Embed Size (px)
Citation preview

Percutaneous Revascularization of SubclavianArtery Chronic Occlusion With Dual Cerebral
Artery Protection
Nehal Shah, MBBS, Lisa M. Nee, MD, and Amish N. Raval,* MD
Percutaneous intervention for symptomatic subclavian artery chronic occlusion is anoccasionally performed, minimally invasive alternative to surgical bypass. Potential com-plications include stroke, perforation, and recanalization failure.We discuss a case of suc-cessful percutaneous revascularization of symptomatic subclavian artery chronic occlu-sion using coronary devices and dual cerebral embolic protection. ' 2008Wiley-Liss, Inc.
Key words: angioplasty; atherosclerosis; embolism; filter; stent; claudication; stroke
INTRODUCTION
Patients with obstructive subclavian artery atheroscle-rosis may present with upper extremity claudication,syncope, vertigo due to subclavian steal syndrome, armcoolness, or digital emboli [1]. While percutaneousintervention for subclavian artery stenosis is widely per-formed, there is relatively little experience with percuta-neous revascularization for subclavian artery chronictotal occlusion (CTO). Potential risks include stroke,perforation, and recanalization failure. We present acase of symptomatic subclavian artery CTO success-fully treated percutaneously, using coronary devices anddual cerebral artery embolic protection.
CASE REPORT
A 48-year-old woman presented with progressive,disabling right arm and shoulder claudication for 1year. Risk factors included hypertension, dyslipidemia,diabetes mellitus, and tobacco abuse. Right arm pulseswere absent and noninvasive blood pressure wasimmeasurable. CT angiography revealed right subcla-vian artery occlusion proximal to the right vertebral ar-tery. The left vertebral artery did not appear enlargedcompared to the right vertebral artery. Selective bra-chiocephalic angiography demonstrated flush occlusionof the ostial right subclavian artery with distal recon-stitution via thyroid artery collaterals which convergedto flow retrograde to the right thyrocervical artery(Fig. 1). This resulted in antegrade flow in the rightvertebral artery. Treatment options including surgicalcarotid-subclavian bypass were presented; however, thepatient opted for percutaneous revascularization.A 6F, 45 cm long Pinnacle Destination Sheath
(Terumo Medical, Somerset, NJ) and a 7F, 100 cm
long Shuttle Sheath (Cook, Bloomington, IN) wereintroduced from the right brachial artery and femoralartery, respectively. Heparin was administered to main-tain ACT near 250 sec. A pressure gradient of 50 mmHg was measured across the occlusion. 4 mm and7 mm SpiderFX1 (eV3, Plymouth, MN) embolic pro-tection devices were placed in the right vertebral andright common carotid arteries, respectively (Fig. 2).The subclavian artery occlusion was initially crossedfrom the right brachial sheath with a 0.01400 ASAHIMiracleBros 6 (Abbott Vascular, Santa Fe, CA) coro-nary wire with a 2.0 mm Voyager (Cordis Endovascu-lar, Miami Lakes, FL) balloon catheter for support.After the occlusion was successfully traversed, angio-plasty was performed with a 4.0 mm OPTA Proballoon (Cordis Endovascular, Miami Lakes, FL). Briskantegrade flow was re-established in the subclavianartery; however, significant radiolucency consistentwith trapped bulky atheroemboli was now visualizedin the right carotid artery filter (Fig. 3). Despite this,carotid artery flow was not compromised. The right
Division of Cardiovascular Medicine, Department of Medicine,University of Wisconsin School of Medicine and Public Health,Madison, Wisconsin
*Correspondence to: Amish N. Raval, MD, FRCPC, Assistant Pro-
fessor of Medicine, Division of Cardiovascular Medicine, University
of Wisconsin School of Medicine and Public Health, H6/321 Clini-
cal Sciences Center, 600 Highland Ave, Madison, WI 53792-3248.
E-mail: [email protected]
Received 10 January 2008; Revision accepted 12 January 2008
DOI 10.1002/ccd.21520
Published online 26 March 2008 in Wiley InterScience (www.
interscience.wiley.com).
' 2008 Wiley-Liss, Inc.
Catheterization and Cardiovascular Interventions 71:992–994 (2008)

