Embed Size (px)
Citation preview

Percutaneous Coronary Interventions in Facilities
without On-Site Cardiac Surgery:
A Report from the National Cardiovascular Data Registry
(NCDR)ACC/SCAI – i2 SummitLate Breaking Clinical Trials
March 29, 2008
On Behalf of the National Cardiovascular Data Registry
Michael A. Kutcher, MDLloyd W. Klein, MDThomas P. Wharton, Jr., MDMandeep Singh, MD, MPHGregory J. Dehmer, MDH. Vernon Anderson, MDJohn S. Rumsfeld, MD, PhDWilliam S. Weintraub, MDEric D. Peterson, MD, MPHFang-Shu Ou, MSSarah Milford-Beland, MSAl Woodward, PhD. MBARalph G. Brindis, MPH
Wake Forest University Health Sciences
Rush University School of MedicineExeter Hospital, Exeter, NHMayo ClinicTexas A&M School of MedicineUniv Texas Health Science, HoustonChief Science Officer, NCDRChristiana Health Care, Wilmington,
DEDuke Clinical Research Institute (DCRI) DCRIDCRINCDRChief Executive Officer, NCDR

Special Thanks• Jessica Morris
Data Clarification Project Contact Staff• Kristi Mitchell, MPH
Data Clarification Project Coordinator• NCDR and DCRI support staff• Matthew Sacrinty, MS
Wake Forest University Health Sciences
All the hospitals and their staff that have committed to participate in the NCDR

No DisclosuresRelated to this presentation

Background
• There are few published large studies that have examined whether the procedural outcomes at PCI facilities that do not have surgery on-site are as safe and effective compared to those facilities that have cardiac surgery on-site.
Wennberg DE et al. JAMA 2004;292:1961-68.Ting HH et al. J Am Coll Cardiol 2006;47:1713-21.Carlsson J et al. SCARR. Heart 2007;93:335-8.

Background
• The National Cardiovascular Data Registry (NCDR) CathPCI Registry is a large ongoing multi-center database that offers a unique opportunity to provide contemporary insights into this controversial issue.
Standard data sets Written definitions Uniform data entry Secure transmission requirements Data quality and auditing checks Risk adjustment algorithms

Study PopulationNCDR CathPCI Registry
Consecutive PCI cases January 1, 2004 to March 30, 2006
308,161 patients465 centers
OFF-SITE Surgery Back-Up9,029 patients
61 centers
ON-SITE Surgery Back-up299,132 patients
404 centers

Off-Site Data Clarification Project
• A Data Clarification (DC) Project was undertaken to address potentially ambiguous data issues unique to Off-Site PCI centers.
• Sites with questionable data were sent a Data Clarification Form (DCF) to clarify whether a patient “transferred for CABG” was elective or emergency and to verify eventual survival.
• An additional Off-Site Capabilities Survey (OSCS) was developed to gather information regarding organization, staffing, and logistics.

Off-Site Data Clarification Project
• Each Off-Site PCI program was formally contacted with follow-up by NCDR staff over a 4 month time period.
• 44 sites with 174 patients had data points that required verification.
• 38 sites (86%) were able to fill out the DCF to reconcile transfer and/or mortality data on 153 patients (88%).
• 49 out of 61 sites (80%) filled out the Off-Site Capabilities Survey (OSCS).

