Embed Size (px)
Citation preview

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR1
ARTHUR B. OTIS, HERMANN RAHN, MARVIN A. EPSTEIN AND
WALLACE 0. FENN
From the Department of Physiology, School of Medicine and Dentistry, University of Rochester, Rochester, New York
Received for publication December 26, 1945
In a previous report (Rahn et al., 1946) some effects of hyperventilation on performance test scores were described. In these experiments oxygen was breathed at a simulated altitude of 30,000 feet. The results could be related to changes in alveolar carbon dioxide tension alone, since the alveolar oxygen tension never fell below the normal ground level range.
The experiments reported below constitute an attempt to relate performance to alveolar gas composition when both the oxygen and carbon dioxide tensions are varied simultaneously and when one or the other is varied singly.
METHODS. All experiments were conducted in our high altitude chamber. Alveolar gas tensions were varied by 1, hyperventilation with the aid of the G.E.X. pneumolator; 2, by the addition of dead space (rubber hose) between mask and demand valve, and 3, by change of pressure in the high altitude cham- ber. Performance was measured bv the Hecht contrast discrimination test v and by a modification of the hand steadiness test described in a previous report (Fenn et al., 1946).
In the hand steadiness test, as originally described, the score w ‘as taken as the total number of contacts made by the subject during a 30 second test period. Preliminary experiments showed that this method of scoring may involve a serious error when the subject is very anoxic. Such a subject tends to allow the stylus to remain in contact with the plate for relatively long intervals of time during the test period.2 The number of hits, which tends to be relatively few in such a case, is a poor measure of the subject’s steadiness, because it is much easier for a subject to rest the stylus against the side of the hole than to hold it in the hole without touching. This problem has been solved by taking as the score, not the number of hits, but the total time during which the stylus makes contact in a period of 30 seconds. This time was measured in units of & second by an A.C. impulse counter included in a circuit that was closed when- ever the stylus made contact with the plate.
The general plan for an experiment was as follows. The subject entered the
1 Work done under contract recommended by the Committee on Medical Research be- tween the Office of Research and Development and the University of Rochester.
2 In this test the subject endeavors to hold a stylus in a hole in a brass plate for a period of 30 seconds without making electrical contact with the sides of the hole. The stylus has a diameter of &” and the hole t”. The elbow rests on the table but not the hand. The hole was l$" above the table in a brass plate tilted at an angle of 45” with the vertical. A very similar apparatus is sold by Stoelting and Co., Chicago, catalogue no. 19523.
207

208 OTIS, RAHN, EPSTEIN AND FENN
high altitude chamber in which the illumination was set at a level which had previously been determined as being suitable for administering the contrast discrimination test. Following a period of 15 minutes, which was allowed for the subject to become adapted to this degree of illumination, the subject put on a mask and breathed air or oxygen from a demand system. The steadiness test and the contrast discrimination test were then administered alternately until three trials of each were completed. The scores thus obtained served as normal control values. In a few flights the control scores were obtained at 16,000 feet breathing oxygen instead of at ground level. In experiments where the use of the pneumolator was anticipated
9 the subject performed the control trials of the
steadiness test while temporarily breathing on the pneumolator. This was done so as to have a control on the possible mechanical disturbance caused by the action of the pneumolator.
The subject with an observer was then taken to altitude where he proceeded to breathe air or oxygen either from a demand valve, or from a demand valve with added dead space, or from the G.E.X. pneumolator. The maximum altitude used in these experiments was 24,000 feet. After a period of from 5 to 10 minutes, allowed for the subject to become adjusted to the conditions, the tests were administered in the same fashion as at ground level. Upon completion of the second trial of the tests, an alveolar air sample, subsequently analyzed by the Haldane method, was taken. Following this a third trial of the tests was administered. Approximately half an hour was required to complete the series of measurements. Upon completion of the third trial of the tests, the chamber was changed to a new altitude or the setting of the pneum&t,or was changed or a different dead space was substituted, and another series of tests was administered and an alveolar sample was obtained.
During these experiments the subject wore electrodes connected to a car- diotachometer, and a heart rate record was obtained during the performance of each contrast discrimination test. In flights where anoxia was involved the subject also wore an ear oximeter. Unfortunately the oximeter readings proved to be so unreliable during most of these flights that it has seemed wise to discard the results. The cause of our difficulty seems to have been a faulty ear piece, since replaced by the manufacturer.
Eleven individuals (ten males and one female) served as subjects for these experiments. pleted.
A total of 85 control runs and 171 experimental runs were com-
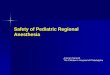
RESULTS: One method of presenting the data is shown in figures 1 and 2. Each experimental series of three tests is represented by a symbol on one of these charts. The location of a symbol is determined by the alveolar carbon dioxide and oxygen tensions which existed during the performance. The type of symbol designates the probability, as determined by Fisher’s “t” test, that the subject’s scores in an experimental series of three trials of a test were not different from his control scores obtained breathing air or oxygen at ground level. The specific meaning of each type of symbol is indicated in the legend accompanying the figures.

