a sample death, or non-evaluable echocardiograms, a sample size of size of 120 as-treated patients 120 as-treated patients was required (40 per was required (40 per group)group)
9

10
Between December 2010 and October 2013, Between December 2010 and October 2013, 126 patients were randomized at 27 sites in 126 patients were randomized at 27 sites in Europe, the Middle East, and the United States Europe, the Middle East, and the United States
PRomPT: PRomPT: EnrollmentEnrollment
LV and RV pacingLV and RV pacing(n=41)(n=41)
LV pacing onlyLV pacing only(n=40)(n=40)
No implantNo implant(n=45)(n=45)
Randomized 1:1:1Randomized 1:1:1
18-month FU (n=38)18-month FU (n=38)As-treated (n=37)As-treated (n=37)
ITT (n=41)ITT (n=41)
18-month FU (n=36)18-month FU (n=36)As-treated (n=38)As-treated (n=38)
ITT (n=40)ITT (n=40)
18-month FU (n=36)18-month FU (n=36)As-treated (n=45)As-treated (n=45)
ITT (n=45)ITT (n=45)
Successful implant (n=37)Successful implant (n=37) Successful implant (n=38)Successful implant (n=38)
1 withdrew1 withdrew1 withdrawn1 withdrawn
1 withdrew1 withdrew1 withdrawn1 withdrawn 5 withdrew5 withdrew
3 lost to FU3 lost to FU1 missed 1 missed
18-mo FU18-mo FU1 withdrew1 withdrew 2 lost to FU2 lost to FU

PRomPT: PRomPT: Top 5 Enrolling SitesTop 5 Enrolling Sites1.1. East-Slovak Institute of Cardiovascular Diseases, Kosice, Slovakia (20): East-Slovak Institute of Cardiovascular Diseases, Kosice, Slovakia (20): B. B.
Stancak, J. Ignac, M. Jankajova, E. KomanovaStancak, J. Ignac, M. Jankajova, E. Komanova
2.2. The Lindner Research Center, Cincinnati, OH, USA (17): The Lindner Research Center, Cincinnati, OH, USA (17): E. E. Chung, T. Waller, S. Menon, M. Gupta, K. Bailey, E. Chung, T. Waller, S. Menon, M. Gupta, K. Bailey, E. Schloss, D. Kereiakes, D. WahlSchloss, D. Kereiakes, D. Wahl
3.3. Rigshospitalet, Copenhagen, Denmark (11): Rigshospitalet, Copenhagen, Denmark (11): J. Svendsen, J. Bro-JeppesenJ. Svendsen, J. Bro-Jeppesen
4.4. Emory University Hospital Midtown, Atlanta, GA, USA (9): Emory University Hospital Midtown, Atlanta, GA, USA (9): A. Leon, M. El-Chami, M. Lloyd, M. Hoskins, J. Langberg, A. Leon, M. El-Chami, M. Lloyd, M. Hoskins, J. Langberg, D. DeLurgio D. DeLurgio
5.5. University of Pennsylvania, Philadelphia, PA, USA (7): University of Pennsylvania, Philadelphia, PA, USA (7): W. W. Matthai, W. Groh, R. Li, J. Stern, J. Bullinga, G. Chang, C. Matthai, W. Groh, R. Li, J. Stern, J. Bullinga, G. Chang, C. Frankil, C. Gasperetti, C. Leng, A. Moak Frankil, C. Gasperetti, C. Leng, A. Moak

PRomPT: PRomPT: Baseline featuresBaseline features
Pooled pacing
(n=75)Control (n=45)
Age (yrs)* 59 ± 11 54 ± 11Gender (male) 73.3% 73.3%Body mass index (kg/m2) 29 ± 6 29 ± 4Hypertension 56.0% 55.6%Hyperlipidemia 40.0% 46.7%Diabetes mellitus 20.0% 22.2%Current smoking 45.3% 42.2%MI location Anterior 76.0% 77.8% Non-anterior 24.0% 22.2%PCI performed 96.0% 97.8% Symptom onset to PCI (hrs) 7.6 ± 8.2 9.0 ± 12.7Peak CPK (U/L) 4513 ± 1316 5248 ± 2832
*P=0.02; otherwise there were no significant differences between groups*P=0.02; otherwise there were no significant differences between groups

PRomPT: PRomPT: Implant performanceImplant performance
Pooled pacing groups*Pooled pacing groups*
•Devices were successfully implanted in 75/76 attempts Devices were successfully implanted in 75/76 attempts (98.7%) at 7.0 ± 2.3 days after MI(98.7%) at 7.0 ± 2.3 days after MI
•The LV lead was successfully placed within the The LV lead was successfully placed within the echocardiographic peri-infarct zone in 95.5% of echocardiographic peri-infarct zone in 95.5% of patients, and in the pre-specified target zone in 62.7% patients, and in the pre-specified target zone in 62.7% of patientsof patients
•The median (25%, 75%) percent LV pacing during The median (25%, 75%) percent LV pacing during follow-up was 98.9% (97.9%, 99.0%) follow-up was 98.9% (97.9%, 99.0%)
13*There were no significant differences between single and dual lead groups*There were no significant differences between single and dual lead groups