Statistical Analysis by DCRI
• Major endpoints In-hospital death from all causes following PCI Incidence of emergency surgery (version 3.04
definitions): Emergency – CABG performed within <24 hours following PCI
in which there was evidence of active ischemia or mechanical dysfunction.
Emergent/Salvage – patient required cardiopulmonary resuscitation en route to the OR or before anesthesia.
• Secondary endpoints Cerebrovascular accident Renal failure Hemorrhage Myocardial infarction Reperfusion time in cases of primary PCI
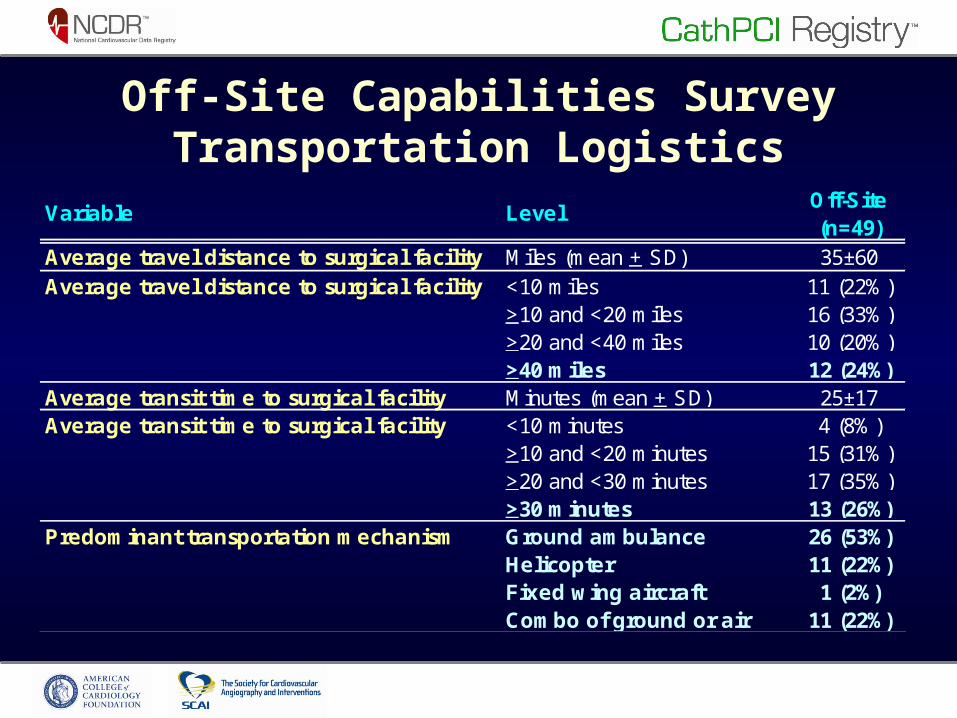
Off-Site Capabilities SurveyTransportation Logistics
Off-Site(n=49)
Average travel distance to surgical facility Miles (mean + SD) 35±60<10 miles 11 (22%)>10 and <20 miles 16 (33%)>20 and <40 miles 10 (20%)>40 miles 12 (24%)
Average transit time to surgical facility Minutes (mean + SD) 25±17<10 minutes 4 (8%)>10 and <20 minutes 15 (31%)>20 and <30 minutes 17 (35%)>30 minutes 13 (26%)Ground ambulance 26 (53%)Helicopter 11 (22%)Fixed wing aircraft 1 (2%)Combo of ground or air 11 (22%)
Predominant transportation mechanism
Variable Level
Average travel distance to surgical facility
Average transit time to surgical facility

