-
460 J Formos Med Assoc | 2011 • Vol 110 • No 7
Contents lists available at ScienceDirect
Journal of the Formosan Medical Association
Journal homepage: http://www.jfma-online.com
J Formos Med Assoc 2011;110(7):460–466
Journal of the Formosan Medical Association
ISSN 0929 6646
Formosan Medical AssociationTaipei, Taiwan
Volume 110 Number 7 July 2011
Enterovirus 71 vaccine: When will it be available?GRP78 in
embryonic development and neurological disordersDirectly observed
therapy for Tuberculosis patients in TaiwanHIV infection among
incarcerated female drug users
Original Article
Percutaneous Computed Tomography-guidedCryotherapy of Thoracic
Masses in NonsurgicalCandidates: Experience in 19
PatientsSiu-Cheung Chan,1,5* Hui-Ping Liu,2 Winnie Chiu-Wing Chu,3
Tzu-Ping Chen4,5
Background/Purpose: Percutaneous cryotherapy has become a
minimally invasive treatment option forunresectable lung
malignancies. We report the experience and outcomes with
percutaneous computed tomography (CT)-guided cryotherapy of primary
lung malignancies, as well as recurrence and metastases,in patients
ineligible for surgery.Methods: The procedure was performed after
administration of local anesthesia on 23 tumors in 19 patients(10
male and 9 female patients; mean age, 58.7 years). None of the
patients were surgical candidates and un-derwent CT-guided
percutaneous cryotherapy for treatment of the malignant mass in the
lung. Visualizationof low-attenuation ice ball formation was
performed using CT scanning after each cycle of freezing and
thaw-ing therapy. Subsequent CT scans were scheduled at 3-month
intervals post-procedure to assess tumor control.Results: No lethal
complication, major bleeding or bronchial damage was observed in
any of the 23-cryotherapy sessions performed. Three patients
developed pneumothorax and one patient required chest
tubeinsertion. Thirteen tumors (56.5%) regressed, including two
complete responses, five tumors (21.7%) werestationary and the
remaining five tumors (21.7%) were found to be progressing at the
3-month follow-ups.No recurrence was found in the 11 regressed
tumors for 6 months, and there was also no recurrence in thetwo
tumors that completely responded up to 12 months later with a
satisfactory procedure.Conclusion: Percutaneous cryotherapy for
primary lung cancer, recurrence and metastatic lung tumors
isfeasible and safe for local control.
Key Words: computed tomography, cryotherapy, pulmonary
nodules
Percutaneous cryotherapy is recommended for
a range of anatomic and tumor treatment options
because of its low pain, good ice visualization,
and preservation of collagenous tissue architecture.
Cryotherapy has been performed in the liver, pros-
tate, kidney, and breast with good outcomes.1–4
In patients in whom the lung tumor is inaccessible
through the tracheobronchial tree, and surgical
©2011 Elsevier & Formosan Medical Association. . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . .
1Department of Diagnostic Radiology, Chang Gung Memorial
Hospital at Keelung and Linkou Medical Center, Keelung,Taiwan;
2Division of Thoracic Surgery, BenQ Medical Center, Nanjing, China;
3Department of Diagnostic Radiology and OrganImaging, The Chinese
University of Hong Kong, Hong Kong SAR, China; 4Division of
Thoracic Surgery, Chang Gung MemorialHospital at Keelung and Linkou
Medical Center, Keelung, and 5College of Medicine, Chang Gung
University, Taoyuan, Taiwan.
Received: November 27, 2009Revised: May 16, 2010Accepted: May
24, 2010
*Correspondence to: Dr Siu-Cheung Chan, Department of Diagnostic
Radiology, ChangGung Memorial Hospital at Keelung, 222 Mei Chin
Road, Keelung, Taiwan.E-mail: [email protected]
-
Percutaneous CT-guided cryotherapy of thoracic masses
J Formos Med Assoc | 2011 • Vol 110 • No 7 461
resection is not indicated, oncological treatment
of large tumors is often of limited benefit. There-
fore, treatment options are severely restricted.1
Computed tomography (CT)-guided percutaneous
cryotherapy of lung malignancy is considered for
patients ineligible for surgery, and a metastatic
tumor is associated with low procedural morbid-
ity.5 Cryotherapy causes coagulation necrosis con-
fined to the tissues within the region of probe
application, and ice-ball formation occurs as a
result of the dehydration caused by the intracellu-
lar ice crystals that form at very low temperatures.
