Embed Size (px)
Citation preview

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S VO L . 8 , N O . 2 , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U NDA T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 4 . 0 7 . 0 3 0
STATE-OF-THE-ART REVIEW
Percutaneous Circulatory Assist Devicesfor High-Risk Coronary Intervention
Aung Myat, MBBS,* Niket Patel, MBBS,y Shana Tehrani, MD,z Adrian P. Banning, MD, PHD,y Simon R. Redwood, MD,*Deepak L. Bhatt, MD, MPHxJACC: INTERVENTIONS CME
This article has been selected as this issue’s CME activity, available online
at http://interventions.onlinejacc.org/ by selecting the CME tab on the
top navigation bar.
Accreditation and Designation Statement
The American College of Cardiology Foundation (ACCF) is accredited by
the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
The ACCF designates this Journal-based CME activity for a maximum of
1 AMA PRA Category 1 Credit(s) �. Physicians should only claim credit
commensurate with the extent of their participation in the activity.
Method of Participation and Receipt of CME Certificate
To obtain credit for this CME activity, you must:
1. Be an ACC member or JACC: Cardiovascular Interventions subscriber.
2. Carefully read the CME-designated article available online and in this
issue of the journal.
3. Answer the post-test questions. At least 2 out of the 3 questions
provided must be answered correctly to obtain CME credit.
4. Complete a brief evaluation.
5. Claim your CME credit and receive your certificate electronically by
following the instructions given at the conclusion of the activity.
CME Objective for This Article: At the completion of this article, the
learner should be able to: 1) consider the patient, anatomical and pro-
cedural characteristics that can elevate percutaneous coronary inter-
vention to a high-risk procedure; 2) discuss the physiology underpinning
the application of percutaneous circulatory assist devices for high risk
percutaneous coronary intervention; and 3) determine which patients
may benefit most from the utilization of the intra-aortic balloon pump,
Impella, TandemHeart or extracorporeal membrane oxygenation.
CME Editor Disclosure: JACC: Cardiovascular Interventions CME Editor
Olivia Hung, MD, PhD, has received research grant support from NIH T32,
Gilead Sciences. and Medtronic Inc.
From the *King’s College London BHF Centre of Research Excellence, The R
Hospital, London, United Kingdom; yDepartment of Cardiology, Oxford He
Oxford, United Kingdom; zHatter Cardiovascular Institute, University Co
xBrigham and Women’s Hospital Heart & Vascular Center and Harvard Med
ported by the Department of Health via the National Institute for Health Re
Author Disclosures: Dr. Myat is supported by the Department of
Health via the National Institute for Health Research (NIHR)
Comprehensive Biomedical Research Centre award to Guy’s & St.
Thomas’ NHS Foundation Trust in partnership with King’s College
London and King’s College Hospital NHS Foundation Trust; and also
receives financial support from the British Heart Foundation via a
Clinical Research Training Fellowship (grant no. FS/11/70/28917). Dr.
Banning is partially funded by the National Institute for Health
Research (NIHR) Oxford Biomedical Research Centre. Dr. Redwood
has received unrestricted grant support for the BCIS-1 Trial; and
travel support from Maquet. Dr. Bhatt is on the advisory board of
Elsevier Practice Update Cardiology, Medscape Cardiology, Regado
Biosciences; is on the Board of Directors of Boston VA Research
Institute and the Society of Cardiovascular Patient Care; is Chair of
the American Heart Association Get With the Guidelines Steering
Committee; is on Data Monitoring Committees of Duke Clinical
Research Institute, Harvard Clinical Research Institute, Mayo Clinic,
and Population Health Research Institute; has received honoraria
from the American College of Cardiology (Editor of Clinical Trials
and Cardiosource), Belvoir Publications (Editor-in-Chief of the
Harvard Heart Letter), HMP Communications (Editor-in-Chief,
Journal of Invasive Cardiology), and Slack Publications (Chief
Medical Editor, Cardiology Today’s Intervention); is Associate Editor
of Clinical Cardiology; is Section Editor of Journal of the American
College of Cardiology; is on the clinical trial steering committees of
Duke Clinical Research Institute, Harvard Clinical Research
Institute, and Population Health Research Institute; is on the CME
steering committee of WebMD; and has received research grants
from Amarin, AstraZeneca, Bristol-Myers Squibb, Eisai, Ethicon,
Medtronic, Roche, Sanofi, and The Medicines Company. All other
authors have reported that they have no relationships relevant to
the contents of this paper to disclose.
CME Term of Approval
Issue Date: February 2015
Expiration Date: January 31, 2016
ayne Institute, Cardiovascular Division, St. Thomas’
art Centre, Oxford University Hospitals NHS Trust,
llege London, London, United Kingdom; and the
ical School, Boston, Massachusetts. Dr. Myat is sup-
search (NIHR) Comprehensive Biomedical Research

Myat et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5
Hemodynamic Support for High-Risk PCI F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4
230
Percutaneous Circulatory A
ssist Devices forHigh-Risk Coronary InterventionABSTRACT
Ce
Ho
Tra
(N
su
Bio
the
Re
ho
Ch
Pu
Jou
Ha
ha
Me
dis
Ma
A unifying definition of what constitutes high-risk percutaneous coronary intervention remains elusive. This
reflects the existence of several recognized patient, anatomic, and procedural characteristics that, when combined,
can contribute to elevating risk. The relative inability to withstand the adverse hemodynamic sequelae of
dysrhythmia, transient episodes of ischemia-reperfusion injury, or distal embolization of atherogenic material asso-
ciated with coronary intervention serve as a common thread to tie this patient cohort together. This enhanced
susceptibility to catastrophic hemodynamic collapse has triggered the development of percutaneous cardiac assist
devices such as the intra-aortic balloon pump, Impella (Abiomed Inc., Danvers, Massachusetts), TandemHeart
(CardiacAssist, Inc., Pittsburgh, Pennsylvania), and extracorporeal membranous oxygenation to provide adjunctive
mechanical circulatory support. In this state-of-the-art review, we discuss the physiology underpinning their
application. Thereafter, we examine the results of several randomized multicenter trials investigating their use in
high-risk coronary intervention to determine which patients would benefit most from their implantation and whether
there is a signal to delineate whether they should be used in an elective pre-procedure, standby, rescue, or routine
post-procedure fashion. (J Am Coll Cardiol Intv 2015;8:229–44) © 2015 by the American College of Cardiology
Foundation.
T he evolution of percutaneous coronaryintervention (PCI) has witnessed unprece-dented advances in the past 2 decades. In
the wake of such progress, interventional cardiolo-gists are now attempting revascularization of morecomplex coronary anatomy in patients oftendeclined for surgical intervention. Yet with greatercomplexity comes greater risk, hence the develop-ment of percutaneous mechanical circulatory support(MCS) devices. Borne from a sound physiological plat-form, in theory they serve to maintain coronary perfu-sion pressure and reduce myocardial workload,allowing the operator sufficient time to optimally
ntre award to Guy’s & St. Thomas’ NHS Foundation Trust in partnersh
spital NHS Foundation Trust; and also receives financial support from t
ining Fellowship (grant no. FS/11/70/28917). Dr. Banning is partially fu
IHR) Oxford Biomedical Research Centre. Dr. Redwood has received unres
pport from Maquet. Dr. Bhatt is on the advisory board of Elsevier Practic
sciences; is on the Board of Directors of Boston VA Research Institute and
American Heart Association Get With the Guidelines Steering Committee
search Institute, Harvard Clinical Research Institute, Mayo Clinic, and
noraria from the American College of Cardiology (Editor of Clinical Trial
ief of the Harvard Heart Letter), HMP Communications (Editor-in-C
blications (Chief Medical Editor, Cardiology Today’s Intervention); is Assoc
rnal of the American College of Cardiology; is on the clinical trial steeri
rvard Clinical Research Institute, and Population Health Research Institut
s received research grants from Amarin, AstraZeneca, Bristol-Myers Squib
dicines Company. All other authors have reported that they have no rel
close.
nuscript received July 8, 2014; accepted July 17, 2014.
complete the procedure. In this review, we highlightthe criteria that elevate PCI to the high-risk category.Thereafter, we compare and contrast the physiologyand evidence base underpinning MCS use to deter-mine where these devices sit in the wider context ofhigh-risk PCI.
WHAT DEFINES HIGH-RISK PCI?
A universally accepted definition of high-risk PCIremains elusive. This reflects the myriad adverseclinical, anatomic, and hemodynamic factors that, iftaken in isolation, are potentially surmountable but
ip with King’s College London and King’s College
he British Heart Foundation via a Clinical Research
nded by the National Institute for Health Research
tricted grant support for the BCIS-1 Trial; and travel
e Update Cardiology, Medscape Cardiology, Regado
the Society of Cardiovascular Patient Care; is Chair of
; is on Data Monitoring Committees of Duke Clinical
Population Health Research Institute; has received
s and Cardiosource), Belvoir Publications (Editor-in-
hief, Journal of Invasive Cardiology), and Slack
iate Editor of Clinical Cardiology; is Section Editor of
ng committees of Duke Clinical Research Institute,
e; is on the CME steering committee of WebMD; and
b, Eisai, Ethicon, Medtronic, Roche, Sanofi, and The
ationships relevant to the contents of this paper to

