Embed Size (px)
Citation preview
HypertensionPenny Mosley MRPharmS
Outline of presentation
• Introduction to hypertension
• Physiological control of arterial blood pressure
▫ What determines our bp?
▫ What determines the heart rate?
▫ What determines stroke volume?
▫ What determines our peripheral resistance?

Cont.,
• Antihypertensive drugs
▫ Drugs that act on the RAAS
▫ Diuretics
▫ Calcium Channel Blockers
▫ α1 –Adrenergic antagonists
▫ β- adrenergic antagonists
• NICE guideline CG 127
Introducing ‘Andrew’
•35 year old male•PMH: moderate hypertension•SH: lives with fiancée and 2 daughters•Smokes 20 cigarettes/day•Weighs 95kg

Andrew cont.,
• What are you going to do?
• What ‘could’ be his diagnosis?
• What ‘could’ be the consequences of this diagnosis?

Hypertension
• Common in UK1
• One of the most important preventable causes of premature morbidity & mortality1
• One of the major risk factors CHD2
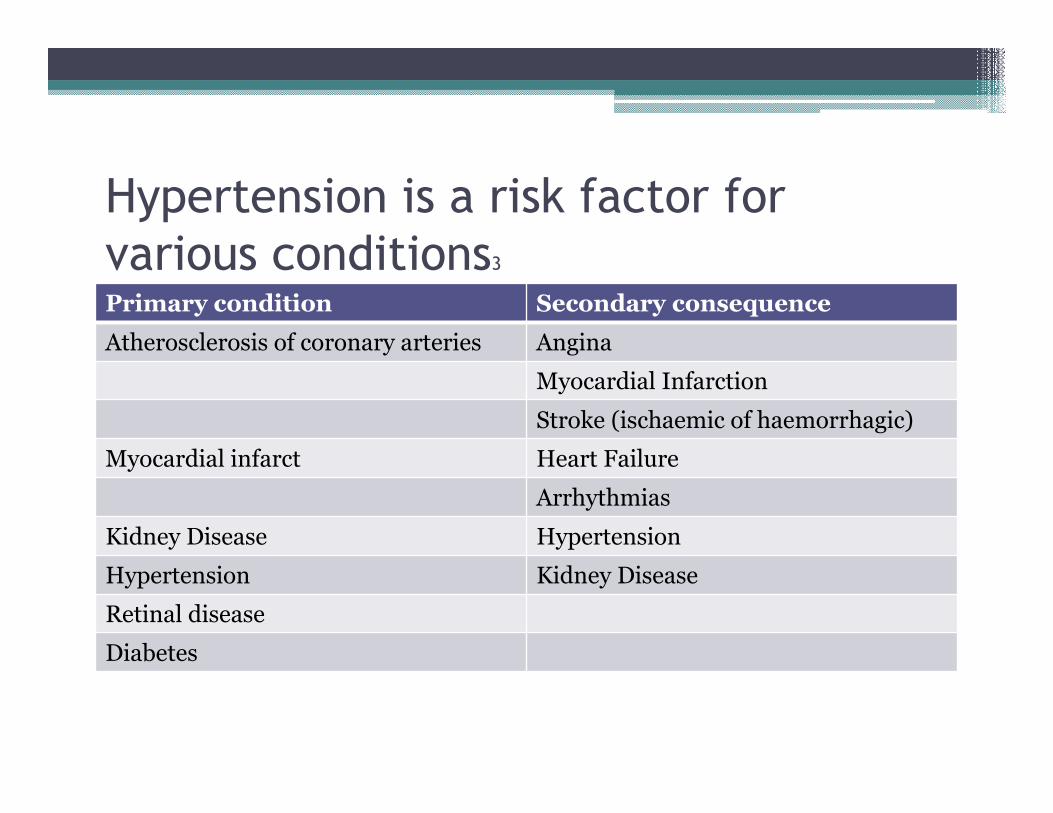
Hypertension is a risk factor for
