Embed Size (px)
Citation preview

Develop. Med. Child Neurol. 1982, 24, 752-770
Perceptual, Motor and Attentional Deficits in Seven-year-old Children: Background Factors
Christopher Gillberg Peder Rasmussen
Introduction The large and ever-increasing number of
studies on the long-term outcome for children ‘at risk’ neurologically (e.g. Neligan et a/. 1976, Drillien 1980, Rubin and Balow 1980) has demonstrated beyond question that non-optimal pregnancy f a c t o r s , i n t r a p a r t a l a n d n e o n a t a l complications, as well as neurological abnormalities in infancy, eventually may interfere with the child’s no rma l development. They may cause (or rather, be factors in the aetiology of) not only major neurological handicaps but also learning disabilities, motor problems and behavioural difficulties, often classified together under the heading ‘minimal brain dysfunct ion’ ( M B D ) . However , t he contributory effects of other factors, such as heredity and psychosocial conditions, are less well understood. Many studies have purported to investigate aetiological factors in MBD, but the definitions used are vague and the populations of children extremely heterogenous (see Rutter 1982 for overview).
The present study reports on neuro- pathogenic, hereditary and psychosocial background factors in a total population sample of children with strictly-defined MBD syndromes. The uniform organisation and reporting of medical data in Swedish
obstetric and neonatal departments is a special advantage in studies of this kind.
Definition MBD is regarded as an operational
diagnosis, requiring signs of both attentional deficit and fine motor, gross motor or perception dysfunction. It is applied only to children who do not have obvious mental retardation or cerebral palsy. This definition is in agreement with the one formulated by Clements (1966) and with the Scandinavian concept of MBD as outlined by various authors (Hagberg 1975, Korhonen and Sillanpaa 1976, Frisk 1979).
Method A total of 138 children were given
extensive neuropsychiatric examinations at age seven years and diagnosed in accordance with strict criteria as suffering from minimal brain dysfunction (MBD), motor perception dysfunction (MPD), attention deficit disorder (ADD), or as having none of these disorders. These 138 children had participated originally in a population study of six-year-old children in public pre-schools in Gothenburg, which are attended by almost 95 per cent of children in that age-group. This initial study consisted of a simple yes/no
~
Correspondence to Dr. C . Gillberg, Torild Wulffsgatan 41, S-413 19 Goteborg, Sweden.
752

CHRISTOPHER GILLBERG
. . . . . . . . .. :*+*. &I-
! 8 51;: 2 g :caw:: k ? * ' * a w ; pc :: 8 $ .. . . . . . . . .
PEDER RASMUSSEN
All six-year-old chi ldren in public p r e - schools in Gothenburg participating in questionnaire screening study (N = 3448)
questionnaire relating to five areas of development: behaviour problems/ attentional deficit signs, fine motor, gross motor, speech/language and perceptual problems. The questionnaires were completed by pre-school teachers for 72 per cent of the target group. (For details see Gillberg et al. 1982a, Gillberg and Rasmussen 1982.) The mean inter-rater reliability for the questionnaire, as judged by a Pearson r=0.91 (N=26, p<O*OOl). The large number of unanswered questionnaires was mainly accounted for by teachers' reluctance to participate, but it is argued elsewhere that this was unlikely to have a disproportionate effect on children with MBD (Gillberg et a/. 1982~).
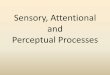
Questionnaires were completed for 3448 children (Fig. 1). A factor analysis of the 34
survey questions was performed, using varimax rotation (Heal th Sciences Computing Facility (1977)). Only factors with eigenvalues of 1.0 or more were included. Five clinically relevant factors were found: attention deficit/distracti- bility, conduct problem, motor dys- function 1, motor dysfunction 2 and conceptualisation dysfunction factor. These together accounted for 40 per cent of the total variance.
Of the 3448 children, 340 showed pre- school signs of abnormality in the areas of attention deficit/distractibility or conduct problems, combined with abnormalities in at least one of the other three relevant areas. 141 of these children were then selected and sampled for extensive neuropsychiatric study in the following
Fac tor analysis - selection criteria high/low -load index groups
Random control group
Sampling
I I 31 I 309 I
Attrition
Study groups
Fig. 1. Sampling,selection andstudygroups. *Eight childreninrandomcontrolgroup were foundinindexgroup.
753

PERCEPTUAL, MOTOR A N D ATTENTIONAL DEFICITS IN SEVEN-YEAR-OLDS
way. 31 were selected to represent all children who had shown either ‘abnorm- ality’ (i.e. one or two ‘symptoms’, depend- ing on clinical relevance and frequency distribution) in all five factor categories, or at least one ‘symptom’ in all five areas of the original questionnaire. Nine of these children were excluded or failed to participate for various reasons, leaving 22 in this high-load index group. According to a list of random numbers, another sample of 81 children was drawn from the remaining 309, but 21 failed to participate: thus 60 children remained in the low-load index group. Finally, 100 children were randomly selected from all 3448 with completed questionnaires. Eight of these were found in the index groups. 75 of the remaining 92 children were contacted, 59 of whom (the control group) finally took part in the extended study.
During the year following the questionnaire study, all 141 children in the extended study were examined blindly (i . e. without knowledge of which group they belonged to) by a research team consisting of two child psychiatrists, a child neurologist, a child physiotherapist and a child psychologist. The mean age of the children at the time of examination was 7 . 5 f 0 . 3 years (range 7 . 0 to 7.9, except for one girl who was 8 . 4 years old). EEG recordings were obtained for 106 of the children (for details see Gillberg et al. 19826). Diagnostic procedures a re described in the Appendix.
Three boys with mental retardation (wSC results and clinical assessment) were excluded at this stage, so the total number left for analysis in the present study was reduced to 138.
Study groups The 138 children were subdivided as
follows: (a) MBD group: 42 children (33 boys, nine girls) were referred to this group, of whom
28 (2 1 boys, seven girls) were diagnosed as having mild to moderate MBD and 14 (12 boys, two girls) as having severe MBD. One girl with marked attention deficit disorder and marked motor perceptual dysfunction was excluded from this group because her parents were in the midst of a difficult divorce at the time of the examination, which may have been a factor in her attention deficit. She was referred instead to the MPD group. (b) MPD group: seven children (four boys, three girls) were referred to this group, two of whom were in the original control group. All had marked fine or gross motor dysfunction o r marked perception dysfunction. Apart from the girl referred to above, none had marked signs of attention deficit disorder. (c) A D D group: 12 children (10 boys, 2 girls), four of whom had been in the control group, were referred to this group with attention deficit disorder, but without marked signs of motor or perception dysfunction. (d) COMP I group: the first of three comparison groups consisted of the children in the original control group, excluding those with a diagnosis of MBD (two). The total number in this group was 57 (28 boys, 29 girls). (el COMP 2 group: the second comparison group was made up of the children in the original control group, excluding two with a diagnosis of MBD, two with MPD and four with ADD, leaving a total of 51 children. If) COMP 3 ,Froup: the third comparison group was made up of all the original 138 children, except those with diagnoses of MBD, MPD or ADD. There were 77 children in this group (45 boys, 32 girls). The group thus included children from both the original index and the control groups.