This leads to protein denaturation and solute tox-
icity within the cells.6,7 The extent and degree of
tissue destruction correlate with the size of the
ice ball and the temperature within it. The latest
generation of cryotherapy machines use the Joule-
Thomson effect, in which different gases undergo
unique temperature changes when depressurized,
according to unique gas coefficients. The proper-
ties of argon make it useful for cooling to below
−180ºC, whereas helium is ideal for thawing andre-warming. The
use of gas allows for rapid tran-
sition from freezing to defrosting, which facili-
tates tighter control, as well as expedition of the
procedure.8 Based on the biological effect of ex-
treme cold, a lethal temperature of approximately
−100ºC at the tumor level is required to achievetotal
destruction of tumors 2 cm or larger in di-
ameter.9 We performed percutaneous cryotherapy
under CT guidance with local anesthesia as a lo-
cally curative treatment for unresectable lung tu-
mors. Twenty-three cryotherapy procedures were
performed successfully in 19 patients, with tissue
proof of unresected primary lung malignancy,
recurrent lung malignancy and lung metastasis.
Materials and Methods
PatientsThe institutional review board of our hospital
approved this retrospective study and informed
consent was waived due to the retrospective and
anonymous nature of the analysis. A total of 23
pulmonary masses in 19 patients (10 male and
9 female patients; mean age, 58.7 years; age range,
19–77 years) were treated with cryotherapy be-
tween October 2007 and September 2009. Five pa-
tients had unresectable non-small cell lung cancer,
six had non-small cell lung cancer after lobectomy
with recurrence, and the remaining eight patients
had lung metastasis. The patients were considered
ineligible for surgery or had undergone other lung
cancer therapies that were unsuccessful. All of the
patients met at least one of the following inclu-
sion criteria: (1) single or multiple peripheral lung
masses larger than 1 cm but less than 5 cm in di-
ameter, with previous therapies (radiation ther-
apy, chemotherapy, and/or surgery) having failed;
(2) a nonresectable central lung cancer (as deter-
mined by means of surgical consultation, accord-
ing to size, stage or health status); (3) fewer than
five metastatic tumors; and (4) a mass or adenopa-
thy involving the mediastinum and/or the peri-
cardium without distant metastasis. The latter was
considered as an inclusion criterion only when it
was associated with a distant measurable primary
lung tumor.
Cryotherapy techniqueThe location and size of tumors were noted
at
preoperative evaluation. A tumor was considered
a central mass if it abutted any of the mediastinal
or hilar structures. Tumor measurements were ob-
tained in two dimensions on CT images, at the
level of the tumor’s most prominent appearance in
the transverse plane. Patients were placed feet first
into the CT gantry for better cryoprobe access.
Cryotherapy was performed after administra-
tion of local anesthesia by one thoracic surgeon
and one radiologist. For sedation, the patients re-
ceived 50 mg pethidine (Demoral; Roche, Basel,
Switzerland) and 5 mg midazolam (Dormicum;
Roche, Basel, Switzerland).
A 21-gauge 15-cm needle was inserted into the
center of each mass under CT-guidance (Light
speed VCT, GE Medical System, Milwaukee, WI,
USA), and used as a guide for subsequent insertion
of cryoprobes. The cryoprobe used was a PERC24
(Endocare, Irvine, CA, USA), it was 2.4 mm in
diameter and it was inserted directly into the
-
S.C. Chan, et al
462 J Formos Med Assoc | 2011 • Vol 110 • No 7
patient. The cryosurgical unit, the Cryocare Surgical
System (Endocare), offers a “stick” function for
fixating a probe’s position once it is inserted into
the tumor. This maximized accuracy when multi-
ple cryoprobes were placed.
Cryoablation is achieved using high-pressure
argon and helium gas for freezing and thawing,
respectively, based on the Joule-Thompson prin-
ciple. Rapid freezing of tissue with a cryoprobe
is based on the rapid expansion of argon gas in
a sealed probe with a distal uninsulated portion.
