Embed Size (px)
Citation preview

Earn
2 CE creditsThis course was
written for dentists, dental hygienists,
and assistants.
The Use and Efficacy of Professional Topical Fluorides A Peer-Reviewed Publication Written by N. Sue Seale, DDS, MSD and Diane M. Daubert, RDH, MS
PennWell designates this activity for 2 Continuing Educational Credits
Publication date: 9/2010Expiry date: 8/31/2013
Go Green, Go Online to take your course
This course has been made possible through an unrestricted educational grant. The cost of this CE course is $49.00 for 2 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.

2 www.ineedce.com
Educational ObjectivesThe overall goal of this article is to provide the reader with infor-mation on the use, efficacy and safety of professional topical fluo-rides. In addition, current recommendations based on caries risk level are addressed. Upon completion of this course, the reader will be able to do the following: 1. List the types of professional topical fluorides that are avail-
able in the US and Canada2. List and describe the ADA recommendations on the use of
professional topical fluorides3. List and describe the evidence on efficacy and safety for
sodium fluoride varnishes4. List and describe the methods by which different professional
topical fluorides can be applied
AbstractFollowing the discovery that fluoride plays a role in the preven-tion of dental caries, professional topical fluorides were devel-oped. Traditionally, fluoride gels and, later, fluoride foams were used in the US and Canada. More recently, fluoride varnishes were introduced first in Canada, and then in the US where they are cleared for use as desensitizing agents. The use of fluoride varnishes for caries prevention is ‘off-label’ in the US. A recent publication by the ADA Council on Scientific Affairs recom-mends the use of fluoride varnish or fluoride gel for professional topical fluoride treatments, with the choice depending on patient age and risk category. Due to insufficient evidence, foams are not recommended for professional topical fluoride treatment and there is no evidence to support rinses. Fluoride gel and varnish have both proven to be effective, with only varnish recommend-ed in the under-6 age group. Evidence-based treatment requires that the clinician assess a patient’s risk level prior to treatment, which can be done with formal risk assessment tools such as CAries Management by Risk Assessment (CAMBRA) and the Caries Assessment Tool (CAT).
Introduction Fluoride has maintained an important role in the field of preventive dentistry since the 1940s. The discovery of high levels of fluoride in the water in the 1930s1 led to the formation of the Dental Hy-giene Unit at the National Institutes headed by H. Trendly Dean, who noticed an inverse relationship between caries prevalence and fluoride concentration that leveled off above 1 ppm. A large-scale prospective study that evaluated 30,000 children over a period of 15 years resulted in the conclusion that fluoridated water resulted in a significant reduction in caries for the fluoridated cities.2 The Centers for Disease Control and Prevention (CDC) reported in 2006 that 69.2 % of US citizens served by public water supplies were receiving fluoridated water.3 Recognition of the role of fluoridated water in caries reduction led to the development of other modes of fluoride delivery, including the addition of fluoride to toothpastes, mouth rinses, gels and tablets. It also led to the development of methods of professional fluoride application for caries prevention, including gels, foams, rinses and varnishes. Specific fluoride products are also
used to treat dentinal hypersensitivity, including fluoride varnish and other in-office desensitizers as well as home-use products.
Recognition of the role of fluoridated water in caries reduction led to the development of other modes
of fluoride delivery.
Professional Topical FluoridesProfessional topical fluorides include fluoride gels, foams, rinses and varnishes. Traditionally, professional fluoride treatment in the US and Canada involved the use of fluoride gels in trays. This was followed by the introduction of fluoride foams used in trays, which are generally considered easier to use than gels and have less risk of ingestion of fluoride. Less total fluoride is applied with foam, and a lower volume of product is used. These factors reduce the risk of the patient gagging and swallowing fluoride and also the amount of fluoride that could be ingested as a result. Fluoride varnish has been in use in Europe for more than 30 years as a method of profes-sional application of topical fluoride.4 In North America, sodium fluoride varnish was introduced first in Canada, and later in the US when it was cleared by the Food and Drug Administration (FDA) for use as a desensitizing agent and cavity liner. As such, its use for caries prevention in the US is “off-label” (i.e., it is being used for a purpose that has not received FDA approval or clearance). Since its introduction in the United States in the 1990s, its use for the prevention of caries has increased among the dental community.5
The use of fluoride varnish for caries prevention is off-label.
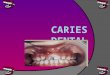
Mechanisms of ActionProfessional topical fluorides inhibit demineralization and promote remineralization. Available fluoride helps to prevent the loss of minerals during acid attacks and helps to replenish demineralized areas. Fluoride varnish utilizes a natural tree resin base that facilitates adherence of the varnish to the teeth and prolongs the contact time between fluoride and the tooth surfaces. The fluoride varnish forms calcium fluoride compound deposits that create a reservoir of fluoride ions that are slowly released when the pH of plaque drops (Figure 1). This reservoir acts as a prolonged source of fluoride ions.6,7,8 Numerous studies have concluded that fluoride varnishes are capable of depositing large amounts of fluoride on human enamel and it has also been concluded that the amount deposited on demineralized enamel is greater than that on sound enamel.9
As desensitizing agents, fluorides work by blocking the den-tinal tubules. Brannström’s hydrodynamic theory suggests that hypersensitivity is caused by the movement of fluid backward and forward within the dentinal tubules in response to stimuli and that it is this movement that results in the sensation of pain.10 Therefore, blocking the dentinal tubules blocks the movement of fluid for a period of time.