AB BR EV I A T I O N S
AND ACRONYM S
AMI = acute myocardial
infarction
CBF = coronary blood flow
CI = cardiac index
CO = cardiac output
CS = cardiogenic shock
ECMO = extracorporeal
membrane oxygenation
IABP = intra-aortic balloon
pump
LV = left ventricular
MAP = mean arterial pressure
MCS = mechanical circulatory
support
PCAD = percutaneous
circulatory assist device
PCI = percutaneous coronary
intervention
PPCI = primary percutaneous
coronary intervention
RCT = randomized controlled
trial
STEMI = ST-segment elevation
ardial infarction
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5 Myat et al.F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4 Hemodynamic Support for High-Risk PCI
231
when combined, will significantly increase the chanceof periprocedural, subacute, medium- and long-termmajor adverse cardiac and cerebrovascular eventsoccurring.
HIGH-RISK CRITERIA USED IN
THE CURRENT EVIDENCE BASE
The diversity of criteria adopted by investigators tostudy the performance of percutaneous circulatoryassist devices (PCADs) (Table 1, Online Appendix)would suggest a lack of consensus on what defineshigh-risk PCI. This makes robust intertrial compari-son speculative at best and standardization prob-lematic, especially when patient characteristics,procedural adjuncts, timing of hemodynamic sup-port, and metrics of risk are largely heterogeneous(1,2). To this end, the definition of high-riskPCI becomes somewhat arbitrary, reflecting a needto pigeonhole the population under investigationto satisfy inclusion criteria rather than correspondingto universally accepted parameters. This also limitsour ability to recommend one model of risk stratifi-cation over another. Moreover, risk scores mayidentify who might benefit from MCS, but theydo not, as yet, inform the operator as to which PCADto use or whether it should be used in an electivepre-procedure, standby, rescue, or routine post-procedure fashion. Despite these inconsistencies,there is a common thread. It is the relative inability ofthe high-risk patient to withstand the deleterioushemodynamic consequences of dysrhythmia, tran-sient intervals of ischemia-reperfusion injury, or thedistal embolization of atherogenic material (i.e., theno-reflow phenomenon) associated with PCI. A high-risk patient may have significantly attenuated car-diovascular reserve and be increasingly susceptibleto post-ischemic stunning. The onus falls on theheart team to recognize this patient subset, antici-pate potential difficulties that may occur during theprocedure, and decide whether MCS is an appro-priate intervention. Otherwise, a chain of deleteriousevents may ensue, leading to further reduction incardiac output (CO) and an amplification of ischemia,culminating in cardiogenic shock (CS) or malignantventricular arrhythmia. Conversely, the patient mayalready be in CS on presentation, a diagnosis basedon evidence of hypotension (systolic bloodpressure <90 mm Hg), end-organ hypoperfusion(cool extremities and urine output <30 ml/h), a car-diac index (CI) of #2.2 l/min/m2, and a pulmonarycapillary wedge pressure of $15 mm Hg (3). A mixedvenous blood oxygen saturation <65% may also beincorporated (4).
KEY FUNDAMENTALS OF MECHANICAL
CIRCULATORY SUPPORT
Once Kantrowitz et al. (5) had performed thefirst-in-human intra-aortic balloon pump(IABP) implantation in 1968, the following 4basic characteristics for an MCS device tohave a therapeutic impact on CS managementhad already been proposed: effective inser-tion with minimal surgical application;simplicity of initiation and maintenance forwidespread use by minimally trained profes-sional personnel; capability for aiding thecoronary and peripheral circulation inter-mittently or continuously for hours or days;significant support for the ischemic myocar-dium by reducing its work (Figures 1 and 2).
MAINTENANCE OF
END-ORGAN PERFUSION
The landmark SHOCK (Should We EmergentlyRevascularize Occluded Coronaries for Car-diogenic Shock) trial demonstrated a mid-to long-term survival advantage for earlyrevascularization versus medical stabilization
for managing acute myocardial infarction (AMI)complicated by CS (3,6,7). Although not primarily atrial of IABP, $86% of participants in each trial armreceived a balloon pump, reflecting both the severityof the clinical setting and it being the recognizedmainstay of adjunctive MCS at the time. Moreover,IABP was recommended in the study design for thosepatients randomized to medical stabilization. Post-hoc analysis of the parallel SHOCK trial registry alsoconfirmed the benefit of IABP for lowering in-hospitalmortality (8,9). The SHOCK investigators introducedthe concept of cardiac power output (in W ¼ meanarterial pressure [MAP] � CO/451) and cardiac powerindex (in W/m2 ¼ cardiac power output/bodysurface area) as novel hemodynamic parameters forthe assessment and subsequent management of CS.Although seldom performed now, cardiac poweroutput (p ¼ 0.002) and cardiac power index (p ¼0.004) were shown to be the strongest independentpredictors of in-hospital mortality (10). A core func-tion, therefore, of any PCAD should be to augmentMAP and CO to maintain end-organ perfusion,thereby avoiding (or rationalizing) the use of sup-plementary vasopressor or inotrope therapy.OPTIMIZATION OF MYOCARDIAL PERFUSION
When the epicardial coronary arteries are patent,myocardial tissue perfusion is almost universally
myoc

TABLE 1 Clinical, Anatomic, and Hemodynamic Criteria Used
to Identify the High-Risk Percutaneous Coronary Intervention
Patient
Clinical criteria
Cardiogenic shock occurring within 24 h or at the start of coronaryintervention
Left ventricular systolic dysfunction on presentation: ejectionfraction #30%–40%
Killip class II–IV on presentation or congestive heart failure
Coronary intervention after resuscitated cardiac arrest within 24 h
ST-segment elevation myocardial infarction
Acute coronary syndrome complicated by unstable hemodynamics,dysrhythmia, or refractory angina
Mechanical complications of acute myocardial infarction
Age $70–80 yrs
History of cerebrovascular disease, diabetes, renal dysfunction, orchronic lung disease
Anatomic criteria
Intervention to an unprotected left main coronary artery or left mainequivalent
Multivessel disease
Distal left main bifurcation intervention
Previous coronary artery bypass graft surgery including interventionto a graft, particularly a degenerated graft
Last remaining coronary conduit
Duke Myocardial Jeopardy score $8/12
Target vessel providing a collateral supply to an occluded secondvessel that supplies >40% of the left ventricular myocardium
SYNTAX score $33
Hemodynamic criteria
Cardiac index <2.2 l/min/m2
Pulmonary capillary wedge pressure >15 mm Hg
Mean pulmonary artery pressure >50 mm Hg
A summary of the most frequently used metrics to define high risk in studies ofmechanical circulatory support for percutaneous coronary intervention. This tableis by no means exhaustive or validated but provides a snapshot of the wide rangeof clinical, anatomic, and hemodynamic criteria that various investigators haveused as inclusion criteria in observational and randomized studies. See the OnlineAppendix for a more complete list of high-risk criteria.
Myat et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5
Hemodynamic Support for High-Risk PCI F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4
232
determined by an inverse correlation with microvas-cular resistance and the pressure gradient betweenthe driving aortic force (proximal to the subtendedmyocardium) and coronary sinus/right atrial pressure(the distal vascular bed). During AMI, the microvas-cular resistance is high as a result of vasoconstriction,plugging related to microemboli, and ischemia-reperfusion injury. In CS, this is compounded by adecrease in driving pressure and an increase in rightatrial pressure (11). Mechanical support devicesshould ideally facilitate myocardial perfusion byincreasing the MAP and reducing right atrial pressureto overcome the higher resistance encountered in theinfarct-related territory.
During systole, ventricular contraction exerts acompressive force on the microvasculature, and dur-ing ventricular relaxation in diastole, a large suctioneffect. As such, coronary blood flow (CBF) occurs pre-dominantly in diastole (12). The ideal PCAD should
lower left ventricular (LV) end-diastolic pressure.This, in turn, diminishes microvascular resistanceand increases the perfusion pressure, subsequentlyincreasing CBF and hencemyocardial oxygen delivery.
INTRA-AORTIC BALLOON
COUNTERPULSATION
The benefit of the IABP is underpinned by the conceptof diastolic augmentation (13,14). Theoretically, thisgives rise to greater myocardial perfusion byincreasing the coronary pressure gradient from theaorta to the epicardial coronary circulation at a timewhen the aortic valve is closed (15). Active deflationimmediately before the onset of systole and preciselyat the beginning of isovolumic contraction creates adead space in the thoracic aorta, which reducesafterload and promotes forward flow from the LV.This stimulates a reduction in LV end-diastolic pres-sure, volume, wall tension, and work (leading to alowering of myocardial oxygen demand) along withpreservation of or an increase in stroke volume,ejection fraction and overall CO (15). The magnitudeof the hemodynamic effect is dependent on theballoon size in proportion to the aorta. The larger theballoon is, the greater the volume of blood displaced(Figure 1) (15). The blood volume displaced toward theaortic root has been calculated at 6.4% (during 1:1inflation) and 10.0% (with 1:2 support) of the nominalballoon volume (16). The remainder is stored in thecompliant aortic wall during balloon inflation ordistributed among the branches along the arch.Although this percentage appears small, it representsa significant fraction of baseline coronary flow (16).
An increase in aortic compliance (or reduction insystemic vascular resistance), however, will result indiminution of the IABP effect. Moreover, as heart rateincreases to maintain CO, LV and aortic diastolicfilling times decrease, resulting in less balloonaugmentation per unit of time elapsed. There isconflicting evidence on the degree of post-stenoticCBF augmentation achieved despite the increase inperfusion pressure. Some reports demonstrate noincrease in CBF distal to a critical stenosis (17–19),whereas others have revealed an enhancement ofdistal flow, regardless of the presence or absence ofobstruction (20,21). As such, the predominant benefitof IABP on high-risk patients with severe coronarystenosis may relate to a reduction in oxygen demandthrough LV systolic unloading over and above thatstimulated by diastolic augmentation of CBF (19).
OBSERVATIONAL AND REGISTRY DATA. A recent U.S.CathPCI Registry analysis revealed that IABP use was