Background and associated factors Pregnancy, obstetrical and medical
records were collected and examined. 754

CHRISTOPHER GILLBERG PEDER RASMUSSEN
TABLE I Clusters of background and psychosocial factors
analysed Factor Optimal Score
Pmnatal Maternal age Parity Abortions in history Bleedings in pregnancy Severe infection in pregnancy Gcneralized oedema Albuminuria Blood pressure Psychiatric specialist care Maternal diabetes Medication Gestational age (weeks) Smallness for gestational age
Twins o r multiple birth Breech or foot presentation Vacuum extraction Epidural anaesthesia Apgar score Cord prolapse/around neck/ knot Amniotic Huid Child severely traumatized
Pprfnatal
(fractures. lots of petechiae) Neonatal
Respiratory distress Septicaemia/meningitis Hyperbilirubinemia,
non-treated requiring phototherapy requiring transfusion
Anaemia, requiring transfusion Irritable infant/floppy infant Difficulties regulating temperature Cljnical 'dysmaturity' Oxygen treatment >30%
Po.stnaral Encephalitis Meningitis Convulsions Concussion
Spcech-language retardation* Hyperactivity** Learning disorder* Clumsiness (motor)* Left-handedness* Delayed onset puberty***
Rrar-inr condition s Inconsistency Parents disagree LaisseL-faire attitude Mother unawarc of child's
If l,,.(YlI lor),
interest5 ' 7i.ouh/cj\omi,' diilil ixtin,y
'Problematic child' 'Child causes larnily upset' 'Ditficulties brinrine up'
20-30 1-2 0-2
absent absent absent absent
<95/140 no
absent < I week
36-4 1 no
no no no no
9-10 no
clear no
absent absent
absent absent absent absent
n o no no no
absent absent absent absent
absent absent absent absent absent absent
no-rarely no-rarely
n o
no
no-only a little no-only a little no-onlv a little
Score 0 wah given tor cach tactor with optimal conditions. score 1 for each lactor with nonoptimal conditions. "I'irst-degree relative\ only: ""male Iirst-degree relatives only (reporting i n females unlikely); ***al l relatives.
Three children had been born abroad and records were not available. The questionnaire giving details of the child's health and development, as well as the information obtained during direct interview with the mother, were reviewed to analyse background and associated fact ors.
Table I shows the clusters of back- ground and psychosocial fac tors studied. Non-optimal scores for prenatal, perinaral and neonatal conditions (according to medical-record data) were calculated on the basis of a modified version of the system suggested by Prechtl and colleagues (Prechtl 1968, Michaelis et al. 1979). Non-optimal postnatal, potentially CNS-damaging factors were assessed on the basis of interview data from the mother, verified by medical- record data, and neurodevelopmental hereditary factors on the basis of interview data alone. Throughout, minor physical anomalies were assessed in accordance with the method described by Waldrop and Halverson (1971).
A cluster of non-optimal rearing conditions was formed. The Graffar( 1956) classification system was used, which takes account of educational and occupational level of both parents plus number of rooms per person. In some of the analyses the five-grade version of this classification system was used, but in others we used a three-grade version in which social classes I1 and I11 are treated as one class and social classes IV and V as another. Information about 'social problem area' (area frequency of registrations in the social register) was obtained from the local social authorities. Maternal stress scores were calculated in accordance with the method described by Mendeloff et al. (1970).
Finally, a rating as to whether the child was regarded as 'troublesome' or not was made o n the basis of three questions put to the mother.
755

TA
BL
E 1
1 B
ackg
roun
d fa
ctor
st
~ ~~
~
~
GR
OU
PS
Bac
kgro
und
facr
or
(a)
(b)
(Ci
(4
(e)
(0
p le
vel
of
drff
eren
ces$
A
DD
C
OM
Pl
CO
MP
2
CO
MP
3 M
BD
M
PD
(N
=42
) (N
=7
) (N
=12
) (N
=57
) (N
=51
) (N
=77
) <O
1
<O
05
<0
01
<O
001
Boy
:&
rati
o Po
siti
on i
n si
bshi
p N
umbe
r ch
ildr
en i
n fa
mily
O
nly
chil
d (%
) M
ater
nal
age
at b
irth
of
child
N
on-o
ptim
al h
ered
ity
Lef
t-ha
nded
ness
*(R
) L
earn
ing
diso
rder
s*(%
) H
yper
kine
sis*
*('%
) D
elay
ed o
nset
pub
erty
***(
'% 1
Non
-opt
imal
pre
-, p
eri-
or
neon
atal
fac
tors
Pren
atal
fac
tors
Intr
apar
tal
fact
ors
Neo
nata
l fa
ctor
s B
irth
wei
ght
Non
-opt
imal
pos
tnat
al f
acto
rs
Min
or p
hysi
cal
anom
alie
s M
onth
s br
east
-fee
ding
St
arte
d w
alki
ng (
mon
ths)
3.7:
1 2
.1f1
.1
2.5
i 1.1
12
26
.5 i
5.3
2
-Ok
1.7
31
60
41
4- l
i2.0
3.0
+1
.5
0.4
f0.R
0
.6k
1.0
33
28i6
01
0.3
f0-6
2
-7i-
3.6
2
.5i2
.4
13
.1k
2-8
in
1.3:
l 2
.05
0.8
2
-65
1.1
14
2
3.6
i 3.4
I -
4i
1.0
29
29
0 43
3-7
iO.8
3-7
i0.R
0 0 40
5754
50
0 1
.7i0
.8
1.7
11
.6
12
.7t0
-8
5,O
:I 2
-Ok
0.7
2
.3k
0.9
17
2
7.4
iR.5
I .
0i0
.9
17
33
25 0
2.8
i2. I
2.3
k1
.4
0.3
i 0
.9
0.3i0.5
3269
k 38
7 0
,35
0-5
I-
3i2
.0
2.2
i1.5
in
.9t
1-0
O.9
:I
1-9
iO.8
2
.5iO
.X
2 26
.4+
5. I
0
.9*1
:1
14
24
14 9
2-6
k1
.3
2- 1
i0.9
0.3
10
.6
0.2
+0
'h
3497
i 60
I 0
-2fW
4
0.8
i2.0
2
-9k
2.2
I2
-2i2
4
1.5:
1 I.
9k
0.9
2
.5t0
-9
6 26
. I k
5.3
0
.95
1.2
I6
25
19
6 2
.6i1
-3
2.1
31
-0
0.3
i0-6
0
.3i0
.6
35
14
i 572
0
2k
0.5
I.
Oi2
-3
3- 1
k2
.2
I2.0
i2- 1
a/f -
-
-
-
-
a/d
a/d
b/c,
d
-
-
b/c -
ale
. t
e/b.
f/h
-
-
-
a/f
>
0
tCro
uu m
eans
+st
anda
rd d
evia
tion
s un
less
sho
wn
othe
rwis
e.
:Fi\h
e;
non-
para
met
ric
perm
utat
ion
test
. 1
*Fir
st-d
egre
e re
lativ
es:
**m
ale
fir
st-d
egre
e re
lativ
es:
***a
ll r
elat
i\es
. m 22
Psyc
ho-s
ocia
l con
ditio
nst
2 T
AB
LE
111
4
(a)
(b)
(0
(4
(e)
If)
p le
vel
of
diff
eren
ces:
v1
m
AD
D
CO
MP
l C
OM
P2
C
OM
P3
MB
D
MPD
(N
=42
) (N
=7
) (N
=12
) (N
=57
) (N
=51
) (N
=77
) <
0.1
<
O.0
5 <
0.0
1
<O.0
01
2 ? M
othe
r ps
ych.
ill
child
's 1s
t ye
ar (
%)
31
29
8 16
18
21
M
othe
r ps
ych.
ill
at e
xam
inat
ion (q)
45
29
25
16
16
13
-
-
a/d,
e
a/f
> F1 <
rn
-
-
-
-
Mat
erna
l so
cial
str
ess
scor
e 8
.3k
5-I
4
.4+
2.
I 8
.0i3
-0
4.7
k3
.3
4-6
i3.2
5
.0k
3.3
-
a/b,
c/
b c/
e, f
a/
d, e
, f
One
-par
ent
fam
ily ((5 )
21
14
50
14
12
17
-
c/f
c/e
Soci
al c
lass
2
.8+
0.5
2
.9+
0.4
2
.8+
0-4
2
.5k
0.6
2
-5f0
.h
2-5
20
.7
b/e,
c/f
a/
d, c
/e
a/c,
I
r
-
-
c/e.
f
a/d,
f
a/e
-
Soci
al p
robl
em a
rea
(Q)
48
29
50
18
14
IX
Livi
ng in
ten
emen
t ho
use (r
4 ) 71
43
83
47
45
49
Day
-nur
sery
car
e: f
rom
3rd
yea
r ('
i )
26
0 17
9
8 in
-
a/d,
e,
f -
a/b
a/d,
e, f
-
-
c/e,
r -
-
-
22
25
a/e.
f. c
/b
a/d
from
4th
yea
r (4)
40
0 42
21
N
on-o
ptim
al r
eari
ng c
ondi
tion
s 0
.9il
-2
0
.6k
1.0
0
.7k
O-7
0
.2i0
.5
0.l
iO.4
0
-2k
0.5
-
c/f
c/c
a/d.
e.