Off-Site Capabilities SurveyOrganization and Staff
Off-Site(n=49)
24 hours - 7 days a week (24/7) 45 (92%)Daytime during weekdays only 3 (6%)Variable time frames 1 (2%)Only Primary PCI for acute MI 9 (18%)Both Primary PCI and Elective PCI 40 (82%)Only Elective PCI 0 (0%)Work only at off-site PCI center 39 (80%)Rotate between Off-Site and Off-Site center 9 (18%)N/A 1 (2%)
Interventional operators at facility Mean + SD 5±41 5 (10%)2 to 3 18 (37%)4 to 5 9 (18%)6 or more 17 (35%)Work only at off-site PCI center 8 (16%)Rotate between Off-site and On-Site center 40 (82%)N/A 1 (2%)
Interventional operators experience
LevelVariable
Dedicated staff and facilities for PCI
Type of PCI provided
Cath Lab staff experience
Interventional operators at facility
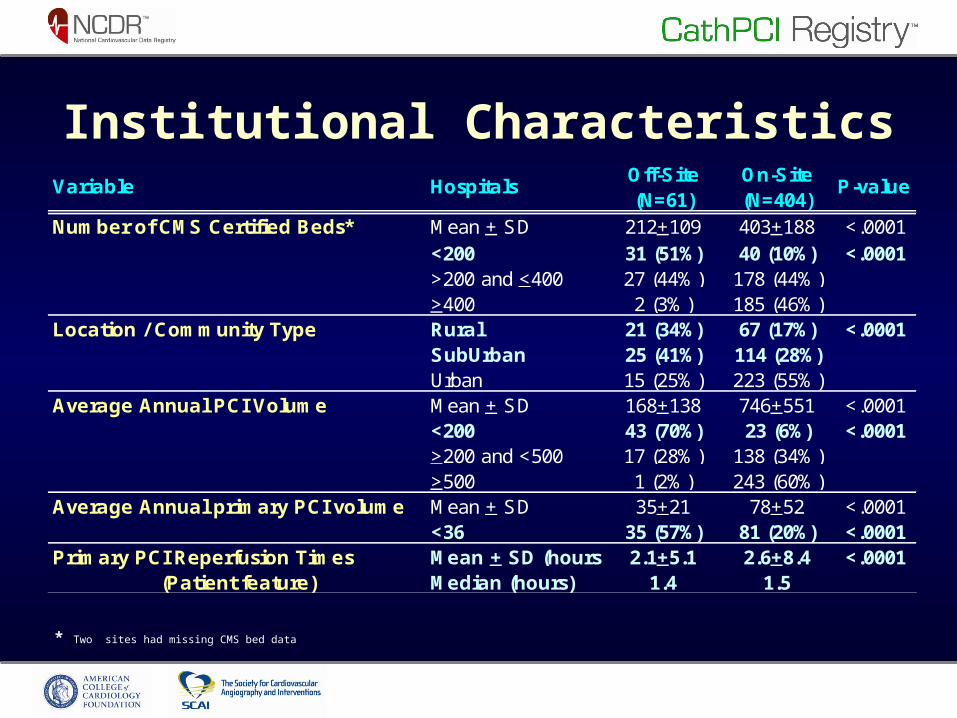
Institutional CharacteristicsOff-Site On-Site(N=61) (N=404)
Number of CMS Certified Beds* Mean + SD 212+109 403+188 <.0001<200 31 (51%) 40 (10%) <.0001>200 and <400 27 (44%) 178 (44%)>400 2 (3%) 185 (46%)Rural 21 (34%) 67 (17%) <.0001SubUrban 25 (41%) 114 (28%)Urban 15 (25%) 223 (55%)
Average Annual PCI Volume Mean + SD 168+138 746+551 <.0001<200 43 (70%) 23 (6%) <.0001>200 and <500 17 (28%) 138 (34%)>500 1 (2%) 243 (60%)
Average Annual primary PCI volume Mean + SD 35+21 78+52 <.0001<36 35 (57%) 81 (20%) <.0001
Primary PCI Reperfusion Times Mean + SD (hours) 2.1+5.1 2.6+8.4 <.0001(Patient feature) Median (hours) 1.4 1.5
P-value
Location / Community Type
Variable Hospitals
* Two sites had missing CMS bed data

MI PresentationOff-Site Backup N=9,029 patients
5,352(59.3%)
2,208(24.4%)
1,469(16.3%)
On-Site Backup N=299,132 patients
44,869(15.0%)
41,681(13.9%)
212,582(71.1%)
No MI Non-STEMI STEMI P < .0001

Procedural Success and Complications
Off-Site Backup On-Site Backup(N=9,029) (N=299,132)
PCI Procedure Success 8,453 (94%) 278,585 (93%) 0.0682
Any Complications 572 (6.4%) 18,791 (6.3%) 0.8075
Variable P-value

Observed Outcomes: All PCI Patients
1.81.7
13.6
0.31.21.2
12.6
0.4
0.0
5.0
10.0
15.0
20.0
EmergencyCABG
Mortality:Emergency
CABG
Mortality: NoEmergency
CABG
Overall Mortality
% O
utc
om
es
Off-Site Backup (N=9,029)
On-Site Backup (N=299,132)
(P=0.3560)(P=0.8838) (P<.0001)
(P<.0001)

Risk Adjusted Outcomes
Odds Ratio (OR): outcomes for patients at On-Site (vs. Off-Site) facilities Adjusting for site correlations and potential confounding variables

Limitations
• In-hospital outcomes were analyzed – long term follow-up was not available.
• Definitions did not discriminate whether emergency surgery was performed for complications of a PCI or whether PCI was a temporizing measure prior to staged surgery.
• Our study was based on a voluntary observational registry and a selection bias cannot be excluded.