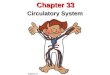
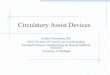
FIGURE 1 Percutaneous Coronary Assist Devices
A comparison of the intra-aortic balloon pump versus the Impella (Abiomed Inc., Danvers, Massachusetts) versus the TandemHeart (CardiacAssist, Inc., Pittsburgh,
Pennsylvania) devices. (Permission to reproduce images received from Maquet Cardiopulmonary AG, Rastatt, Germany; CardiacAssist, Inc., Pittsburgh, Pennsylvania; and
BMJ Publishing Group Ltd., London, United Kingdom.)
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5 Myat et al.F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4 Hemodynamic Support for High-Risk PCI
233
limited to just 10.5% of all high-risk PCI procedures(22). This could partly reflect a lack of interoperatorand interhospital consensus on what is deemed highrisk. Indeed, the criteria used to define high-risk weresuperimposed retrospectively by the authors of theanalysis and were not labeled as such by the opera-tors at individual hospitals inputting the raw data(22). This should negate any selection bias at thesource but could amplify any disconnect betweenwhat the operator or specific hospital protocol wouldrecognize as high risk and what the registry analysisdeems to be high risk. Furthermore, the registryanalysis did not provide any information on thetiming of MCS. Notably, after multivariate adjust-ment, neither in-hospital mortality nor complicationrate varied between hospitals categorized by theirfrequency of IABP implantation. We must also accept
how difficult it is to quantify the expertise, familiar-ity, and confidence that an individual operator haswith the “kit” and what effect this, and the overridingprotocol of the center, has on their decision to use amechanical adjunct.
Similarly, a EuroHeart Survey PCI Registry of thosepatients revascularized for CS as a complication ofAMI revealed that the IABP was only used in 24.8% ofcases (23). Interhospital differences in the definitionof CS may have led to significant selection bias. AgainIABP use did not confer an overall survival advantagein this patient cohort (n ¼ 653), lending credence tothe decision not to use the device routinely (23).
Ultimately, current data from registries and retro-spective analyses cannot be used to confidentlysupport the IABP in high-risk PCI despite its beinga low-risk therapeutic option. Some studies have

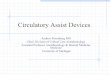
FIGURE 2 Percutaneous Extracorporeal Membrane Oxygenation
Venoarterial extracorporeal membrane oxygenation provides continuous, nonpulsatile cardiac output. Devices have become more portable so
they can now be implanted percutaneously. Permission to reproduce image received from Maquet Cardiopulmonary AG, Rastatt, Germany.
Myat et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5
Hemodynamic Support for High-Risk PCI F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4
234
shown a significant benefit of IABP in terms of in-hospital mortality (24) and freedom from catheteri-zation laboratory events (25,26), whereas others havedemonstrated no benefit (22,27–30) or even a trendtoward harm (23,31).
RANDOMIZED TRIAL DATA. Early ST-segment ele-vation myocardial infarction (STEMI) trials haveshown benefit when IABP was implanted post-procedure for 36 to 48 h (4,32,33). Extrapolation tomodern-day PCI, however, is difficult because pa-tients were treated primarily by balloon angioplasty.The IABP has also been associated with reducedmortality when combined with thrombolysis forAMI (8,31). Latter-day single-center, randomizedcontrolled trials (RCTs) have been underpowered toprovide meaningful answers; trial participants andmetrics of risk are heterogeneous, timing of MCSinitiation varies, and their findings conflict (OnlineAppendix).
THE BCIS-1 TRIAL. The BCIS-1 (Balloon Pump-Assisted Coronary Intervention Study-1) was thefirst prospective, open, multicenter RCT designed todetermine whether elective IABP insertion beforehigh-risk single-vessel or multivessel PCI was able to
reduce major adverse cardiac and cerebrovascularevents at 28 days (34). Metrics of high risk included amodification of the Duke Jeopardy score. There was,however, no protocol-mandated assessment of coro-nary disease complexity or requirement for completerevascularization of all amenable lesions. BailoutIABP was permitted in the no-planned IABP group ifclinical circumstances justified the intervention.There were similar rates of the primary endpoint ofmajor adverse cardiac and cerebrovascular events inboth treatment arms (15.2% elective IABP vs. 16.0%no planned IABP, p ¼ 0.85). There was no significantdifference in the secondary endpoint of 6-monthmortality or overall rates of bleeding. When brokendown, there were significantly more minor bleeds inthe elective IABP arm (15.9% elective IABP vs. 7.3%no-planned IABP arm, p ¼ 0.02). Conversely, peri-procedural complications occurred more frequentlyin the no-planned IABP arm, predominantly due toprocedural hypotension (1.3% vs. 10.7% in favor ofelective IABP, p < 0.001), which might explain theneed for rescue/bailout IABP in 18 patients (12%).
Overall, the study did not support the use of pro-phylactic IABP insertion before high-risk PCI. Giventhe rate of crossover, an initial strategy of standby

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5 Myat et al.F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4 Hemodynamic Support for High-Risk PCI
235
IABP for PCI in those patients with compromisedmyocardial reserve and extensive coronary arterydisease could attenuate the delay in gaining arterialaccess, and would therefore seem a sensible strategy.Interestingly, those patients requiring rescue IABPin the no-planned IABP group had a significantlyhigher BCIS-1 Jeopardy score (Jeopardy score 11.2 vs.10.2, p ¼ 0.02), further emphasizing the need forstandby MCS in those at the extreme end of the riskspectrum.
Five-year all-cause mortality data from the BCIS-1study are now available with complete capture of alltrial participants using a central national database(35). The Kaplan-Meier curves demonstrated a sig-nificant survival advantage in favor of elective IABP(hazard ratio: 0.66, 95% confidence interval: 0.44 to0.98, p ¼ 0.039), which appear to be diverging furtherstill at the 5-year mark. Analysis by treatmentreceived also confirmed a mortality benefit in those 18
TABLE 2 Current Guideline Recommendations for the Use of Percuta
Guidelines, Year (Ref.#) IABP
American College of Cardiology/American Heart Associat
PCI, 2011 (48) A hemodynamic support device is recommenwith pharmacological therapy.
Class I, Level of Evidence: BElective insertion of an appropriate hemodynClass IIb, Level of Evidence: CHigh-risk patients include:
� Unprotected left main or last remaining con� Cardiogenic shock.
STEMI, 2013 (44) IABP can be useful for patients in cardiogenicwho do not quickly stabilize with pharma
Class IIa, Level of Evidence: B
UA/NSTEMI, 2013 (50) IABP is reasonable in UA/NSTEMI patients fofrequently recurring severe ischemia despmedical therapy, hemodynamic instabilityangiography, and for mechanical complica
Class IIa, Level of Evidence: C
European Soc
PCI, 2014 (49) Short-term mechanical circulatory support inClass IIb, Level of Evidence: C
IABP insertion should be considered in patienhemodynamic instability/cardiogenic shocmechanical complications.
Class IIa, Level of Evidence: CRoutine use of IABP in patients with cardioge
not recommended.Class III, Level of Evidence: A
STEMI, 2012 (45) IABP may be considered for the treatment ofshock (Killip class IV) after STEMI.
Class IIb, Level of Evidence: B
UA/NSTEMI, 2011 (51) No recommendations.
The Impella device is manufactured by Abiomed Inc. (Danvers, Massachusetts). The Tan
ACS ¼ acute coronary syndrome; IABP ¼ intra-aortic balloon pump; NSTEMI ¼ non–ST-myocardial infarction; UA ¼ unstable angina.
patients who had crossed over. No systematic differ-ences were found between groups at baseline orregarding the extent of revascularization; both arepotential confounders (35,36). The etiology of death,however, is unknown, hampering any efforts tomechanistically understand the reduced mortalityseen in the elective IABP arm and limiting the abilityto make any robust cause-and-effect associations.Since the trial was not originally designed to inves-tigate all-cause mortality, inferences made can onlybe hypothesis generating. Nevertheless, the resultsshould stimulate future studies to be poweredadequately for all-cause mortality and to incorporatelong-term surveillance so that differences not imme-diately apparent may be detected later.
THE CRISP-AMI TRIAL. The CRISP AMI (Counter-pulsation to Reduce Infarct Size Pre-PCI AcuteMyocardial Infarction) trial was a prospective, open,
neous Circulatory Assist Devices During High-Risk PCI
Impella TandemHeart Extracorporeal Membrane Oxygenation
ion/Society for Cardiovascular Angiography and Interventions Recommendations
ded for patients with cardiogenic shock after STEMI who do not quickly stabilize
amic support device as an adjunct to PCI may be reasonable in carefully selected high-risk patients.
duit PCI. � PCI of a vessel subtending a large territory on a background of severelydepressed left ventricular function.
shock after STEMIcological therapy.
Alternative left ventricular assist devices for circulatory support may beconsidered in patients with refractory cardiogenic shock.
Class IIb, Level of Evidence: C
r continuing orite intensivepre- or post-tions of MI
No individual device recommendations.
iety of Cardiology Recommendations
ACS patients with cardiogenic shock may be considered.
ts withk due to
nic shock is
No other individual device recommendations.
cardiogenic Left ventricular assist devices maybe considered for circulatory support forpatients in refractory shock post-STEMI on anindividual basis, taking into account theexperience of the group along with patientage and comorbidities. They are notrecommended as first-line treatment.
Class IIb, Level of Evidence: C
demHeart device is manufactured by CardiacAssist, Inc. (Pittsburgh, Pennsylvania).
segment elevation myocardial infarction; PCI ¼ percutaneous coronary intervention; STEMI ¼ ST-segment elevation