www.ineedce.com 3
Figure 1. Release and availability of ions during acid attack
Recommendations for Professional Topical Fluorides Treatment recommendations should be based on scientific evidence in combination with knowledge of the patient’s health history, oral condition and preferences. This means that the dental professional needs to understand the scientific and evidence-based merits of a product and also consider the patient’s caries risk when recom-mending fluoride treatment.11 In May 2006, the American Dental Association’s Council on Scientific Affairs published recommenda-tions on the use of available professional topical fluorides by caries risk category, based on results from published clinical trials and evidence-based studies. The use of only fluoride varnish is recom-mended for patients less than 6 years of age. (Note that recommen-dations for varnish refer to 5% sodium fluoride varnish.) For patients 6 years and older, fluoride varnish or gel is recommended. The rec-ommended frequency of use is two to four times per year for patients with a high caries risk, and twice per year for moderate risk patients. It is also stated that if a patient has low risk for caries, the person may not receive additional benefit from professional topical fluoride ap-plication. The use of foam is not recommended, due to the fact that although laboratory data supports its effectiveness there have been only two clinical trials on its anti-caries efficacy. In addition, the use of 1-minute products (gels and foams) is not endorsed.12
Table 1. ADA Council on Scientific Affairs recommendations
High Risk Moderate RiskUnder age 6 Fluoride varnish; 2-4
times per year (6 month or 3 month intervals)
Fluoride varnish at 6 month intervals
6 - 18 years of age
Fluoride varnish or gel; 2 - 4 times per year (6 month or 3 month intervals)
Fluoride varnish or gel at 6 month intervals
Over 18 years of age
Fluoride varnish or gel; 2 - 4 times per year (6 month or 3 month intervals)
Fluoride varnish or gel at 6 month intervals
Low risk patients may not benefit from professional topical fluoridesSource: Adapted from the ADA Report of the Council on Scientific Affairs, May 2006.
The patient’s caries risk, age and the scientific as well as evidence-based merits of a product must be considered
when recommending fluoride treatment.
In order to provide evidence-based patient care, it is neces-sary to know the patient’s caries risk. A person is considered to be at low risk if she or he has had no caries, including incipient lesions, in the past three years and has no other risk factors.Caries risk factors include but are not limited to the following: one or two incipient or cavitated carious lesions in the past three years, low socioeconomic status, suboptimal fluoride exposure, xerostomia, poor oral hygiene, cariogenic diet, exposed root sur-faces, drug or alcohol abuse, many existing multisurface restora-tions, defective restorations, orthodontic therapy, and physical or mental disability.
Table 2. Caries risk factors
Poor oral hygiene
Cariogenic diet
Incipient or cavitated carious lesions in the past three years
Xerostomia
Suboptimal fluoride exposure
Existence of many multisurface restorations
Exposed root surfaces
Drug or alcohol abuse
Low socioeconomic status
Physical or mental disability
Formal caries risk assessment tools that can be used to deter-mine a patient’s caries risk include CAries Management By Risk Assessment (CAMBRA) and the Caries Assessment Tool (CAT).13,14 Twenty-five data points are gathered and assessed using CAMBRA, after which a protocol is developed for risk management and treatment of the child or adult patient. CAT is a separate program recommended by the American Academy of Pediatric Dentistry that is intended for use with children of all ages. Other formal risk assessment tools are also available, and the criteria and definition of low, medium and high risk vary with the program used. The ADA provid-ed definitions of low, medium and high-risk patients by age, together with the recommendations for professional topical fluorides in the Council on Scientific Affairs publication.15
Level of Evidence and EfficacyThe studies on professional topical fluorides for caries preven-tion have largely been conducted on medium- and high-risk children and adolescents. One meta-analysis found overall car-ies reductions of 38% (DMFS/dmfs) with the use of fluoride varnishes.16 Many systematic reviews and meta-analyses have
Acid
F/
PO4///Ca++
Ca++
F/
PO4///
F/
Ca++
PO4///
PO4///Ca++
F/

4 www.ineedce.com
documented the effectiveness of fluoride varnish, as well as some for fluoride gel, in inhibiting caries in this age group.17 However, professional topical fluorides are also used in adults and geriatric patients who have additional needs. Fluoride varnish must be reapplied to maintain its caries-preventive effect, as must other topical fluorides.18,19 As discussed, recommended schedules of reapplication include two to four times a year, depending on the caries risk of the individual. An intensive treatment protocol using three applications of Duraphat in one week per year over three and four years showed caries reductions of 46% to 67% in proximal surfaces.20,21 This intensive regimen would be appro-priate for highly mobile individuals who might not be available on a regular two to four times a year schedule, such as migrant families who move frequently. The level of evidence-based docu-mentation of the efficacy of professional topical fluorides differs among age groups and by use.
Recommended schedules of professional topical fluoride reapplication include two to four times
a year, depending on caries risk.
Children Under 6 Years of AgeIn children younger than 6 years, there is strong evidence from systematic reviews of randomized controlled trials supporting fluoride varnish applications at six-month intervals for moder-ate- and high-risk patients and for applications of fluoride varnish every three months in high-risk patients. Prior to the introduction of fluoride varnish, there was no safe way to admin-ister topical fluoride to children 0-3 years of age. Their limited ability to control swallowing and variable ability to spit effec-tively on command preclude the use of foams, gels and rinses. These are not recommended for this age group.