I T
roub
leso
me
chil
d I-
Xil
.3
1.1
f0.9
I.
Oil
.0
0-5
iO.8
0
.5i-
0.7
0
.hi0
-9
a/c.
b/e
-
-
a/d.
e.
I ~
~ ~
__
_
~~~~
~
tGro
up m
eans
ista
ndar
d de
viat
ions
unl
ess
show
n ot
herw
ise
{ :F
ishe
r no
n-pa
ram
etri
c pe
rmut
atio
n te
qt

CHRISTOPHER GILLBERG PEDER RASMUSSEN
S tat is tical methods Fisher’s non-parametric permutation
test was used for univariate statistical analyses (Bradley 1968). In the analyses of background factors the stepwise regression techniques described by Draper and Smith (1966) were used. A significance level of 0 . 1 was used. Some of the variables (dependent as well as independent) were of a categorical nature, and this method is not considered the most appropriate for such variables. However, if the results of the regression analysis are verified by non- parametric partial correlation analysis (Mantel 1963)-as wasdonehere-stepwise regression indeed may be one of the best ways of finding the important background variables. In this latter analysis, the influence of single factors found by regression technique was evaluated by keeping the remaining factors constant. Each factor found was tested separately. A significance level of 0 . 1 was required.
A great amount of data is presented in the Results section, so for the sake of brevity these data are presented in tables. Pair-wise tests of statistical significance are used in order t o facilitate the reader’s evaluation of differences. Caution is warranted, of course, in the interpretation of these results because of the number of tests made. However, the number of significant differences by far outnumber the differences which might have been found by chance alone. Use of anlaysis of variance instead would have risked missing any ‘inherent logic’ in the material.
Results For most of the background and
associated factors studied boys and girls were about equally affected, therefore subdivision according t o sex has not been made in the tables.
Familial-hereditary factors There was a marked preponderance of
boys in both the M B D and A D D groups (Table 11). The difference was statistically significant between the M B D group and all the comparison groups.
There was a clear tendency for the M B D children t o be only children. Those with A D D also tended to be only children more often than comparison children.
Non-optimal hereditary factors (especi- ally left-handedness, reading-writing difficulties and hyperkinesis) were more prevalent in the M B D group than in the comparison groups. In 18 per cent of the M B D cases (N = 39, data missing in three cases) there were first-degree relatives who were left-handed and had reading-writing difficulties. The corresponding figure in the comparison groups was 4 per cent. The difference between the M B D group and the COMP 3 group was statistically significant (p<O.O5). It is worth mentioning that family size in M B D cases was equal to that in the comparison groups, and that the mean age of brothers and sisters was fairly equal in the different groups. N o major distortion of results would be likely therefore if siblings were included in the study of ‘first-degree heredity’-as was done in all instances unless otherwise stated-even if some of the variables studied are age-dependent. Delayed onset of puberty had occurred in close relatives of three of the seven cases with MPD, but much less often in the other groups.
Non-optimal prenatal, perinatal and neonatal factors
Non-optimal prenatal, perinatal and neonatal factors occurred more often in the MBD and MPD groups than in the comparison groups. The prenatal non- optimality score was particularly high in the MPD group, whereas the A D D group s h o w e d n o i n c r e a s e in p r e n a t a l ‘pathology’. Non-op t ima l neona ta l factors-especially clinical signs of ‘dysmaturity’, which had been present in
757

PERCEPTUAL, MOTOR A N D ATTENTIONAL DEFICITS IN SEVEN-YEAR-OLDS
31 per cent of MBD cases compared with 9 to 10 per cent in the three comparison groups (p<O.OI, 0 .05 a n d 0.01, respectively)-were much more common in the MBD group than in the comparison groups. Neonatal complications had not been common in the MPD and ADD groups.
Birthweight was somewhat lower in the MBD and ADD groups than in the comparison groups, but the difference did not quite reach statistical significance.
Minor physical anomalies Minor physical anomaly scores were
much higher in the MBD group than in all the comparison groups (p<0.01) .
Breast-feeding There were no clear-cut differences
between the groups with regard to length of breast-feeding period, but there was a tendency for the MBD, MPD and ADD groups to be at a disadvantage. However, when these groups were treated as one, the difference between this index group and the COMP 3 group was significant at the 5 per cent level, both as regards mean number of total months breast-feeding and mean number of months exclusive breast- feeding ( 2 . 2 k 2 . 2 and 1 . 7 k I . 7 ( N =61) vs 3 . 1 k 2 . 2 and 2 . 4 + 2 . 0 (N=77)).
Age at walking Children with MBD were slower to start
walking than COMP 3 group children (p<O.O5). Children with ADD were two months quicker in this respect ( p < 0 . 0 5 compared with the MBD group), and even showed a tendency to be quicker in starting to walk than comparison children.
Background factors Clear-cut background factors were
found in 71 per cent of the MBD cases. These were either (a) a combination of non-optimal hereditary and prenatal, perinatal and neonatal/postnatal factors
(>2SD above the mean values of the COMP 2 group), which occurred in 17 per cent of the MBD cases; fb) non-optimal hereditary factors alone in 21 per cent; or (c) non- optimal prenatal, perinatal and neonatal/ postnatal factors alone in 33 per cent.
Reasonably plausible background factors were found in a further 19 per cent of the MBD cases. These cases had values 2 1 SD above the mean of the COMP 2 group for two of the following four factors: non- optimal hereditary factors, prenatal, perinatal and neonatal factors, postnatal factors and minor physical anomaly scores.
Psychosociai conditions Mothers of MBD, MPD and ADD children
had not been significantly more often treated for psychiatric illness during the child’s first year of life than mothers of comparison children (Table 111). However, mothers of MBD children had sought medical help for psychiatric problems in the 12 months preceding the children’s examinations more often than mothers of comparison children.
Mothers of MBD and ADD children had significantly raised stress scores in relation to mothers of MPD and comparison children.
One-parent families were much more common in the ADD group than in the comparison groups. No significant differences were found with respect to frequency of divorce, but MBD and ADD children were more likely to have divorced parents than the other children.
Social class was lower in all three index groups than in the comparison groups. MBD and ADD children lived in social- p r o b l e m a r e a s m o r e o f t en t h a n comparison children. I n most cases they lived in tenement houses, which was rare among the other children.
Children in the MBD group had been in full-time day nurseries from an earlier age
758

CHRISTOPHER GILLBERG PEDER RASMUSSEN
and more often than comparison children. There was a similar tendency among ADD children.
Non-optimal rearing conditions were more common and more ‘severe’ in MBD than in comparison children (p<O.OOI). ADD children also had higher scores in this category. MBD children were regarded as ‘troublesome’ by their mothers more frequently than comparison children (p<O.OOl). MPD children also had higher scores in this area, but the difference fell slightly short of statistical significance.
Psychiatric abnormality Marked and definite psychiatricabnorm-
ality was found in two-thirds of MBD children, compared with only 10 to 12 per cent ofcomparison children(Tab1e IV).
WISC performance results A full-scale WISC was not performed, as
the verbal tests were likely to yield unreliable results for immigrant children. wx performance results were much lower in the MBD group than in all other groups (Table IV).
Handedness and MBD The frequency of manifest left-
handedness among MBD children was almost three times that of comparison children (Table IV). All cases of left- handed first-degree relatives in the MBD group were accounted for by mothers or fathers. In some cases siblings were also left-handed.
Two of the six left-handed MBD children (five boys, one girl) had left paroxysmal (sharp wave) abnormalities in their EEGs. These two children, together with three of the remaining left-handed MBD children, had only right-handed first-degree relatives. The sixth child (the only left- handed child considered to suffer from severe MBC) had left-handed first-degree relatives.
All right-handed MBD children with left- handed first-degree relatives (two girls, four boys, none of whom had severe MBD), and all left-handed MBD children with no left-handed first-degree relatives (one girl, four boys, none of whom had severM), had speech-language disorders. 26 per cent of the remaining MBD children showed no signs of speech-language disorder.