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR 209
This sort of graph with oxygen and carbon dioxide tensions as coordinates is advantageous in that contour lines representing equivalent altitudes and per cent saturations (nomogram of Henderson 1928) can be drawn readily. A line representing the normal composition of alveolar air from the data of Boothby has been added for reference.
70 t\
65% CO2 NARCOSIS
I 80 36_Hs-+
cc- 0 0
43000’ o?, 0 0 / -,---r-a-r,rrr,--------
I \ 16500’ AIR- R.Q. =I. 0 --
ANOXIC
20-
10 -
COLLAPSE
0 C. D. T.
REGION OF
NORMAL NORMAL AWEOLJR,$O, ~ . - ------ ------w-w
PERFORMANCE
I \ IMPAIRED PERFORMANCE
--I- O
0
8 OO 00
SEVERE AC APN I A
\ ACAPNIC TETANY
\
0’ ’ ’ ’ ’ ’ I I I I I I\I I I\ I I I II
0 IO 20 30 40 50 60 70 80 90 100 ALVEOLAR ~02
Fig. 1. Relationship of alveolar gas composition to steadiness test performance. Ordi- nates: alveolar carbon dioxide tensions in millimeters of Hg. Abscissae: alveolar oxygen tensions in millimeters of Hg. Each type of symbol represents a probability (p) that a subject’s experimental score was not different from his control score :
The blacker the symbol the lower the probability and the greater the certainty of abnormality.
Solid circle with cross, p < 0.01; solid circle, p = 0.01 to 0.05; half solid circle, p = 0.05 to 0.1; open circle with dot, p = 0.1 to 0.5; open circle, p > 0.5.
An attempt has been made to divide the charts into regions of normal per- formance and different sorts of impaired performance. Such regions can be determined only very roughly by the data at hand, and the more uncertain regions are bounded by dotted lines. Certain tentative conclusions are indi- cated by these diagrams.

210 OTIS, RAHN, EPSTEIN AND FENN
1. Following along any given pC0, value from right to left the performance becomes worse, i.e., anoxia does not appear to antagonize acapnia.
2. Starting at a normal pCOz level of 40 mm. and following any given per cent saturation line to lower pCO:! values the performance becomes worse and never better, i.e., acapnia does not antagonize anoxia.
3. Thus acapnia and anoxia are additive or synergistic rather than antagonistic intheir effects on these performance tests.
4. On the other hand, if one starts at a normal pCOz value of 40 mm. and follows down a given altitude diagonal to lower pCOz values the performance may improve over a certain range and then grow worse. There is, therefore, an optimum value or region of values of alveola,r gas composition at each altitude for the best performance.
w- - - - - - - - d - - - - - - - - - -
REGION OF
IMPAIREO PERFORMANCE
SEVERE ACAPNIA
---- --a - -- ---
20 30 40 50 60 70 8Q 90 100 ALVEOLAR p($
Fig. 2. Relationship of alveolar gas composition to contrast discrimination test per- formance. Co-ordinates and symbols as in figure 1. In general the blacker the symbol the greater the probability that the observed performance differed significantly from normal.
It should be emphasized that these conclusions and the regions bounded on the charts are tentative. It is obvious that a much larger number of tests would be needed to establish such a diagram with certainty.
Another method of treating the data which leads to the same general conclu- sions listed above attempts, in addition, to analyze performance impairment