PRomPT: PRomPT: Primary endpoint - Primary endpoint - ΔΔLVEDV LVEDV Paired echocardiographic results between the baseline Paired echocardiographic results between the baseline
and 18-month follow-up visitsand 18-month follow-up visits
LVEDV (mL)
n Baseline 18-monthAdj mean change
(95% CI)
Difference(95%CI)
P
Control 34118.6
± 29.4
133.9 ± 38.9
15.8 (5.5, 26.2)
0.6(-12.3, 13.5)
0.92
Pooled pacing
64106.1 ±
27.6
122.8 ± 40.4
16.4 (8.9, 23.9)

PRomPT: PRomPT: Primary Endpoint – Primary Endpoint – ΔΔLVEDV LVEDV Paired echocardiographic results between the baseline Paired echocardiographic results between the baseline
and 18-month follow-up visitsand 18-month follow-up visits100
Mea
n ∆
LV
ED
V (
mL
)
0
Control
N with data:
75
50
25
0
-25
-50
1 3 6 12 18
313334
Months after randomization
292531
272833
273434
323334
373744
Single-siteDual-site
Control
Single Site Dual Site

PRomPT: PRomPT: ΔΔLVEDV - Subgroup analysis LVEDV - Subgroup analysis
ΔLVEDV was not significantly different in pts in whom the LV lead was vs. was not implanted in the pre-specified target location
(adjusted mean diff (95%CI) = -4.3 (-20.4, 11.8) mL, P=0.60)
ΔLVEDV (Intervention – Control)Mean (95% CI)
ΔLVEDV (Intervention – Control)InteractionP value
Variable # Patients
ALL patients 98 0.6 (-12.3, 13.5)
0.87
Age <median (58 years) ≤median (58 years)
Intervention better Control better-40 -35 -30 -25 -20 -15 -10 -5 0 5 10 15 20 25 30 35 40
4850
3.3 (-14.1, 20.7)1.2 (-18, 20.4)
0.42
Gender Female Male
2771
8.2 (-15.7, 32)-3.2 (-18.6, 12.2)
0.73
Hypertension No Yes
4256
-2.2 (-21.2, 16.8)2.3 (-15.2, 19.8)
0.23
Hyperlipidemia No Yes
5939
6.2 (-10, 22.3)-9.6 (-30.1, 10.9)
0.19
Diabetes No Yes
8117
-3.6 (-17.6, 10.4)20.7 (-13.2, 54.7)
0.34
Infarct Location Anterior Non-anterior
7820
3.6 (-10.6, 17.8)-12.1 (-41.4, 17.3)
0.54
Peak CPK <median (4447 U/L) ≥median (4447 U/L)
4445
0.5 (-19.1, 20.1)8.7 (-9, 26.4)
0.42
Baseline LVEDV <median (105.8 mL) ≥median (105.8 mL)
4949
6.5 (-12.9, 25.9)-4 (-21.5, 13.4)
0.09
Baseline LVEF <median (43.1%) ≥median (43.1%)
4949
9.9 (-8.2, 27.9)-11.5 (-28.6, 5.5)

PRomPT: PRomPT: Secondary echo endpointsSecondary echo endpointsPaired echocardiographic results between the baseline Paired echocardiographic results between the baseline
and 18-month follow-up visitsand 18-month follow-up visits
n Baseline 18-monthAdj mean change
Difference P
LVESV (mL) (95% CI) (95% CI)
Control 3467.7 ± 24.9
81.5 ± 32.5
14.0 (5.4, 22.7) -2.8
(-13.5, 7.9)0.61
Pooled pacing
6461.8
± 21.2
73.1 ± 33.1
11.2 (5.0,
17.5)
LVEF (%)
Control 3443.8 ± 9.1
40.5 ± 10.1
-3.0 (-5.8, -0.2) 2.3
(-1.2, 5.7)
0.20Pooled pacing
6442.5
± 8.9
41.9 ±
10.0
-0.8 (-2.8, 1.3)

PRomPT: PRomPT: Secondary endpoint – 6MWTSecondary endpoint – 6MWTPaired 6 minute walk test results between the 1-month Paired 6 minute walk test results between the 1-month
and 18-month follow-up visitsand 18-month follow-up visits
6MWT (meters)
n Baseline 18-monthAdj mean change
(95% CI)
Difference(95%CI)
P
Control 28399.6 ±
155.0
410.3 ±
151.8
15.6 (-32.1, 63.2)
22.0 (-35.3, 79.3)
0.45
Pooled pacing
63384.2 ±
134.8
424.0 ±
145.6
37.6 (5.8, 69.3)