Seven of the 12 MBD children witH left- handed first-degree relatives also had first- degree relatives who had, or had had, reading-writing difficulties.
The EEG of one of the four ‘ambidextrous’ MBD children had sharp- wave activity, with left-sided pre- dominance. This child and one other ambidextrous child had no left-handed first-degree relative. In the other two cases the mother or father was left-handed. All four children also suffered from speech- language disorders.
Thirty-two per cent of the MBD children without ‘inverted’ handedness (left- handedness in families of right-handers and vice versa) and without ambidexterity had no speech-language disorder.
As can be seen in Table V, MBD children were right-handed equally of ten, irrespective of heredity. The right-handed MBD children who had a left-handed father or mother had higher scores of non-optimal perinatal factors than right-handed MBD children whose parents were both right- handed (p<O.O5).
Specialist treatment Over-all, almost a third of the index
children had attended child guidance or child psychiatric clinics (Table VI). Almost 60 per cent of MBD children and 33 per cent of ADD children had received treatment by a psychiatrist, speech-therapist or ophthamo- logist on more than one occasion during the year before examination. However, the seven children with MPD had not applied for professional help at all.
759

TABL
E IV
Ass
ocia
ted
fact
ors
at e
xam
inat
iont
GR
OIJ
PS
Ass
ociu
ted
fucl
or
m z
Han
dedn
ess
(%):
'righ
t 16
10
0 92
95
94
91
a/
f a/
d,
e -
-
2
a/b,
b/f
a/
c, d
, e,
f b/
e M
inor
neu
rolo
gica
l dys
func
tion
4
43
~1
5
38+1
1 1
6f7
1
4f7
1
3f6
1
6f9
c/
e -
Mar
ked
psyc
hiat
ric
abno
rmal
ity
($7
~)
69
0 17
11
10
12
a/
c a/
h -
a/d,
e, f
r
WIS
C p
erfo
rman
ce (s
tani
ne)'.
3.
63Z
2.2
5.7
52
.3
6.2+
1-0
6.2
+1
-6
6.2
k1
.6
6.2
*1
-6
-
-
-
a/c,
d, e
, f
3 >
0 rn > z 0 >
4 1
14
0 0
4 4
5 a/
f -
-
-
left
-
-
-
-
ambi
dext
erit
y'
10
0 8
2 2
4
tGro
up m
eans
ksta
ndar
d de
viat
ions
unl
ess
show
n ot
herw
ke.
1 Fis
her
non-
para
met
ric
perm
utat
ion
test
. 1.
WIS
C-t
ests
obt
aine
d: N
=32
. 3.
I I
. 50,
45
and
65 r
espe
ctiv
ely.
2.
In
five
cas
es re
sult
s of
WIS
C te
sts
wer
e co
nsid
ered
unr
elia
ble
beca
use
of p
sych
osis
(tw
o bo
ys).
seve
re de
pres
sion
(tw
o bo
ys) a
nd e
xtre
me
lang
uage
diff
icul
ties
of o
nr
imm
igra
nt b
oy.
3. A
mbi
dext
erit
yzus
es r
ight
han
d in
tw
o ou
t of
thr
ee o
f ac
tion
s of
wri
ting.
cut
ting
. po
inti
ng.
;
The
se f
ive
case
s ha
d st
anin
e va
lues
of
I to
2. I
f ex
clud
ed,
mea
n va
lue
wou
ld h
ave
been
4'2
k2
. 1
=! 0
2 0
TABL
E VI
Spec
ialis
t tre
atm
ent r
ecei
ved
Spe
cial
is r
GR
OU
PS
(0)
(b)
Id
(4
(el
cn p
leve
l of
diff
eren
cerf
A
DD
C
OM
PI
CO
MP
2 C
O.b
lP3
MB
D
MPD
(N
=42
) (N
=7
) (N
=1
2)
(N=
57
) (N
=5
1)
(N=
77)
<0
.05
<O
.lll
<0
.001
Chi
ld p
sych
iatr
ist
(480)
Spee
ch th
erap
ist (9%)
Oph
thal
mol
ogis
t (70)
Paed
iatr
icia
n/ch
ild
neur
olog
ist (
% 1
Chi
ld p
sych
iatr
ist,
spee
ch
ther
apis
t or
oph
thal
mol
ogis
t in
yea
r pr
ior
to e
xam
inat
ion
(%)
40
0 17
5
4 5
-
-
a/d,
e, f
14
0
17
5 4
5 2
0 0
4 2
3 2
0 0
14
16
13
-
-
-
-
-
-
-
-
-
57
0 33
14
10
13
a/
b -
a/d.
e.
f
$Fis
her
non-
para
met
ric
perm
utat
ion
tcsf

CHRISTOPHER GILLBERG PEDER RASMUSSEN
TABLE V MBD: handedness in family and child and relationship to perinatal
complications
Child uses Perinatal score, Familial handedness lefr right right-handed No.
hand hand? children ~ ~ ~
% % M e a n f S D Father or mother
Father and mother left-handed 8 92 5 . l i 2 . 9 * 12
right-handed 17 83 3 . 5 f 1 . 2 30
*p<O, 5 ; tambidexterous cases are treated here as right-handed.
Background factors according to social class Table VII shows the distribution of
scores for minor neurological dysfunction, non-optimal heredity and prenatal, perinatal and neonatal factors in MBD and COMP 2 group cases according to social class. Frequencies of present psychiatric illness in the mother are shown, as well as mean number of months breast-feeding. Except for psychiatric illness, there was no tendency for background factors to be correlated with social class.
Background factors according to WISC performance resutrs
When the above background factors were grouped according to the results of WISC testing, no clear-cut correlations were seen except for length of breast-feeding period, which had been particularly short in the group with very low WtSc results. When the nine children with MBD and WISC stanine values of 1 were compared for length of breast-feeding period with the remaining WISC-tested children with MBD ( N = 23), the difference was statistically significant (1 '2f 1 . 2 compared with 3 . 3 f 2.8, p < 0.05).
Background factors distinguishing groups All the background factors in Table I1
and those psychosocial factors in Table 111 which showed significance levels of at least 0.01 in the univariate analysis were
76 1
entered into a stepwise regression model in which a significance level of 0 . 1 was used.* Neonatal non-optimal factors and heredity for reading-writing difficulties appeared as distinguishing factors in the comparison between MBD and both COMP 1 and COMP 2 groups (Table VIII). Together with these factors, non-optimal prenatal factors and rearing conditions accounted for 36 per cent of the total variance between MBD and COMP 2 cases. In the comparison between MBD and COMP 1 cases, minor physical anomalies and maternal psychiatric disturbance were the two most discrimi- nating factors, apart from the two mentioned above.
Table IX shows that a later age at walking and increased rate of reading- writing difficulties among first-degree relatives were the two factors that most distinguished the MBD from the ADD group.
There were no significant differences between severe and mild-moderate MBD children with regard to background, psychosocial and associated factors studied. There was a tendency for severe cases to have higher minor physical anomaly scores and to be more troublesome than mild-moderate cases (p<O. 1 in both instances).
*Boy:girl ratio was excluded. T h e factor of 'troublesome child' was also excluded, a s this mirrored the mother's subjective view of the child.

TA
BL
E V
11
Bac
kgro
und
and
asso
ciat
ed fa
ctor
s ac
cord
ing
to s
ocia
l cl
ass?
MB
D
Bac
kyro
und
or a
ssoc
rare
dfar
ror
Soct
al L
IUIJ
I 2
I II
II
I (N
=l)
(N
=3
) (N
=3)
Min
or n
euro
logi
cal
dysf
unct
ion
49 in
4
9i1
5
56
i19
N
on-o
ptim
al h
ered
itar
y fa
ctor
s i+
n 3
-05
4.2
1
.7ii
.s
Non
-opt
imal
per
inat
al f
acto
rs
3+
0
2.3
in-6
3
.7io
.h
Mon
ths
brea
st-f
eedi
ng
2rtn
0
.31
0.6
5.
3i3.