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR 211
into anoxic and acapnic components. Tables 1 and 2 were constructed for this purpose. For these tabulations the mean of the three trials of a test taken under a given set of conditions was taken as the score.
TABLE 1 Hand steadiness test scores as related to alveolar air compositions
\
\ PC02 45 ’ 15-24.9 25-34.9 35-50
PO2 \
pCO2 ’ pO2 Score n pCO2 pot Score SDM n pCO2 ~02 Score SDM n pCO2 pO2 Score SDM n P-P-- ----- -P-P------
<30 22.427.81812 262 529.927.9 783 228 7 30-34.9 12.433.2~2708 215.931.31917 231.333.5 779 1221537.732.7 826 147 8 35-39.9 22.137.81681 425 531.440.4 640 731137.636.6 810 200 12 40-49.9 13.442.82111 220.641.21269 331.643.2 611 1351039.943.8 328 70 16 50-75 18.3 59.4 1056 334.950.8 208 240.654.6 177 82 6 100 13.2 1150 3 19.5 480 822430.2 215 89 842.3 177 14 111
I The heading of each horizontal row indicates the range of alveolar oxygen tension in
millimeters Hg existing when the test scores entered in the row were obtained. The main headings of the vertical columns similarly indicate ranges of alveolar carbon dioxide ten- sion. The sub-headings of the columns have the following meaning.
pCO,, the average alveolar carbon dioxide tension in millimeters of Hg. ~02, the average alveolar oxygen tension. Score, the mean of all scores in a particular range. SDM, t,he standard deviation of this mean. (Calculated only when the mean was based
on 5 or more cases.) n, the number of individual scores (each individual score being the average of three
trials) on which the mean score was based.
TABLE 2 Contrast discrimination test scores as related to alveolar air composition
\ \y2
PO2 \ \
<30 30-34.9 35-39.9 40-49 * 9 50-75
100
/ <lS
pC02 1 pO2 IScore --
12.433.225.5
13.4 42.8 19.4
13.4 I I 16.5
- n
-
2
2
2
15-24.9 25-34.9
pCO2 pO2 Score SDM TZ pCO2 ~02 Score SDM n -- P -- --- --
22.4 27.8 24.3 1.17 5 29.6 27.9 16.5 1.72 8 18.9 31.3 26.2 2 31.4 33.4 15.2 1.14 16 22.137.819.9 1.93 5 31.440.4 11.7 1.76 11 20.641.218.2 3 31.643.2 5.2 1.87 9 18.3 59.4 16.1 3 34.950.8 5.7 2 20.0 12.4 1.5821 29.7 10.1 2.50 6
35-50
PC021 pOz jScoreiSDM/ n
37.7 32.4 14.0 1.69 9 37.6 36.6 14.3 1.70 12 40.3 43.7 10.4 1.10 19 40.654.610.11.41 6 42.3 6.7 .3384
The legend of table 1 applies.
Each value entered in these tables is the average of all scores obtained within the range of conditions indicated by the headings of the vertical columns and the horizontal rows. Examination of the columns of these tables indicates that, in general, performance grows worse as the alveolar oxygen tension is lowered in each of the ranges of alveolar carbon dioxide tension. A similar examination of the horizontal rows shows a tendency for performance to deteriorate as the alveolar carbon dioxide tension falls within each range of alveolar oxygen ten-

212 OTIS, RAHN, EPSTEIN AND FENN
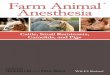
sions. This suggests the possibility of plotting performance scores against one of the independent variables and indicating the second independent variable by contour lines. . This has been attempted in figures 3 and 4 in which per- formance test scores are plotted against alveolar oxygen tensions with ranges of
3500
3000
W OI: 2500 0 0 co + 2000 CD P u) 1500 co s 5 a 1000
P cn
500
0 20 30 40 50 60 70 80 so 100
ALVEOLAR ,aO, MM. HG.
Fig. 3. Steadiness test scores as related to alveolar air composition. Based on the data shown in table 1.
Ordinates : Steadiness test scores in & second. Abscissae : Alveolar oxygen tension in millimeters of Hg. The types of symbols designate the range of alveolar carbon dioxide tensions as follows:
solid circles, < 15 mm. Hg; half solid circles, 15-24.9 mm. Hg; open circle plus center dot, 25-34.9 mm. Hg; open circles, 35-50 mm. Hg.
The vertical lines through some of the points indicate the standard deviation of the mean. Since the test trials were 30 seconds in duration, the maximum possible score would be
3600 as indicated by the horizontal line on the graph.
alveolar carbon dioxide tensions bounded by contour lines. These graphs show that with lowered oxygen tension, performance becomes worse in all ranges of carbon dioxide tensions. The slope of the lines rapidly becomes steeper as the oxygen tension falls below 40 mm. Hg.
The lowest of the family of curves in each graph is of particular interest.