PRomPT: PRomPT: Secondary endpoints - QoLSecondary endpoints - QoLPaired Minnesota Living with Heart Failure and EQ-5D Paired Minnesota Living with Heart Failure and EQ-5D
results between the baseline and 18-month follow-up visitsresults between the baseline and 18-month follow-up visits
n Baseline 18-monthAdj mean change
Difference P
MLWHF score (95% CI) (95% CI)
Control 3229.6 ±
29.7
26.8 ± 25.4
-0.1 (-8.5,
8.3) 0.5 (-9.6, 10.7)
0.92Pooled pacing
6924.6 ±
24.5
26.2 ±
24.2
0.4 (-5.3,
6.1)
EQ-5D score
Control 330.8 ± 0.2
0.8 ± 0.2
0.1 (0.0,
0.1)-0.0 (-
0.1, 0.1)
0.99Pooled pacing
690.8 ±
0.2
0.8 ± 0.2
0.1 (0.0, 0.1)

PRomPT: PRomPT: Secondary endpoints - NYHASecondary endpoints - NYHAPaired NYHA classification between the baseline and 18-Paired NYHA classification between the baseline and 18-
month follow-up visitsmonth follow-up visits
NYHA class
Control group Pooled pacing groups
Pro
po
rtio
n
P=0.67P=0.67

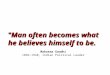
PRomPT: PRomPT: Death or HF Hospitalization Death or HF Hospitalization
Pooled Pacing vs. ControlHR 0.79 (0.34, 1.86)
P = 0.59
Pooled Pacing (n=75)Control (n=45)
82.6%
Number at Risk:7545
Pooled PacingControl
1.0
Fre
edo
m f
rom
Dea
th o
rH
F H
osp
ital
izat
ion
0.8
0.6
0.4
0.2
0
6738
50
6635
100
Days after Randomization
6334
150
6232
200
6132
250
6132
300
6131
350
6131
400
6030
450
5930
500
5825
Month 18
0.0
78.3%

PRomPT: PRomPT: Adverse events during FUAdverse events during FU
Pooled pacing Pooled pacing
(n=75)(n=75)Control Control (n=45)(n=45) HR (95% CI)HR (95% CI)
PP
valuevalue
DeathDeath 3 (4.0%)3 (4.0%) 2 (4.7%)2 (4.7%)0.83 0.83
(0.14, 4.98)
0.840.84
- Cardiac death- Cardiac death 3 (4.0%)3 (4.0%) 1 (2.4%)1 (2.4%)1.64 1.64 (0.17,
15.82)0.660.66
- Sudden death- Sudden death 1 (1.4%)1 (1.4%) 1 (2.4%)1 (2.4%) 0.56 0.56 (0.03, 9.03)
0.680.68
- Non-cardiac death- Non-cardiac death 0 (0.0%)0 (0.0%) 1 (2.3%)1 (2.3%) -- 0.190.19
Hospitalization, allHospitalization, all 29 (39.9%)29 (39.9%) 18 (44.7%)18 (44.7%)0.81 0.81
(0.45, 1.46)
0.480.48
- For heart failure- For heart failure 11 (15.0%)11 (15.0%) 8 (19.6%)8 (19.6%)0.75 0.75
(0.30, 1.87)
0.540.54
Death or hospDeath or hosp 31 (41.5%)31 (41.5%) 19 (46.3%)19 (46.3%)0.82 0.82 (0.46,
1.46)0.500.50
Death or HF hospDeath or HF hosp 13 (17.4%)13 (17.4%) 9 (21.7%)9 (21.7%)0.79 0.79 (0.34,
1.86)0.590.59
Data are time to event Kaplan-Meier estimates, compared by log rank

PRomPT: PRomPT: LimitationsLimitations
• Sample size – reduced to 120 as-treated patientsSample size – reduced to 120 as-treated patients
Nonetheless, the largest trial of its type to dateNonetheless, the largest trial of its type to date
With 95% confidence we can exclude With 95% confidence we can exclude a >12.3 mL reduction in ΔLVEDV with a >12.3 mL reduction in ΔLVEDV with successful peri-infarct pacing successful peri-infarct pacing
• The study was not powered to assess most secondary endpoints, or compare outcomes between the individual pacing groups
• Cannot exclude benefit in subgroups that the trial Cannot exclude benefit in subgroups that the trial was under-powered to detectwas under-powered to detect

In the present multicenter, randomized In the present multicenter, randomized
trial, peri-infarct pacing did not prevent trial, peri-infarct pacing did not prevent
LV remodeling or improve functional or LV remodeling or improve functional or
clinical outcomes during 18 months of clinical outcomes during 18 months of
follow-up in patients with large first MIfollow-up in patients with large first MI
24
PRomPT: PRomPT: ConclusionsConclusions