Embed Size (px)
Citation preview
PENSACOLA PODIATRY, P.A. Frank J. Castagna, DPM, FACFAS
Matthew H. Etheridge, DPM, FACFAS Diplomates, American Board of Podiatric Surgery
WELCOME
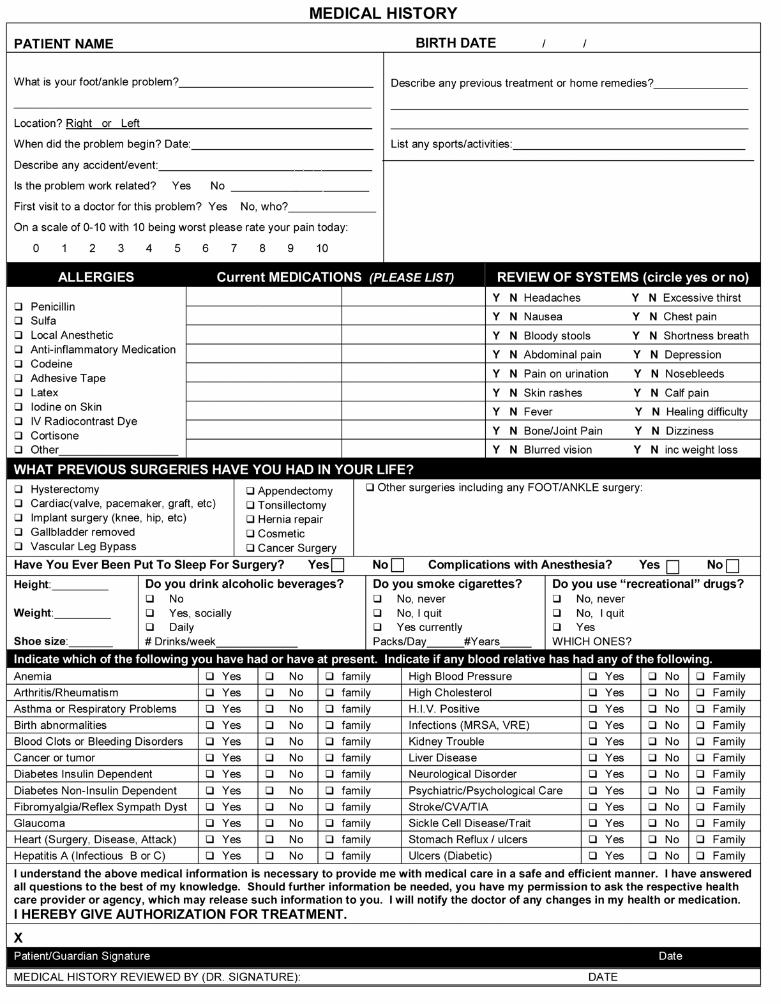
Thank you for the opportunity of adding you to the growing family of satisfied patients of Pensacola Podiatry, P.A. Our goal is to provide you with the best medical care available in a relaxed warm atmosphere. The information you gave us at the onset of your appointment was the first step to assist us in better serving you as our valued patient. We feel that mailing you the attached paperwork prior to your appointment will save valuable time that can be better spent with the physician. Please complete the enclosed paperwork prior to your appointment and bring it with you along with your insurance ID Card, a picture ID card and any other information as may be required in your insurance handbook. Please arrive 20 minutes before your scheduled appointment time. If you cannot keep your appointment as scheduled, we expect our patients to grant us the courtesy of notifying us within 24-hours in order to give that time to another patient. If you are being seen for a second opinion, or have seen another doctor for foot problems or past surgery, please bring your past medical records, x-rays, MRIs or any other diagnostic reports with you. This will assist the doctor in providing you with the best care and address your foot problems during your first visit so you can get on the road to recovery. If your insurance requires an authorization, it will be your responsibility to furnish that at the time of your visit. As a courtesy to our patients, we will verify your insurance benefits prior to your appointment. Payment for insurance co-pays, deductibles or coinsurance amounts as well as non-covered services by your insurance company are due at the time the services are rendered. For your convenience we accept cash, personal checks, Visa and MasterCard. Please do not hesitate to call our office if you have any questions. We look forward to treating you. Sincerely, Doctors & Staff Pensacola Podiatry, P.A.
