Embed Size (px)
Citation preview

CASE REPORT
Percutaneous Treatment of an Infected Aneurysmal SacSecondary to Aortoesophageal Fistula with a Historyof Stent-Graft Treatment for Thoracic Aortic Aneurysm
Furuzan Numan • Fatih Gulsen • Murat Cantasdemir •
Serdar Solak • Harun Arbatli
Received: 19 May 2011 / Accepted: 29 July 2011 / Published online: 19 August 2011
� Springer Science+Business Media, LLC and the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) 2011
Abstract A 68-year-old man who was subjected to stent-
grafting of a descending thoracic aortic aneurysm (TAA)
4 months previously was admitted to our hospital with
constitutional symptoms, including high fever, sweating,
nausea, vomiting, weight loss, and backache. An infected
aneurysmal sac was suspected based on computed tomog-
raphy (CT) findings, and an aortoesophageal fistula (AEF)
was identified during esophagoscopy. CT-guided aspiration
was performed using a 20-G Chiba needle, confirming the
presence of infection. For treatment of the infected aneu-
rysmal sac, CT-guided percutaneous catheter drainage in a
prone position was performed under general anesthesia
with left endobronchial intubation. Drainage catheter
insertion was successfully performed using the Seldinger
technique, which is not a standard treatment of an infected
aneurysmal sac. Improvement in the patient’s clinical
condition was observed at follow-ups, and CT showed total
regression of the collection in the aneurysmal sac.
Keywords Thoracic endovascular aortic repair �Aortoesophageal fistula � Infected aneurysmal sac �Percutaneous drainage
Introduction
Aortoesophageal fistula (AEF) is a rare clinical condition
associated with high morbidity and mortality rates and a
fatal outcome if treated surgically or medically; limited
treatment alternatives exist. Thoracic aortic aneurysms
(TAA) are the most frequent primary cause of AEF and are
responsible for two-thirds of all AEF cases [1]. Other
causes of primary AEF include ulcerated plaques of the
thoracic aorta, esophageal neoplasms, and drinking corro-
sive materials [2, 3]. Uncommon cases of AEF secondary
to endoscopic or operative esophageal procedures and
endoluminal stent-grafting also have been reported [4].
AEF secondary to prosthetic graft replacement of the tho-
racic aorta is a rare but frequently catastrophic complica-
tion. Other than occurring as a communication between the
aorta and esophagus, AEF secondary to prosthetic graft
replacement may occur as an esophagoparaprosthetic fis-
tula [5]. True AEF, which occurs as a direct communica-
tion between the aorta and esophagus, is usually
characterized by massive, fatally progressing upper gas-
trointestinal bleeding, has high mortality rates, and is more
commonly identified by postmortem examination. AEF
between the esophagus and aneurysmal sac adjacent to an
endovascular stent-graft of the thoracic aorta may occur
secondary to sepsis when the fistula reaches the proximal
or distal aspect of the stent-graft, with the presence of an
endoleak inside the aneurysmal sac, or with graft infection.
In this case report, AEF between the esophagus and
thrombosed aneurysmal sac adjacent to a stent-graft of the
thoracic aorta developed in the late period after thoracic
endovascular aortic repair (TEVAR). We present a case of
an infected aneurysmal sac related to AEF that developed
after TEVAR and its treatment by computed tomography
(CT)-guided insertion of a drainage catheter.
F. Numan (&) � F. Gulsen � M. Cantasdemir � S. Solak
Department of Interventional Radiology, Cerrahpasa Faculty
of Medicine, Istanbul University, Fatih, Istanbul 34098, Turkey
e-mail: [email protected]
H. Arbatli
Department of Cardiovascular Surgery, Faculty of Medicine,
Maltepe University, Istanbul, Turkey
123
Cardiovasc Intervent Radiol (2012) 35:690–694
DOI 10.1007/s00270-011-0256-1
Case Report
A 68-year-old man with a history of hypertension, hyper-
cholesterolemia, heavy smoking, and chronic renal failure
underwent surgery in our hospital for an abdominal aortic
aneurysm 4 years prior and was subjected to stent-grafting
of a descending TAA 4 months prior. After TEVAR, dur-
ing the follow-up period, both clinical and radiological
course was uneventful until he was admitted to our hospital
for constitutional symptoms, including weight loss in the
previous 2 months and nausea, vomiting, backache, and
high fever that had developed in the previous 2 weeks. On
physical examination, a generally poor condition, dehy-
dration, and cachexia were noted. Blood pressure was
within normal limits. Clinical analysis reported a white
blood cell count of 24,300/ml and C-reactive proteins at
86.4 mg/dl. The fever persisted despite treatment with a
broad-spectrum antibiotic. Chest radiography revealed
no source of infection. A contrast-enhanced CT was plan-
ned but due to preexisting chronic renal insufficiency,
contrast-enhanced CT was contraindicated by consultant
nephrologist.