8 M
othe
r py
ch.
ill a
t ex
amin
atio
n (C
Z)
0 0
33
3 IV
V
(N=
26)
(N=
Y)
42C
16
39C
2O
2-O
-Cl.
6 1
.92
1.7
4
.5i2
.2
3.7-
Cl.
4 2
.Sk
2.4
2
-4-C
l.7
46
67
I I (N
=3
)
CO
MP
2
Soci
al c
lass
2
3 I1
111
IV
V (N
=10
) (N
=Y
) (N
=23
) (N
=6
)
12
i11
0
.3iO
-6
2.O
k-1-
0 3
.7i3
-2
0
tGro
up
mea
nsf s
tand
ard
devi
atio
ns u
nles
s sh
own
othe
rwis
e.
TA
BL
E V
lll
Fact
ors
dist
ingu
ishi
ng M
BD
fro
m c
ompa
riso
n gr
oups
1 a
nd 2
T
AB
LE
IX
Fa
ctor
s di
stin
guis
hing
MB
D f
rom
AD
D
CO
MP
I C
OM
P 2
C
umul
ativ
e .S
tep\
c,ise
int
rodu
ctio
n st
ep n
o cu
mul
ativ
e .x
tep
no
cum
ulat
ive
Step
wis
e in
trod
uctio
n of
-fac
tor
vari
ance
of
fact
or
vari
anw
va
rian
ce
expl
aine
d e.
Ypla
incd
q
da
ined
%
> %
' %
M
inor
phy
sica
l ano
mal
ies
1 13
M
othe
r ps
ych.
ill
at
exam
inat
ion
2 24
N
on-o
ptim
al n
eona
tal
fact
ors
3 30
3
32
Her
edit
y: l
earn
ing
diso
rder
* 4
36
1 15
N
on-o
ptim
al p
rena
tal
Non
-opt
imal
rea
ring
fa
ct o r
s
cond
itio
ns
2 25
4 36
Age
whe
n st
arte
d w
alki
ng
ii
Her
edity
: le
arni
ng d
isor
der*
17
~~
~~
~~
No
oth
er f
acto
rs m
et 0
. 1 s
igni
fica
nce
leve
l fo
r en
try
into
mod
el.
Five
cas
es w
ith M
BD
and
fou
r w
ith A
DD
wer
e de
lete
d be
caus
e of
sin
gle
mis
sing
da
ta.
*Fir
st-d
egre
e re
lativ
es
>
z 0
No
othe
r fa
ctor
s m
et
0. 1
si
gnif
ican
ce l
evel
fo
r en
try
into
mod
el.
Four
cas
es w
ith M
BD
. 7
CO
MP
1 an
d 7
CO
MP
2 ca
ses
wer
e de
lete
d be
caus
e of
sin
gle
mis
sing
dat
a.
*Fir
st-d
egre
e re
lativ
es.

Discussion To our knowledge, this population
study is the first to attempt to analyse the importance of various background factors in operationally diagnosed MBD cases. The findings agree with results obtained by other authors in research on aetiological and pathogenetic mechanisms in learning disorders, behavioural difficulties and psychiatric disturbances. Thus, Frisk (1967) found teenage dyslexia to be associated with hereditary factors or non- optimal prenatal or perinatal factors, or both, in a majority of the cases. Retrospective studies of psychiatric problems and learning disorders have demonstrated increased rates of pre- and perinatal complications (Kawi and Pasaman ick 1958, Knob loch a n d Pasamanick 1966). Drillien and co- workers (1980) found that children with minor physical anomalies who had been small for gestational age were at much greater risk of displaying motor/per- ceptuaVbehaviour problems than children without these background factors. In more than 90 per cent of the MBD cases in the present study, non-optimal heredity, prenatal, perinatal, neonatal or postnatal factors, or a combination of these were considered to be responsible for the disorder. In more than two-thirds of the MBD cases the scores for non-optimality in the areas mentioned were >2SD above the mean values of one of the comparison groups.
The choice of comparison groups in the present study requires some discussion. One might argue that the COMP I group was the most appropriate for comparison with the M R D group, as i t consisted of originally randomly-selected children, except for those with MBD. However, it turned out that MPD and ADD cases had a number of background factors in common with the M B D group, which means that the COMP 2 group ( i n which all cases with M B D ,
CHRISTOPHER GILLBERG PEDER RASMUSSEN
763
MPD and ADD had been excluded from the original random control group) in some instances was better suited for comparison with the MBD group. The COMP 3 group, although having the advantage of being larger than the other groups, had one or two serious shortcomings: the boy:girl ratio was not consistent with ‘normal’ populations; and although all the children in this group had been acquitted of MBD symptoms in the extensive neuro- psychiatric diagnostic procedure, it was nevertheless ‘special’ in that it contained both original ‘index’ and random ‘control’ children. However the comparison groups on the whole showed quite similar results, so the significance of the deviant results in the MBD group was even more firmly underlined.
The M P D and ADD groups were small, and differences between them and other groups only rarely reached statistical significance.
On the other hand, the MBD group differed significantly from the comparison groups in most of the background, psychosocial and associated factors studied. Those with the highest level of significance (p<O. 001) were non-optimal hereditary factors, non-optimal prenatal, perinatal and neonatal factors, maternal social stress scores, social problem area, non-optimal rearing conditions, ‘trouble- some child’, marked psychiatric abnorma- l i ty and low W [ S c performance results. These findings indicate that hereditary, brain-damaging and psychosocial con- ditions interact in a complex fashion in MRD symptomatology. It is of interest that there were no significant differences in background factors between severe and mild-moderate MBD children.
The high ratio of boys to girls found in almost all studies of neurodevelopmental/ neuropsychiatric disturbances in child- hood (Rutter 1977) was also seen in our M H D group, and was even more

PERCEPTUAL, MOTOR AND ATTENTIONAL DEFICITS IN SEVEN-YEAR-OLDS
pronounced in the ADD group. There was no difference between the sexes in the MPD group. This fact, together with the findings that non-optimal prenatal factors were particularly ‘typical’ for this group and non-optimal psychosocial conditions not so common, might indicate that children with MPD constitute a more homogeneous aetiological group than children with MBD and ADD. However, the high frequency of relatives with delayed onset of puberty shows that even in the MPD group background factors are likely to interact in a complex manner. Extremes of normal variation may also account for a proportion of the MPD cases. However, it is impossible to draw definite conclusions about this group because of the very limited number of children.
High maternal age has recently been implicated as one of the risk factors in MBD (Gillberg et al. 1980, 1 9 8 2 ~ ) and dyslexia (Jayasekara and Street 1978). Mothers of MBD children in this study were not significantly older than comparison mothers. However, the number of mothers giving birth after the age of 37, for example, is relatively very small, and even a high proportion of such mothers having children with MBD would not be expected to have great effect on the mean age of mothers of children with MBD.
It is rather difficult t o interpret the results as regards left-handedness and MBD. The finding that manifest left- handedness in the child is more frequent in the MBD group than in the other groups is consistent with the pathological left- handedness model hypothesized by Satz (1972), and in some cases is indicative of brain damage (for example two of these six children had sharp-wave foci on the left side in their EEGs). O n the other hand, the frequency of left-handedness among MBD children with at least one left-handed parent was much below the expected rate (Annett 1979). This, combined with the
result that non-optimal perinatal scores were particularly high among right- handed children born to left-handed parents, also seems to indicate brain- damage with a pathological shift of handedness in at least some of these cases. Speech-language problems were present in all MBD cases with ‘inverted’ handedness, compared with 74 per cent of the remaining MBD cases. This finding, too, is consistent with the notion that damage to the ‘dominan t ’ hemisphere is of importance in a certain proportion of MBD cases. However, no clear-cut right-sided or left-sided pathology in the neurological examination could substantiate this conclusion. Finally, the raised incidence of left-handed first-degree relatives in the MBD group (and, it appears, in the MPD group also) might indicate that children with heredity for left-handedness are at greater risk of suffering clinical sequelae of non-optimal perinatal factors.