TABLE 3 Meta-Analyses of Percutaneous Circulatory Assist Devices in Acute Myocardial Infarction With or Without Cardiogenic Shock
First Author (Ref.#),Year Published
No. of StudiesIdentified n
Device(s) UnderInvestigation Clinical Scenario Primary Endpoint Secondary Endpoint Salient Messages
Sjauw et al.(74), 2009
7 RCTs in first M-A,9 cohort studiesin second M-A
1,00910,529
IABP STEMI and STEMIcomplicated by CS
All-cause mortality at30 days
LVEF, stroke, bleeding First M-AIABP in STEMI was not associated with a change in
30-day mortality (p ¼ 0.75).IABP was associated with a significant increase in the
rate of stroke (p ¼ 0.03) and bleeding (p ¼ 0.02).Second M-AIn the thrombolysis era, IABP associated with 18%
lower 30-day mortality (p < 0.0001).In PPCI studies, IABP associated with 6% higher
30-day mortality (p ¼ 0.0008).
Cheng et al.(79), 2009
2 RCTs, IABP vs.TandemHeart
1 RCT, IABP vs.Impella
100 IABP (n ¼ 47) vs.Impella orTandemHeart(n ¼ 53)
Cardiogenic shock 30-day mortality Cardiac index, MAP,PCWP, leg ischemia,major bleeding
No significant difference in survival at 30 days(p ¼ 0.80).
Percutaneous LVAD gave rise to a higher cardiac index(p < 0.01), higher MAP (p < 0.01), and lowerPCWP (p < 0.05).
Similar rates of leg ischemia were observed in bothgroups (p ¼ 0.13).
Bleeding was more frequently associated with theTandemHeart device (p < 0.01).
Hemolysis was significantly higher with the Impelladevice (p < 0.05).
Bahekar et al.(75), 2012
16; 13 prospective,3 retrospective
Note: Majority ofpatients camefrom NRMI-2Registry (4)(n ¼ 23,180)
27,690 IABP IABP vs. no IABP usein AMI with orwithout CS
In-hospital mortality,reinfarction, recurrentischemia
Moderate and severebleeding at 7 days
No difference in in-hospital mortality with or withoutIABP in AMI without CS (RR: 1.11,95% CI: 0.69–1.78, p ¼ 0.67).
IABP was associated with significantly improvedin-hospital mortality when used in AMI with CS(RR: 0.72, 95% CI: 0.60–0.86, p < 0.0004).
No significant reduction in reinfarction or recurrentischemia with IABP.
IABP was associated with a significant increase inthe risk of moderate (p [ 0.04) and major(p < 0.0001) bleeding.
Cassese et al.(76), 2012
6, all RCTs 1,054 IABP (49.1% IABPvs. 50.9%no IABP)
AMI without CS All-cause death CHF, reinfarction,recurrent myocardialischemia, CVA,bleeding
IABP did not reduce the risk of all-cause death (4.4%vs. 4.1%, OR: 1.11, 95% CI: 0.49–2.54, p ¼ 0.80).
IABP did not reduce the risk of CHF (17.1% vs. 18.0%,OR: 0.92, 95% CI: 0.43–1.96, p ¼ 0.83).
IABP did not reduce the risk of reinfarction (5.3% vs.7.7%, OR: 0.68, 95% CI: 0.23–1.76, p ¼ 0.42).
IABP caused significantly more bleeding (21.4% vs.16.1%, OR: 1.46, 95% CI: 1.05–2.04, p [ 0.02).
Chen et al.(77), 2013
10, all RCTs 2,037 IABP High-risk reperfusiontherapy, CS excludedfrom this M-A
30-day mortality,$6-month mortality
Composite incidence ofreischemia and HF
No significant difference between IABP and no IABPwith regard to early mortality (OR: 0.79, 95%CI: 0.48–1.29, p ¼ 0.34).
IABP significantly reduced long-term mortality(OR: 0.63, 95% CI: 0.45–0.90, p [ 0.01).
Subgroup analysis of more contemporary studies(n [ 5) all using PCI still confirmed a significantrisk reduction in 6-month mortality (p [ 0.01)and ‡6-month mortality (p [ 0.002) withIABP use.
IABP associated with 25% relative risk reduction ofreischemia and HF events (p ¼ 0.04).
IABP significantly reduced the risk of 30-dayreischemia rate (p ¼ 0.01).
Continued on the next page
Myat
etal.
JACC:CARDIO
VASCULAR
INTERVENTIO
NS
VOL.8,NO.2,2015
Hem
odynamic
Supportfor
High-R
iskPCI
FEBRUARY
2015:2
29–44
236

TABLE
3Co
ntinue
d
FirstAut
hor(R
ef.#),
Yea
rPub
lishe
dNo.
ofStud
ies
Iden
tified
nDev
ice(s)
Und
erInve
stigation
Clinical
Scen
ario
PrimaryEn
dpoint
Seco
ndaryEn
dpoint
Salie
ntMes
sage
s
Rom
eoet
al.
(78),20
1311;7RCT
san
d4
observationa
lstud
ies
2,134(1,595from
RCT
san
d53
9from
observationa
lstud
ies)
IABP
High-ris
kPC
Isup
ported
byprop
hylactic
IABP
In-hospitalmortality
MACC
E,access-site
complications,s
trok
eIABPwas
notassociated
withasign
ificant
redu
ctionin
theov
erallRRforde
ath(RR:0.97,
p¼
0.91).
Nosign
ificant
differen
cein
riskof
MACC
E(AMI,
reinfarction
,recu
rren
tisch
emia,a
ndcerebrov
ascu
larev
ents
durin
gho
spitalization)
betw
eenthe2grou
ps(RR:0.83,
p¼
0.44).
Therewereno
sign
ificant
differen
cesin
theris
kof
stroke
(p¼
0.21)
oraccess
site
complications
betw
eenthe2grou
ps(p
¼0.35).
TheIm
pella
device
isman
ufacturedby
Abiom
edInc.
(Dan
vers,M
assach
usetts).Th
eTa
ndem
Hea
rtde
vice
isman
ufacturedby
CardiacA
ssist,Inc.
(Pittsbu
rgh,
Penn
sylvan
ia).
AMI¼
acutemyo
cardialinfarction;
CHF¼
cong
estive
heartfailu
re;C
I¼co
nfide
nceinterval;C
S¼
cardioge
nicshoc
k;CV
A¼
cerebrov
ascu
laraccide
nt;L
VAD¼
left
ventric
ular
assist
device;L
VEF
¼left
ventric
ular
ejection
fraction
;M-A
¼meta-an
alysis;M
ACC
E¼
major
adve
rsecardiacan
dcerebrov
ascu
lare
vents;MAP¼
mea
narteria
lpressure;
NRMI¼
Nationa
lReg
istryof
Myo
cardialInfarction;
OR¼
odds
ratio;
PCWP¼
pulm
onarycapilla
rywed
gepressure;P
PCI¼
prim
arype
rcutan
eous
corona
ryinterven
tion
;RCT
¼rand
omized
controlle
dtrial;RR¼
relative
risk;
othe
rab
brev
iation
sas
inTa
ble2.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5 Myat et al.F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4 Hemodynamic Support for High-Risk PCI
237
multicenter RCT undertaken to determine whetherprophylactic IABP insertion within 6 h of pain onsetand planned primary PCI (PPCI) for anterior STEMI(without CS) could reduce the mean infarct size, asmeasured by cardiac magnetic resonance imagingbetween 3 and 5 days post-intervention (37). IABPinsertion in the PPCI alone group was at the opera-tor’s discretion for indications such as persistenthypotension, overt CS, malignant arrhythmias, andAMI complications. Of note, 15 patients (8.5%)initially receiving standard care crossed over toIABP. This again highlights the susceptibility ofthese high-risk patients to hemodynamic collapse,which in turn further supports the argument forstandby MCS.
The primary efficacy endpoint was not significantlydifferent between the 2 groups. Secondary cardiacmagnetic resonance imaging measures such as meanLV ejection fraction and LV systolic volume were alsosimilar. There were no significant differences in majorbleeding/transfusion or major vascular complicationsat 30 days. By 6 months, mortality rates along withthe composite endpoint of death, recurrent MI, ornew or worsening heart failure had not diverged.There was a significant difference in the exploratorycomposite endpoint of time to death, shock, or new orworsening heart failure in favor of PPCI plus IABP(5.0% vs. 12.0%, p ¼ 0.03). Like BCIS-1, longer termfollow-up is planned for the CRISP-AMI population,which may uncover further trends as events accrue.For now, the investigators postulate that meanischemic times (time between symptom onset to firstdevice application) of longer than 3 h may havebeen outside a therapeutic window in which sig-nificant myocardial salvage could have occurred(37–39). This explanation contradicts an RCT inwhich LV infarct size was significantly reduced bymechanical reperfusion in AMI patients presenting12 to 48 h after symptom onset (40). Overall, thetrial was underpowered for the evaluation of clinicaloutcomes after IABP implantation. Moreover, thecohort studied was not that sick. Couple that withearly reperfusion from PPCI having such a dominanteffect on myocardial salvage and hence mortality, itcould be argued that any further adjunctive mea-sures would add very little to the net clinicalbenefit. A strategy of routine prophylactic IABP im-plantation in PPCI of STEMI without CS cannottherefore be advocated.
THE IABP-SHOCK II (INTRAAORTIC BALLOON PUMP
IN CARDIOGENIC SHOCK II) TRIAL. The trial enrolled600 patients with CS complicating AMI proceeding toearly revascularization (almost double that of the

