Embed Size (px)
Citation preview

−−
−
−−− −−−
−
− −−
−−
−
−−
− −
−
−
−0
25
50
75
100
10−2 10−1 100 101 102
cfDNA VAF (%)
Tiss
ue V
AF (%
)
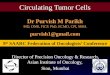
Clonal Statusclonal: called in cfDNA (n=130, 90%)clonal: not called in cfDNA (n=15, 10%)subclonal: called in cfDNA (n=35, 46%)subclonal: not called in cfDNA (n=41, 54%)undetermined: called in cfDNA (n=23, 79%)undetermined: not called in cfDNA (n=6, 21%)
Metastatic Breast Cancer
−−
−−−
−−−
−
−
−−
−−
−
−−
−
−
− −−−
−−
−
−
−−−
− − −
−
−−
−
−0
25
50
75
100
10−2 10−1 100 101 102
cfDNA VAF (%)
Tiss
ue V
AF (%
)Clonal Status
clonal: called in cfDNA (n=164, 80%)clonal: not called in cfDNA (n=42, 20%)subclonal: called in cfDNA (n=39, 59%)subclonal: not called in cfDNA (n=27, 41%)undetermined: called in cfDNA (n=40, 82%)undetermined: not called in cfDNA (n=9, 18%)
Metastatic Lung Cancer
−
−−
−
−
−
−
−−
−
−
−
−
−
−−−−−
−
−
−
−−
0
25
50
75
100
10−2 10−1 100 101 10cfDNA VAF (%)
Tiss
ue V
AF (%
)
Clonal Statusclonal: called in cfDNA (n=87, 77%)clonal: not called in cfDNA (n=26, 23%)subclonal: called in cfDNA (n=15, 52%)subclonal: not called in cfDNA (n=14, 48%)undetermined: called in cfDNA (n=20, 77%)undetermined: not called in cfDNA (n=6, 23%)
Metastatic Prostate Cancer
2
− hotspot (n = 23) − hotspot (n = 38) − hotspot (n = 24)
Performance of a high-intensity 508-gene circulating-tumor DNA (ctDNA) assay in patients with metastatic breast, lung, and prostate cancerPedram Razavi1, Bob T. Li1, Wassim Abida1, Alex Aravanis9, Byoungsok Jung9, Ronglai Shen2, Chenlu Hou9, Ino De Bruijn4, Sante Gnerre9, Raymond S. Lim4, Earl Hubbell9, Dalicia Reales3, Tara Maddala9, Michael F. Berger1, 4, 6, Gregory J. Riely7, Howard I. Scher1, 8, William F. Novotny9, David B. Solit1, 3, 6, Mark Lee9, Jorge S. Reis-Filho4, Jose Baselga1, 3
1. Department of Medicine, Memorial Sloan Kettering Cancer Center (MSKCC), 1275 York Avenue, New York, NY, USA. 2. Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center. 3. Human Oncology and Pathogenesis Program, Memorial Sloan Kettering Cancer Center. 4. Department of Pathology, Memorial Sloan Kettering Cancer Center. 5. Department of Pathology, Molecular Diagnostics Service, Memorial Sloan Kettering Cancer Center. 6. Marie-Josée and Henry R. Kravis Center for Molecular Oncology, Memorial Sloan Kettering Cancer Center. 7. Thoracic Oncology Service, Division of Solid Tumor Oncology, Department of Medicine, Memorial Sloan Kettering Cancer Center. 8. Genitourinary Oncology Service, Department of Medicine, Memorial Sloan Kettering Cancer Center 9. GRAIL, Menlo Park, CA 94402 USA
Background• ctDNA assays can noninvasively assess
tumor burden and biology by identifying tumor-derived somatic alterations
• To date, ctDNA studies have focused primarily on detecting driver mutations to inform treatment strategies in advanced disease or monitoring disease burden in patients with established cancer diagnoses. Platforms used for these purposes target individual variants or limited genomic regions informed by sequencing of tumor tissue. (Wan 2017)
• Analysis of plasma cell-free DNA may enable early cancer detection in previously undiagnosed individuals but will require de novo variant calling (in the absence of tissue) as well as sufficient genomic coverage to address the spectrum of variant profiles that are cancer-defining. (Aravanis 2017)
• We propose that a high-intensity approach (ultra-deep sequencing of plasma cell-free DNA with broad genomic coverage) will add a new dimension to our understanding of intra-patient and population-level heterogeneity.
Objectives• Assess concordance of variants detected in
tissue with MSK-IMPACT™ versus detected in plasma cell-free DNA.
• Assess the cell-free DNA variant detection rate based on observing at least one MSK-IMPACT™ tissue variant in the same patient.
• Assess concordance using tissue as a reference according to:
- Clinical actionability - Clonality
Methods: Patient Population• Metastatic breast, lung, or prostate cancer,
either de novo or with progressive disease on current therapy.
• All patients have provided written informed consent to an MSK institutional protocol (NCT01775072) allowing research of cfDNA and clinical tumor sequencing.
• Blood and tissue were prospectively collected within 6 weeks of each other with no intervening therapy change.
- Two tubes of blood collected in Streck. - Tissue from surgical resection or biopsy.
• Blood and tissue were analyzed independently and blinded to the results of each.
Results: Patient Disposition
Methods: AnalysiscfDNA variant calling pipeline• The variant calling pipeline includes the following steps:
- Read alignment, error correction (consisting of read collapsing by position and UMI, as well as stitching paired reads), de novo assembly, variant calling, and variant filtering.