A number of studies (e.g. Neligan et al. 1976) have shown that low-birthweight infants are at risk for developing later MBD-type symptoms. This risk is particularly pronounced if the child is small for gestational age (and ‘dysmature’) rather than born too soon. In our study, signs of clinical dysmaturity had been much more common in the MBD group than in the other groups. Mean birthweight was only slightly lower in the MBD group. Thus these results indicate that smallness for gestational age is of importance in the genesis of MBD only in a minority of the cases.
The high scores for minor physical anomalies could have suggested damage to the fetus in the first three months of pregnancy, but evidence is accumulating that stigmata of this kind are often hereditary rather than an effect of insult t o the fetus (Firestone et al. 1978). Future studies could well examine the parents of MBD children to see if they also have a
764

higher proportion of minor physical anomalies.
The findings with regard t o breast- feeding periods agree with those of Menkes (1977) and Broad( 1979), that children with learning disorders (children with a special kind of perception dysfunction), and especially boys, have had shorter breast- feeding periods than controls. In our study, children with MBD and very low wISC results had been breast-fed for particularly short periods. I t is possible that factors directly attributable to formula-feeding itself influence the child negatively. On the other hand, it is quite possible that motor-disabled o r mentally handicapped children have had sucking difficulties and therefore have been more often bottle-fed than breast-fed.
Children with MBD were socially disadvantaged compared with both the comparison children and those with MPD. Children with ADD more often lived in one- parent family homes than other children in this study. There is no clear evidence that children with ADD are more troublesome than children with MBD, for example, so thereisnoobvious reason toassumethatthe child is the cause of divorce more often than in othergroups.
This finding possibly indicates the aetiological r81e of psychosocial factors. It deserves mention, though, that children with ADD, as well as those with MBD, tended to be only children more often than comparison children.
Children with MBD had been in full-time day-nurseries from an earlier age and more often than comparison children. This might mean that MBD in the child causes the parents to want to go back to work Sooner and leave the child in the care of others, but of course it may also be a reflection of the poorer social circum- stances and the need to return to work earlier.
The number of mothers who had sought
CHRISTOPHER GILLBERG PEDER RASMUSSEN
765
psychiatric treatment for themselves increased between the child’s first and seventh years in the MBD group: the difference between this group and the comparison groups was significant a t age seven but not at age one. This may well reflect the ‘pathogenetic’ influence of a disturbed child on the psychiatric health of the mother.
Marked psychiatric abnormality was extremely common among the MBD children: it appears to be even more common than among children with gross neurological and epileptic handicaps (Rutter et a/. 1970). I t may be that the relative ‘invisibility’ of the MBD child’s handicap, and hence the failure of parents and specialists to recognize it a s a handicap, is the main reason for the very high rates of psychiatric disturbance. Detailed results with regard to psychiatric problems are reported separately (Gillberg 1982).
Mean WISC IQs are lowered in hyperkinetic children (Palkes and Stewart 1972). The very great difference between the MBD group and the rest of the groups in the present study possibly was due t o the fact that only the performance part of the WISC had been used. Brain-damaged children score particularly low on this scale (Rutter et al. 1970).
In the stepwise regression analysis, further support was found for the view that hereditary and potentially CNS-damaging factors are the most important back- ground factors in MBD. That the factor of non-optimal rearing conditions was found to be a distinguishing one calls for some discussion. Ch i ld ren with m o t o r / perceptual problems brought up in a very inconsistent a n d negligent m a n n e r possibly show more outward signs of disturbance than children reared by firm and loving parents (see Thomas et al. 1968). This could account for the finding. Conversely, it is possible that the disruptive, unpredictable behaviour of the

PERCEPTUAL, MOTOR A N D ATTENTIONAL DEFICITS I N SEVEN-YEAR-OLDS
child causes family upset, marital discord and inconsistent (‘non-optimal’) rearing methods.
Social class, although in itself highly correlated with the M B D diagnosis, was not in any major way a factor directly affecting the background var iab les s tud ied . However, mental disturbance in the mother is a n exception, in which social disadvantage appears t o be of great importance.
In summary, children diagnosed according to strict criteria as suffering from MBD have a variety of non-optimal hereditary and potentially CNS-damaging factors in their histories. O n the whole they are socially disadvantaged, but that in itself is not an aetiological factor. Children with MBD require specialist treatment twice as often as normal children and child psychiatric help is needed 10 times more often. There is some indication that the disturbed child causes the mother to seek
APPENDIX All mothers of the 141 children in the extended
study completed detailed questionnaires about hereditary factors, family factors, maternal and paternal health, siblings’ health and development and child’s health and development. These questionnaires were sent out two weeks before examination of the child. Mothers of the majority of the children also completed a Swedish translation of the Behavioral Style Questionnaire developed by Carey and McDevitt (1978).
The child’s psychiatric examination took place in the child’s home and comprised a detailed structured and semi-structured interview with the mother (by one of the psychiatrists, who a t that time had no knowledge about the child), plus neurological and psychiatric assessment of the child. Mean inter-rater reliability for different items, as judged by Pearson r, was acceptable ( r = 0 : 82 for the neurological and r = 0 . 7 5 for the psychiatric part of the child’s psychiatric examination (N=36, p<O.OOI)). For details of this part o f the study the reader is referred to Gillberg (1982).
The child neurologist’s assessments (for details see Rasmussen et a/. 1983) were made in children’s out- patient clinics, where the child was seen by the neurologist together with a n experienced child
766
psychiatric help. On the evidence so far, it may be concluded that biological and psychosocial factors interact in a complex fashion to create a neurodevelopmental syndrome of definite clinical significance. Long-term follow-up, now in progress, will reveal the prognostic significance of a diagnosis of MBD.
Acknowledgements: T h e a u t h o r s acknowledge the children a n d parents w h o par t ic ipated in the s tudy. We are grateful t o Nils-Gunnar Pehrsson, M.A. , a n d Ander s O d h , Ph .D . , f o r invaluable help with the statistical pa r t of the s tudy. We also thank Mrs . G u n J a k o b s s o n f o r never-failing patience in secretarial assistance.
Th i s w o r k would n o t have been possible without the generous suppor t of t he Swedish Delegat ion for Social Research, Ministry o f Hea l th a n d Social Affairs. Financial suppor t was also given to o n e o f t he a u t h o r s (C .G . ) by t he Forenade Liv Insurance C o m p a n y .
A U T H O R S ’ A P P O I N T M E N T S Chr i s tophe r Gil lberg, M.D. , I n s t i t u t e o f c h i l d a n d You th Psychiatry, University of Uppsa la ,Sweden . Peder Rasmussen, M . D . , Inst i tute of Pediatrics 1 1 , University of Go teborg , Sweden.
physiotherapist and was examined in accordance with many of the items of the Touwen manual Examination of rhr Child with Minor Nrurolo,yical D.v.!function (Touwen and Prechtl 1970, Touwen 1979). All fine- motor items wereratedas0, 1 or2(2indicatingmarked abnormality) and a total score for fine-motor problems was calculated by summing all the scores for the individual items. All gross-motor items were rated accordingly and a total score for gross-motor problems was calculated in the same fashion. ‘Minor neurological dysfunction’ was calculated by adding the scores for fine-motor and gross-motor problems. Routine paediatric status was also taken.
The psychological examination was also performed in children’s out-patient clinics and consisted of testing with the battery of the Southern California Sensory Integration Tests (SCSIT) developed by Ayres (1972) and the performance part of the WISC test.