CT examination showed the presence of a collection
with a size of 4- 9 8-cm containing air bubbles around the
aortic stent-graft, which was a sign of possible infection of
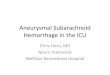
the aneurysmal sac (Fig. 1). Subsequent esophagogastros-
copy and esophagography examinations revealed a small
fistula between the TAA and mid-third esophagus (Figs. 2,
3A). A swallow study revealed contrast extending into the
aneurysmal sac around the endograft. Because of there
were no signs of bleeding in esophagogastroscopy exami-
nation, presence of an endoleak was not considered.
However, due to history of chronic renal failure in our
patient, contrast-enhanced CT examination was not per-
formed. There were no imaging finding that could explain
the inflammatory symptoms and laboratory findings, except
the collection around the aortic stent-graft. A prediagnosis
of abscess around the aortic stent-graft was made depending
on a combination of clinical, laboratory, and imaging find-
ings. For empirical antibiotherapy, cefazolin was admin-
istered (3 9 1 g) by intravenous injection for 2 weeks.
Because there was no improvement in the patient’s clinical
status, to confirm the presence of an abscess and identify the
microbiological agent, percutaneous diagnostic aspiration
and drainage was planned.
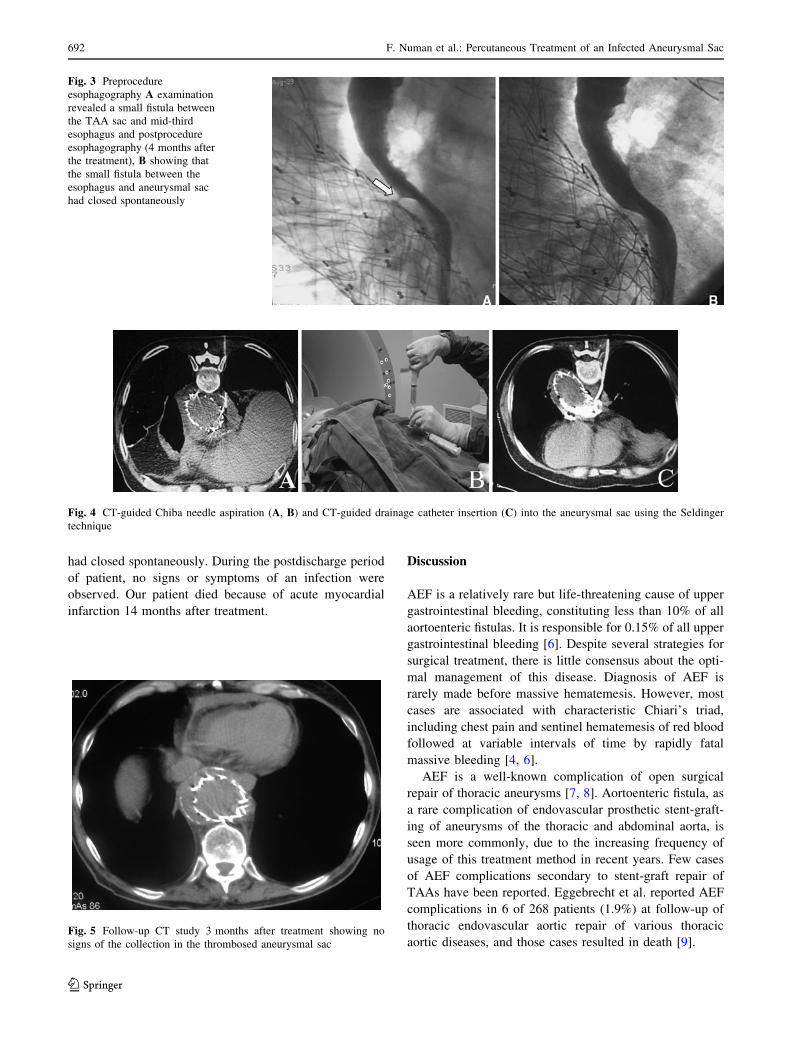
The patient was placed in the prone position and
underwent general anesthesia with endobronchial intuba-
tion. A 20-G Chiba needle was inserted into the aneurysmal
sac via a posterior approach under CT guidance (Fig. 4A).