- Variants are filtered using two approaches (1) heuristics applied based on the surrounding sequence context and type and quality of reads supporting the variant and (2) empirical noise levels observed in a set of healthy samples.
- Blood samples from an independent cohort of 24 non-cancer (self-reported) individuals (vendor sourced) were used to set a baseline noise level in this study.
- Variant calls are further filtered using matching WBC for each patient. - Bioinformatics filters included removing non-COSMIC dbSNP variants as well as restricting to protein coding regions.
MSK tissue variant calling pipeline has been described extensively in the past (Cheng 2015, Zehir 2017)
FACETS algorithm and clonality analysis:• To classify the variants identified in tissue into clonal and subclonal mutations, the cancer cell fraction (CCF) was
calculated based on mutant variant allele frequency (VAF) adjusting for tumor purity, ploidy, and local allele-specific copy number obtained from the FACETS algorithm (Shen 2016).
• Exact confidence intervals (CI) were calculated around the point estimate of CCF: - Mutations with lower bound of 95% CI ≥75% were classified as “clonal”. - Mutations with CCF ≥ 80% and lower bound of 95% CI below 75% were classified as “likely clonal”. - Mutations with CCF < 80% and lower bound of 95% CI below 75% were classified as “subclonal”.
Statistical Methods• Only regions covered by both panels were used for concordance analysis and synonymous variants were excluded from
the concordance analysis since they are not called by the MSK-IMPACT™ pipeline.• Concordance is calculated as positive percent agreement (PPA) with tissue as a reference (cfDNA/tissue).
Methods: Sample Workflows and Assays Results: Per Patient Variant Detection | Primary Analysis – Independent cfDNA and Tissue Assessment
Actionable Mutations in Tissue and Plasma
Consistency of Mutational Signature | APOBEC Hypermutation in Both Tissue and Plasma
• Patient mutational signatures were identified by deconvolving the observed triplet mutation profile of patients using constrained linear regression onto COSMIC mutational signatures (Alexandrov 2013). Patients with evidence for signatures compatible with APOBEC hypermutation were prioritized for cfDNA signature analysis.
• Seven patients (6 breast, 1 prostate) exhibited evidence for increased signature 2 and/or 13 in both tissue and plasma, which are both associated with APOBEC hypermutation; Two patients (MSK-VB-0023 and MSK-VB-0046) shown here.
Patient Characteristics Cancer Characteristics
Enrollment
Analysis
Assigned pt ID (N = 232)
Breast80
Lung82
Prostate70
EligibleEligibleClinically Eligible and Lab Evaluable (N = 161)
NBreast
53
Lung
53
Prostate
55
EligibleClinically Eligible and Lab Evaluable (N = 161)
Breast53
Lung53
Prostate55
cfDNA Assay Evaluable (N = 151)Breast
48Lung
49Prostate
54
Tissue assay unevaluable (N = 27)
Breast
95
Lung
84
Prostate
101cfDNA assay unevaluable (N = 10)
Excluded subjects (N = 71)
Clinical exclusion*Lab exclusions for insufficient sampleTissue or cfDNA assay unevaluable
Breast
27
9108
Lung
29
20**81
Prostate
15
708
* Clinical exclusion includes new systemic therapy, disease progression not
Tissue Assay Evaluable (N = 134)Breast
44Lung
45Prostate
45
Concordance Cohort (N = 124)
Breast39
Lung41
Prostate44
Both Tissue and cfDNA Evaluable
** Includes 2 pseudoprogressionconfirmed on review, etc
Percent of patients for whom at least 1 of the variants detected in tumor tissue was also detected in plasma: Breast cancer - 97%, Lung cancer - 85%, Prostate cancer - 84%.
*Analytical sensitivity and specificity determined by cell line and cfDNA titrations, respectively
cfDNA and tissue assays share 1.2 Mb of targeted sequence.