various conditions3
Primary condition Secondary consequence
Atherosclerosis of coronary arteries Angina
Myocardial Infarction
Stroke (ischaemic of haemorrhagic)
Myocardial infarct Heart Failure
Arrhythmias
Kidney Disease Hypertension
Hypertension Kidney Disease
Retinal disease
Diabetes
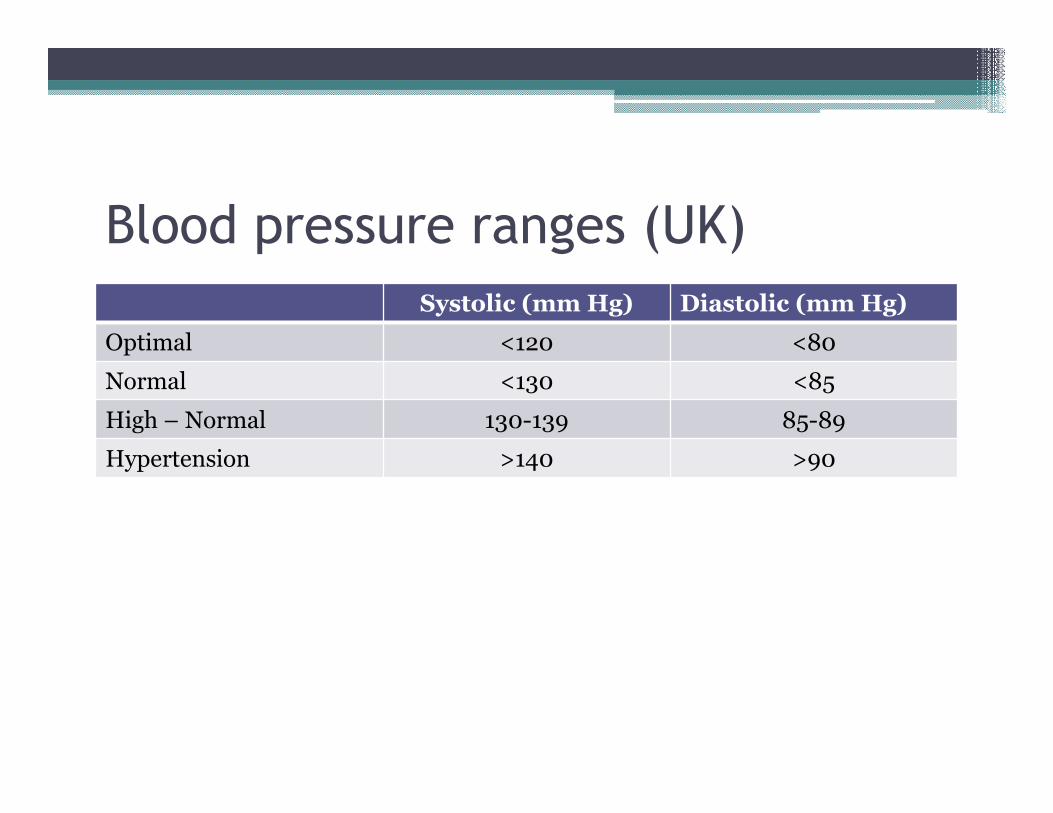
Blood pressure ranges (UK)
Systolic (mm Hg) Diastolic (mm Hg)
Optimal <120 <80
Normal <130 <85
High – Normal 130-139 85-89
Hypertension >140 >90