Comprehensive diagnoses were made in the following manner: Ma,-ketlp.~j,chinrric. ahnornialirj, was rated globally by the psychiatrists as 0 = no abnormality, 1 =some abnormality and 2=definite and marked psychi- atric abnormality. Fin<, motor +.sfunction was rated by the neurologist as

CHRISTOPHER GILLBERG PEDER RASMUSSEN
0 = no signs (total scores for fine-motor problems0 to lo), I=slight dysfunction (total scores of 11 to 21) and 2=marked dysfunction (total scores of >21). Gross motor dysfunction was rated as O = n o signs (total scores for gross motor problems of 0 to 6 ) , 1 =slight dysfunction (total scores of 7 to 13) and 2=marked dysfunction (total scores of > 13). Percepfion dy’funcrion, according to SCSIT-testing, was rated as 0 = normal (values down to - lSD for all 19 variables studied), I =some abnormality (values between -1 and -2SD for up to six of the variables or below -2SD in not more than two of the four areas visual, kinaesthetic and tactile perception plus ‘sensory integration’) and 2 = marked dysfunction (seven or more of the 19 values below -1SDor 3 t o 4 values below -2SD in the four areas). The results of WISC testing were presented as stanine values: the range of the nine different classes of this scale are defined by the mean value of 100 and a standard deviation of 15. Speech-language disorder was rated as 0 = normal, t =slight deviances ( e . g . slight dysarticulation or minimal errors 0fgrammar)and 2=markeddeviances (children needing or already having speech therapy). Grammar errors by immigrant children were rated as 0. The basis for tating was the child’s psychiatric examination, as the child talked most freely during this examination. AffmfKJn d</ictf 5i~yn.v. Mothers were asked about the child’s activity level, ability to concentrate and to sit still. Scores of 0, 1 or 2 were assigned to each item, 2 indicating marked abnormality. A ‘maternal score for attention deficit signs’ was rated as 0 if there were 0 to 2 scores of I , as I if there was one score of 2 or a total of three, and as 2 if the total score was 2 4 . The results from the Behavioral Style Questionnaire could substitute the scores in the following way: Oxnot
more than one of the relevant scores (attention- persistence, activity and distractibility) between 0 and +ISD above the mean oftheoriginaIstudy,as 1 if two or three scores were in this range, and as 2 if any one of the relevant scores was more than ISD above the mean value. In both the psychiatric and neurological evaluations, ability to sit still, distractibility, attention span and activity level were rated in thesame fashion, with 0 indicating no and 2 marked abnormality for each individual item. The ‘psychiatrist’s score for attention deficit signs’ and the ’neurologist’s score for attention deficit signs’ were rated uniformly as 0 if the total score was 0 to I , as I if the total score was 2, and as 2 i f the total score was 2 3 . Inter-rater reliability for total scores, as judged by a Pearson r, was 0 . 8 2 ( N = 3 6 , p<0.001). In the child’s psychological examination, scores of 0, 1 or 2 were given to describe the child’s attention level, with 2 indicating extremely short attention span. Alfenfion &f?ci/ di.sorder (ADD) was considered t o be present if the child showed cross-situational attention deficit signs and was rated as 1 if the total sum of the scores obtained in the four different evaluations was 2 to 3 and as 2 if the total score was 4 to 8.
Molor pcrceprion dj~sfunc~tion (MPD) was considered to he present if the child had a score of 2 for any of fine motor dysfunction, gross motor dysfunction or perception dysfunction.
Minimal bruin dysfunction (MEDJ was diagnosed if a child had a score of 2 for attention deficit disorder and a score of 2 for line motor dysfunction, gross motor dysfunction or perception dysfunction. Speech- language disorder was then included in the total scoring system to distinguish cases with mi/& moderafr. MBD (total scores 4 to 8 ) from .rcvcrrMBD (total scores 9 to 10).
SUMMARY A total of 141 children selected from a pre-school programme screening for problems in
motor control, perception, attention and behaviour were examined blindly at age seven by two psychiatrists, a neurologist and a psychologist. Operational diagnoses of minimal brain dysfunction (MBD) were made, consisting of concomitant motor/perception ‘dysfunction and attention deficit disorder. Background factors, with special regard to heredity, neuropathogeneity and psychosocial conditions, were analysed. Non-optimal prenatal, perinatal or postnatal events and non-optimal neurodevelopmental heredity-or a combination of these-were much more common in the MBD group than in comparison groups. Non-optimal psychosocial conditions were found to interact with the other background factors in defining a clinically significant syndrome. Social disadvantage in itself did not appear to be a major aetiological factor.
Dtficit percept13 rnoteuv et &attention chcz des enfants de sept ans: facteurs htrtditaires. neuropathogbniques et d‘environnement psychosocial
141 enfants silectionnts par examen systkmatique d’une cohorte prt-scolaire, a partir 767
RESUME

PERCEPTUAL, MOTOR A N D ATTENTIONAL DEFICITS IN SEVEN-YEAR-OLDS
d’une mesure du contrde moteur, de la perception, de l’attention et du comportement ont ktk examinks en mkthode aveugle B I’ige de sept ans par deux psychiatres, un neurologue et un psychologue. Des diagnostics fonctionnels de MBD (dommage cerkbral a minima) ktablis sur une dysfonction associke motrice et perceptive et un trouble de I’attention ont pu l tre portks. Des facteurs d’environnement en rapport avec l’hkrkditk, la neuropathogknie et les conditions psychosociales ont pu l tre dtfinis. Des circonstances non optimales prk, ptri ou nko-natales, une hkrkditt non optimale du dkveloppement neurologique ou une combinaison des deux ont ktk trouvkes beaucoup plus frtquemment dans le groupe MBD que dans les cas de rkfkrences. Les conditions psychosociales non optimales ont paru interfkrer avec les autres facteurs d’environnement dans la constitution d’un syndrome clinique significatif. Les dksavantage social en soi-mlme ne semble pas un facteur d’importance ktiologique majeur.
ZUSAMMENFASSUNG Storungen der Perception, der Motorik und der Aufmerksamkeit bei sieben Jahre alten
Kindern: Heriditare, neuropathogene und psycho-soziale Faktoren 141 Kinder, die bei einem Vorschul-Screening hinsichtlich Motorkontrolle/Perception/
Aufmerksamkeit/Verhalten ausgewahlt worden waren, wurden im Alter von sieben Jahren von zwei Psychiatern, einem Neurologen und einem Psychologen blind nachuntersucht. Es wurden Diagnosen der MBD gestellt (gleichzeitige Storung von Motorik und Perception und Aufmerksamkeitsmangel). Es wurden anamnestische Faktoren unter besonderer Berucksichtigung der Heriditat, Neuropathogenitat und psychosozialer Bedingungen vermerkt. Bei der MBD Gruppe fanden sich sehr vie1 haufiger nicht optimale pra-, peri, und neonatale Bedingungen, nicht optimale Heriditat und eine Kombination dieser Faktoren als bei den Kontrollen. Nicht optimale psychosoziale Bedingungen verbanden sich mit den anderen anamnestischen Faktoren zu einem klinisch signifikanten Syndrom. Soziale Nachteile allein schienen nicht von besonderer atiologischer Bedeutung zu sein.
RESUMEN Dkjicits perceptivos, motores y de atencidn en nifios de siete afios de edad: Factores de fondo
hereditarios, neuropatogknicos y psicosociales Ciento cuarenta y un niiios seleccionados a partir de un screening escolar en relaci6n con
control motor- perceptidn- atencidn-comportamiento fueron examinados a ciegas a la edad de siete aiios por dos psiquiatras, un neurdogo y u n psic6logo. Se realizaron diagnosticos operacionales de MBD (disfunctibn concomitante motor-percepti6n y dkficit de atenciitn). Se tuvieron en cuenta 10s factores de fondo y en especial 10s hereditarios, neuropatogenia y caracteristicas psicosociales. Acontecirnientos no 6ptimos pre, peri o neo-natales, herencia neuroevolutiva no 6ptima o una combinacidn de esto factores eran mucho mhs abundantes en el grupo MBD que en 10s casos control. Se ha116 que las condiciones no 6ptimas psicosociales no eran interactivas con otros factores de fondo en el moldeo de un sindrome clinicamente significativo. La desventaja social per se no aparecio como un factor de importancia etiol6gica mayor.
REFERENCES Annett, M. (1979) ‘Family handedness in three generations predicted by the right shift theory.’ Annuli
Ayres, A. J . (1972) Southern California Sensory Integration Tests. Los Angeles: Western Psychological
768
of Human Genetics, 42, 479-491.
Services.

CHRISTOPHER GILLBERG PEDER RASMUSSEN
Bradley, J. V. (1968) Distribution,free .Statistical Tests. Englewood Cliffs, N. J.: Prentice-Hall.
Broad, F. E. (1979) ‘Early feeding history of children with learning disorders.’ Developmental Medicine and Child Neurology, 21, 822. (Letter.)