Most actionable mutations detected in tissue were also detected in plasma (54/71, 76%; SNVs only: 28/31, 90%). A subset of driver mutations were observed in plasma but not tissue, including some with potential therapeutic implications:• Breast: PIK3CA (E453K, E542K, E545K, E726K, M1043I), ERBB2 I767M• Lung: EGFR T790M• Prostate: AR amp, AR (L702H, T878A), BRCA1 trunc, BRCA2 trunc, MLH1, PIK3CA E545K
Num
ber o
f Var
iant
s
0
5
10
15
20
Metastatic Breast Cancer Metastatic Lung Cancer Metastatic Prostate Cancer
AK
T1−E
17K
ER
BB
2 A
mp
FGFR
1 A
mp
FGFR
2 A
mp
PIK
3CA
−E54
2K
PIK
3CA
−E54
5K
PIK
3CA
−E72
6K
PIK
3CA
−H10
47R
PIK
3CA
−M10
43I
PIK
3CA
−N34
5K
EG
FR E
xon
19
EG
FR−G
719A
EG
FR−L
858R
EG
FR−L
861Q
EG
FR−T
790M
ME
T A
mp
RO
S1
Fusi
on
AR
Am
p
AR
−H87
5Y
AR
−L70
2H
BR
CA
1 tru
n
BR
CA
2 tru
n
PIK
3CA
−E54
2K
MSK−IMPACT onlyMSK−IMPACT & GRAIL
MSK−VB−0023 cfDNA
# M
utat
ions
(cfD
NA
)
0
200
400
600
800
1000
C>A C>G C>T T>A T>C T>G
MSK−VB−0023 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
MSK−VB−0046 cfDNA
# M
utat
ions
(cfD
NA
)
0
10
20
30
40
50
60
C>A C>G C>T T>A T>C T>G
MSK−VB−0046 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
Metastatic Prostate CancerTissue calls detection rate by cfDNA
Metastatic Lung CancerTissue calls detection rate by cfDNA
Metastatic Breast CancerTissue calls detection rate by cfDNA
S30S18S15S13S10S7S6S2S1
MS
K−V
B−0
013
MS
K−V
B−0
004
MS
K−V
B−0
024
MS
K−V
B−0
053
MS
K−V
B−0
005
MS
K−V
B−0
006
MS
K−V
B−0
008
MS
K−V
B−0
030
MS
K−V
B−0
059
MS
K−V
B−0
066
MS
K−V
B−0
076
MS
K−V
B−0
016
MS
K−V
B−0
032
MS
K−V
B−0
036
MS
K−V
B−0
062
MS
K−V
B−0
001
MS
K−V
B−0
054
MS
K−V
B−0
063
MS
K−V
B−0
069
MS
K−V
B−0
072
MS
K−V
B−0
084
MS
K−V
B−0
077
MS
K−V
B−0
033
MS
K−V
B−0
037
MS
K−V
B−0
031
MS
K−V
B−0
034
MS
K−V
B−0
012
MS
K−V
B−0
041
MS
K−V
B−0
058
MS
K−V
B−0
040
MS
K−V
B−0
044
MS
K−V
B−0
067
MS
K−V
B−0
029
MS
K−V
B−0
045
MS
K−V
B−0
073
MS
K−V
B−0
023
MS
K−V
B−0
057
MS
K−V
B−0
050
MS
K−V
B−0
046
Metastatic Breast Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
L−00
73M
SK
−VL−
0002
MS
K−V
L−00
10M
SK
−VL−
0015
MS
K−V
L−00
64M
SK
−VL−
0009
MS
K−V
L−00
83M
SK
−VL−
0005
MS
K−V
L−00
13M
SK
−VL−
0051
MS
K−V
L−00
67M
SK
−VL−
0069
MS
K−V
L−00
71M
SK
−VL−
0007
MS
K−V
L−00
21M
SK
−VL−
0028
MS
K−V
L−00
03M
SK
−VL−
0061
MS
K−V
L−00
76M
SK
−VL−
0077
MS
K−V
L−00
82M
SK
−VL−
0012
MS
K−V
L−00
42M
SK
−VL−
0044
MS
K−V
L−00
56M
SK
−VL−
0027
MS
K−V
L−00
45M
SK
−VL−
0054
MS
K−V
L−00
17M
SK
−VL−
0057
MS
K−V
L−00
22M
SK
−VL−
0038
MS
K−V
L−00
80M
SK
−VL−
0074
MS
K−V
L−00
75M
SK
−VL−
0048
MS
K−V
L−00
55M
SK
−VL−
0008
MS
K−V
L−00
60M
SK
−VL−
0065
MS
K−V
L−00
35
Metastatic Lung Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
P−0
030
MS
K−V
P−0
040
MS
K−V
P−0
002
MS
K−V
P−0
005
MS
K−V
P−0
007
MS
K−V
P−0
028
MS
K−V
P−0
029
MS
K−V
P−0
034
MS
K−V
P−0
035
MS
K−V
P−0
003
MS
K−V
P−0
008
MS
K−V
P−0
015
MS
K−V
P−0
016
MS
K−V
P−0
018
MS
K−V
P−0
026
MS
K−V
P−0
037
MS
K−V
P−0
042
MS
K−V
P−0
045
MS
K−V
P−0
051
MS
K−V
P−0
056
MS
K−V
P−0
001
MS
K−V
P−0
031
MS
K−V
P−0
032
MS
K−V
P−0
059
MS
K−V
P−0
004
MS
K−V
P−0
009
MS
K−V
P−0
010
MS
K−V
P−0
014
MS
K−V
P−0
033
MS
K−V
P−0
038
MS
K−V
P−0
046
MS
K−V
P−0
047
MS
K−V
P−0
050
MS
K−V
P−0
061
MS
K−V
P−0
006
MS
K−V
P−0
021
MS
K−V
P−0
054
MS
K−V
P−0
019
MS
K−V
P−0
024
MS
K−V
P−0
025
MS
K−V
P−0
058
MS
K−V
P−0
057
MS
K−V
P−0
041
MS
K−V
P−0
023
Metastatic Prostate Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
Tissue assay onlyTissue & cfDNA assay
Post-hoc Analysis | Association between Cancer Cell Fraction (CCF) in Tumor and Detection Rate in Plasma
• Clonal variants in tissue were more likely to be detected in plasma than subclonal variants (p<.0001).• The greater the representation of cancer cell fraction (CCF) from FACETS in the tumor, the higher the detection in plasma.