Discussion
• Our study involves the largest clinical analysis and comparison of diverse PCI centers in the United States with and without on-site cardiac surgery support.
• The results of the Off-Site Capabilities Survey provides detailed information regarding the organization and logistics of the Off-Site PCI programs participating in the NCDR.

Conclusions
• Off-Site PCI centers participating in the NCDR are well organized with good logistical plans:Dedicated staff and facilities.Travel time, distances, and modality of
transport are generally within range for timely transfer to the off-site surgery center.
92% of sites provide 24/7 coverage.All sites are committed to provide primary PCI
for STEMI.
Conclusions
• Compared to On-Site PCI centers, Off-Site PCI programs:Have smaller bed capacities.Are predominantly located in rural and
suburban areas. Have lower annual PCI volume.Treat a higher percentage of patients who
present with subsets of MI (STEMI and NSTEMI).Have better reperfusion times in primary PCI.

Conclusions
• Compared to On-Site PCI centers, Off-Site PCI programs have similar observed:Procedure successMorbidityEmergency CABG surgery ratesMortality in cases that require emergency
CABG
• The risk-adjusted mortality rate in Off-Site facilities was comparable to those PCI centers that have cardiac surgery on-site.

Implications
• Off-Site PCI centers can provide excellent care to patients – if the organization of the program is thoughtfully developed.
• The Off-Site programs in our study have demonstrated a strong commitment to key structure, process, and outcomes measurements. Without such a commitment, similar results may not be achievable.

Implications
• The findings of our study should not be extrapolated to encourage the wide-spread proliferation of Off-Site PCI programs.
• Our study does confirm the safety of an Off-Site strategy at existing PCI centers where rigorous clinical, operator, and institutional criteria are in place and are monitored to assure high quality outcomes.

Thank You

Backup Slides
Sensitivity Analysis
• Since there was some missing data for follow-up mortality that was not clarified, a sensitivity analysis was performed to assess the stability of the risk adjusted results.
• The analysis was comprised of 4 different models which imputed missing mortality to various potential scenarios.

Sensitivity Analysis
**
**
*Worst case scenario – Patients with missing mortality were considered as all died
**Best case scenario – Patients with missing mortality were considered as all alive

Sensitivity Analysis
• Although the Odds Ratio could change from 1.1 to 0.8, the sensitivity analysis of risk adjusted mortality for any of the 4 models was not statistically significant between Off-Site versus On-Site facilities.
• Based on these results, the missing data would not have significantly affected the stability or the conclusions of the risk adjusted model.

Statistical Analysis
Data Analysis was performed by DCRI: • To test for independence of a patient’s
baseline characteristics, in-hospital care patterns and outcomes with respect to Off-Site vs. On-Site centers were analyzed.
• Mann-Whitney-Wilcoxon nonparametric tests were used for continuous variables.
• Pearson chi-square tests were used for categorical variables.

Statistical Analysis
• A multivariable logistic regression was utilized to estimate the association surgical status (On-Site versus Off-Site) and outcomes.
• The Generalized Estimate Equation (GEE) method was applied to account for within-hospital clustering, assuming patients at the same hospital are more likely to have similar responses relative to patients in other hospitals.

Variables in Risk Adjusted Mortality Model
• Age • Gender • Insulin treated diabetes • Hypercholesterolemia• Hypertension• GFR/dialysis• Cerebrovascular disease• COPD• PVD• CHF• Prior CABG• Prior PCI• Prior MI
• Cardiogenic shock • MI presentation (STEMI,
NSTEMI, no MI) • Preoperative IABP• PCI status (salvage,
emergent, urgent, elective)• Subacute thrombosis• Treated left main lesion• Treated total occlusion • Treated lesion TIMI flow = 0• Treated lesion High/C • Total number of lesions
treated

Variables in Risk Adjusted Emergency Surgery Model
• Cardiogenic shock• MI Presentation
STEMINSTEMINo MI
• Pre-operative IABP• PCI status
SalvageEmergentUrgentElective
• Any treated left main lesion