Fluoride varnish’s tenacious adherence to the tooth provides for slow release of the fluoride over time and results in only a small amount being swallowed at a time. Weintraub et al. reported that children ages 6-44 months who received no varnish were more than two times as likely to develop decay as those who received annual varnish application.22 Stearns et al. reported that children 6-44 months of age who had four or more visits where varnish was applied as a part of a preventive/referral service showed a 39% reduction in caries-related treatment in anterior teeth.23 Fluoride varnish should be part of all preventive strategies aimed at high-risk children in this age group.
Miller and Vann expanded on the ADA panel’s recommenda-tions, which addressed recommendations for topical fluoride use in children under age 6, but not specifically ages 0-3 years; they recommended that “based on available evidence including dose reductions and efficacy justifications, we advocate that varnish should be the only topical fluoride modality used for children 0-3. Because of safety concerns we advocate further that varnish should also be the only modality used for children with special health care needs who exhibit attention span and/or cooperation problems.”24
Children Ages 6-18 YearsIn children ages 6-18 years with moderate and high caries risk, there is evidence from systematic reviews to support the use of fluoride varnish or gel every six months as well as to support the use of fluoride varnish every three months in high-risk children. The level of evidence for the use of fluoride gel every three months in high-risk children ages 6-18 is lower. For children 6-18 years of age, a systematic review by the Cochrane Collaboration found a caries reductions of 28% for gels, and a separate review for varnish found DMFS reductions of 46% for permanent teeth and dmfs reductions of 33% for primary teeth in children up to 16 years of age. 25,26
There is strong evidence to support the use of fluoride varnish or gel every six months in at-risk
children ages 6-18 years, as well as strong evidence to support the use of fluoride varnish every three
months in those at high risk.
Orthodontic treatment usually begins during this age range, and it is well established that orthodontic appliances can increase the risk for enamel demineralization around brackets. Investigations have shown that fluoride varnish can reduce or minimize demin-eralization of enamel adjacent to brackets.27,28,29
Figure 2. At-risk adolescent undergoing orthodontic treatment
Adults (All Patients Over 18 Years of Age)The primary uses for fluoride varnish in adults are for reminer-alization or control of root caries in older patients, prevention of caries in high-risk adults and treatment of dentinal sensitivity. There is some evidence supporting the use of fluoride of either modality (varnish or gel) every six months for patients over 18 years of age at moderate and high risk, and for high-risk patients at three-month intervals. The level of evidence is lower and is based on expert committee reports or opinions rather than pro-spective, randomized clinical trials.
Data on the effectiveness of fluoride varnish being superior to other treatment options for root caries is equivocal. Several

www.ineedce.com 5
investigations show equivalence – no superiority of fluoride var-nish over the use of chlorhexidine varnish or stannous fluoride solution (8%) or in combination with Cariosolve chemome-chanical technique.30,31 There is tentative support for three-monthly application of fluoride varnish for remineralization of root caries.32 There are no clinical trials providing evidence to support the use of professional topical fluoride gels or foams for the prevention and treatment of root caries. Support is definitely adequate to recommend using fluoride varnish as a part of a total preventive plan including the other agents investigated in these reported studies.
One study found 5% sodium fluoride varnish to produce sensitivity relief results that are equivalent to that of oxalate preparations. In another study 2% fluoride iontophoresis, Gluma Comfort Bond Plus Desensitizer, copal varnish and 5% sodium fluoride varnish all resulted in significant relief at 24 hours; after 7 days, results were statistically significant for 2% fluoride iontophoresis and Gluma Comfort Bond Plus Desensi-tizer.33,34 A recent study compared the use of 5% sodium fluoride varnish and shellac-based fluoride varnish for sensitivity relief and found both to be equally effective and to provide relief.35 Fluoride varnish can be effective for up to three to six months for sensitivity relief, depending on the patient, when used according to the directions for use.36
Table 3. Level of evidence for professional topical fluorides - moderate and high caries risk
Varnish GelUnder age 6
Moderate risk High for every 6 months Not recommendedHigh risk High for every 6 months Not recommended
and every 3 months Not recommended6-18 year-olds
Moderate risk High for every 6 months High for every 6 monthsHigh risk High for every 6 months High for every 6 months
and every 3 months Lower for every 3 monthsOver 18 years Lower Lower
Source: ADA Report of the Council on Scientific Affairs, May 2006.
SafetySeveral aspects provide for the safety of sodium fluoride varnish compared to other methods of delivery of professional topical fluorides. Even though the concentration of fluoride in 5% NaF varnish (22.6 mg F/ml) is about twice as high as in APF gel (12.3 mg F/ml), the amount required for a treatment ranges from 0.1 – 0.5 ml (2.26 - 11.3 mg F) for varnish depending on age, com-pared with 4-8 ml (49.2-98.4 mg F) with APF gels.37
Additionally, the potential for ingestion is basically solved by the tenacious adherence of fluoride varnish to the teeth. Thus, any fluoride that is swallowed is minimal and ingested over longer periods of time, virtually eliminating the possibility of nausea, vomiting or other fluoride toxic reactions.38 In fact,
there were no safe ways to administer topical fluoride to children 0-3 years of age until the introduction of fluoride varnish, and certainly the varnish provides a safer delivery system for the 3-to-6-year age group, where swallowing of gels and foams is a major concern. The risk of dental fluorosis with professional topical fluorides is minimal, since children are not frequently exposed to these, as they are to fluoride supplements and other sources of fluoride.39 There is a warning on package inserts to avoid sodium fluoride varnish in patients who have histories of asthma, as a result of a low but potential risk of allergic reactions to the resin base, including contact allergic dermatitis. Isaks-son reported on two cases of contact allergy to sodium fluoride varnish.40 Miller and Vann reported no adverse outcomes with asthma at the time of their US publication.41 If a patient is al-lergic to the resin contained in the varnish base, or any other ingredient, fluoride varnish should not be used for that patient. Fluoride varnish is contraindicated if a patient has ulcerative gingivitis or stomatitis.