Num
ber o
f Var
iant
s
0
5
10
15
20
Metastatic Breast Cancer Metastatic Lung Cancer Metastatic Prostate Cancer
AK
T1−E
17K
ER
BB
2 A
mp
FGFR
1 A
mp
FGFR
2 A
mp
PIK
3CA
−E54
2K
PIK
3CA
−E54
5K
PIK
3CA
−E72
6K
PIK
3CA
−H10
47R
PIK
3CA
−M10
43I
PIK
3CA
−N34
5K
EG
FR E
xon
19
EG
FR−G
719A
EG
FR−L
858R
EG
FR−L
861Q
EG
FR−T
790M
ME
T A
mp
RO
S1
Fusi
on
AR
Am
p
AR
−H87
5Y
AR
−L70
2H
BR
CA
1 tru
n
BR
CA
2 tru
n
PIK
3CA
−E54
2K
MSK−IMPACT onlyMSK−IMPACT & GRAIL
MSK−VB−0023 cfDNA
# M
utat
ions
(cfD
NA
)
0
200
400
600
800
1000
C>A C>G C>T T>A T>C T>G
MSK−VB−0023 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
MSK−VB−0046 cfDNA#
Mut
atio
ns (c
fDN
A)
0
10
20
30
40
50
60
C>A C>G C>T T>A T>C T>G
MSK−VB−0046 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
Metastatic Prostate CancerTissue calls detection rate by cfDNA
Metastatic Lung CancerTissue calls detection rate by cfDNA
Metastatic Breast CancerTissue calls detection rate by cfDNA
S30S18S15S13S10S7S6S2S1
MS
K−V
B−0
013
MS
K−V
B−0
004
MS
K−V
B−0
024
MS
K−V
B−0
053
MS
K−V
B−0
005
MS
K−V
B−0
006
MS
K−V
B−0
008
MS
K−V
B−0
030
MS
K−V
B−0
059
MS
K−V
B−0
066
MS
K−V
B−0
076
MS
K−V
B−0
016
MS
K−V
B−0
032
MS
K−V
B−0
036
MS
K−V
B−0
062
MS
K−V
B−0
001
MS
K−V
B−0
054
MS
K−V
B−0
063
MS
K−V
B−0
069
MS
K−V
B−0
072
MS
K−V
B−0
084
MS
K−V
B−0
077
MS
K−V
B−0
033
MS
K−V
B−0
037
MS
K−V
B−0
031
MS
K−V
B−0
034
MS
K−V
B−0
012
MS
K−V
B−0
041
MS
K−V
B−0
058
MS
K−V
B−0
040
MS
K−V
B−0
044
MS
K−V
B−0
067
MS
K−V
B−0
029
MS
K−V
B−0
045
MS
K−V
B−0
073
MS
K−V
B−0
023
MS
K−V
B−0
057
MS
K−V
B−0
050
MS
K−V
B−0
046
Metastatic Breast Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
L−00
73M
SK
−VL−
0002
MS
K−V
L−00
10M
SK
−VL−
0015
MS
K−V
L−00
64M
SK
−VL−
0009
MS
K−V
L−00
83M
SK
−VL−
0005
MS
K−V
L−00
13M
SK
−VL−
0051
MS
K−V
L−00
67M
SK
−VL−
0069
MS
K−V
L−00
71M
SK
−VL−
0007
MS
K−V
L−00
21M
SK
−VL−
0028
MS
K−V
L−00
03M
SK
−VL−
0061
MS
K−V
L−00
76M
SK
−VL−
0077
MS
K−V
L−00
82M
SK
−VL−
0012
MS
K−V
L−00
42M
SK
−VL−
0044
MS
K−V
L−00
56M
SK
−VL−
0027
MS
K−V
L−00
45M
SK
−VL−
0054
MS
K−V
L−00
17M
SK
−VL−
0057
MS
K−V
L−00
22M
SK
−VL−
0038
MS
K−V
L−00
80M
SK
−VL−
0074
MS
K−V
L−00
75M
SK
−VL−
0048
MS
K−V
L−00
55M
SK
−VL−
0008
MS
K−V
L−00
60M
SK
−VL−
0065
MS
K−V
L−00
35
Metastatic Lung Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
P−0
030
MS
K−V
P−0
040
MS
K−V
P−0
002
MS
K−V
P−0
005
MS
K−V
P−0
007
MS
K−V
P−0
028
MS
K−V
P−0
029
MS
K−V
P−0
034
MS
K−V
P−0
035
MS
K−V
P−0
003
MS
K−V
P−0
008
MS
K−V
P−0
015
MS
K−V
P−0
016
MS
K−V
P−0
018
MS
K−V
P−0
026
MS
K−V
P−0
037
MS
K−V
P−0
042
MS
K−V
P−0
045
MS
K−V
P−0
051
MS
K−V
P−0
056
MS
K−V
P−0
001
MS
K−V
P−0
031
MS
K−V
P−0
032
MS
K−V
P−0
059
MS
K−V
P−0
004
MS
K−V
P−0
009
MS
K−V
P−0
010
MS
K−V
P−0
014
MS
K−V
P−0
033
MS
K−V
P−0
038
MS
K−V
P−0
046
MS
K−V
P−0
047
MS
K−V
P−0
050
MS
K−V
P−0
061
MS
K−V
P−0
006
MS
K−V
P−0
021
MS
K−V
P−0
054
MS
K−V
P−0
019
MS
K−V
P−0
024
MS
K−V
P−0
025
MS
K−V
P−0
058
MS
K−V
P−0
057
MS
K−V
P−0
041
MS
K−V
P−0
023
Metastatic Prostate Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
Tissue assay onlyTissue & cfDNA assay
Post-hoc Analysis | ctDNA VAF versus Tissue VAF by Clonal Status
Num
ber o
f Var
iant
s
0
5
10
15
20
Metastatic Breast Cancer Metastatic Lung Cancer Metastatic Prostate Cancer
AK
T1−E
17K
ER
BB
2 A
mp
FGFR
1 A
mp
FGFR
2 A
mp
PIK
3CA
−E54
2K
PIK
3CA
−E54
5K
PIK
3CA
−E72
6K
PIK
3CA
−H10
47R
PIK
3CA
−M10
43I
PIK
3CA
−N34
5K
EG
FR E