A purulent collection by needle aspiration confirmed
infection of the aneurysmal sac adjacent to the aortic stent-
graft (Fig. 4B), and CT-guided drainage catheter insertion
into the aneurysmal sac by the Seldinger method was
performed (Fig. 4C). Approximately 210 ml of infected
fluid was drained via the catheter during 7 days.
Cultures of the aortic sac fluid later grew Staphylococcus
aureus and specific intravenous antibiotherapy (ciprofloxa-
cin and sultamicillin) was started. At 7 days postdrainage,
catheter output had decreased to less than 10 ml/24 h during
the preceding 2 days, and the patient remained afebrile.
Because a follow-up CT study showed total regression of the
collection in the aneurysmal sac and the patient’s clinic
condition had improved, the drainage catheter was removed
1 week after the procedure. The subsequent postprocedure
course was uneventful, and the patient was discharged in
good condition.
The follow-up CT study 3 months after treatment
revealed no signs of the collection in the thrombosed
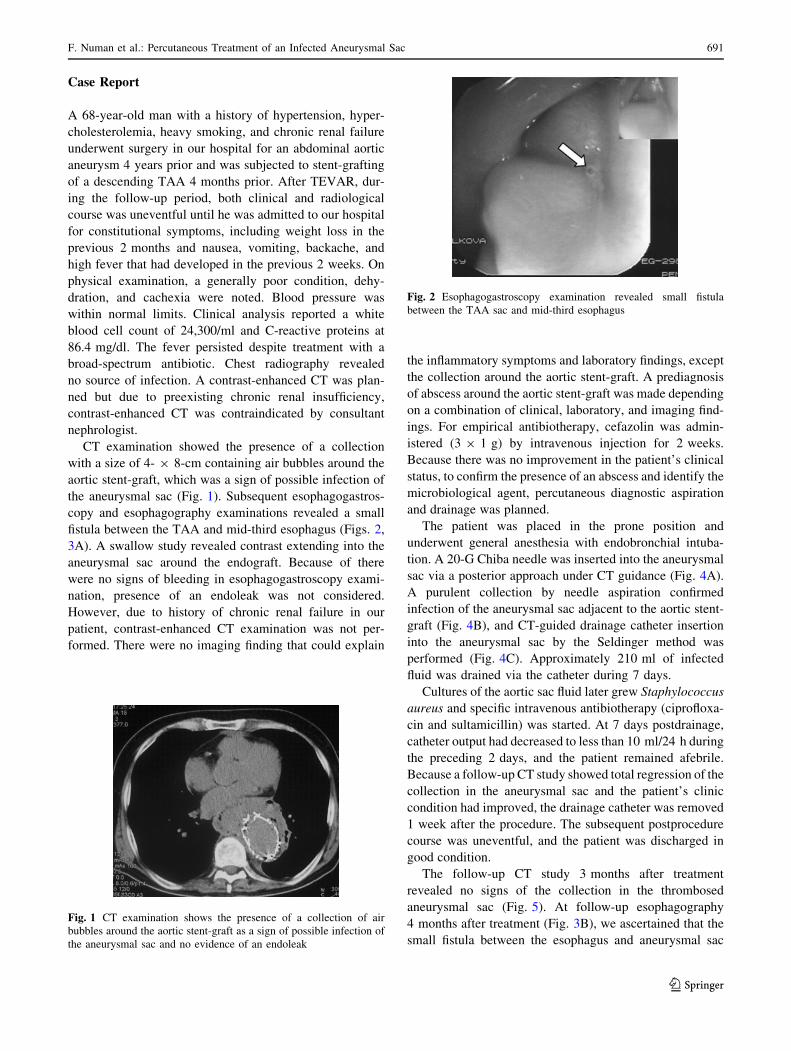
aneurysmal sac (Fig. 5). At follow-up esophagography
4 months after treatment (Fig. 3B), we ascertained that the
small fistula between the esophagus and aneurysmal sac
Fig. 1 CT examination shows the presence of a collection of air
bubbles around the aortic stent-graft as a sign of possible infection of
the aneurysmal sac and no evidence of an endoleak
Fig. 2 Esophagogastroscopy examination revealed small fistula
between the TAA sac and mid-third esophagus
F. Numan et al.: Percutaneous Treatment of an Infected Aneurysmal Sac 691
123
had closed spontaneously. During the postdischarge period
of patient, no signs or symptoms of an infection were
observed. Our patient died because of acute myocardial
infarction 14 months after treatment.