Myat et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5
Hemodynamic Support for High-Risk PCI F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4
238
landmark SHOCK trial), who were then randomized inan open-label manner to IABP or no IABP (3,41).Importantly, the timing of MCS was at the discretionof the operator and could be applied before PCI (n ¼37, 13.4%) or immediately post-procedure (n ¼ 240,86.6%). The trial did not achieve its primary endpointof 30-day all-cause mortality (IABP group 39.7% vs.control group 41.3%; p ¼ 0.69). Indeed, the mortalityrate itself appears relatively low compared with theoriginal SHOCK trial (30-day mortality rate of 46.7%in the early revascularization arm), although trendsin hospital outcomes associated with CS do confirmdeclining short-term death rates over time (42.0%case fatality rate in 2005) (3,42). As such IABP-SHOCK II may well have been underpowered todetect a difference in mortality. The “low” mortalityrate also calls into question the definition of CSused by the investigators. There was an absenceof mixed venous saturation, wedge pressure, andCI parameters used to satisfy a CS diagnosis (3,4).Moreover, there were a significant proportion ofpatients (IABP group 42.2% vs. control group 47.8%)who required resuscitation before randomization.Given that resuscitation for more than 30 min wasan exclusion criteria, we can only assume that thesepatients required resuscitation for 30 min or longer,during which time their hemodynamic indicesmay have transiently satisfied a protocol-driven CSdiagnosis. Furthermore, w80% of patients in eacharm also required mechanical ventilation for a me-dian of 3 days and spent a median of 6 days in theintensive care unit. The lower-than-expected mor-tality could thus be attributed to superior criticalcare management. Although entirely speculative,it does reinforce the notion that the populationunder investigation was not entirely representativeof true CS.
There was also no significant difference in mor-tality between either MCS strategy (pre-PCI 36.4% vs.post-PCI 36.8%; p ¼ 0.96). That patients receivedan IABP post-procedure would suggest that theirperceived hemodynamic instability at randomizationwas not severe enough to warrant prophylactic sup-port. On the contrary, had there been a protocolstipulation for prophylactic counterpulsation only,we might have observed greater benefit becausesusceptibility to circulatory collapse is heightenedduring PCI in this cohort. There was also a liberal useof catecholamines in almost 90% of patients in botharms at randomization. Given that a standoutadvantage of using MCS is to obviate the need tocontinue pharmacological circulatory support, itwould seem to defeat the purpose of investigatingIABP effects if these agents were so widely used.
Catecholamines were continued for a median of 3days in each trial arm. At 1 year, mortality remainedsimilar in both arms (IABP group 52% vs. controlgroup 51%; p ¼ 0.91). IABP insertion did no excessharm, with no significant differences between eithergroup in terms of stroke, bleeding, sepsis, or periph-eral ischemic complications requiring intervention(41).
Are we expecting too much from a devicethat can only augment systemic blood flow by<500ml/min/m2? Bear inmind the pathophysiology ofCS is not only a compromise in cardiac contractilefunction but also encompasses a multiorgan dysfunc-tion syndrome secondary to peripheral hypoperfusionalong with microcirculatory dysfunction, oftencomplicated by a systemic inflammatory responsesyndrome and sepsis (11,43). In light of these equivocalresults, the use of IABP in CS complicating AMIhas been downgraded from a previous Class I indica-tion to a Class IIa and Class IIb recommendation in themost recent U.S. and European STEMI guidelines,respectively (Table 2) (44,45).
IMPELLA
The Impella (Abiomed Inc., Danvers, Massachsetts)is positioned across the aortic valve under radio-graphic or echocardiographic guidance. It aspiratesblood from the left ventricle into the ascendingaorta. Impella-mediated LV unloading reduces end-diastolic wall stress, improves diastolic compliance,increases aortic and intracoronary pressure and cor-onary flow velocity reserve, and stimulates a decreasein coronary microvascular resistance (46,47). Thismay allow for recovery of hibernating or stunnedmyocardium. The pigtail conformation promotesstable positioning in the left ventricle and preventsadherence to the endocardium. The mode ofdeployment underscores the importance of rulingout pre-existing aortic valve disease or LV muralthrombus before implantation.
The Impella 5.0 requires surgical cutdown of thefemoral or axillary artery and so is not truly percu-taneous. The Impella 2.5 received U.S. Food and DrugAdministration approval in June 2008 and can pro-vide antegrade flow up to 2.5 l/min (Figure 1). Thenewly introduced Impella CP (known as cVAD inEurope) received U.S. Food and Drug Administrationapproval in September 2012 and is based on the same2.5 platform but can provide flow up to 4.0 l/min.The IMPRESS in Severe Shock (IMPella versus IABPREduces mortality in STEMI patients treated withprimary PCI IN SEVERE and deep cardiogenic SHOCK)trial (NTR3450) will compare the Impella cVAD with

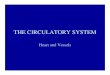
FIGURE 3 Case Vignette #1
Intra-aortic balloon counterpulsation facilitated emergency angioplasty for acute unpro-
tected left main stem coronary artery occlusion. See Online Appendix for detailed
commentary of this case vignette.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5 Myat et al.F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4 Hemodynamic Support for High-Risk PCI
239
IABP in patients with CS complicating AMI awaitingPPCI. Current guideline recommendations for theImpella are shown in Table 2 (44,45,48–51).
The use of the Impella in high-risk PCI includingCS is feasible according to registries and small single-center studies, with demonstrable improvementsin CI and myocardial performance (Online Appendix).However, the increase in vascular access–relatedissues and the propensity for hemolysis due to thehigh rotational speed of the axial flow pump donot appear to be outweighed by any significant gainsin survival. The EUROSHOCK registry reported a30-day mortality of 64.2% in patients presentingwith CS complicating AMI, a figure compounded byaccess site complications occurring in 24.2% of thestudy cohort (52). Potentially, the excess mortalityhere could have been secondary to a selection biasisolating the very sickest patients with a poorhemodynamic profile and imminent risk of death.Indeed, Impella support was only instituted once CShad become refractory to high-dose inotropes andIABP (52).
The ISAR-SHOCK (Efficacy Study of LV AssistDevice to Treat Patients With Cardiogenic Shock)study randomized 25 patients with AMI complicatedby CS to IABP (n ¼ 13) or the Impella LP 2.5 (n ¼ 12)implanted post-revascularization (53). The Impellaachieved significantly greater augmentation of CI, butthis did not result in improved 30-day mortality.There were nonsignificant trends toward greaterrequirements for packed red blood cells and freshfrozen plasma for the Impella group, further empha-sizing the issues associated with higher-profiledevices.
The PROTECT II (Prospective Randomized ClinicalTrial of Hemodynamic Support with Impella 2.5versus Intra-Aortic Balloon Pump in Paitents Under-going High-Risk Percutaneous Coronary Intervention)study is the largest randomized comparison of theImpella and IABP to support nonemergent high-riskPCI to date (54). It did not meet its target recruit-ment of 654 patients because the trial was terminatedearly for reasons of futility. The primary compositeendpoint of major adverse events at hospitaldischarge or 30 days (whichever came sooner) in theintention-to-treat population (n ¼ 448) was similar inboth arms (Impella 35.1% vs. IABP 40.1%; p ¼ 0.277).At 90 days, there was a nonsignificant trend towarda lower major adverse event rate for the Impella (p ¼0.066). At 90 days in the per-protocol population(n ¼ 427), that trend became significant (p ¼ 0.023),suggesting that the Impella may hold promise overthe longer term. The patient cohort studied in PRO-TECT II was similar to that of BCIS-1 (34). Given that
the BCIS-1 study did not support the use of electiveIABP insertion before high-risk PCI, it would seemintuitive to expect that the superior hemodynamicsupport provided by the Impella would offer nosupplementary impact on adverse outcomes.
TANDEMHEART
The TandemHeart (CardiacAssist, Inc., Pittsburgh,Pennsylvania) is inserted via the femoral vein andright atrium into the left atrium via a transseptalpuncture. The outflow cannula is inserted in eitherfemoral artery and positioned at the level of theaortic bifurcation, providing left heart bypass at a