This process results in rapid cooling to −100ºCwithin a few
seconds. Active thawing of the ice
ball is achieved by introducing helium gas into
the probes instead of argon gas. The cryoablation
procedure we used consisted of two cycles of
10 minutes of freezing and a 5-minute active thaw
between the cycles. During freezing, ice ball growth
and tumor coverage were monitored at 5-minute
intervals by CT scan. For a mass within the lung
tissue, a 2.4-mm cryoprobe can generate an ice
ball up to 3.7 cm in diameter and up to 5.7 cm
along the probe shaft. For this reason, a single
cryoprobe was placed for tumors 2 cm or less in
diameter. An additional cryoprobe was used for
larger tumors to ensure that an adequate freezing
margin of 5–10 mm was achieved. After comple-
tion of the final freeze in the cryotherapy proce-
dure, the cryoprobes were warmed by helium gas
until the temperature was higher than 20ºC. The
cryoprobes were then withdrawn.
Post-procedural evaluationImmediately after the cryoprobes were
removed,
the patient was placed back into the CT gantry for
scanning and measurement of the low-attenuation
ice ball formation. All CT scans obtained after the
percutaneous cryoablation were acquired within
2–3 minutes of termination of freezing; the visible
size of the ice ball remains relatively unchanged
during this time.2,10,11 A repeat CT scan was per-
formed 24 hours after the procedure to evaluate
the type and frequency of complications.
Follow-up helical CT scans of patients were
performed at 3 months post-procedure. Changes
in tumors following cryotherapy were measured
using the Response Evaluation Criteria in Solid
Tumors (RECIST) protocol,12,13 which is based on
objective measurements of lesion size before and
after treatment. “Complete response” (CR) indica-
tes disappearance of the lesion, “partial response”
(PR) is a decrease of at least 30% in the sum of the
longest diameter of target lesions, “progressive
disease“ (PD) is an increase of at least 20% in the
sum of the longest diameter of target lesions, and
“stable disease” (SD) is neither sufficient shrink-
age to qualify for partial response nor a sufficient
increase to qualify for progressive disease.
Results
A total of 23 pulmonary masses in 19 patients
were treated with cryotherapy. In all cases, cryo-
therapy was performed percutaneously under CT
guidance with local anesthesia without major
complications. Complications are listed in Table 1.
The mean hospital stay after treatment was 2.8 days
(range, 2–9 days). There were no treatment-related
deaths or conversions to surgical intervention.
The responses to cryotherapy, measured using
the RECIST protocol, are listed in Table 2. We
observed a CR in two (8.7%) tumors, PR in 11
(47.8%) tumors, SD in five (21.7%) tumors and
PD in five (21.7%) tumors, giving a response rate
of 56.5% (Figures 1 and 2).
Discussion
Percutaneous cryotherapy of lung masses is tech-
nically feasible and may provide an important
Table 1. Complications after cryoablation
Complications n (%)
Pneumothorax 4 (17.4)Chest tube 1 (4.3)Observation 3 (13)
Hemoptysis (without additional treatment) 4 (17.4)
Pleural effusion (without additional 3 (13)treatment)
-
Percutaneous CT-guided cryotherapy of thoracic masses
J Formos Med Assoc | 2011 • Vol 110 • No 7 463
treatment alternative when other treatments do
not yield sufficient local tumor control.14 The
ability to visualize a low-attenuating ice ball as it
thoroughly covers a soft tissue tumor mass during
the freeze cycles is a potential benefit that is not
available with heat-based treatment.