Fluoride vehicles and dosingThe first and most extensively studied 5% sodium fluoride var-nish was Duraphat. Originally, varnishes were yellow-tinted and dispensed from a tube (Duraphat; Duraflor). A number of 5% sodium fluoride varnishes are now available, and they differ in properties such as viscosity, color (clear/white/tinted) and taste. One milliliter of the varnish contains 22.6 mg fluoride/ml. Some manufacturers provide unit-dosed packaging, which offers several advantages: each patient gets a controlled amount of fluoride, preventing over-application and minimizing any potential possibility (already minimal) of fluoride ingestion. An additional advantage of unit doses relates to sodium fluoride’s tendency to settle in the varnish due to its particulate nature, potentially affecting the amount of fluoride dispensed from multiple use containers. With unit dosing, the amount of sodium fluoride will be consistent in each application.42 Fluoride gels are dispensed directly into mouth trays from larger bottles, as well as being available in trays with pre-loaded and pre-dosed gel. Most manufacturers have mechanisms to help advise the proper amount of their product to dispense. For a 5% NaF varnish, in general it is advised to provide 5.65 mg F, or 0.25 ml, for the primary dentition; 9.04 mg F, or 0.40 ml, varnish for the mixed dentition; and 11.3 mg F, or 0.50 ml, varnish for the permanent dentition. For gels, the amount placed in the tray depends on the age of the patient (and thus also the size of the tray) and ranges from 49.2 - 98.4 mg fluoride.
Table 4. Treatment doses
Varnish Gel
Permanent dentition 0.5 ml (11.3 mg F) 4 – 8 ml (49.2 – 98.4 mg F)
Mixed dentition 0.4 ml (9.04 mg F) 4 – 8 ml (49.2 – 98.4 mg F)
Primary dentition 0.25 ml (5.65 mg F) Not recommended
Infants 0.1 ml (2.26 mg F) Not recommended

6 www.ineedce.com
The following section shows the application in a pediatric and an adult case.
Case 1. Application of fluoride varnish for a pediatric patientThe child represented in Figure 3 is a three-year old with high caries risk and early childhood caries. The first step in preparing to provide a fluoride varnish treatment for a pediatric patient is to de-termine the proper dosage for the child’s dentition, primary, mixed or full permanent. The varnish should be thoroughly mixed after it is dispensed. When only a thin layer of plaque is present, fluoride varnish can be directly applied without prior removal of the plaque. If a thick layer of plaque is present, this can be removed (prior to the application of professional topical fluoride) by toothbrushing or prophylaxis (neither is considered superior to the other).43
Moisture should be removed from the teeth with gauze or cotton rolls. It is not necessary for the teeth to be air-dried, nor is absolute moisture control necessary although excessive saliva flow over the teeth should be avoided. The varnish is then applied with a brush or cotton-tip applicator or the applicator supplied by the manufacturer, and until set will flow on the teeth, including into interproximal ar-eas. Fluoride varnish can be rapidly applied and there is no waiting time after application. Total application time varies, depending on how many teeth need to be varnished. It will set in the presence of intraoral moisture, and no rinsing or suctioning is required follow-ing the application. The child may be able to feel the thin film of the varnish with his/her tongue. (Note: Tinted varnishes leave a yellow film over the teeth, and parents and older patients would need to be warned of this effect if a tinted varnish is used.)
Figure 3a. Missing tooth structure and carious lesion
Figure 3b. Application of varnish
The directions that patients in all age groups should follow post-application are specific. The patient should not eat hard and crunchy, or hot, foods for several hours after application (typically four to six hours), should refrain from drinking hot liquids or liquids containing alcohol, should avoid alcohol-containing mouth rinses, and should wait until the following day before resuming tooth brushing and flossing. In contrast, it is generally recommended that patients completely refrain from eating or drinking immediately following the application of gels or foams for at least 30-60 minutes, which, although a shorter period of time, relies on no food or drink being taken (or rinsing) and patient compliance. Following topical fluoride application, if fluoride supplements are used, these should not be taken and should be resumed several days later.
Case 2. Application for an adult periodontal patientThis example involves a 68-year-old adult female with a history of periodontal surgery and regular three-monthly periodontal maintenance. The patient is at caries risk due to drug-induced xerostomia, has exposed roots and also com-plains of dentinal hypersensitivity. In a periodontal practice with patients who commonly have both dentin exposure and caries risk factors, it is advantageous to use one treatment that addresses two areas of concern. Part of her periodontal maintenance therapy includes fluoride varnish application, with the dual benefit that it is effective in both preventing car-ies and treating dentinal hypersensitivity. The application of fluoride varnish can be targeted to specific areas. In the case of periodontal patients with extensive areas of exposed roots, the varnish can easily be applied to areas that may not easily be accessed using a gel and tray. It would also be anticipated that the patient would achieve simultaneous relief from dentinal hypersensitivity. The general application technique and post-application instructions are described above.