Discussion
AEF is a relatively rare but life-threatening cause of upper
gastrointestinal bleeding, constituting less than 10% of all
aortoenteric fistulas. It is responsible for 0.15% of all upper
gastrointestinal bleeding [6]. Despite several strategies for
surgical treatment, there is little consensus about the opti-
mal management of this disease. Diagnosis of AEF is
rarely made before massive hematemesis. However, most
cases are associated with characteristic Chiari’s triad,
including chest pain and sentinel hematemesis of red blood
followed at variable intervals of time by rapidly fatal
massive bleeding [4, 6].
AEF is a well-known complication of open surgical
repair of thoracic aneurysms [7, 8]. Aortoenteric fistula, as
a rare complication of endovascular prosthetic stent-graft-
ing of aneurysms of the thoracic and abdominal aorta, is
seen more commonly, due to the increasing frequency of
usage of this treatment method in recent years. Few cases
of AEF complications secondary to stent-graft repair of
TAAs have been reported. Eggebrecht et al. reported AEF
complications in 6 of 268 patients (1.9%) at follow-up of
thoracic endovascular aortic repair of various thoracic
aortic diseases, and those cases resulted in death [9].
Fig. 3 Preprocedure
esophagography A examination
revealed a small fistula between
the TAA sac and mid-third
esophagus and postprocedure
esophagography (4 months after
the treatment), B showing that
the small fistula between the
esophagus and aneurysmal sac
had closed spontaneously
Fig. 4 CT-guided Chiba needle aspiration (A, B) and CT-guided drainage catheter insertion (C) into the aneurysmal sac using the Seldinger
technique
Fig. 5 Follow-up CT study 3 months after treatment showing no
signs of the collection in the thrombosed aneurysmal sac
692 F. Numan et al.: Percutaneous Treatment of an Infected Aneurysmal Sac
123

Mechanic and infective factors are disputably thought to
play roles in the development of aortoenteric fistulas,
secondary to surgical aortic repair. These factors include
rupture of abscesses of graft infections into the intestine
and erosion of structures adjacent to the prosthetic material
due to pulsation and pseudoaneurysm development on the
anastomosis line. In cases of aortoesophageal fistula fol-
lowing endovascular repair, Hance et al. suggested that
fistulas may arise secondary to (1) the development of
pseudoaneurysm, (2) endoleak into the residual aneurysmal
sac, or (3) erosion of the stent-graft through the aorta [10].
Eggebrecht et al. stated that AEF formation may be related
to pseudoaneurysm because they found periaortic hema-
toma in two of three AEF cases secondary to TEVAR [8].
Other important factors that play roles in AEF development
include the occlusion of esophageal arteries originating
from the thoracic aorta after stent-grafting and esophageal
erosions related to these occlusions. Collateral weakness of
the middle part of the esophagus, as opposed to the cervical
and distal portions, is thought to be related to the frequency
of AEF secondary to TEVAR in this segment.
However, hypotheses about mechanisms of fistulization
remain highly speculative. Some authors claim that a pri-
mary infection of the endograft due to contamination may
evolve into an aortic wall abscess with subsequent drainage
in to the esophagus or gastrointestinal system. This
mechanism implies a graft contamination during implan-
tation, maybe secondary to iatrogenic maneuvers, as a
result of bacteremia, or even due to migration of micro-
organism from the aortic mural thrombus [11]. Also, in
case of contained ruptured aneurysms, chronic inflamma-
tion due to the reabsorption of the posterior mediastinal
hematoma may represent another potential mechanism of
fistulization [12].