xon
19
EG
FR−G
719A
EG
FR−L
858R
EG
FR−L
861Q
EG
FR−T
790M
ME
T A
mp
RO
S1
Fusi
on
AR
Am
p
AR
−H87
5Y
AR
−L70
2H
BR
CA
1 tru
n
BR
CA
2 tru
n
PIK
3CA
−E54
2K
MSK−IMPACT onlyMSK−IMPACT & GRAIL
MSK−VB−0023 cfDNA
# M
utat
ions
(cfD
NA
)
0
200
400
600
800
1000
C>A C>G C>T T>A T>C T>G
MSK−VB−0023 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
MSK−VB−0046 cfDNA
# M
utat
ions
(cfD
NA
)
0
10
20
30
40
50
60
C>A C>G C>T T>A T>C T>G
MSK−VB−0046 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
Metastatic Prostate CancerTissue calls detection rate by cfDNA
Metastatic Lung CancerTissue calls detection rate by cfDNA
Metastatic Breast CancerTissue calls detection rate by cfDNA
S30S18S15S13S10S7S6S2S1
MS
K−V
B−0
013
MS
K−V
B−0
004
MS
K−V
B−0
024
MS
K−V
B−0
053
MS
K−V
B−0
005
MS
K−V
B−0
006
MS
K−V
B−0
008
MS
K−V
B−0
030
MS
K−V
B−0
059
MS
K−V
B−0
066
MS
K−V
B−0
076
MS
K−V
B−0
016
MS
K−V
B−0
032
MS
K−V
B−0
036
MS
K−V
B−0
062
MS
K−V
B−0
001
MS
K−V
B−0
054
MS
K−V
B−0
063
MS
K−V
B−0
069
MS
K−V
B−0
072
MS
K−V
B−0
084
MS
K−V
B−0
077
MS
K−V
B−0
033
MS
K−V
B−0
037
MS
K−V
B−0
031
MS
K−V
B−0
034
MS
K−V
B−0
012
MS
K−V
B−0
041
MS
K−V
B−0
058
MS
K−V
B−0
040
MS
K−V
B−0
044
MS
K−V
B−0
067
MS
K−V
B−0
029
MS
K−V
B−0
045
MS
K−V
B−0
073
MS
K−V
B−0
023
MS
K−V
B−0
057
MS
K−V
B−0
050
MS
K−V
B−0
046
Metastatic Breast Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
L−00
73M
SK
−VL−
0002
MS
K−V
L−00
10M
SK
−VL−
0015
MS
K−V
L−00
64M
SK
−VL−
0009
MS
K−V
L−00
83M
SK
−VL−
0005
MS
K−V
L−00
13M
SK
−VL−
0051
MS
K−V
L−00
67M
SK
−VL−
0069
MS
K−V
L−00
71M
SK
−VL−
0007
MS
K−V
L−00
21M
SK
−VL−
0028
MS
K−V
L−00
03M
SK
−VL−
0061
MS
K−V
L−00
76M
SK
−VL−
0077
MS
K−V
L−00
82M
SK
−VL−
0012
MS
K−V
L−00
42M
SK
−VL−
0044
MS
K−V
L−00
56M
SK
−VL−
0027
MS
K−V
L−00
45M
SK
−VL−
0054
MS
K−V
L−00
17M
SK
−VL−
0057
MS
K−V
L−00
22M
SK
−VL−
0038
MS
K−V
L−00
80M
SK
−VL−
0074
MS
K−V
L−00
75M
SK
−VL−
0048
MS
K−V
L−00
55M
SK
−VL−
0008
MS
K−V
L−00
60M
SK
−VL−
0065
MS
K−V
L−00
35
Metastatic Lung Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
P−0
030
MS
K−V
P−0
040
MS
K−V
P−0
002
MS
K−V
P−0
005
MS
K−V
P−0
007
MS
K−V
P−0
028
MS
K−V
P−0
029
MS
K−V
P−0
034
MS
K−V
P−0
035
MS
K−V
P−0
003
MS
K−V
P−0
008
MS
K−V
P−0
015
MS
K−V
P−0
016
MS
K−V
P−0
018
MS
K−V
P−0
026
MS
K−V
P−0
037
MS
K−V
P−0
042
MS
K−V
P−0
045
MS
K−V
P−0
051
MS
K−V
P−0
056
MS
K−V
P−0
001
MS
K−V
P−0
031
MS
K−V
P−0
032
MS
K−V
P−0
059
MS
K−V
P−0
004
MS
K−V
P−0
009
MS
K−V
P−0
010
MS
K−V
P−0
014
MS
K−V
P−0
033
MS
K−V
P−0
038
MS
K−V
P−0
046
MS
K−V
P−0
047
MS
K−V
P−0
050
MS
K−V
P−0
061
MS
K−V
P−0
006
MS
K−V
P−0
021
MS
K−V
P−0
054
MS
K−V
P−0
019
MS
K−V
P−0
024
MS
K−V
P−0
025
MS
K−V
P−0
058
MS
K−V
P−0
057
MS
K−V
P−0
041
MS
K−V
P−0
023
Metastatic Prostate Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
Tissue assay onlyTissue & cfDNA assay
Patient Characteristics Breast (n=39) Lung (n=41) Prostate (n=44)
Age at enrollment
Mean (SD) 56.5 (11.55) 65.2 (11.18) 67.3 (10.03)
Median 60 67 67
Range 30, 79 33, 83 46, 87
Gender, N (%)
Female 39 (100.0%) 28 (68.3%) N/A
Histology N (%)
Metastatic Breast Cancer (n=39)
Breast Invasive Ductal Carcinoma 32 (82.1%)
Breast Invasive Lobular Carcinoma 2 (5.1%)
Breast Mixed Ductal and Lobular Carcinoma 5 (12.8%)
Metastatic Lung Cancer (n=41)
Lung Adenocarcinoma 38 (92.7%)
Lung Non-adenocarcinoma 3 (7.3%)
Metastatic Prostate Cancer (n=44)
Prostate Adenocarcinoma 39 (88.6%)
Prostate Neuroendocrine 5 (11.4%)