Cryotherapy kills cells and ablates tissue by
direct cell injury resulting from ice crystal forma-
tion and related deleterious effects, as well as vas-
cular stasis caused by microcirculatory failure. As
temperatures fall, direct cellular injury occurs as
a result of cellular metabolism failure. When the
temperature reaches −20ºC, water in the extra-cellular
environment crystallizes into ice, and with-
drawal of the water from the system results in a
hyperosmotic extracellular environment. Conse-
quently, denaturation and electrolyte imbalances
occur.15,16 During thawing, ice crystals fuse to
form larger crystals, which eventually disrupt the
cell membrane, which is another pathway for
causing cell injury. Gage and Baust recommend a
minimum freezing temperature of −40ºC for atleast 3 minutes for
complete eradication of the tu-
mor and a minimum of two freeze-thaw cycles.15,16
This leads to modification of cryotherapy tech-
niques, in turn leading to improved biochemical
and histological outcomes.17
In our series, the response of the lung masses
was evaluated using the RECIST protocol. In the
11 (47.8%) of 23 tumors diagnosed as PR, local
Table 2. Radiographic response and clinical result
Patient Nodules Each tumor’s
Clinical outcome (prognosis after Primary tumor treated with
response after
no.cryotherapya 3 mob
initial cryotherapy)
1 Alveolar soft part sarcoma 2 CRof the thigh PR Stationary (24
POM)
2 Recurrent NSCLC 1 PR Stationary (18 POM)3 Recurrent NSCLC 1 PD
Progression (3 POM, 9 POM dead)4 Recurrent NSCLC 1 SD Liver
metastasis (19 POM alive)5 Recurrent NSCLC 1 PR New pulmonary
nodule (16 POM alive)6 Liposarcoma of the chest wall 2 SD, SD
Stationary (17 POM)7 Esophageal cancer 2 PR, PR New pulmonary
nodule (7 POM,
15 POM dead)8 Rectal cancer 1 PR Liver metastasis (7 POM alive
under
chemotherapy)9 NSCLC 1 PR New pulmonary nodule and multiple
metastasis (10 POM, alive)10 NSCLC 1 PR Stationary (16 POM)11
NSCLC 1 PR Focal regression
New pulmonary nodule (6 POM alive)12 NSCLC 1 PD Died at 4 POM13
Recurrent NSCLC 1 CR Disease-free at 14 POM14 Osteogenic sarcoma 2
PD, PD Progression (3 POM alive)15 NSCLC 1 SD Stationary (6 POM)16
Recurrent NSCLC 1 PD Progression and new pulmonary
nodule (3 POM alive)17 Colon cancer 1 PR Regression (6 POM)18
High-grade sarcoma of the thigh 1 PR Regression (6 POM)19 Renal
cell carcinoma 1 SD Stationary (6 POM)
aTotal pulmonary nodules (n = 23); bCR (n = 2, 8.7%), PR (n =
11, 47.8%), SD (n = 5, 21.7%), and PD (n = 5, 21.7%). CR = complete
regression; PR = partial response; SD = stable disease; PD =
progressive disease; POM = post operative months; NSCLC = non-small
celllung cancer.
-
S.C. Chan, et al
464 J Formos Med Assoc | 2011 • Vol 110 • No 7
recurrence did not occur during more than
6 months of follow-up. In the two (8.7%) of 23
tumors diagnosed as CR, there was no recurrence
during 12 months of follow-up; therefore, our
series had a response rate of 56.5%.
Cryotherapy offers the opportunity to have ex-
cellent healing and resistance to infection. The
cryogenic lesion is an anesthetic lesion that ini-
tially shows minimal surrounding edema or in-
flammation.15,16 Because of this localized effect,
cryotherapy is a well-tolerated procedure. These
lesions, which have been found to be relatively
resistant to infection, show excellent healing, with
minimal scar formation and preservation of tissue
planes.15,16
We achieved our major treatment goals of
using local sedation during the procedures and
preserving underlying tissue architecture with
minimal complications. Because metastatic lung
tumors may associate with other latent metastatic
lesions in the lung, pulmonary reserve after treat-
ment can be important. Greater pulmonary reserve
is expected after cryotherapy, when applied to cen-
trally located tumors than after surgical procedures
such as lobectomy, which is usually required for
resection of such tumors.
In conclusion, percutaneous CT-guided cryo-
therapy offers a viable alternative for a nonsur-
gical lung mass, because it is minimally invasive
and uses local anesthesia, with satisfactory local
control. It preserves respiratory function and
is well tolerated by the patient. The procedure
demands careful patient selection and technical
expertise to achieve satisfactory cancer control,
patient satisfaction, and acceptable quality of
life.