Frank J. Castagna, DPM, FACFAS
Matthew H. Etheridge, DPM, FACFAS
6160 N. Davis Hwy, Ste 1Pensacola, FL, 32504
(850) 476-2805
www.pensacolapodiatry.com
8333 N .Davis HwyPensacola, FL32514
(850) 969-2550
5211 Hwy 90Milton, FL 32571(850) 994-0927
!"#$%&'(%)!'*+%,-./)!010)2-%#3)40)5%$,%6#%/)7!8/)215219)8%,,:";)<0)=,:"-+*6"/)7!8/)215219)!"#$%&'!#(!)*%+,&-!)*,&$%&'.!/(('&$%+'!"#+'01'*!234!5667!>:+$)#',+&")*"$&-+?"$):';):"%(,:.)+#@'-A%,+'#)%?'B,).'B/)%$)%)C%,+"#,)'@),:+$)C-%&,+&"/)A%.)?")B$"*)%#*)*+$&('$"*/)%#*):';).'B)&%#)6",)%&&"$$),').'B-):"%(,:)+#@'-A%,+'#0)>:+$)+$)-"DB+-"*)?.),:")!-+E%&.)F"6B(%,+'#$)&-"%,"*)%$)%)-"$B(,)'@),:")<"%(,:)G#$B-%#&")!'-,%?+(+,.)%#*)1&&'B#,%?+(+,.)1&,)'@)HIIJ)K<G!!1L0)!89*!�%$0':$!$#!-#9*!;*%+,&-!MB-)C-%&,+&")+$)*"*+&%,"*),')A%+#,%+#+#6),:")C-+E%&.)'@).'B-):"%(,:.)+#@'-A%,+'#0)N")%-")-"DB+-"*)?.)(%;),')A%+#,%+#),:")&'#@+*"#,+%(+,.)'@).'B-):"%(,:)+#@'-A%,+'#0)N")-"%(+O"),:%,),:"$")(%;$)%-")&'AC(+&%,"*/)?B,);")AB$,)C-'E+*").'B);+,:),:")@'((';+#6)+AC'-,%#,)+#@'-A%,+'#P)!<.'!,:=!=%.&>#.9*'!#(!-#9*!?',>$?!%:(#*0,$%#:!%:!&'*$,%:!.;'&%,>!&%*&90.$,:&'.!>:")@'((';+#6)&+-&BA$,%#&"$)A%.)-"DB+-")B$),')B$")'-)*+$&('$").'B-):"%(,:.)+#@'-A%,+'#P))2@)>')CB?(+&):"%(,:)%B,:'-+,+"$)%#*):"%(,:)'E"-$+6:,)%6"#&+"$),:%,)%-")%B,:'-+O"*)?.)(%;),')&'(("&,)+#@'-A%,+'#0))5@)Q%;$B+,$)%#*)$+A+(%-)C-'&""*+#6$)+#)-"$C'#$"),')%)&'B-,)'-)%*A+#+$,-%,+E")'-*"-0))A@)G@)-"DB+-"*),')*')$')?.)%)(%;)"#@'-&"A"#,)'@@+&+%(0))7@)N:"#)#"&"$$%-.),')-"*B&")'-)C-"E"#,)%)$"-+'B$),:-"%,),').'B-):"%(,:)%#*)$%@",.)'-),:"):"%(,:)%#*)$%@",.)'@)%#',:"-)+#*+E+*B%()'-),:")CB?(+&0)N");+(()'#(.)A%3")*+$&('$B-"$),')%)C"-$'#)'-)'-6%#+O%,+'#)%?("),'):"(C)C-"E"#,),:"),:-"%,0))3@)G@).'B)%-")%)A"A?"-)'@)R090)'-)@'-"+6#)A+(+,%-.)@'-&"$)K+#&(B*+#6)E","-%#$L)%#*)+@)-"DB+-"*)?.),:")%CC-'C-+%,")%B,:'-+,+"$0))B@)>')@"*"-%()'@@+&+%($)@'-)+#,"((+6"#&")%#*)#%,+'#%()$"&B-+,.)%&,+E+,+"$)%B,:'-+O"*)?.)(%;0))C@)>')&'--"&,+'#%()+#$,+,B,+'#$)'-)(%;)"#@'-&"A"#,)'@@+&+%($)+@).'B)%-")%#)+#A%,")'-)B#*"-),:")&B$,'*.)'@)%)(%;)"#@'-&"A"#,)'@@+&+%(0))D@)2'-)N'-3"-$)5'AC"#$%,+'#)%#*)$+A+(%-)C-'6-%A$0)!E#9*!*%F?$.!*'F,*=%:F!-#9*!?',>$?!