Number of patients
Evaluable With at least one clonal mutation detected in tissue
At least one clonal mutation detected in cfDNA
Metastatic Breast Cancer 39 36 35 (97%)
Metastatic Lung Cancer 41 37 31 (84%)
Metastatic Prostate Cancer 44 40 33 (83%)
Post-hoc Analysis on Clonal Mutations
Pooled Variant Detection | Primary Analysis – Independent cfDNA and Tissue Assessment
PPA = positive percent agreement with tissue as a reference (cfDNA/tissue)In tissue, pooled across patients, 864 variants were detected across the 3 tumor types, with 627 (73%) also detected in plasma: single nucleotide variants/indels - 75%, fusions - 67%, and copy number alterations - 58%. * For breast and lung cancer, defined based on OncoKB, precision knowledge base maintained at MSKCC. In breast cancer, variants known to contribute to progression, level 1, 2, or 3 evidence. In lung cancer, variants shown to predict sensitivity or resistance to targeted therapy, level 1 or 2 evidence. In prostate cancer, variants shown to contribute to progression (Chang 2015, Robinson 2015).
All Variants (SNV, indels, CNA, Fusions) SNV/ indels ONLY Clinically Actionable Mutations*
/tissue PPA (95% CI) cfDNA/tissue PPA (95% CI) cfDNA/tissue PPA (95% CI)
Metastatic Breast Cancer Patient 221 / 300 74% (68, 79) 188 / 250 75% (69, 80) 24 / 27 89% (71, 98)
Metastatic Lung Cancer Patient 256 / 355 72% (67, 77) 243 / 321 76% (71, 80) 11 / 18 61% (36, 83)
Metastatic Prostate Cancer Patient 150 / 209 72% (65, 78) 122 / 168 73% (65, 79) 19 / 26 73% (52, 88)
All Patients 627 / 864 73% (69, 76) 553 / 739 75% (72, 78) 54 / 71 76% (64, 85)
cfDNA Assay Tissue Assay
Inputs PlasmaWBC
FFPE tissue biopsyWBC
Genes 508 410
Breadth (Mb) 2.13 1.36
Raw sequencing coverage >60,000X (~3-4000 error corrected depth) 500 - 1000X
Enrichment Hybridization capture Hybridization capture
Analytical Metrics
SNV/indel detection (30 ng input DNA)Sensitivity*: >95% @ 0.2% MAF >70% @ 0.1% MAF Specificity*: 99.992%
LOD of 2% for hotspot mutations and 5% for non-hotspot mutations
Num
ber o
f Var
iant
s
0
5
10
15
20
Metastatic Breast Cancer Metastatic Lung Cancer Metastatic Prostate Cancer
AK
T1−E
17K
ER
BB
2 A
mp
FGFR
1 A
mp
FGFR
2 A
mp
PIK
3CA
−E54
2K
PIK
3CA
−E54
5K
PIK
3CA
−E72
6K
PIK
3CA
−H10
47R
PIK
3CA
−M10
43I
PIK
3CA
−N34
5K
EG
FR E
xon
19
EG
FR−G
719A
EG
FR−L
858R
EG
FR−L
861Q
EG
FR−T
790M
ME
T A
mp
RO
S1
Fusi
on
AR
Am
p
AR
−H87
5Y
AR
−L70
2H
BR
CA
1 tru
n
BR
CA
2 tru
n
PIK
3CA
−E54
2K
MSK−IMPACT onlyMSK−IMPACT & GRAIL
MSK−VB−0023 cfDNA
# M
utat
ions
(cfD
NA
)
0
200
400
600
800
1000
C>A C>G C>T T>A T>C T>G
MSK−VB−0023 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
MSK−VB−0046 cfDNA
# M
utat
ions
(cfD
NA
)
0
10
20
30
40
50
60
C>A C>G C>T T>A T>C T>G
MSK−VB−0046 Tumor
# M
utat
ions
(Tum
or)
0
2
4
6
8
C>A C>G C>T T>A T>C T>G
0.0
0.2
0.4
0.6
0.8
1.0
0.0
0.2
0.4
0.6
0.8
1.0
Metastatic Prostate CancerTissue calls detection rate by cfDNA
Metastatic Lung CancerTissue calls detection rate by cfDNA
Metastatic Breast CancerTissue calls detection rate by cfDNA
S30S18S15S13S10S7S6S2S1
MS
K−V
B−0
013
MS
K−V
B−0
004
MS
K−V
B−0
024
MS
K−V
B−0
053
MS
K−V
B−0
005
MS
K−V
B−0
006
MS
K−V
B−0
008
MS
K−V
B−0
030
MS
K−V
B−0
059
MS
K−V
B−0
066
MS
K−V
B−0
076
MS
K−V
B−0
016
MS
K−V
B−0
032
MS
K−V
B−0
036
MS
K−V
B−0
062
MS
K−V
B−0
001
MS
K−V
B−0
054
MS
K−V
B−0
063
MS
K−V
B−0
069
MS
K−V
B−0
072
MS
K−V
B−0