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR 213
These curves may be considered as pure anoxia curves since they fit the points obtained with alveolar carbon dioxide tensions in the 35-50 mm. range which is within the normal ground level range. The points for the 25-34.9 mm. are hardly different . This confirms our previous conclusion (Fenn et al., 1946) that the alveolar carbon dioxide tension may be lowered to 25-30 mm. in the average
I I I 1 I 1 J I f
CHANCE SCORE
.-‘--‘cc . ^
20 30 40 50 60 70 80 90 100 ALVEOLAR PO2 MM. HG.
Fig. 4. Contrast discrimination test scores as related to alveolar air composition. Based on the data shown in table 2.
Ordinates : Contrast discrimination test score. The maximum possible score is 36. The score that would be obtained by chance is 31.5.
Abscissae: Alveolar oxygen tensions in millimeters of Hg. The meaning of the types of symbols is the same as for figure 3.
individual without serious impairment of performance as judged by these partic- ular tests.
The points obtained in the ranges of CO2 tensions below 25 mm. are consid- erably elevated above the pure anoxia curve. The performance impairment represented by these elevated points is due to the combined effects of anoxia and acapnia.
The data in the lowest row of tables 1 and 2 show the effect of acapnia alone on performance, because they were obtained with alveolar oxygen tensions of

214 OTIS, RAHN, EPSTEIN AND FENN
100 or above. Pure acapnia curves constructed from these data are shown in figures 5 and 6.
If the effects of anoxia and acapnia are simply additive, it should be possible to determine how much of the performance impairment represented by any point in figures 3 or 4 is due to anoxia, by subtracting the increment of score that would have been caused by the degree of acapnia existing. Accordingly the following procedure was followed with each score entered in table 2.
1. The pC0, existing when the score was obtained was noted. 2. The increment of score that this pC0, would cause was read from figure 5. 3. This increment was subtracted from the original score. 4. The corrected score was plotted against the alveolar oxygen tension.
IO I5 20 25 30 36 40 On
ALVEOLAR PC09 WY. HO.
Fig. 5 Fig. 6
Fig. 5. The effect of acapnia on contrast discrimination test performance. Plotted from the data of the last row of table 2.
Ordinates: Increments of test score above normal. Abscissae : Alveolar carbon dioxide tension in millimeters of Hg. Fig. 6. The effect of acapnia on steadiness test score. Abscissae : Alveolar carbon dioxide tension in millimeters of Hg. Ordinates: The scale on the left gives steadiness test scores as time of contact in units of
r-&v second during a 30 second test period and applies to the open circles which represent the data in the last row of table 1. The scale on the right gives steadiness test scores as number of hits during a 30 second test period and applies to the closed circles which represent the data from another series of experiments described in a previous report (Fenn et al., 1946). Those points have been plotted here to show that the two methods of scoring the steadiness test give similar results as far as acapnia is concerned.
Figure 7 shows that this procedure has resulted in fitting all the points reason- ably well to the pure anoxia curve for the contrast discrimination test. It is justifiable, therefore, to conclude that the effects of acapnia and anoxia on this type of performance are approximately additive.
In the case of the steadiness test data, however, the “corrected” scores gave a much poorer fit. Most of the points lay well above the pure anoxia curve, indicating that the correction for acapnia was inadequate. Consequently, a modified procedure was applied to each of the steadiness test scores entered in table 1.
1. The pC0, existing when the score was obtained was noted. 2. The multiple of the control score that this pC0, would give was determined
from figure 6.