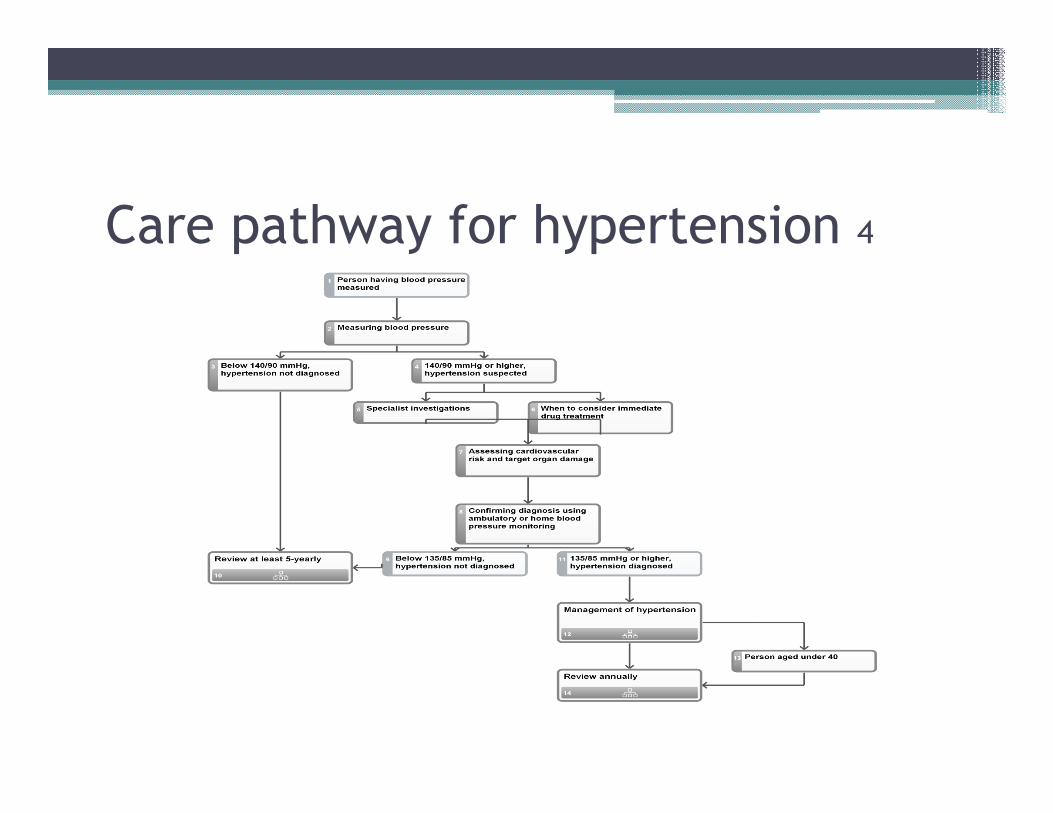
Care pathway for hypertension 4
Physiological control of arterial blood
pressure
• Cardiac Output (CO)
• Total Peripheral Resistance (TPR)
• BP = CO x TPR
What determines Blood Pressure?
• BP = CO x TPR
• CO = HR x SV
• BP = HR x SV x TPR

1. What determines Heart Rate?
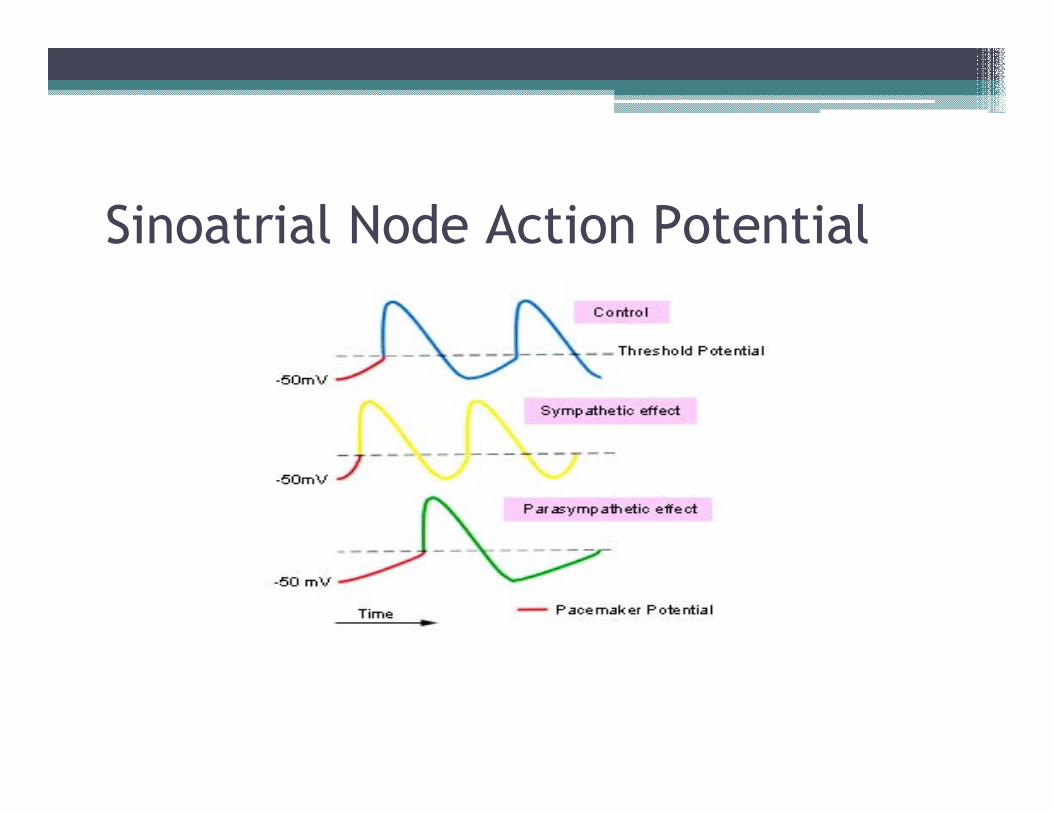
Sinoatrial Node Action Potential

2. What determines Stroke Volume?
• Directly influencing ventricular myocytes
• Indirect influences on SV