%:(#*0,$%#:!2@))5'AAB#+&%,+'#$0)S'B)&%#)-"DB"$,),:%,)'B-)C-%&,+&")&'AAB#+&%,");+,:).'B)%?'B,).'B-):"%(,:)%#*)-"(%,"*)+$$B"$)+#)%)C%-,+&B(%-)A%##"-)'-)%,)%)&"-,%+#)('&%,+'#0)2'-)+#$,%#&"/).'B)A%.)%$3),:%,);")&'#,%&,).'B)%,):'A"/)-%,:"-),:%#);'-30)N");+(()%&&'AA'*%,")-"%$'#%?(")-"DB"$,$0)5@))S'B)&%#)-"DB"$,)%)-"$,-+&,+'#)+#)'B-)B$")'-)*+$&('$")'@).'B-):"%(,:)+#@'-A%,+'#)@'-),-"%,A"#,/)C%.A"#,)'-):"%(,:)&%-")'C"-%,+'#$0)1**+,+'#%((./).'B):%E"),:")-+6:,),')-"DB"$,),:%,);")-"$,-+&,)'B-)*+$&('$B-")'@).'B-):"%(,:)+#@'-A%,+'#),')'#(.)&"-,%+#)+#*+E+*B%($)+#).'B-)&%-")'-),:")C%.A"#,)@'-).'B-)&%-"/)$B&:)%$)@%A+(.)A"A?"-$)%#*)@-+"#*$0)N")%-")#',)-"DB+-"*),')%6-""),').'B-)-"DB"$,T):';"E"-/)+@);")*')%6-""/);")%-")?'B#*)?.)'B-)%6-""A"#,)"U&"C,);:"#)',:"-;+$")-"DB+-"*)?.)(%;/)+#)"A"-6"#&+"$/)'-);:"#),:")+#@'-A%,+'#)+$)#"&"$$%-.),'),-"%,).'B0)A@))S'B):%E"),:")-+6:,),')+#$C"&,)%#*)'?,%+#)%)&'C.)'@),:"):"%(,:)+#@'-A%,+'#),:%,)A%.)?")B$"*),')A%3")*"&+$+'#$)%?'B,).'B/)+#&(B*+#6)C%,+"#,)A"*+&%()-"&'-*$)%#*)?+((+#6)-"&'-*$/)?B,)#',)+#&(B*+#6)C$.&:',:"-%C.)#',"$0)S'B)AB$,)$B?A+,).'B-)-"DB"$,)+#);-+,+#6),'),:")M@@+&")8%#%6"-0)7@))S'B)A%.)%$3)B$),')%A"#*).'B-):"%(,:)+#@'-A%,+'#)+@).'B)?"(+"E")+,)+$)+#&'--"&,)'-)+#&'AC(","/)%#*)%$)('#6)%$),:")+#@'-A%,+'#)+$)3"C,)?.)'-)@'-)'B-)C-%&,+&"0)>')-"DB"$,)%#)%A"#*A"#,/).'B-)-"DB"$,)AB$,)?")A%*")+#);-+,+#6)%#*)$B?A+,,"*),'),:")M@@+&")8%#%6"-0))S'B)AB$,)C-'E+*")B$);+,:)%)-"%$'#),:%,)$BCC'-,$).'B-)-"DB"$,)@'-)%A"#*A"#,0)3@))F+6:,),')%)&'C.)'@),:+$)#',+&"0)S'B)%-")"#,+,("*),')-"&"+E")%)&'C.)'@),:+$)V',+&")'@)!-+E%&.)!-%&,+&"0)B@))F+6:,),')@+(")%)&'AC(%+#,0)G@).'B)?"(+"E").'B-)C-+E%&.)-+6:,$):%E")?""#)E+'(%,"*/).'B)A%.)@+(")%)&'AC(%+#,);+,:)'B-)C-%&,+&")'-);+,:),:")9"&-",%-.)'@),:")7"C%-,A"#,)'@)<"%(,:)%#*)<BA%#)9"-E+&"$0)>')@+(")%)&'AC(%+#,);+,:)'B-)C-%&,+&"/)&'#,%&,),:")M@@+&")8%#%6"-0)1(()&'AC(%+#,$)AB$,)?")$B?A+,,"*)+#);-+,+#60)S'B);+(()#',)?")C"#%(+O"*)@'-)@+(+#6)%)&'AC(%+#,0)C@))F+6:,),')C-'E+*")%#)%B,:'-+O%,+'#)@'-)',:"-)B$"$)%#*)*+$&('$B-"$0)MB-)C-%&,+&");+(()'?,%+#).'B-);-+,,"#)%B,:'-+O%,+'#)@'-)B$"$)%#*)*+$&('$B-"$),:%,)%-")#',)+*"#,+@+"*)?.),:+$)#',+&")'-)C"-A+,,"*)?.)%CC(+&%?(")(%;0)))G@).'B):%E")%#.)DB"$,+'#$)-"6%-*+#6),:+$)#',+&")'-)'B-):"%(,:)+#@'-A%,+'#)C-+E%&.)C'(+&+"$/)C("%$")&'#,%&,)B$)%,)%?'E")('&%,+'#0)