AEF secondary to TEVAR could occur as a direct
communication between the thoracic aorta and esophagus
or between the esophagus and aneurysmal sac adjacent to
the stent-graft. The clinical presentation of the patient is
highly associated with the type of AEF. The case may
present itself as massive upper gastrointestinal bleeding
when the esophagus directly communicates with the aorta
or aneurysmal sac with an existing endoleak, or, as in our
case, as an infection when the esophagus communicates
with a completely thrombosed aneurysmal sac.
There is no consensus in the literature about which
should be the optimal antimicrobial therapy for infected
aneurysmal sac or for how long it should be administrated.
Generally, it is given intravenously at the maximal toler-
ated dosage for at least the initial 4–6 weeks and followed
by a sequential oral regimen once the acute phase of the
infection has subsided. In cases when surgery is not per-
formed because of an excessive risk from the procedure, it
seems prudent to continue with an oral regimen indefinitely
[13]. However, most stent-graft infections were identified
causative microorganisms that are highly virulent patho-
gens, such as methicillin-resistant Staphylococcus aureus,
Streptococcus spp., or gram-negative species, such as
Pseudomonas and Klebsiella [14]. Control of sepsis in
these cases could not be achieved even with optimal anti-
biotic therapy, and the need for an adjunct therapy should
be evaluated.
Most authorities agree that an infected stent graft should
be removed if a patient’s condition permits. Patients with
aortic aneurysms often have multiple existing comorbidi-
ties, including coronary artery disease, cerebral vascular
disease, and hypertension. All of these factors may preclude
a patient from being a desirable surgical candidate. High-
risk patients have been reported to survive with conservative
treatment consisting of antimicrobial therapy and percuta-
neous drainage [15]. However, the clinical outcome of
conservative treatment is poor and this option should be
reserved for selected patients such as patients with a nonb-
leeding AEF, who has comorbidities or poor general con-
ditions. Also conservative treatment with appropriate
antibiotics and percutaneous drainage in patients with sepsis
secondary to nonbleeding AEF can promote the reduction of
sepsis and decrease the perioperative morbidity in case of
a subsequent surgical treatment for the closure of the
fistula [16].
As a surgical option, left thoracotomy with subsequent
aortic graft replacement and esophageal fistula resection
may be appropriate AEF therapy [3, 7]. Temporary or
permanent extra-anatomic bypass can be performed in the
presence of no active bleeding. However, mediastinitis,
sepsis, and bleeding are common complications after sur-
gical treatment of AEF, and this treatment option has high
morbidity and mortality rates [17]. Recently, stent-graft
placement has been successfully used to treat secondary
AEF after surgery.
There are few reports of AEF complications of TAA
after stent-graft repair in the literature but, as we know,
AEF without direct aortic communication between the
esophagus and a completely thrombosed aneurysmal sac,
which is successfully treated conservatively, has not been
reported. We believe that, as in our case, to impede sepsis
occurrence, draining infected material with a drainage
catheter in aneurysmal sacs secondary to fistula is an
effective, inexpensive, and feasible treatment option. We
should keep in mind that draining infected collections in
this way may hinder extension of the fistula tract to distal
or proximal ends of the stent-graft. In our case, the small
fistula had closed spontaneously, but in case of persistence
of the fistula, esophageal cover stents can be considered as
a treatment option for the closure of the fistula tract.
However, cover stents will not provide sufficient thera-
peutic effect on collection.
F. Numan et al.: Percutaneous Treatment of an Infected Aneurysmal Sac 693
123

Various complications, such as pneumothorax, catheter-
related pain, and of utmost importance—in case of pres-
ence of an endoleak or rupture of stent-graft—massive
bleeding can occur during or after the procedure. In our
case, left endobronchial intubation was performed and
contralateral lung was deflated to prevent pneumothorax.
Also, because of possible catastrophic results, this kind of
procedure should be planned thoroughly before the inter-
vention and performed in a step-by-step manner. Because
of this, at first the presence of abscess was confirmed by
percutaneous aspiration with 20-G Chiba needle and then
after confirmation of a purulent material drainage catheter
was inserted into the aneurysmal sac by the Seldinger
method. At the postprocedure period, the possibility of
massive bleeding should not be neglected and the patient
should be followed up closely. A major drawback in our
case was the inability to perform a contrast-enhanced CT
because of our patient’s chronic renal failure. It should not
be forgotten that it is essential to confirm the absence of an
endoleak and demonstrate the abscess or retention by using
contrast-enhanced CT in patients who have suitable med-
ical conditions.