Results
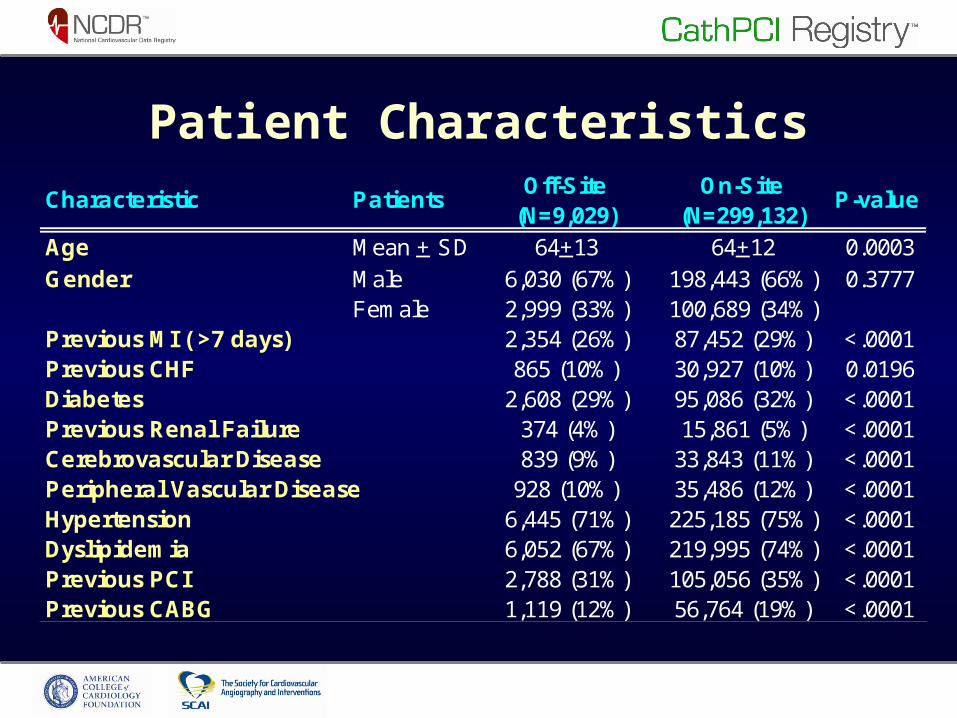
Patient CharacteristicsOff-Site On-Site
(N=9,029) (N=299,132)Age Mean + SD 64+13 64+12 0.0003
Male 6,030 (67%) 198,443 (66%) 0.3777Female 2,999 (33%) 100,689 (34%)
Previous MI ( >7 days) 2,354 (26%) 87,452 (29%) <.0001Previous CHF 865 (10%) 30,927 (10%) 0.0196Diabetes 2,608 (29%) 95,086 (32%) <.0001Previous Renal Failure 374 (4%) 15,861 (5%) <.0001Cerebrovascular Disease 839 (9%) 33,843 (11%) <.0001Peripheral Vascular Disease 928 (10%) 35,486 (12%) <.0001Hypertension 6,445 (71%) 225,185 (75%) <.0001Dyslipidemia 6,052 (67%) 219,995 (74%) <.0001Previous PCI 2,788 (31%) 105,056 (35%) <.0001Previous CABG 1,119 (12%) 56,764 (19%) <.0001
Characteristic Patients P-value
Gender
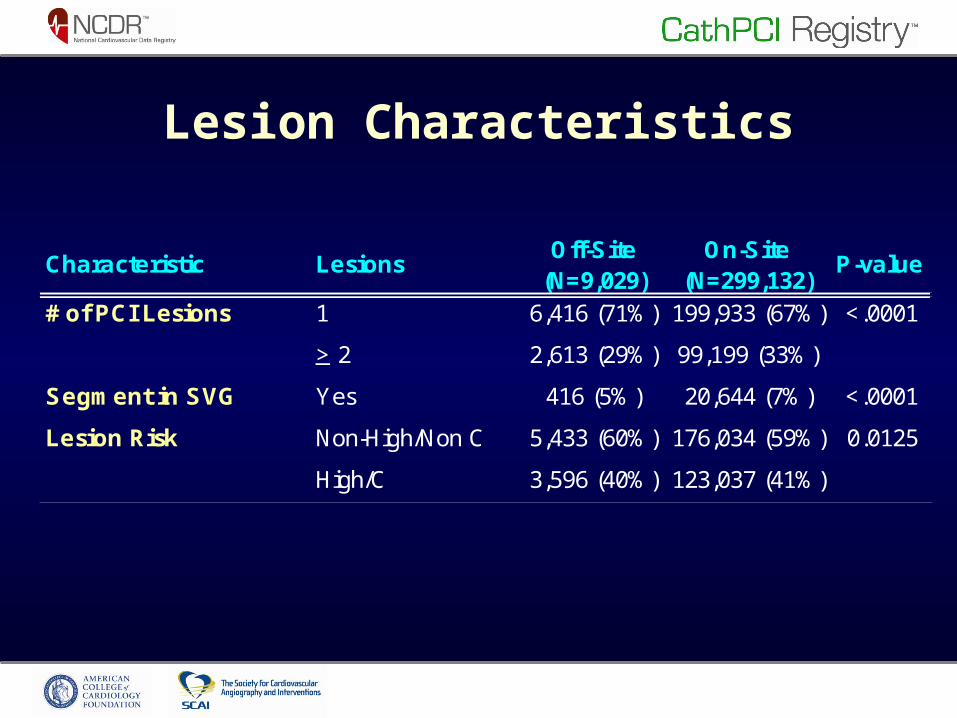
Lesion Characteristics
Off-Site On-Site(N=9,029) (N=299,132)
# of PCI Lesions 1 6,416 (71%) 199,933 (67%) <.0001
> 2 2,613 (29%) 99,199 (33%)
Segment in SVG Yes 416 (5%) 20,644 (7%) <.0001
Lesion Risk Non-High/Non C 5,433 (60%) 176,034 (59%) 0.0125
High/C 3,596 (40%) 123,037 (41%)
Characteristic Lesions P-value