)!
6160 N. Davis Hwy, Ste 1 8333 N. Davis Hwy 5211 Hwy 90 Pensacola, FL 32504 Pensacola, FL 32514 Milton, FL 32571 (850) 476 – 2805 (850) 969 -‐ 2550 (850) 994 -‐ 0927
Pensacola Podiatry, P.A. Frank J. Castagna, DPM, FACFAS
Matthew H. Etheridge, DPM, FACFAS Diplomates, American Board of Podiatric Surgery
Patient name:________________________________________________ The Practice: a. Is required by federal law to maintain the privacy of your Personal Health Information (PHI) and to provide you with this Privacy Notice detailing the Practice’s legal duties and privacy practices with respect to your PHI. b. Under the Privacy Rule, may be required by State law to grant greater access or maintain greater restrictions on the use or release of your PHI than that which is provided for under federal law. c. is required to abide by the terms of this Privacy Notice. d. Reserves the right to change the terms of this Privacy Notice and to make the new Privacy Notice provisions effective for your entire PHI that it maintains. e. Will distribute any revised Privacy Notice to you prior to implementation. f. Will not retaliate against you for filing a complaint.
EFFECTIVE DATE This notice is effective as of 11/15/04
PATIENT ACKNOWLEDGMENT
By signing my name below, I acknowledge receipt of a copy of this Notice, and my understanding and agreement to its terms. Print Name:_________________________________________________________________________________ Signature: __________________________________________________________________________________ Date: ____________________________________________________

![FIALLUX VARI]S - The Podiatry Institute · 2015. 9. 17. · CHAPTER 38 FIALLUX VARI]S Scott R..lolrn A. Roman, DPM Ruclt, DPM INTRODUCTION Hallux varus can be classified as either](https://img.pdfslide.us/doc/110x75/60a4138d91e10948ca4df10f/fiallux-varis-the-podiatry-2015-9-17-chapter-38-fiallux-varis-scott-rlolrn.jpg)