Figure 4a. Periodontal patient at-risk for caries and with dentinal hypersensitivity

www.ineedce.com 7
Figure 4b. Application of varnish
Figure 4c. Application of varnish
Note the exposed roots and bifurcations that are accessible with the applicator.
SummaryProfessional topical fluoride treatments are recommended for use in patients at risk for dental caries. Based on the evidence and safety considerations, only fluoride varnish is recommended for patients under the age of 6, while for patients age 6 and older, either fluoride gel or varnish is recommended. The selection of a professional topi-cal fluoride should be guided by the scientific evidence, age and risk level of the patient as well as specific intra-oral considerations.
References1 CDC.Achievementsinpublichealth,1900-1999:fluoridation
ofdrinkingwater to prevent dental caries. MMWR. October 22, 1999;48(41):933-40.
2 CDC. Achievements in public health, 1900-1999: fluoridation of drinking water to prevent dental caries. MMWR. October 22, 1999;48(41):933-40.
3 CDC. Populations receiving optimally fluoridated public drinking water – United States, 1992-2006. MMWR. July 11, 2008;57(27):737-41.
4 Bawden JW. Fluoride varnish: a useful new tool for public
health dentistry. J Public Health Dent. 1998;58:266-69.5 Autio-Gold J. Fluoride varnishes for everyday practice.
Pract Proced Aesthet Dent. 2005;17:398, 400.6 Fejerskov O, Thylstrup A, Larsen MJ. Rational use of
fluorides in caries prevention: a concept based on possible cariostatic mechanisms. Acta Odontol Scand. 1981;39:241-49.
7 Ogaard B, Seppa L, Rolla G. Professional topical fluoride applications – clinical efficacy and mechanism of action. Adv Dent Res. 1994;8:190-201.
8 Ten Cate JM. Review on fluoride, with special emphasis on calcium fluoride mechanisms in caries prevention. Eur J Oral Sci. 1997;105(5 pt 2):461-65.
9 Beltran-Aguilar ED, Goldstein JW, Lockwood SA. Fluoride varnishes: a review of their clinical use, cariostatic mechanism, efficacy and safety. J Am Dent Assoc. 2000;131:589-96.
10 Brannstrom M, Astrom A. The hydrodynamics of the dentine: its possible relationship to dentinal pain. Int Dent J. 1972;22:219-27.
11 ADA. Report of the Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. JADA. May 2006;137(8):1151-59.
12 ADA. Report of the Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. JADA. May 2006;137(8):1151-59.
13 Young DA, Featherstone JDB, Roth JR, et al. Caries Management by Risk Assessment: Implementation Guidelines. Consensus Statement. Calif Dent J. 2007:799-805.
14 American Academy of Pediatric Dentists. Policy on the use of a caries-risk assessment tool (CAT) for infants, children and adolescents. Reference Manual 2002-2003. 15-17. Available at: http://www.aapd.org/members/referencemanual/pdfs/02-03/Caries%20Risk%20Assess.pdf.
15 ADA. Report of the Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. JADA. May 2006;137(8):1151-59.
16 Helfenstein U, Steiner M. Fluoride varnishes (Duraphat): a meta-analysis. Community Dent Oral Epidemiol. 1994;22:1-5.
17 Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride varnishes for preventing dental caries in children and adolescents (a review). Cochran Database Syst Rev. 2002;3:CD 002279.
18 Seppa L. Fluoride content of enamel during treatment and 2 years after discontinuation of treatment with fluoride varnishes. Caries Res. 1984;18:278-81.
19 Seppa L, Tuutti H, Luoma H. Post-treatment effect of fluoride varnishes in children with a high prevalence of dental caries in a community with fluoridated water. J Dent Res. 1984;63:1221-22.
20 Petersson LG, Arthursson L, Östberg C, Jonssön G, Gleerup A. Caries-inhibiting effects of different modes of Duraphat varnish reapplications: a 3-year radiographic study. Caries Res. 1991;24:70-73.
21 Skold L, Sundquist B, Eriksson B, Edeland C. Four-year study of caries inhibition of intensive Duraphat application in 11-15-year-old children. Community Dent Oral Epidemiol. 1994;22:8-12.
22 Weintraub JA, Ramos-Gomez F, Jue B, Shain S, Hoover C, Featherstone J, Gansky S. Fluoride varnish efficacy in preventing early childhood caries. J Dent Res. 2006;85:172-76.
23 Stearns SC, Rozier RG, Pahel BT, Park JY, Quinonez RB.

8 www.ineedce.com
Effects of expanding preventive dental care in medical offices for young children covered by Medicaid. http://apha.confex.com/apha/135am/techprogram/paper_160757.htm. Accessed June 2010.
24 Miller EK, Vann WF. The use of fluoride varnish in children: a critical review with treatment recommendations. J Clin Pediatri Dent. 2008;32(4):259-64.
25 Marinho VC, Higgins JP, Logan S, Sheiham A. A systematic review of controlled trials on the effectiveness of fluoride gels for the prevention of dental caries in children. J Dent Edu. 2003;67:448-58.
26 Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2002;(3):CD002279.
27 Farhadian N, Miresmaeili A, Eslami B, Mehrabi S. Effect of fluoride varnish on enamel demineralization around brackets: an in-vivo study. Am J Orthod Dentofacial Orthop. 2008 Apr;133(4 Suppl):S95-98.