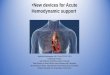
FIGURE 4 Case Vignette #2
The Impella 2.5 (Abiomed Inc., Danvers, Massachsetts: red arrow) to provide essential
hemodynamic support during high-risk multivessel percutaneous coronary intervention.
See Online Appendix for detailed commentary of this case vignette.
Myat et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5
Hemodynamic Support for High-Risk PCI F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4
240
flow rate of w4 l/min into the lower abdominal aortaor iliac arteries (Figure 1). Studies of the TandemHeartin severe refractory CS have shown the device toimprove CI, MAP, and reduce pulmonary capillarywedge pressure, pulmonary artery pressure, andcentral venous pressure, leading to decreased fillingpressures in both ventricles (55–58). This culminatesin an amelioration of myocardial workload and oxy-gen demand.
The TandemHeart is a high-profile system; thus,critical limb ischemia, bleeding, and vascular
complications are a major concern. This was borneout in a randomized comparison of IABP (n ¼ 20) withthe TandemHeart (n ¼ 21) in patients revascularizedfor AMI complicated by CS (59). Although the deviceimproved hemodynamic and metabolic variablesmore effectively, this did not result in a survivaladvantage. Furthermore, severe bleeding and limbischemia occurred more frequently with the Tan-demHeart. Single-center series have demonstratedthe device to be hemodynamically effective andstraightforward to deploy in expert hands (OnlineAppendix). However, the arrival of the Impella CP,which promises to maintain an equivalent flow ratebased on a lower-profile cannula system, may impedethe widespread dissemination of the TandemHeart inthe high-risk PCI arena.
EXTRACORPOREAL MEMBRANE
OXYGENATION
Venoarterial extracorporeal membrane oxygenation(ECMO) is effectively a modified cardiopulmonarybypass circuit that provides a continuous, non-pulsatile CO that can be applied percutaneously viacannulation of the femoral artery and vein (Figure 2)(60,61). ECMO removes carbon dioxide from and addsoxygen to venous blood via an artificial membrane,thereby bypassing the pulmonary circulation (62). Assuch, it is the only PCAD that also oxygenates theblood. ECMO can provide significant hemodynamicsupport but has a propensity to increase LV afterloadand wall stress, which in turn can increase myocardialoxygen demand and therefore limit any cardio-protective benefit.
The implantation procedure requires considerabletechnical skill and full collaboration between thecardiologist, surgeon, catheterization laboratorystaff, anesthesiologist, and perfusionist. The systemis composed of a venous reservoir, external centrif-ugal blood pump, membrane oxygenator, and arewarming heparin-coated circuit. The technologyhas become smaller and more portable. Systemicanticoagulation with heparin is required to achieve anactivated clotting time of 150 to 180 s (63). Contrain-dications to ECMO include significant aortic valveincompetence, severe peripheral arterial disease,bleeding diathesis, recent stroke or head trauma, anduncontrolled sepsis (62).
A retrospective analysis of prophylactic versusstandby cardiopulmonary support revealed signifi-cantly greater procedural morbidity (e.g., femoralaccess site complications) in the former (41% vs.9.4%, p < 0.01) but higher procedural mortality inthe latter (4.8% vs. 18.8%, p < 0.05) (64). The

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5 Myat et al.F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4 Hemodynamic Support for High-Risk PCI
241
investigators suggested that standby CPS was pref-erable in the majority although patients withLVEF <20% may benefit from a prophylactic strategy.Early institution of ECMO for STEMI complicated byprofound CS has been shown to significantly reduce30-day mortality when compared with an historicalcohort of patients not receiving cardiopulmonarysupport (65). Monocentric observational studies andindividual case reports constitute the remainder ofthe evidence base on ECMO-assisted high-risk PCI(60,61,66–73). All confirm the feasibility and efficacyof ECMO, but vascular complications remain a notableproblem. A reduction in platelet count, hemolysis,and a consumptive coagulopathy along with systemicheparinization can further increase the hemorrhagicrisk. Intrathoracic, abdominal, or retroperitonealhemorrhage not related to the access site may alsooccur as a result. Since no RCT or meta-analysis dataare available for ECMO, current guidelines can onlybe based on expert consensus (Table 2).
CAN META-ANALYSES
SHED LIGHT ON THE MATTER?
The majority of meta-analyses have studied outcomesfor IABP versus control in high-risk PCI (74–78). Allecho what we already know. In the PPCI era, IABPdoes not confer a 30-day survival advantage whenused for AMI without CS (74–78). At 6 months orlonger, however, there appears to be a mortalitybenefit signal with an associated reduction in re-ischemia and heart failure events (77). When theanalysis was limited to those with STEMI complicatedby CS, a significantly improved in-hospital outcomewas noted in favor of IABP support, although much ofthis benefit emanated from the thrombolysis era(74,75). This must be taken with a note of cautionbecause thrombolysed patients in those studies ten-ded to be younger and male, and were more likely toundergo subsequent revascularization (74). A singlemeta-analysis compared the Impella and Tandem-Heart with IABP (79). Ventricular assist devicesdelivered superior hemodynamic support, althoughuse of all 3 resulted in similar 30-day mortality rates.There were also similar rates of limb ischemia, butbleeding occurred more often with the TandemHeartand hemolysis with the Impella. The conclusions hereremain tenuous because the analysis was based onjust 100 patients (80) (Table 3).
DISCUSSION
Despite a sound physiological platform, the modestuptake of PCADs to support high-risk PCI (22,23)
reflects the equivocal results and mixed messagesemanating from the current evidence base andlatent uncertainty as to what constitutes high riskoutside of CS. From a clinical standpoint, the IABP,Impella, TandemHeart, and ECMO should have aplace in high-risk PCI, although they cannot beadvocated as standard of care for every procedure.It is up to the heart team to assess, on a case-by-case basis, which patient may benefit from aparticular device and thereafter ensure MCS avail-ability as a standby adjunct in the catheterizationlaboratory. This can only come from shared exper-tise, familiarity with and confidence in using all4 adjuncts, supported by an experienced multi-disciplinary team (Figures 3 and 4, Case Vignettes#1 and #2). The onus should also be on devicecompanies to foster educational relationships withcenters undertaking high-risk PCI and to encourageproctoring of operators keen to learn and gainproficiency.
Moving forward, we must level the playing field.Akin to the consensus definitions proposed for stentthrombosis, bleeding, and trials of transcatheteraortic valve implantation (81–83), there must be awillingness to establish standardized criteria todefine what high-risk PCI is. Thus far, only theAmerican College of Cardiology Foundation/Amer-ican Heart Association/Society for CardiovascularAngiography and Interventions guideline writingcommittee has documented these features (Table 2)(48). It is a fundamental first step in benchmarkinga degree of uniformity between future trials ofhigh-risk PCI to allow researchers, policymakers,and clinicians alike to compare outcomes of a spe-cific intervention with a degree of scientific andstatistical equipoise. Only then can we be moreproscriptive as to which combination of lesioncomplexity and LV ejection fraction, for instance,would indicate the use of a particular PCAD. Thesame applies for trials of CS. The definition fromthe outset should incorporate right heart catheteri-zation parameters and mixed venous saturations toensure that the population under study truly re-flects a CS sample, although we do accept the im-practicalities of conducting the former in criticallyill patients (3,4).
In the end, we return full circle to the days ofHarken, Kantrowitz, and Moulupoulos and theessential features for a viable PCAD. We believe thatthe IABP, Impella, TandemHeart, and ECMO fulfilleach criterion to some degree. It should no longerbe a case of determining which device is superior.There should be a shift in emphasis moving forwardto identify the patient, anatomic, hemodynamic,