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR 215
3. The original score was divided by this multiple. 4. The corrected score was plotted against the alveolar oxygen tension. The result is shown as figure 8. The fact that this method resulted in a
reasonably good fit of all the steadiness test scores to the pure anoxia curve indicates that the steadiness test score is a logarithmic rather than an arithmetic function of performance.
Fig. 7 Fig. 8
Fig. 7. The effect of anoxia on contrast discrimination test score. Ordinates : Contrast discrimination test scores. Abscissae : Alveolar oxygen tensions in millimeters of Hg. Open circles: Scores obtained with alveolar carbon dioxide tensions between 35-50
mm. Hg. Closed circles: Scores obtained with alveolar carbon dioxide tensions below 35 mm. but
corrected for the effects of acapnia by the method described in the text. Fig. 8. The effect of anoxia on steadiness test scores. Ordinates : Steadiness test scores as time of contact in units of &J second during a 30
second test period. Abscissae : Alveolar oxygen tensions in millimeters of Hg. Open circles : Scores obtained with alveolar carbon dioxide tensions in the range of 35-50
mm. Hg. Closed circles: Scores obtained with alveolar carbon dioxide tensions below 35 mm. but
corrected for acapnia by the method described in the text.
Having separated the effects of acapnia and anoxia and having determined the nature of their combined action on the test scores, it is possible to determine a theoretical score for any combination of alveolar oxygen and carbon dioxide tensions, or to construct isopleths of constant score on a pCOz-~02 grid as has been done in figures 9 and 10. Such lines were constructed as follows:
1. The desired score was chosen. 2. Reference to the pure acapnia curve established the right hand end of the line (at
PO2 = 100 mm.). 3. Reference to the pure anoxia curve established the left hand end of the line (at
pco2= 40 mm.). 4. Intermediate points were established by choosing an oxygen tension, determining from
the pure anoxia curve what score would be obtained at this tension, and then determining from the pure acapnia curve what the pCO2 would have to be to give an increment (in the case of the contrast discrimination test) or a multiple (in the case of the steadiness test) that would yield the arbitrarily chosen score when added to or multiplied by the pure anoxia

216 OTIS, RAHN, EPSTEIN AND FENN
Fig. 9. The relationship of contrast discrimination test scores to alveolar air composition and equivalent altitude.
Ordinates : Alveolar carbon dioxide tensions in millimeters of Hg. Abscissae : Alveolar oxygen tensions in millimeters of Hg. Curved lines are isopleths of constant score constructed by the method described in the
text. Diagonals represent the equivalent altitudes indicated for breathing oxygen and for air
when the R.Q. = 1.
ALVEOLAR PO2 MM. HG.
Fig. 10 Fig. 11
Fig. 10. The relationship of steadiness test scores to alveolar air composition and equiv- alent altitude.
Ordinates : Alveolar carbon dioxide tensions in millimeters of Hg. Abscissae: Alveolar oxygen tensions in millimeters of Hg. Curved lines are isopleths of constant score constructed by the method described in the
text. Diagonals represent the equivalent altitudes indicated for breathing oxygen and for
air when the R. Q. = 1. Fig. 11. Heart rate increase as a function of alveolar oxygen tension. Plotted from the
data in the last main column of table 3. Ordinates: Increase in heart rate above the control rate in beats per minute. Abscissae : Alveolar oxygen tensions in millimeters of Hg. The vertical lines through the points indicate the standard deviation of the mean.
By constructing an altitude diagonal which is tangent to an isopleth, the optimal alveolar air composition for this altitude is established by the co-or- dinates of the point of tangency. When oxygen is breathed only one altitude