28 Vivaldi-Rodrigues G, Demito CF, Bowman SJ, Ramos AL. The effectiveness of a fluoride varnish in preventing the development of white spot lesions. World J Orthod. 2006 Summer;7(2):138-44.
29 Gontijo L, de Almeida Cruz R, Brandao PR. Dental enamel around fixed orthodontic appliances after fluoride varnish application. Braz Dent J. 2007;18(1):49-53.
30 Schaeken MJ, Keltjens HM, VanDer Hoeven JS. Effects of fluoride and chlorhexidine on the microflora of dental root surfaces and progression of root-surface caries. J. Dent Res. 1991 Feb;70(2):150-53.
31 Fure S, Lingstrom P. Evaluation of different fluoride treatments of initial root carious lesions in vivo. Oral Health Prev Dent. 2009;(7):147-54.
32 Schaeken MJ, Keltjens HM, VanDer Hoeven JS. Effects of fluoride and chlorhexidine on the microflora of dental root surfaces and progression of root-surface caries. J. Dent Res. 1991 Feb;70(2):150-53.
33 Merika K, HeftitArthur F, Preshaw PM. Comparison of two topical treatments for dentine sensitivity. Eur J Prosthodont Restor Dent. 2006 Mar;14(1):38-41.
34 Olusile AO, Bamise CT, Oginni AO, Dosumu OO. Short-term clinical evaluation of four desensitizing agents. J Contemp Dent Pract. 2008 Jan 1;9(1):22-29.
35 Hoang-Dao BT, Hoang-Tu H, Tran-Thi NN, Koubi G, Camps J, et al. Clinical efficiency of a natural resin fluoride varnish (Shellac F) in reducing dentin hypersensitivity. J Oral Rehabil. 2009;36(2):124-31.
36 Landry RG, Voyer R. Treatment of dentin hypersensitivity: a retrospective and comparative study of two therapeutic approaches. J Can Dent Assoc. 1990;56(11):1035-41.
37 Miller EK, Vann WF. The use of fluoride varnish in children: a critical review with treatment recommendations. J Clin Pediatri Dent. 2008;32(4):259-64.
38 Ekstrand J, Koch G, Petersson LG. Plasma fluoride concentration and urinary fluoride excretion in children following application of the fluoride-containing varnish Duraphat. Caries Res. 1980;14:185-89.
39 Beltran-Aguilar ED, Goldstein JW, Lockwood SA. Fluoride varnishes: a review of their clinical use, cariostatic mechanism, efficacy and safety. J Am Dent Assoc. 2000;131:589-96.
40 Isaksson M, Bruz M, Bjorkner B, Niklasson B. Contact allergy to Duraphat. Scand J Dent R. 1993;101:49-51.
41 Miller EK, Vann WF. The use of fluoride varnish in children: a critical review with treatment recommendations. J Clin
Pediatri Dent. 2008;32(4):259-64.42 Vaikuntam J. Fluoride varnishes: should we be using them?
Pediatr Dent. 2000;22(6):513-16.43 Seppa L. Effect of dental plaque on fluoride uptake by
enamel from a sodium fluoride varnish in vivo. Caries Res. 1983;17:71-75.
Author ProfilesN. Sue Seale, DDS, MSDDr. N. Sue Seale is Regents Professor, Department of Pediatric Dentistry, Baylor College of Dentistry, Texas A&M Health Sci-ence Center in Dallas, Texas. She received her DDS in 1970, her certificate in pediatric dentistry in 1972 and her MSD in 1979 from Baylor and has been a full-time faculty member since 1974. She was president of the Texas Academy of Pediatric Dentistry 1996-1997 and received the Distinguished Alumni Award from the Baylor College of Dentistry Alumni Association in 1997; she served on the Board of Trustees of the American Academy of Pediatric Dentistry from 1999-2002. In 2001, the American Academy of Pediatric Dentistry named her Pediatric Dentist of the Year and presented her with the Merle C. Hunter Leadership Award in 2003. She is a diplomate of the American Board of Pedi-atric Dentistry and received Fellowship in the American College of Dentists in 1984 and in the International College of Dentists in 2001. She was Chairman of the Department of Pediatric Dentistry at Baylor from 1986 until 2009.
Diane M. Daubert, RDH, MSMs. Daubert currently works as an affiliate instructor in the de-partment of periodontics at the University of Washington and is also responsible for the management of a faculty intramural prac-tice in the graduate periodontal clinic where she is also the coordi-nator for clinical research projects. Diane received the University of Washington School of Dentistry Distinguished Staff Award in 2003. She is a member of the American Dental Hygienist’s As-sociation, Washington State Dental Hygienist’s Association, and the American Dental Education Association. Diane received her Bachelor of Science degree in Dental Hygiene from the University of Washington and her Master of Science in 2009. She is currently enrolled in the PhD program in Oral Biology at the University of Washington.
AcknowledgmentFigure 2 courtesy of Dr. Michael Florman. Figures 3a and 3b courtesy of Dr. Simon Lin. Cover tooth illustration © Andreus | Dreamstime.com
DisclaimerThe author(s) of this course has/have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
Reader FeedbackWe encourage your comments on this or any PennWell course. For your convenience, an online feedback form is available at www.ineedce.com.