084
MS
K−V
B−0
077
MS
K−V
B−0
033
MS
K−V
B−0
037
MS
K−V
B−0
031
MS
K−V
B−0
034
MS
K−V
B−0
012
MS
K−V
B−0
041
MS
K−V
B−0
058
MS
K−V
B−0
040
MS
K−V
B−0
044
MS
K−V
B−0
067
MS
K−V
B−0
029
MS
K−V
B−0
045
MS
K−V
B−0
073
MS
K−V
B−0
023
MS
K−V
B−0
057
MS
K−V
B−0
050
MS
K−V
B−0
046
Metastatic Breast Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
L−00
73M
SK
−VL−
0002
MS
K−V
L−00
10M
SK
−VL−
0015
MS
K−V
L−00
64M
SK
−VL−
0009
MS
K−V
L−00
83M
SK
−VL−
0005
MS
K−V
L−00
13M
SK
−VL−
0051
MS
K−V
L−00
67M
SK
−VL−
0069
MS
K−V
L−00
71M
SK
−VL−
0007
MS
K−V
L−00
21M
SK
−VL−
0028
MS
K−V
L−00
03M
SK
−VL−
0061
MS
K−V
L−00
76M
SK
−VL−
0077
MS
K−V
L−00
82M
SK
−VL−
0012
MS
K−V
L−00
42M
SK
−VL−
0044
MS
K−V
L−00
56M
SK
−VL−
0027
MS
K−V
L−00
45M
SK
−VL−
0054
MS
K−V
L−00
17M
SK
−VL−
0057
MS
K−V
L−00
22M
SK
−VL−
0038
MS
K−V
L−00
80M
SK
−VL−
0074
MS
K−V
L−00
75M
SK
−VL−
0048
MS
K−V
L−00
55M
SK
−VL−
0008
MS
K−V
L−00
60M
SK
−VL−
0065
MS
K−V
L−00
35
Metastatic Lung Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
MS
K−V
P−0
030
MS
K−V
P−0
040
MS
K−V
P−0
002
MS
K−V
P−0
005
MS
K−V
P−0
007
MS
K−V
P−0
028
MS
K−V
P−0
029
MS
K−V
P−0
034
MS
K−V
P−0
035
MS
K−V
P−0
003
MS
K−V
P−0
008
MS
K−V
P−0
015
MS
K−V
P−0
016
MS
K−V
P−0
018
MS
K−V
P−0
026
MS
K−V
P−0
037
MS
K−V
P−0
042
MS
K−V
P−0
045
MS
K−V
P−0
051
MS
K−V
P−0
056
MS
K−V
P−0
001
MS
K−V
P−0
031
MS
K−V
P−0
032
MS
K−V
P−0
059
MS
K−V
P−0
004
MS
K−V
P−0
009
MS
K−V
P−0
010
MS
K−V
P−0
014
MS
K−V
P−0
033
MS
K−V
P−0
038
MS
K−V
P−0
046
MS
K−V
P−0
047
MS
K−V
P−0
050
MS
K−V
P−0
061
MS
K−V
P−0
006
MS
K−V
P−0
021
MS
K−V
P−0
054
MS
K−V
P−0
019
MS
K−V
P−0
024
MS
K−V
P−0
025
MS
K−V
P−0
058
MS
K−V
P−0
057
MS
K−V
P−0
041
MS
K−V
P−0
023
Metastatic Prostate Cancer
Num
ber o
f Var
iant
s
0
5
10
15
20
25
30
35
Tissue assay onlyTissue & cfDNA assay
Triplet mutational counts and signatures deconvolved from cfDNA for both samples VB-0046 (left), VB-0023 (right)
At least 1 MSK-IMPACT™-detected variant in tumor N PatientscfDNA/tissue
DetectionRate (%) 95% CI
All Patients 110/124 89 (82, 94)
Metastatic Breast Cancer Patients 38/39 97 (87, 100)
Metastatic Lung Cancer Patients 35/41 85 (71, 94)
Metastatic Prostate Cancer Patients 37/44 84 (70, 93)
ConcordanceAnalysis
Normal Cells
FFPE Tissue
PathologyReview
MSK-IMPACT 410-gene panel
TM
500 - 1,000x rawtarget coverage
Variant callingAnnotationFiltering
Blood(Streck BCT)
Plasma/Buffy CoatSeparation
Optimized single-tube library prepUnique Molecular Identifiers for error suppression
Error suppressionVariant callingAnnotationFiltering
508-gene cancer panel (2.1 Mb)
>60,000x raw target coverage for both cfDNA and gDNA
High-intensity Sequencing
DNA Extraction
Library Prep
Target Capture
Sequencing
Analysis
Tissue Assay cfDNA Assay
Tumor D
NA
Norm
al cell DN
A
Plasma cfD
NA
WB
C gD
NA
# of lines of therapy, N (%)
0 20 (51.3%) 25 (61.0%) 12 (27.3%)
1 2 (5.1%) 9 (22.0%) 14 (31.8%)
2 2 (5.1%) 3 (7.3%) 9 (20.5%)
>=3 15 (38.5%) 4 (9.8%) 9 (20.5%)
Tissue Sampled for MSK-IMPACT™, N (%)
Metastatic 35 (89.7%) 28 (68.3%) 44 (100.0%)
Primary 4 (10.3%) 13 (31.7%) 0
Receptor Status, N (%)
HR+/HER2+ 3 (7.7%) N/A N/A
HR+/HER2- 26 (66.7%) N/A N/A
HR-/HER2+ 2 (5.1%) N/A N/A
Triple Negative 8 (20.5%) N/A N/A
Summary • Tumor tissue variants identified by MSK-IMPACT™,
a validated tumor tissue profiling platform, enabled a demonstration of high overall detection rates (>70%) of the same variants in cfDNA.