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR 217
diagonal can be drawn tangent to a given isopleth. If air is the inspired gas, however, a multitude of such lines can be drawn, because of the R.Q. effect. The diagonals drawn in figures 9 and 10 represent air breathing altitudes if the R.Q. is equal to 1, or oxygen breathing altitudes at any R.Q.
That the two tests employed have different optimums is obvious from a comparison of figures 9 and IO. At the altitude of 47,090 feet, for example, the optimum pCO2 for the steadiness test is 27 mm., but for the contrast dis- crimination test it is at 18 mm. These values should not be taken too seriously as far as their absolute magnitudes are concerned, but it seems fair to draw the conclusion that a degree of hyperventilation greater than the normal for the average individual at altitude will not improve his steadiness test score but will
TABLE 3 Heart rate change as related to alveolar air composition
PC02
\ PO2
<30 3034.9 35-39.9 40-49.9 50-75
100
<15
pCO2 ~02 Rate ---
12.4 33.2 $19.5
13.4 42.8 $13.0
12.6 -3.0
15-24.9 25-34.9 35-50 ALL
- PZ pCO2 ~02 Rate TZ _----
22.4 27.8 $21.4 5 2 18.9 31.3 $22.5 2
21.7 37.4 $12.0 4 2 20.6 41.2 $7.0 3
18.3 59.4 34.5 3 2 20.2 -0.8 20
PC02 PO2 Rate n -
8 15 10 9 2 7
PC02 PO2 I SDM
29.6 31.1 31.5 31.9 34.9 30.6
27.9 32.5 40.7 43.1 50.8
$18.6 $17.5 $15.3 $11.8
$6.0 $1.1
37.7 37.8 41.1 41.3 42.3
32.4 36.7 44.3 54.1
Rate /ilpOl/ Rate 1
27.9 $19.4 $19.2 9 32.4 $18.5 $16.3 11 38.4 $15.2 $4.3 15 43.5 $7.5 38.8 555.0 36.5 $1.2 26 $0.4
1.53 1.51 2.33 1.67 1.98 0.95
The heading of each horizontal row indicates the range of alveolar oxygen tension in millimeters of Hg existing when the heart rate measurements were obtained. The main headings of the vertical columns similarly indicate ranges of alveolar carbon dioxide tension. The sub-headings of the columns have the following meamngs.
pCO2, the average alveolar carbon dioxide tension in millimeters of Hg. ~02, the average alveolar oxygen tension. Rate, the mean change with respect t,o normal of all heart rates measured in the indicated range. n, the number of determinations (each determination being the average of three measurements) on which the
mean change in heart rate was based. The last main column is a summation of results for all ranges of carbon dioxide tensions. The sub-heading, SD&I,
in this column refers to standard deviation of the mean.
improve his contrast discrimination test score. There is an optIimum alveolar pCO2 at each altitude for a given type of performance, but the optimum for another type of performance is likely to be different.
The conclusion that one should not hyperventilate below a pC0, level of 27 mm. at 47000 feet is borne out by a series of flights which we have made to 30000 and 46000 feet Measurements. were made of the alveolar pCO2 level and the hand steadiness by the test described. Data are available on 4 subjects at each altitude. At 460b0 feet the steadiness begins to decrease below 25 or 28 mm. Hg pC0, in spite of the concomitant increase of ~0,. Furthermore, for the same pCOz level, the hand is always more unsteady at the higher altitude than at 30000 ft. and is more unsteady at 46000 ft. at any pC0, level t,han at ground level breathing normally. These results also confirm therefore the idea that anoxia and acapnia are additive in their effects.
Relationship of heart rate to alveolar gas tensions. Table 3 shows the mean change in heart rate obtained in various ranges of alveolar oxygen and carbon

218 OTIS, RAHN, EPSTEIN AND FENN
dioxide tensions. The results show that heart rate is definitely related to alveolar oxygen tension, but is not significantly changed by alterations in the carbon dioxide tension over the limits investigated. Consequently, heart rate increments for all ranges of carbon dioxide tensions within each range of oxygen tension have been averaged as indicated in the extreme right hand column of the table. These values are shown plotted against the alveolar oxygen tension in figure 11.
TABLE 4
Summary of experiments in which subjects breathed naturally
ALT.
ALft.
G.L. 12 16 18 20 22
18 19 7
18 4 2
pco2 PO2 R.Q.
mm.Hg
38.1 39.8 33.8 33.7 31.9 29.2
9?ZVLHg
47.1 0.88 22 40.8 0.94 28 34.0 0.94 22 34.0 1.12 19 27.9 1.00 23
min.
S.T.
147 157 455 495
1070
C.D.T. H.R.
6.7 0 10.0 +5.1 12.6 +15.5 13.8 +15.1 17.8 +20.0 21.9 +lS.O
SAT.
#et- cent
81 78 69 71 64
The column headings have the following meanings: Alt ., simulated altitude in thousands of feet. n, the number of experiments performed. pCO,, the alveolar carbon dioxide tension in millimeters of Hg. ~02, the alveolar oxygen tension in millimeters of Hg. R.Q., the respiratory quotient as calculated from the alveolar oxygen and carbon dioxide
tensions. Time, the time in minutes which had been spent at altitude when the alveolar sample
was taken. S.T., steadiness test score. C .D .T., contrast discrimination test score. H.R., change in heart rate with respect to normal. y0 Sat., the per-cent saturation of arterial blood as est,imated from the alveolar oxygen
and carbon dioxide tensions with the aid of Henderson’s nomogram. G. L., ground level.
In so far as heart rate increment is a criterion of added circulatory strain, these results indicate that although anoxia may act as a considerable stress acapnia does not.
Variations in performance, alveolar gas composition, and heart rate with altitude. Some of the experiments described above were performed with the subject breathing naturally from the demand regulator. The number of such runs at some of the altitudes is small, but it seems worth while to summarize the results briefly, because they indicate what individuals will do at air breathing altitudes when left to their own resources.
Table 4 shows the mean values obtained at each altitude for the various quanti- ties measured or calculated, and figure 12 shows the same results in graphic form. The values for per cent saturation are estimated from the alveolar oxygen and carbon dioxide tensions, and are not oximeter readings. As mentioned above the behavior of our oximeter was unsatisfactory during this series of flights.