vertebral artery filter was removed to avoid it beingjailed by the stent. A 7.0 mm 3 24 mm Palmaz Gene-sis stent (Cordis Endovascular, Miami Lakes, FL) wasdeployed via the brachial artery sheath. Followingstenting, brisk antegrade flow was achieved and therewas complete resolution of the pressure gradient. Sig-nificant atheromatous debris was visibly evident in thefilter devices upon removal. The patient returned towork the following day, without neurologic sequelaeand is currently symptom free 6 months after revascu-larization.
DISCUSSION
We present a case of successful percutaneous sub-clavian artery CTO revascularization with coronarydevices and dual cerebral embolic protection. Becauseof the flush occlusion of the ostial right subclavian, thelesion was approached from the ipsilateral brachialartery. Coronary devices were initially chosen to mini-mize the risk of severe thoracic hemorrhage in case ofguide wire induced perforation. Filter embolic protec-tion systems are indicated to contain and remove em-bolic material (thrombus/debris) while performing ca-rotid artery interventions. In our case, stroke risk wasconsidered increased due to the ostial location of theright subclavian artery occlusion, the presence of ante-grade vertebral artery flow, the large atheroma burden,and the retrograde recanalization approach. Therefore,filter wires were positioned in both the ipsilateral ver-tebral and carotid arteries for cerebral protection. Toour knowledge, this is the first report of dual cerebralprotection devices for subclavian artery intervention.Typically, obstructive subclavian artery disease leads
to ipsilateral vertebral artery blood flow reversal asblood is drawn from contralateral vertebral, basilar, orcarotid arteries via cerebral communicating arteries.The contralateral vertebral arteries may appear enlargedor ‘‘dominant’’ to accommodate increased flow demand.This physiology may protect against vertebrobasilarstroke with percutaneous revascularization. Alternatively,the patient we present had antegrade vertebral artery flowdue to subclavian artery reconstitution from thyrocervicalcollaterals. This latter physiology may warrant vertebral
Fig. 1. Ostial right subclavian artery occlusion is demon-strated by selective angiography from right brachial arterysheath (left image) and brachiocephalic artery sheath (rightimage).
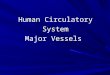
Fig. 2. Dual cerebral embolic protection filters (white arrows)positioned in the right vertebral artery and right carotid arteryduring successful subclavian occlusion recanalization.
Fig. 3. Significant, bulky atheroembolic debris is seentrapped in the carotid artery filter (arrow) after successfulintervention.
Subclavian Chronic Occlusion Revascularization 993
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

artery embolic protection during proximal percutaneoussubclavian artery intervention [2].Percutaneous transluminal angioplasty and stenting for
subclavian artery stenosis is widely performed; how-ever, the experience for subclavian artery CTO inter-vention is confined to a few, small case series [3–7].Potential advantages include avoidance of a cervicalincision and general anesthesia, shorter duration ofinduced occlusion, improved access to some lesions,reduction in hospital stay, and more rapid postopera-tive recovery with return to function. Potential compli-cations include vascular access site bleeding, emboliza-tion, dissection, stent dislodgement or fracture, intra-thoracic hemorrhage, and restenosis [6]. Sharma et al.reported stroke events in two patients undergoing prox-imal subclavian artery angioplasty and both had ante-grade ipsilateral vertebral artery flow [4]. It is sug-gested that the greatest risk of embolism occurs withballoon predilatation, rather than with stent deploy-ment, which was the case in our patient [6]. Alterna-tively, Martinez et al. reported a series of 17 patientswith subclavian artery occlusion treated percutaneously[5]. Although no major complications were reported,no patients were observed to have antegrade ipsilateralvertebral artery flow. Mathias et al. attempted subcla-vian artery occlusion recanalization in 46 patients,with an 83% procedural success rate and no neurologiccomplication [7].
To conclude, low profile coronary artery devicescombined with cerebral embolic protection devicesmay offer enhanced safety for percutaneous subclavianartery CTO revascularization. The case presented illus-trates an example of how major stroke was potentiallyaverted with the use of cerebral protection devices.
REFERENCES
1. Lehmann MF, Mounayer C, Benndorf G, Piotin M, Moret J. Pul-
satile tinnitus: A symptom of chronic subclavian artery occlusion.
AJNR Am J Neuroradiol 2005;26:1960–1963.
2. Gimelli G, Tefera G, Turnipseed WD. Vertebral artery embolic
protection via ipsilateral brachial approach during left subclavian
artery angioplasty and stenting—A case report. Vasc Endovascu-
lar Surg 2006;40:235–238.
3. Duber C, Klose KJ, Kopp H, Schmiedt W. Percutaneous translumi-
nal angioplasty for occlusion of the subclavian artery: Short- and
long-term results. Cardiovasc Intervent Radiol 1992;15:205–210.
4. Sharma S, Kaul U, Rajani M. Identifying high-risk patients for
percutaneous transluminal angioplasty of subclavian and innomi-
nate arteries. Acta Radiol 1991;32:381–385.
5. Martinez R, Rodriguez-Lopez J, Torruella L, Ray L, Lopez-
Galarza L, Diethrich EB. Stenting for occlusion of the subclavian
arteries. Technical aspects and follow-up results. Tex Heart Inst J
1997;24:23–27.
6. Amor M, Eid-Lidt G, Chati Z, Wilentz JR. Endovascular treat-
ment of the subclavian artery: Stent implantation with or without
predilatation. Catheter Cardiovasc Interv 2004;63:364–370.
7. Mathias KD, Luth I, Haarmann P. Percutaneous transluminal
angioplasty of proximal subclavian artery occlusions. Cardiovasc
Intervent Radiol 1993;16:214–218.
994 Shah et al.
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).