As a result, the probability of AEF complications should
be kept in mind. In patients with infected aneurysmal sacs
secondary to fistula between a completely thrombosed
aneurysmal sac and the esophagus, without direct aortic
communication, we think that the method we used in this
case could contribute to hindering the extension of the
fistula tract to the aorta and subsequent probable sepsis and
could be a life-saving treatment option. However, this
technique should be reserved for selected patients who are
not responding to aggressive antibiotic regimens, as a bail-
out option for those unfit for intervention, or as an adjunct
during optimization for those awaiting definitive treatment.
Conflict of interest The authors declare that they have no conflict
of interest.
References
1. Flores J, Shiiya N, Kunihara T et al (2004) Aortoesophageal
fistula: alternatives of treatment case report and literature review.
Ann Thorac Cardiovasc Surg 10(4):241–246
2. Hollander JE, Quick G (1991) Aortoesophageal fistula: a com-
prehensive review of the literature. Am J Med 91:279–287
3. Amin S, Luketich J, Wald A (1998) Aortoesophageal fistula: case
report and review of the literature. Dig Dis Sci 43:1665–1671
4. Lin CS, Tung CF, Yeh HZ et al (2008) Aortoesophageal fistula
with a history of graft treatment for thoracic aortic aneurysm.
J Chin Med Assoc 71(2):100–102
5. Kieffer E, Chiche L, Gomes D (2003) Aortoesophageal fistula:
value of in situ aortic allograft replacement. Ann Surg 238(2):
283–290
6. Takano S, Katsuhara K, Nobuhara K et al (2009) Aortoesopha-
geal fistula due to esophageal ulcer. Gen Thorac Cardiovasc Surg
57(5):255–257
7. Isasti G, Gomez-Doblas JJ, Olalla E (2009) Aortoesophageal
fistula: an uncommon complication after stent-graft repair of an
aortic thoracic aneurysm. Interact Cardiovasc Thorac Surg
9(4):683–684
8. Eggebrecht H, Baumgart D, Radecke K et al (2004) Aorto-
esophageal fistula secondary to stent-graft repair of the thoracic
aorta. J Endovasc Ther 11(2):161–167
9. Eggebrecht H, Mehta RH, Dechene A et al (2009) Aortoesoph-
ageal fistula after thoracic aortic stent-graft placement: a rare but
catastrophic complication of a novel emerging technique. JACC
Cardiovasc Interv 2(6):570–576
10. Hance KA, Hsu J, Eskew T et al (2003) Secondary aortoesoph-
ageal fistula after endoluminal exclusion because of thoracic
aortic transection. J Vasc Surg 37(4):886–888
11. Martens K, De Mey J, Everaert H et al (2007) Aortoesophageal
fistula following endovascular exclusion of a thoracic aneurysm.
Int Angiol 26(3):292–296
12. Czerny M, Zimpfer D, Fleck T et al (2005) Successful treatment
of an aortoesophageal fistula after emergency endovascular tho-
racic aortic stent-graft placement. Ann Thorac Surg 80(3):
1117–1120
13. Chiesa R, Tshomba Y, Kahlberg A et al (2010) Management of
thoracic endograft infection. J Cardiovasc Surg 51(1):15–31
14. Perera GB, Fujitani RM, Kubaska SM (2006) Aortic graft
infection: update on management and treatment options. Vasc
Endovascular Surg 40(1):1–10
15. Saleem BR, Berger P, Zeebregts CJ et al (2008) Periaortic en-
dograft infection due to Listeria monocytogenes treated with graft
preservation. J Vasc Surg 47:635–637
16. Belair M, Soulez G, Oliva V et al (1998) Aortic graft infection: the
value of percutaneous drainage. AJR Am J Roentgenol 171(1):
119–124
17. Iguchi A, Miyazaki S, Akimoto H et al (2001) Successful man-
agement of secondary aortoesophageal fistula with graft infec-
tion. Thorac Cardiovasc Surg 49(2):126–128
694 F. Numan et al.: Percutaneous Treatment of an Infected Aneurysmal Sac
123