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR 219
40
30
ALVEOLAR pC02
I2 16 ALTITUDE IN THOUSANDS OF FEET
I8
Fig. 12. The normal response of individuals to altitude. Graphic representation of the data in table 4. The vertical lines through some of the points indicate the standard devi- ation of the mean values represented by the points.
The values shown for alveolar air composition, in general, are in good agree- ment with the much more extensive series of Boothby. (See Helmholz et al., 1944.) Our data fail to show any lowering of the pCOft at the 12,000 foot altitude,

220 OTIS, RAHN, EPSTEIN AND FENN
but this may be due to the fact that the ground level values and the altitude values were not necessarily obtained on the same subjects on the same day.
The 12,000 foot altitude shows a small but significant effect on the contrast discrimination test and on heart rate, but leaves the steadiness test score un- changed from the ground level value. The higher altitudes show progressively greater effects on all items measured, with performance deteriorating very rapidly above 18,000 feet. The highest altitude studied, 22,000 feet, is probably close to the maximum at which most unacclimatized individuals will maintain con- sciousness for a half hour period. Similar effects of altitude have been described by McFarland (1938), who used choice reaction time, a color naming test, a code test, and a memory test as criteria of performance. He found that the mean impairment of performance was not statistically significant at altitudes below 12,000 feet.
The question may be asked as to whether the effect of altitude on the perform- ante of individuals breathing n aturally is purely an anoxic effect or whether the hyperventilation which normally accompanies 12,000 feet produces significant acapnic effects.
the anoxia at altitudes above A comparison of the results
shown in figure 12 with the pure anoxia curves in figures 7 and 8 indicates that the performance impairment of altitude is essentially a matter of anoxia alone. The fact that the alveolar pCOz drops below 30 mm. only at the highest altitude, 22,000 feet, (and only slightly below even at this altitude) would also indicate, on the basis of the pure acapnia curves, that acapnia could be, at most, only a very small factor. It is probable, of course, that a few, relatively rare individuals may spontaneously but the large majori
hyperventilate enough to experience acapnic impai rment, .ty will suffer only from anoxia when t’heir breathing is guided
by their own reflexes at air breathing altitudes. We wish to acknowledge the kindness of Mr. John H. Slough, President of
the General Electric X-Ray Corporation, who placed the pneumolator at our disposal. We are grateful also to Dr. Selig He&t for providing us with the c contrast discrimination test used in t,hese studies.
It is a pleasure also to offer our thanks to the many subjects who have faith- fully and willingly served in these experiments, particularly Mary &dge, Flo- rence Neiman, M. I3rontman and four members of C.P.S. ITnit &. 115, T. IIor- vath, H. Mitchell, J. Heil, and A. Culp.
SUMMARY
1. Performance (contrast discrimination test and steadiness test) and heart rates of I1 subjects were measured over a wide range of alveolar oxygen and carbon dioxide tensions. A total of 171 half-hour experiments and 85 control runs were made.
2. The results are plotted on an alveolar pCO,-~0, grid, and regions of normal performance and of various kinds of impaired performance are indicated.
3. A method for analyzing performance impairment into anosic and acapnic coniponentls is described.
4. The results indicate the following conclusions :

PERFORMANCE AS RELATED TO COMPOSITION OF ALVEOLAR AIR 221
a. Acapnia and anoxia are additive rather than antagonistic in their effects on performance.
b. There exists at each altitude an optimum alveolar gas composition for best performance.
c. This optimum may be different for different types of performance. d. Heart rate is increased by anoxia, but is not consistently affected
by acapnia. e. Performance impairment in most individuals breathing naturally at air-
breathing altitudes is essentially a matter of anoxia alone.
REFERENCES
RAHN, H., A. B. OTIS, M. A. EPSTEIN, M. HODGE, S. W. HUNTER AND W. 0. FENN. J. Aviation Med. (In press.)
HENDERSON, L. J. Blood. Yale University Press, New Haven, 1928. MCFARLAND, R. Report no. 13. Dept. of Commerce, Bureau of Air Commerce, Safetyand
Planning Division, May 1938. HELMHOLZ, H. F., J. B. BATEMAN AND W. M. BOOTHBY. J. Aviation Medicine 16: 366,194.