Online CompletionUse this page to review the questions and answers. Return towww.ineedce.comand sign in. If you have not previously purchased the program select it from the “Online Courses” listing and complete the online purchase. Once purchased the exam will be added to your Archives page where a Take Exam link will be provided. Click on the “Take Exam” link, complete all the program questions and submit your answers. An immediate grade report will be provided and upon receiving a passing grade your “Verification Form” will be provided immediately for viewing and/or printing. Verification Forms can be viewed and/or printed anytime in the future by returning to the site, sign in and return to your Archives Page.
Questions
1. Recognition of the role of _________ in caries reduction led to the development of other modes of fluoride delivery.a. topical fluorideb. topical iodidec. fluoridated waterd. all of the above
2. Sodium fluoride varnish is cleared by the Food and Drug Administration (FDA) for use as a _________.a. desensitizing agent b. desensitizing agent and cavity linerc. desensitizing agent and caries preventived. none of the above
3. Professional topical fluorides act to _________.a. inhibit remineralization and promote demineralizationb. inhibit demineralization and promote remineralizationc. promote the status quo with incipient lesionsd. all of the above
4. Fluoride varnish utilizes ________ that facilitates adherence of the varnish to the teeth and prolongs the contact time between fluoride and the tooth surfaces.a. an agar gum baseb. a natural tree resin basec. a colloidal based. none of the above
5. As desensitizing agents, fluorides work by _________.a. blocking nerve transmissionb. ameliorating nerve transmissionc. blocking dentinal tubulesd. all of the above
6. The American Dental Association’s Council on Scientific Affairs published recommenda-tions on the use of available professional topical fluorides in ________.a. March 2004b. May 2006c. July 2008d. January 2010
7. The use of ________ is recommended for patients less than 6 years of age at moderate or high risk for caries.a. fluoride varnishb. fluoride varnish or gelc. fluoride varnish, gel or foamd. none of the above
8. The use of 1-minute products (gels and foams) is _________.a. strongly endorsedb. ineffectivec. never advisedd. none of the above
9. Fluoride varnish or gel at 6 month intervals is recommended for children _________.a. age 6 and olderb. under age 6c. over age 13 onlyd. a and b
10. In order to provide evidence-based patient care, it is necessary to know the patient’s _________.a. caries scaleb. caries riskc. caries futured. all of the above
11. _________ is a caries risk factor.a. Submicrobial fluoride exposureb. Suboptimal fluoride exposurec. Lack of fluoride exposured. b and c
12. Incipient or cavitated carious lesions are only a risk factor if they have occurred in the last _________ years.a. sevenb. sixc. fived. none of the above
13. One meta-analysis found overall caries reductions of _________ with the use of fluoride varnishes.a. 28%b. 38%c. 48%d. none of the above
14. An intensive fluoride varnish regimen would be appropriate for _________ who might not be available on a regular two to four times a year schedule.a. immobile individualsb. highly mobile individualsc. low caries risk patientsd. all of the above
15. Prior to the introduction of _________, there was no safe way to administer topical fluoride to children 0-3 years of age.a. fluoride gelb. fluoride rinsec. fluoride varnishd. all of the above
16. Stearns et al. reported that children 6-44 months of age who had four or more visits where varnish was applied as a part of a pre-ventive/referral service showed a _________ reduction in caries-related treatment in anterior teeth.a. 19%b. 29%c. 39%d. 49%
17. In children ages 6-18 years with moderate and high caries risk, there is strong evidence to support the use of _________.a. fluoride varnish every 6 monthsb. fluoride gel every six monthsc. fluoride varnish every 3 months in high risk childrend. all of the above
18. Orthodontic appliances can _________ the risk for enamel demineralization around brackets.a. decreaseb. maintainc. increased. none of the above
19. Data on the effectiveness of fluoride varnish being superior to other treatment options for root caries is _________.a. unequivocalb. equivocalc. overwhelmingd. none of the above
20. The primary use for fluoride varnish in adults is for_________.
a. remineralization or control of root caries in older patients
b. prevention of caries in high-risk adultsc. treatment of dentinal sensitivityd. all of the above
21. Fluoride varnish can be effective for up to _________ for sensitivity relief.a. one to two yearsb. three yearsc. three to six monthsd. six to twelve months
22. Fluoride gel is recommended for patients _________ at risk for caries.a. under age 6b. under age 3c. age 6 and overd. all of the above
23. Fluoride varnish is contraindicated if a patient _________.a. has ulcerative gingivitisb. has stomatitisc. is allergic to one of the ingredientsd. all of the above
24. One milliliter of the varnish contains _________.a. 2.26 mg fluoride/mlb. 22.6 mg fluoride/mlc. 226 mg fluoride/mld. none of the above
25. Infants require _________ of fluoride varnish.a. 0.1 mlb. 0.4 mlc. 0.75 mld. none of the above
26. The dose of fluoride varnish for the mixed dentition is _________.a. 0.2 mlb. 0.4 mlc. 0.6 mld. 0.8 ml
27. Following application of fluoride varnish, the patient _________.a. must avoid earing hard, crunchy or hot foodsb. must avoid drinking hot liquids or liquids containing alcoholc. should resume regular oral hygiene the following dayd. all of the above
28. Following application of fluoride gel, the patient _________.a. should refrain from eating for at least 30-60 minutesb. should refrain from drinking for at least 30-60 minutesc. should refrain from crunchy foods for a dayd. a and b
29. When only a _________ is present, fluoride varnish can be directly applied without prior removal of the plaque.a. the pellicleb. a thick layer of plaquec. a thin layer of plaqued. all of the above
30. The selection of a professional topical fluoride should be guided by _________.a. scientific evidenceb. age and risk level of the patientc. specific intra-oral considerationsd. all of the above

PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.