A B
C D
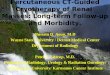
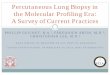
Figure 1. (A) A 1.5-cm lung nodule in the Right lower lobe (RLL)
caused by lung metastasis due to recurrent alveolar softpart
sarcoma. (B) The RLL nodule is being treated from the lateral
approach. One cryoprobe is seen bracketing the nod-ule. Ten minutes
after the beginning of second freezing, an ice ball with hazy
consolidation can be seen surrounding theRLL nodule. (C) Complete
resolution of the RLL nodule with linear scarring was observed 3
months after the procedure.(D) At the 12-month follow-up, complete
resolution of the RLL and no recurrence or residual tumor were
observed.
-
Percutaneous CT-guided cryotherapy of thoracic masses
J Formos Med Assoc | 2011 • Vol 110 • No 7 465
Acknowledgments
We thank William Chan for secretarial assistance.
References
1. Lee FT Jr. Chosy SG, Littrup PJ, et al. CT-monitored
percu-taneous cryoablation in pig liver model: pilot
study.Radiology 1999;211:687–92.
2. Bahn DK, Lee F, Badalament R, et al. Targeted cryo-ablation
of the prostate: 7-year outcomes in the primarytreatment of
prostate cancer. Urology 2002;60(Suppl 1):3–11.
3. Collyer WC, Landman J, Olweny EO, et al. Comparison ofrenal
ablation with cryotherapy, dry radiofrequency, andsaline augmented
radiofrequency in a porcine model. J Am Coll Surgery
2001;193:505–13.
4. Littrup PJ, Freeman-Gibb L, Andea A, et al. Cryotherapyfor
breast fibroadenomas. Radiology 2005;234:63–72.
5. Wang H, Littrup PJ, Duan Y, et al. Thoracic masses
treatedwith percutaneous cryotherapy: initial experience with
morethan 200 procedures. Radiology 2005;235:289–98.
6. Maiwand MO, Homasson JP. Cryotherapy for tracheo-bronchial
disorders. Clin Chest Med 1995;16:427–43.
7. Rubinsky B. Cryosurgery. Ann Rev Biomed Eng
2000;2:157–87.
8. Chin JL, Lim D, Abdelhady M. Review of primary and salvage
cryoablation for prostate cancer. Cancer Control2007;14:231–7.
9. Maiwand O, Glynne-Jones R, Chambers J, et al.
Directcryosurgery for inoperable metastatic disease of the lung.Ann
Thorac Surg 2006;81:718–21.
10. Lee FT, Mahvi DM, Chosy SG, et al. Hepatic cryosurgerywith
intraoperative US guidance. Radiology 1997;202:624–32.
11. Littrup PJ, Mody A, Sparschu RA, et al. Prostatic
cryotherapy:ultrasonographic and pathologic correlation in the
caninemodel. Urology 1994;44:175–84.
12. Tsuchida Y, Therasse P. Response evaluation criteria in
solidtumors (RECIST): new guidelines. Med Pediatr
Oncol2001;37:1–3.
A B
C D
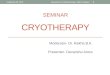
Figure 2. (A) A 3.5-cm lung mass in the RLL due to recurrent
adenocarcinoma. (B) The mass is being treated from theposterior
approach. Two cryoprobes are seen bracketing the mass. (C)
Near-complete resolution of the RLL mass withlinear scarring was
observed 3 months post-procedure. (D) Retained linear scarring
without recurrence or a residualtumor was observed at the 12-month
follow-up.
-
S.C. Chan, et al
466 J Formos Med Assoc | 2011 • Vol 110 • No 7
13. Therasse P, Arbuck SG, Eisenhauer EA, et al. New guide-lines
to evaluate the response to treatment in solid tumors.J Natl Cancer
Inst 2000;92:205–16.
14. Ahmed A, Littrup P. Percutaneous cryotherapy of the thorax:
safety considerations for complex cases. AJR Am JRoentgenol
2006;186:1703–6.
15. Gage AA, Baust JG. Mechanisms of tissue injury in
cryo-surgery. Cryobiology 1998;37:171–86.
16. Baust JG, Gage AA. The molecular basis of cryosurgery.BJU
International 2005;95:1187–91.
17. Patel BG, Parsons CL, Bidair M, et al. Cryoablation for
carcinoma of the prostate. J Surg Oncol 1996;63:256–64.