• In the majority of patients, at least one mutation detected in tissue was also detected in plasma cfDNA of that same patient (97%, 85%, and 84% in breast, lung, and prostate cancer patients).
• Post-hoc analysis focused on the subset of patients with clonal variants in tissue:
- Based on de-novo variant calls, at least one clonal mutation was detected in cfDNA: 97%, 84%, and 83% in breast, lung, and prostate cancer patients.
• The majority of clinically actionable mutations detected in tissue were also detected in plasma (54/71, 76%; SNVs only: 28/31, 90%).
• The breadth of detected variants in plasma cfDNA enables greater insight into tumor biology, including observation of hypermutation signatures.
Conclusions• This novel, high-intensity cell-free DNA sequencing
assay incorporates unprecedented breadth (10X number of genes) compared to previous assays at these sequencing depths, and demonstrated high levels of concordance for both clonal and non-clonal variants between plasma and tissue.
• By interpreting concordance as strong evidence for tumor DNA detection, an extremely high level of tumor DNA detection in plasma was demonstrated.
• Clinically actionable non-biopsy somatic alterations were detected, which may represent tumor heterogeneity not detectable in a single tissue biopsy. Ongoing work is being conducted to distinguish technical noise from the assay and biological signal for the variants detected in plasma but not in tissue.
• The breadth of the panel enabled the first exploration of mutational signature analysis in plasma, revealing samples with APOBEC signatures.
• This study is part of a larger program to evaluate high-intensity sequencing approaches (e.g. whole genome) to characterize potential cancer-defining signals in cell-free nucleic acids, with an ultimate goal of enabling detection of cancer at early curable stages.
ReferencesctDNAWan, J.C., Massie, C., Garcia-Corbacho, J., Mouliere, F., Brenton, J.D., Caldas, C., … Rosenfeld, N. (2017). Liquid biopsies come of age: towards implementation of circulating tumour DNA. Nat Rev Cancer, 17, 223-38. https://doi.org/10.1038/nrc.2017.7
Aravanis, A.M., Lee, M., Klausner, R.D. (2017). Next-generation sequencing of circulating tumor DNA for early cancer detection. Cell, 168, 571-74. https://doi.org/10.1016/j.cell.2017.01.030
Clinically Actionable VariantsChang, M.T., Asthana, S., Gao, S.P., Lee, B.H., Chapman, J.S., ... Taylor, B.S. (2015). Identifying recurrent mutations in cancer reveals widespread lineage diversity and mutational specificity. Nature Biotechnology, 34, 155-63. https://doi.org/10.1038/nbt.3391
Robinson, D., Van Allen, E.M., Wu, Y.M., Schultz, N., Lonigro, R.J., ... Chinnaiyan, A.M. (2015). Integrative Clinical Genomics of Advanced Prostate Cancer. Cell 161:1215-1228. https://doi.org/10.1016/j.cell.2015.05.001
Mutation SignatureAlexandrov, L.B., Nik-Zainal, S., Wedge, D.C., Aparicio, S. a J. R., Behjati, S., Biankin, A.V, … Stratton, M.R. (2013). Signatures of mutational processes in human cancer. Nature, 500, 415–21. https://doi.org/10.1038/nature12477
MSK-IMPACTCheng, D.T., Mitchell, T.N., Zehir, A., Shah, R.H., Benayed, R., Syed, A., … Berger, M.F. (2015). Memorial Sloan Kettering-integrated mutation profiling of actionable cancer targets (MSK-IMPACT): A hybridization capture-based next-generation sequencing clinical assay for solid tumor molecular oncology. Journal of Molecular Diagnostics, 17(3), 251–264. https://doi.org/10.1016/j.jmoldx.2014.12.006
Zehir, A., Benayed, R., Shah, R.H., Syed, A., Middha, S., … Berger, M.F. (2017). Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nature Med, https://doi.org/0.1038/nm.4333
FACETSShen, R., & Seshan, V. E. (2016). FACETS: Allele-specific copy number and clonal heterogeneity analysis tool for high-throughput DNA sequencing. Nucleic Acids Research, 44(16), 1–9. https://doi.org/10.1093/nar/gkw520
Tissue Assay cfDNA Assay