Myat et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5
Hemodynamic Support for High-Risk PCI F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4
242
and procedural characteristics that signal adjunctiveMCS may be necessary, to prepare the subject andcatheterization laboratory accordingly, and thento perform the PCI with the knowledge that a step-wise increment in hemodynamic support can befacilitated.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Deepak L. Bhatt, Brigham and Women’s HospitalHeart & Vascular Center, 75 Francis Street, Boston,Massachusetts 02115. E-mail: [email protected].
RE F E RENCE S
1. Peterson ED, Dai D, DeLong ER, et al.Contemporary mortality risk prediction forpercutaneous coronary intervention: resultsfrom 588,398 procedures in the NationalCardiovascular Data Registry. J Am Coll Cardiol2010;55:1923–32.
2. Brennan JM, Curtis JP, Dai D, et al. Enhancedmortality risk prediction with a focus on high-riskpercutaneous coronary intervention: results from1,208,137 procedures in the NCDR (National Car-diovascular Data Registry). J Am Coll Cardiol Intv2013;6:790–9.
3. Hochman J, Sleeper L, Webb J, et al. Earlyrevascularization in acute myocardial infarctioncomplicated by cardiogenic shock. N Engl J Med1999;341:625–34.
4. Van ’t Hof AW, Liem AL, de Boer MJ,Hoorntje JC, Suryapranata H, Zijlstra F.A randomized comparison of intra-aortic balloonpumping after primary coronary angioplasty inhigh risk patients with acute myocardial infarction.Eur Heart J 1999;20:659–65.
5. Kantrowitz A, Tjonneland S, Freed P, Phillips SJ,Butner A, Sherman J. Initial clinical experiencewith intraaortic balloon pumping in cardiogenicshock. JAMA 1968;203:113–8.
6. Hochman J, Sleeper LA, White HD, et al.One-year survival following early revasculariza-tion for cardiogenic shock. JAMA 2001;285:190–2.
7. Hochman J, Sleeper LA, Webb J, et al. Earlyrevascularization and long-term survival incardiogenic shock complicating acute myocardialinfarction. JAMA 2006;295:2511–5.
8. Sanborn TA, Sleeper LA, Bates ER, et al. Impactof thrombolysis, intra-aortic balloon pump coun-terpulsation, and their combination in cardiogenicshock complicating acute myocardial infarction:a report from the SHOCK trial registry. J Am CollCardiol 2000;36:1123–9.
9. Hochman JS, Buller CE, Sleeper LA, et al.Cardiogenic shock complicating acute myocardialinfarction-etiologies, management and outcome:a report from the SHOCK trial registry. J Am CollCardiol 2000;36:1063–70.
10. Fincke R, Hochman JS, Lowe AM, et al. Cardiacpower is the strongest hemodynamic correlateof mortality in cardiogenic shock: a report fromthe SHOCK trial registry. J Am Coll Cardiol 2004;44:340–8.
11. Reynolds HR, Hochman JS. Cardiogenic shock:current concepts and improving outcomes.Circulation 2008;117:686–97.
12. De Silva K, Foster P, Guilcher A, et al. Coronarywave energy: a novel predictor of functional
recovery after myocardial infarction. Circ Car-diovasc Interv 2013;6:166–75.
13. Clauss R, Birtwell W, Albertal G, et al. Assistedcirculation. I. The arterial counterpulsator.J Thorac Cardiovasc Surg 1961;41:447–58.
14. Kantrowitz A. Experimental augmentation ofcoronary flow by retardation of the arterial pres-sure pulse. Surgery 1953;34:678–87.
15. Myat A, Mcconkey H, Chick L, Baker J,Redwood SR. The intra-aortic balloon pump inhigh-risk percutaneous coronary intervention: iscounterpulsation counterproductive? Interv Car-diol 2012;4:211–34.
16. Kolyva C, Pantalos GM, Pepper JR, Khir AW.How much of the intraaortic balloon volume isdisplaced toward the coronary circulation?J Thorac Cardiovasc Surg 2010;140:110–6.
17. Kern MJ, Aguirre F, Bach R, Donohue T,Siegel R, Segal J. Augmentation of coronary bloodflow by intra-aortic balloon pumping in patientsafter coronary angioplasty. Circulation 1993;87:500–11.
18. Kimura A, Toyota E, Lu S, et al. Effects ofintraaortic balloon pumping on septal arterialblood flow velocity waveform during severe leftmain coronary artery stenosis. J Am Coll Cardiol1996;27:810–6.
19. Yoshitani H, Akasaka T, Kaji S, et al. Effects ofintra-aortic balloon counterpulsation on coronarypressure in patients with stenotic coronary ar-teries. Am Heart J 2007;154:725–31.
20. Takeuchi M, Nohtomi Y, Yoshitani H,Miyazaki C, Sakamoto K, Yoshikawa J. Enhancedcoronary flow velocity during intra-aortic balloonpumping assessed by transthoracic Dopplerechocardiography. J Am Coll Cardiol 2004;43:368–76.
21. Kern MJ, Aguirre F, Tatineni S, et al. Enhancedcoronary blood flow velocity during intraaorticballoon counterpulsation in critically ill patients.J Am Coll Cardiol 1993;21:359–68.
22. Curtis JP, Rathore SS, Wang Y, Chen J,Nallamothu BK, Krumholz HM. Use and effective-ness of intra-aortic balloon pumps among patientsundergoing high risk percutaneous coronaryintervention: insights from the National Cardio-vascular Data Registry. Circ Cardiovasc Qual Out-comes 2012;5:21–30.
23. Zeymer U, Bauer T, Hamm C, et al. Use andimpact of intra-aortic balloon pump on mortalityin patients with acute myocardial infarctioncomplicated by cardiogenic shock: results of theEuro Heart Survey on PCI. EuroIntervention 2011;7:437–41.
24. Mishra S, Chu WW, Torguson R, et al. Role ofprophylactic intra-aortic balloon pump in high-riskpatients undergoing percutaneous coronaryintervention. Am J Cardiol 2006;98:608–12.
25. Brodie BR, Stuckey TD, Hansen C, Muncy D.Intra-aortic balloon counterpulsation beforeprimary percutaneous transluminal coronaryangioplasty reduces catherterization laboratoryevents in high-risk patients with acutemyocardial infarction. Am J Cardiol 1999;84:18–23.
26. Briguori C, Sarais C, Pagnotta P, et al. Electiveversus provisional intra-aortic balloon pumping inhigh-risk percutaneous transluminal coronary an-gioplasty. Am Heart J 2003;145:700–7.
27. Ishihara M, Sato H, Tateishi H, Uchida T,Dote K. Intraaortic balloon pumping as the post-angioplasty strategy in acute myocardial infarc-tion. Am Heart J 1991;122:385–9.
28. Urban PM, Freedman RJ, Ohman EM, et al. In-hospital mortality associated with the use of intra-aortic balloon counterpulsation. Am J Cardiol2004;94:181–5.
29. Ferguson JJ, Cohen M, Freedman RJ, et al. Thecurrent practice of intra-aortic balloon counter-pulsation: results from the Benchmark Registry.J Am Coll Cardiol 2001;38:1456–62.
30. Stone GW, Ohman EM, Miller MF, et al.Contemporary utilization and outcomes of intra-aortic balloon counterpulsation in acutemyocardial infarction. J Am Coll Cardiol 2003;41:1940–5.
31. Barron HV, Every NR, Parsons LS, et al. The useof intra-aortic balloon counterpulsation in patientswith cardiogenic shock complicating acutemyocardial infarction: data from the NationalRegistry of Myocardial Infarction 2. Am Heart J2001;141:933–9.
32. Stone G, Marsalese D, Brodie BR, et al.A prospective, randomized evaluation of prophy-lactic intraaortic balloon counterpulsation in highrisk patients with acute myocardial infarctiontreated with primary angioplasty. J Am Coll Car-diol 1997;29:1459–67.
33. Ohman EM, George BS, White CJ, et al., theRandomized IABP Study Group. Use of aorticcounterpulsation to improve sustained coronaryartery patency during acute myocardial infarction.Results of a randomized trial. Circulation 1994;90:792–9.
34. Perera D, Stables R, Thomas M, et al. Electiveintra-aortic balloon counterpulsation duringhigh-risk percutaneous coronary intervention: arandomized controlled trial. JAMA 2010;304:867–74.