Observed Outcomes: Primary PCI Patients
5.15.1
16.7
0.8
5.25.0
15.9
1.2
0.0
5.0
10.0
15.0
20.0
EmergencyCABG
Mortality:Emergency
CABG
Mortality: NoEmergency
CABG
Overall Mortality
% O
utc
om
es
Off-Site Backup (N=1,971)
On-Site Backup (N=31,062)
(P=0.1213)
(P=0.9439) (P=0.9195)
(P=0.9833)

Background
• Since the introduction of PCI in 1977 by Andreas Gruntzig, a preferred practice has been to have cardiac surgery capabilities on-site to provide emergency CABG in the event of life threatening acute procedural failures.
Background
• Over the last 10 years, as a result of improvements in technology and pharmacology:The incidence of emergency CABG surgery for
failed PCI is now very infrequent (0.3-0.6%)Seshadri N et al. Circulation 2002;106:2346-50.Yang EH et al. J Am Coll Cardiol 2005;2004-20.
Primary PCI has been shown to be superior to fibrinolytic therapy for the treatment of STEMI
Keely et al. Lancet 2003;361:13-20.

Background
• These developments have formed the justification for some hospitals without on-site cardiac surgery to develop PCI programs based on a strategy to:Provide more rapid and superior care for STEMI
in the form of primary PCI Increase the availability of primary and elective
PCI to patients residing in geographically underserved areas.

Background
• The safety and efficacy of performing primary PCI in facilities without on site surgical back-up has been documented in several trials.
Wharton TP Jr. et al. J Am Coll Cardiol 1999;33:1257-65.Aversano T el. C-PORT trial. JAMA 2002;287:1943-51.Wharton TP Jr. et al. PAMI-NoSOS Study. J Am Coll Cardiol
2004;43:1943-50.
• There have been numerous observational reports that extend the Off-Site concept to both primary and elective PCI.
Background
• The ACC/AHA/SCAI 2005 PCI Guidelines designated the following indications for PCI at centers that do not have surgery on-site: Primary PCI – Class IIb “may be considered” Elective PCI – Class III “not recommended”
Smith SC Jr. et al. J Am Coll Cardiol 2006;47:216-35.
• The 2007 Focused PCI Guideline Update did not address or change these designations.
King SB III et al. J Am Coll Cardiol 2008;51:172-209.





