Carey, W., McDevitt, J . (1978) ‘The measurement of temperament in 3-7 year-old children.’ Journal of Child Psychology and Psychiatry, 19, 245-253.
Clements, S. D. ( I 966) Minimal Brain Dysjunction in Children: Terminology and Ident@cation. NINDB Monograph 3. Washington: U.S. Govt. Printing Office.
Draper, N. R., Smith, H. (1966) Applied Regression Analysis. New York: Wiley. Drillien, C. M., Thomson, A. J., Burgoyne, K. (1980) ‘Low-birthweight children a t early school-age:
a longitudinal study.’ Developmental Medicine and Child Neurology, 22, 26-47. Firestone, P., Peters, S. , Rivier, M. , Knights, R . (1978) ‘Minor physical anomalies in hyperactive,
retarded and normal children and their families.’ .Journal qf Child Psychology and P.sychiarry, 19,
Frisk, M. (1979) ‘What is meant by MBD?’ In; Rydefalk, I . (Ed.) Children with MBD-Do they Exist? (in Swedish). Nacka: Esselte studium.
- Wegelius, B., Tenhunen, T., Widholm, O., Hortling, H. (1967) ‘The problem of dyslexia in teenage.’ Acta Paediatrica Scandinavica, 56, 333-343.
Gillberg. C . (1982) ‘Perceptual. motor and attentional deficits in Swedish Drimary school children. Some child psychiatric aspects.’ Journal of Child Psychology and Psychiatry. (in press).
- Rasmussen, P. ( 1982) ‘Perceptual, motor and attentional deficits in six-year-old children. Screening procedure in pre-school.’ Aria Paediarrica Scandinavica. 71, 121-129.
_ _ Wahlstrom, J. (1980) ‘Neuropsychiatric problems among children born t o older mothers’, Acta Paedopsychiatrica. 46, 57-65.
- - Carlstrom, G. , Svenson, B., Waldenstrom, E . ( 1 9 8 2 ~ ) ‘Perceptual, motor and attentional deficits in six-year-old children. Epidemiological aspects.’ Journal qf Child Psychdogy and Psychiatry.
- Matousek, M., Peterstn, I. , Rasmussen. P. (1982b) ‘Perceptual, motor and attentional deficits in seven-year-otd children. Electroencephalographic aspects.’ Acta Paedopsychiatrica, (in press).
- Rasmussen, P., Wahlstrom, J . (19824 ‘Minor neurodevelopmental disorders in children born to older mothers.’ Developmental Medicine and Child Neurolo,qy, 24, 437-447.
Graffar, M. (1956) ‘Une mt thode de classification sociale d’tchantillons de population.’ Courrier,
Hagberg, B. ( 1975) ‘Minimal brain dysfunction in children-effects on development and adjustment.’
Health Sciences Computing Facility (1977) Statistical Computer Library B M D P4M, UCLA. Jayasekara, R., Street, J . (1978) ‘Parental age and parity in dyslexic boys.’ Journal qf Biosocial Science,
Kawi, A. A, , Pasamanick, B. (1958) ‘Association of factors of pregnancy with reading disorders in childhood.’ Journal of the American Medical Association. 166, 1420- 1423.
Knobloch, H. , Pasamanick, B. (1966) ‘Prospective studies o n the epidemiology of reproductive casualty: methods, findings and some implications.’ Merrill-Palmer QuarterIy. 12, 27-43.
Korhonen, T., Sillanpaa, M. (1976) ‘MBD-like behaviour and neuropsychological performances.’ Arta Pat~dop.~~~chiatrica. 42, 75-87.
Mantel, N. (1963) ‘Chi-square tests with one degree of freedom.’ .Journal qf the American Slatistical Association, 58. 690-700.
Mendeloff, A. I., Monk, M., Siegel, C . I . , Liljenfeld, A. (1970) ‘Illness experience and life stresses in patients with irritable colon, ulcerative colitis and regional enteritis in Baltimore, 1960-1964.’ Neb\, England .Journal of Medicine. 282, 14- 17.
Menkes, J . M. (1977) ‘Early feeding history of children with learning disorders.’ DevelopmentalMedicine and Chi/d Neurology, 19, 169- 17 1.
Michaelis, R., Dopfer. R., Dopfer-Feller, P.. Rohr. M. (1979) ‘Die Erfassung obstetrischer und postnataler Risikofaktoren durch eine Liste optimaler Bedingungen.’ Monar.s.\chrift,fiir Kindrrhcilhunrk. 127. 149-155.
Neligan, G . A,, Kolvin, I., Scott, D. M., Garside, R. F. (1976) Born Too Soon or Born Too Small. C/jnic..y in Dpve/opmen/al Me&cinc No. 6 l . London: SIMP with Heinemann Medical; Philadelphia: Lippincott.
Palkes, H., Stewart, M . ( 1972) ‘Intellectual ability and performance of hyperactive children.’ American .Journal of Orrhop.y,vchiatrj,, 42, 35-39.
Prechtl, H.’ F. (1968) ‘Neurological findings in newborn infants after pre- and paranatal complications.’ In: Jonxis, J. H . P. , Visser, H . K . A , , Troelstra. .J. A . (Eds.) A.spwt.s o/Prarmaturitj, andDj~smaturity: A Nutrica Symposium. Leiden: Stenfert Kroese pp. 306-309.
Rasmussen, P., Gillberg, C . , Waldenstrom, E., Svenson, B. (1982) ‘Perceptual, motor ,and attentional deficits in seven-year-old children. Neurological and neurodevelopmental aspects. Developmental Medicine and Child Neurology. (in press).
Rubin, R.. Balow. B. ( 1980) ‘Infant neurological abnormalities as indicators of cognitive impairment.’ 769
pp. 68-86.
1 55- 160.
23, 131-144.
6 , 455-459.
(in Swedish-summary in English). Ldkartidningen. 72, 3296-3300.
10, 225-261.

PERCEPTUAL, MOTOR AND ATTENTIONAL DEFICITS IN SEVEN-YEAR-OLDS
Developmental Medicine and Child Neurology. 22, 336-343.
Approaches. Oxford: Blackwell. p. 368. Rutter, M. (1977) ‘Classification’. In: Rutter, M., Hersov, L. (Eds.). Child P.sl~t%.inti:,~-Mo(I~~rn
- (1982) ‘Svndromes attributed t o “minimal brain dvsfunction” in childhood.’ American Journal o f Psychiatry, -13Y, 21-33.
Medicine Nos 35/36. London: S.I.M.P. with Heinemann Medical: Philadelohia: Liooincott. - Graham, P. , Yule, W. (1970) A Neuropsychiatric Studj. in Childhood. Clinics in Devrlopmental
Satz, P. (1972) ‘Pathological left-handedness; a n explanatory model.’ Corte.~.’ 8, 121-1’35. Shaffer, D. (1977) ‘Brain injury.’ In: Rutter, M., Hersov, L. (Eds.) Child Psj~chia/rj~-Moriern Approachc~.~.
Social Welfare Authorities (Sweden) ( 1980). Demographic data . Thomas, A., Chess, S., Birch, H. G. (1968) Temperument and Behuvior Disorclc~i..~ in Children. New York:
New York University Press. Touwen, B. C. L. ( 1979) Examination o f the Child itsith Minor Neurolri,yic.ol Dj~.sfunc.tion. 2nd Edn. Clinic..\
in Developmental Medicine No 71. London: S.I.M.P. with Heinemann Medical; Philadelphia: Lippincott. - Prechtl, H. F. R. (1970) The Neurological E.t.arnination ?/’ the Child with Minor Nervou.\ D~~/irnc.tion.
Clinics in Developmental Medicine N o 38. London: S.I .M.P. with Heinemann Medical; Philadelphia: Lippincott.
Waldrop, M. , Halverson, C. (1971) ‘Minor physical anomalies and hyperactive behaviour in young children.’ In: Hellmuth, J. (Ed. ) The E.weptiona1 Infant. Vol. 2. Stuc1ic.s in Ahnorma1itir.s. New York: Brunner-Mazel.
Oxford: Blackwell.
770