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5 Myat et al.F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4 Hemodynamic Support for High-Risk PCI
243
35. Perera D, Stables R, Clayton T, et al. Long-term mortality data from the balloon pump-assisted coronary intervention study (BCIS-1): arandomized, controlled trial of elective ballooncounterpulsation during high-risk percutaneouscoronary intervention. Circulation 2013;127:207–12.
36. Perera D, Lumley M, Pijls N, Patel MR. Intra-aortic balloon pump trials: questions, answers, andunresolved issues. Circ Cardiovasc Interv 2013;6:317–21.
37. Patel MR, Smalling RW, Thiele H, et al. Intra-aortic balloon counterpulsation and infarct size inpatients with acute anterior myocardial infarctionwithout shock: the CRISP AMI randomized trial.JAMA 2011;306:1329–37.
38. Boersma E, Maas AC, Deckers JW,Simoons ML. Early thrombolytic treatment inacute myocardial infarction: reappraisal of thegolden hour. Lancet 1996;348:771–5.
39. Boersma E. Does time matter? A pooledanalysis of randomized clinical trials comparingprimary percutaneous coronary intervention andin-hospital fibrinolysis in acute myocardial infarc-tion patients. Eur Heart J 2006;27:779–88.
40. Schomig A, Mehilli J, Antoniucci D, et al.Mechanical reperfusion in patients with acutemyocardial infarction presenting more than 12hours from symptom onset. JAMA 2005;293:2865–72.
41. Thiele H, Zeymer U, Neumann F-J, et al.Intraaortic balloon support for myocardial infarc-tion with cardiogenic shock. N Engl J Med 2012;367:1287–96.
42. Goldberg RJ, Spencer FA, Gore JM, Lessard D,Yarzebski J. Thirty-year trends (1975 to2005) in themagnitude of, management of, and hospital deathrates associated with cardiogenic shock in patientswith acute myocardial infarction: a population-based perspective. Circulation 2009;119:1211–9.
43. Werdan K, Gielen S, Ebelt H, Hochman JS.Mechanical circulatory support in cardiogenicshock. Eur Heart J 2013;35:156–67.
44. O’Gara PT, Kushner FG, Ascheim DD, et al.2013 ACCF/AHA guideline for the managementof ST-elevation myocardial infarction: a report ofthe American College of Cardiology Foundation/American Heart Association Task Force on PracticeGuidelines. J Am Coll Cardiol 2013;61:e78–140.
45. Steg PG, James SK, Atar D, et al. ESC guide-lines for the management of acute myocardialinfarction in patients presenting with ST-segmentelevation. Eur Heart J 2012;33:2569–619.
46. Remmelink M, Sjauw KD, Henriques JPS, et al.Effects of mechanical left ventricular unloading byImpella on left ventricular dynamics in high-riskand primary percutaneous coronary interventionpatients. Catheter Cardiovasc Interv 2010;75:187–94.
47. Remmelink M, Sjauw KD, Henriques J, et al.Effects of left ventricular unloading by Impellarecover LP2.5 on coronary hemodynamics.Catheter Cardiovasc Interv 2007;70:532–7.
48. Levine GN, Bates ER, Blankenship JC, et al.2011 ACCF/AHA/SCAI guideline for percutaneouscoronary intervention. A report of the American
College of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines andthe Society for Cardiovascular Angiography andInterventions. J Am Coll Cardiol 2011;58:e44–122.
49. Windecker S, Kolh P, Alfonso F, et al. 2014ESC/EACTS guidelines on myocardial revasculari-zation: the Task Force on Myocardial Revasculati-zation of the European Society of Cardiology(ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) developed with thespecial contribution of the European Associationof Percutaneous Cardiovascular Interventions(EAPCI). Eur Heart J 2014;35:2541–619.
50. Anderson JL, Adams CD, Antman EM, et al.2012 ACCF/AHA focused update incorporated intothe ACCF/AHA 2007 guidelines for the manage-ment of patients with unstable angina/non-ST-elevation myocardial infarction: a report of theAmerican College of Cardiology Foundation/American Heart Association Task Force. J Am CollCardiol 2013;61:e179–347.
51. Hamm CW, Bassand J-P, Agewall S, et al. ESCguidelines for the management of acute coronarysyndromes in patients presenting without persis-tent ST-segment elevation: the Task Force forthe management of acute coronary syndromes(ACS) in patients presenting without persistentST-segment elevation. Eur Heart J 2011;32:2999–3054.
52. Lauten A, Engström AE, Jung C, et al. Percu-taneous left-ventricular support with the Impella-2.5-assist device in acute cardiogenic shock:results of the Impella-EUROSHOCK-registry. CircHeart Fail 2013;6:23–30.
53. Seyfarth M, Sibbing D, Bauer I, et al.A randomized clinical trial to evaluate the safetyand efficacy of a percutaneous left ventricularassist device versus intra-aortic balloon pumpingfor treatment of cardiogenic shock caused bymyocardial infarction. J Am Coll Cardiol 2008;52:1584–8.
54. O’Neill WW, Kleiman NS, Moses J, et al.A prospective, randomized clinical trial of hemo-dynamic support with Impella 2.5 versus intra-aortic balloon pump in patients undergoinghigh-risk percutaneous coronary intervention: thePROTECT II study. Circulation 2012;126:1717–27.
55. Thiele H, Lauer B, Hambrecht R, Boudriot E,Cohen HA, Schuler G. Reversal of cardiogenicshock by percutaneous left atrial-to-femoralarterial bypass assistance. Circulation 2001;104:2917–22.
56. Burkhoff D, Cohen H, Brunckhorst C,O’Neill WW. A randomized multicenter clinicalstudy to evaluate the safety and efficacy of theTandemHeart percutaneous ventricular assist de-vice versus conventional therapy with intraaorticballoon pumping for treatment of cardiogenicshock. Am Heart J 2006;152:469.e1–8.
57. Ouweneel DM, Henriques JPS. Percutaneouscardiac support devices for cardiogenic shock:current indications and recommendations. Heart2012;98:1246–54.
58. Kar B, Gregoric ID, Basra SS, Idelchik GM,Loyalka P. The percutaneous ventricular assistdevice in severe refractory cardiogenic shock.J Am Coll Cardiol 2011;57:688–96.
59. Thiele H, Sick P, Boudriot E, et al. Randomizedcomparison of intra-aortic balloon support witha percutaneous left ventricular assist device inpatients with revascularized acute myocardialinfarction complicated by cardiogenic shock. EurHeart J 2005;360:1276–83.
60. Dardas P, Mezilis N, Ninios V, et al. ECMO as abridge to high-risk rotablation of heavily calcifiedcoronary arteries. Herz 2012;37:225–30.
61. Koutouzis M, Kolsrud O, Albertsson P,Matejka G, Grip L, Kjellman U. Percutaneous cor-onary intervention facilitated by extracorporealmembrane oxygenation support in a patient withcardiogenic shock. Hellenic J Cardiol 2010;51:271–4.
62. Jones H, Kalisetti D, Gaba M, McCormick D,Goldberg S. Left ventricular assist for high-riskpercutaneous coronary intervention. J InvasiveCardiol 2012;24:544–50.
63. Westaby S, Anastasiadis K, Wieselthaler GM.Cardiogenic shock in ACS. Part 2: role of me-chanical circulatory support. Nat Rev Cardiol 2012;9:195–208.
64. Teirstein PS, Vogel RA, Dorros G, et al. Pro-phylactic versus standby cardiopulmonary supportfor high risk percutaneous transluminal coronaryangioplasty. J Am Coll Cardiol 1993;21:590–6.
65. Sheu J-J, Tsai T-H, Lee F-Y, et al. Earlyextracorporeal membrane oxygenator-assistedprimary percutaneous coronary interventionimproved 30-day clinical outcomes in patientswith ST-segment elevation myocardial infarctioncomplicated with profound cardiogenic shock. CritCare Med 2010;38:1810–7.
66. Arlt M, Philipp A, Voelkel S, et al. Early ex-periences with miniaturized extracorporeal life-support in the catheterization laboratory. Eur JCardiothorac Surg 2012;42:858–63.
67. Chen J-S, Ko W-J, Yu H-Y, et al. Analysis of theoutcome for patients experiencing myocardialinfarction and cardiopulmonary resuscitation re-fractory to conventional therapies necessitatingextracorporeal life support rescue. Crit Care Med2006;34:950–7.
68. Hsu P-C, Lin T-H, Lu Y-H, et al. Unprotectedleft main coronary artery stenting under extra-corporeal membrane oxygenation support in apatient with high-risk acute myocardial infarction.Acta Cardiol Sin 2009;25:98–101.
69. Ricciardi M, Moscucci M, Knight B, Zivin A,Bartlett R, Bates E. Emergency extracorporealmembrane oxygenation (ECMO)-supportedpercutaneous coronary interventions in the fibril-lating heart. Catheter Cardiovasc Interv 1999;48:402–5.
70. Shammas N, Roberts S, Early G. Extracorpo-real membrane oxygenation for unprotected leftmain stenting in a patient with totally occludedright coronary artery and severe left ventricular.J Invasive Cardiol 2002;14:756–9.
71. Taub J, L’Hommedieu B, Raithel S, et al.Extracorporeal membrane oxygenation for percu-taneous coronary angioplasty in high risk patients.ASAIO Trans 1989;35:664–6.
72. Fesc GV, Akret C, Bach V, et al. Assistancecirculatoire extracorporelle percutanée dans les

Myat et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 8 , N O . 2 , 2 0 1 5
Hemodynamic Support for High-Risk PCI F E B R U A R Y 2 0 1 5 : 2 2 9 – 4 4
244
défaillances hémodynamiques aiguës graves:expérience monocentrique chez 100 patientsconsécutifs [Percutaneous extracorporeal lifesupport in acute severe hemodynamic collapses:single centre experience in 100 consecutivepatients]. Can J Cardiol 2009;25:e179–86.
73. Yamauchi T, Masai T, Takeda K, Kainuma S,Sawa Y. Percutaneous cardiopulmonary supportafter acute myocardial infarction at the left maintrunk. Ann Thorac Cardiovasc Surg 2009;15:93–7.
74. Sjauw KD, Engström AE, Vis MM, et al.A systematic review and meta-analysis of intra-aortic balloon pump therapy in ST-elevationmyocardial infarction: should we change theguidelines? Eur Heart J 2009;30:459–68.
75. Bahekar A, Singh M, Singh S, et al. Cardiovas-cular outcomes using intra-aortic balloon pumpin high-risk acute myocardial infarction withor without cardiogenic shock: a meta-analysis.J Cardiovasc Pharmacol Ther 2012;17:44–56.
76. Cassese S, de Waha A, Ndrepepa G, et al. Intra-aortic balloon counterpulsation in patients withacute myocardial infarction without cardiogenic
shock. A meta-analysis of randomized trials. AmHeart J 2012;164:58–65.e1.
77. Chen S, Yin Y, Ling Z, Krucoff MW. Short andlong term effect of adjunctive intra-aortic balloonpump use for patients undergoing high riskreperfusion therapy: a meta-analysis of 10 inter-national randomised trials. Heart 2013;100:303–10.
78. Romeo F, Acconcia MC, Sergi D, et al. Lack ofintra-aortic balloon pump effectiveness in high-risk percutaneous coronary interventions withoutcardiogenic shock: a comprehensive meta-analysisof randomised trials and observational studies. IntJ Cardiol 2013;30:1783–93.
79. Cheng JM, den Uil CA, Hoeks SE, et al.Percutaneous left ventricular assist devices vs.intra-aortic balloon pump counterpulsation fortreatment of cardiogenic shock: a meta-analysis ofcontrolled trials. Eur Heart J 2009;30:2102–8.
80. Desai NR, Bhatt DL. Evaluating percutaneoussupport for cardiogenic shock: data shock andsticker shock. Eur Heart J 2009;30:2073–5.
81. Cutlip DE, Windecker S, Mehran R, et al. Clin-ical end points in coronary stent trials: a case for
standardized definitions. Circulation 2007;115:2344–51.
82. Mehran R, Rao SV, Bhatt DL, et al. Standardizedbleeding definitions for cardiovascular clinical trials:a consensus report from the Bleeding AcademicResearch Consortium. Circulation 2011;123:2736–47.
83. Kappetein AP, Head SJ, Généreux P, et al.Updated standardized endpoint definitions fortranscatheter aortic valve implantation. J Am CollCardiol 2012;60:1438–54.
KEY WORDS diastolic augmentation,extracorporeal membrane oxygenation,high-risk PCI, intra-aortic balloon pump,mechanical circulatory support
APPENDIX For supplemental tables,references, and a figure, please see theonline version of this article.
Go to http://cme.jaccjournals.orgto take the CME quiz for thisarticle.