Ifnottakingonline,mailcompletedanswersheetto
Academy of Dental Therapeutics and Stomatology,A Division of PennWell Corp.
P.O.Box116,Chesterland,OH44026orfaxto:(440)845-3447
Customer Service 216.398.7822
For IMMedIate results, go to www.ineedce.com to take tests online.
answer sheets can be faxed with credit card payment to (440) 845-3447, (216) 398-7922, or (216) 255-6619.
�Paymentof$49.00isenclosed.(Checks and credit cards are accepted.)
Ifpayingbycreditcard,pleasecompletethefollowing: MC Visa AmEx Discover
Acct.Number:______________________________
Exp.Date:_____________________
Charges on your statement will show up as PennWell
AUTHOR DISCLAIMERThe author(s) of this course has/have no commercial ties with the sponsors or the providers of the unrestricted educational grant for this course.
SPONSOR/PROVIDERThis course was made possible through an unrestricted educational grant. No manufacturer or third party has had any input into the development of course content. All content has been derived from references listed, and or the opinions of clinicians. Please direct all questions pertaining to PennWell or the administration of this course to Machele Galloway, 1421 S. Sheridan Rd., Tulsa, OK 74112 or [email protected].
COURSE EVALUATION and PARTICIPANT FEEDBACKWe encourage participant feedback pertaining to all courses. Please be sure to complete the survey included with the course. Please e-mail all questions to: [email protected].
INSTRUCTIONSAll questions should have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification forms will be mailed within two weeks after taking an examination.
EDUCATIONAL DISCLAIMERThe opinions of efficacy or perceived value of any products or companies mentioned in this course and expressed herein are those of the author(s) of the course and do not necessarily reflect those of PennWell.
Completing a single continuing education course does not provide enough information to give the participant the feeling that s/he is an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
COURSE CREDITS/COSTAll participants scoring at least 70% on the examination will receive a verification form verifying 2 CE credits. The formal continuing education program of this sponsor is accepted by the AGD for Fellowship/Mastership credit. Please contact PennWell for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California Provider. The California Provider number is 4527. The cost for courses ranges from $49.00 to $110.00.
Many PennWell self-study courses have been approved by the Dental Assisting National Board, Inc. (DANB) and can be used by dental assistants who are DANB Certified to meet DANB’s annual continuing education requirements. To find out if this course or any other PennWell course has been approved by DANB, please contact DANB’s Recertification Department at 1-800-FOR-DANB, ext. 445.
RECORD KEEPINGPennWell maintains records of your successful completion of any exam. Please contact our offices for a copy of your continuing education credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
CANCELLATION/REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
© 2010 by the Academy of Dental Therapeutics and Stomatology, a division of PennWell
AGD Code 258, 430
ANSWER SHEET
The Use and Efficacy of Professional Topical Fluorides
Name: Title: Specialty:
Address: E-mail:
City: State: ZIP: Country:
Telephone:Home() Office() Lic.RenewalDate:
Requirementsforsuccessfulcompletionofthecourseandtoobtaindentalcontinuingeducationcredits:1)Readtheentirecourse.2)Completeallinformationabove.3)Completeanswersheetsineitherpenorpencil.4)Markonlyoneanswerforeachquestion.5)Ascoreof70%onthistestwillearnyou2CEcredits.6)CompletetheCourseEvaluationbelow.7)MakecheckpayabletoPennWellCorp.For Questions Call 216.398.7822
Educational Objectives1. ListthetypesofprofessionaltopicalfluoridesthatareavailableintheUSandCanada
2. ListanddescribetheADArecommendationsontheuseofprofessionaltopicalfluorides
3. Listanddescribetheevidenceonefficacyandsafetyforsodiumfluoridevarnishes
4. Listanddescribethemethodsbywhichdifferentprofessionaltopicalfluoridescanbeapplied
Course EvaluationPleaseevaluatethiscoursebyrespondingtothefollowingstatements,usingascaleofExcellent=5toPoor=0.
1.Weretheindividualcourseobjectivesmet? Objective#1:YesNo Objective#3:YesNo
Objective#2:YesNo Objective#4:YesNo
2.Towhatextentwerethecourseobjectivesaccomplishedoverall? 5 4 3 2 1 0
3.Pleaserateyourpersonalmasteryofthecourseobjectives. 5 4 3 2 1 0
4.Howwouldyouratetheobjectivesandeducationalmethods? 5 4 3 2 1 0
5.Howdoyouratetheauthor’sgraspofthetopic? 5 4 3 2 1 0
6.Pleaseratetheinstructor’seffectiveness. 5 4 3 2 1 0
7.Wastheoveralladministrationofthecourseeffective? 5 4 3 2 1 0
8.Doyoufeelthatthereferenceswereadequate? Yes No
9.Wouldyouparticipateinasimilarprogramonadifferenttopic? Yes No
10.Ifanyofthecontinuingeducationquestionswereunclearorambiguous,pleaselistthem.
___________________________________________________________________
11.Wasthereanysubjectmatteryoufoundconfusing?Pleasedescribe.
___________________________________________________________________
___________________________________________________________________
12.Whatadditionalcontinuingdentaleducationtopicswouldyouliketosee?
___________________________________________________________________
___________________________________________________________________