▫ Changes to the venous side (Venous return, preload & end diastolic volume)
▫ Changes to the arterial side (BP and afterload)
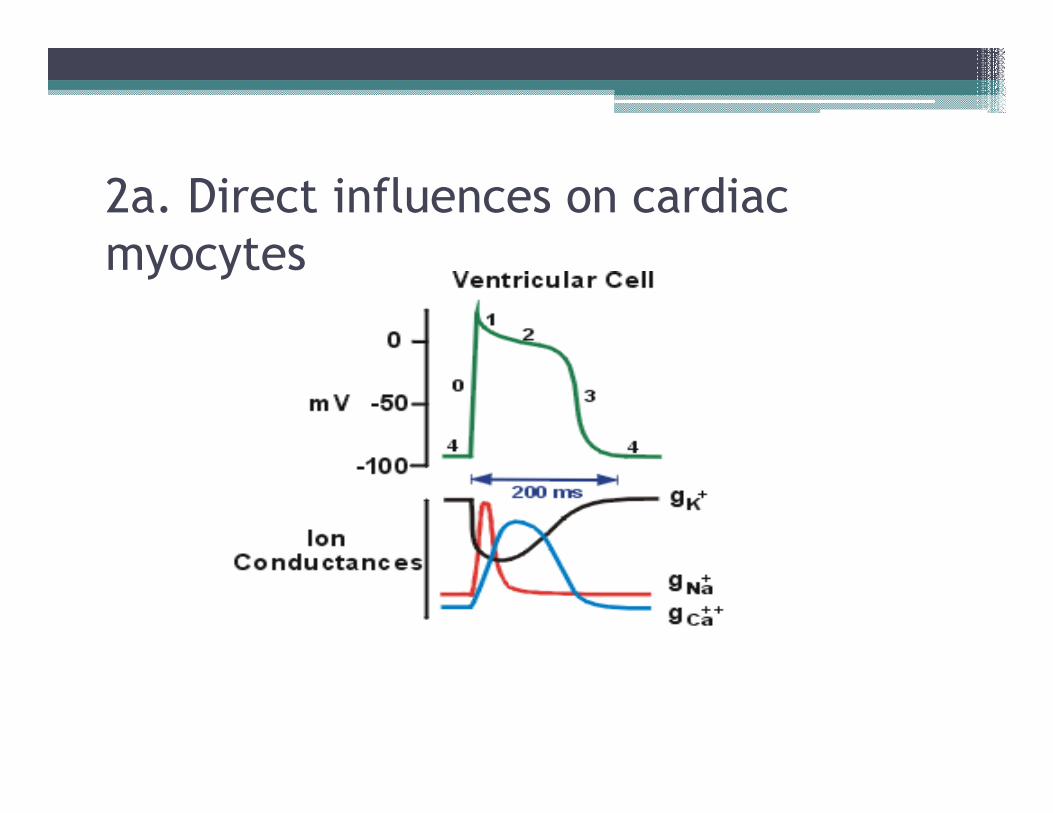
2a. Direct influences on cardiac
myocytes
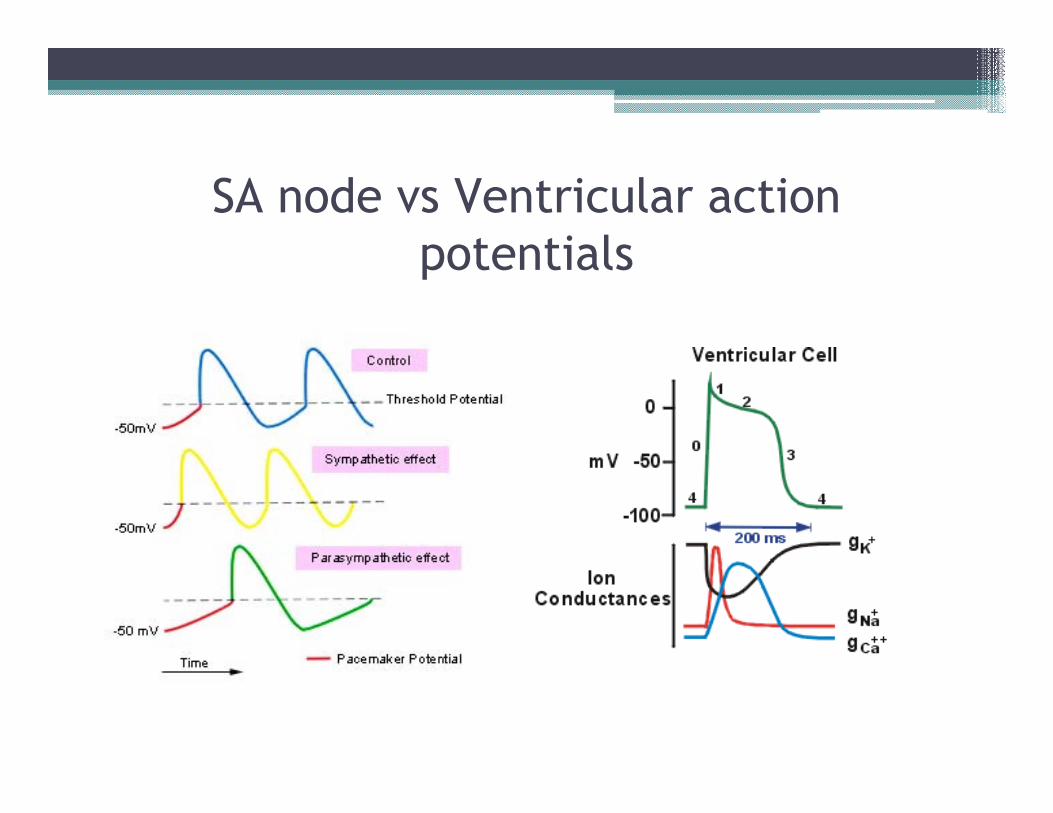
SA node vs Ventricular action
potentials
2b(i). Indirect influences on SV
(venous)• Sympathetic stimulation of large veins
• vasoconstriction
• Valves ensure blood pumped back towards heart
• inc venous return
• inc force of contraction
• inc stroke volume
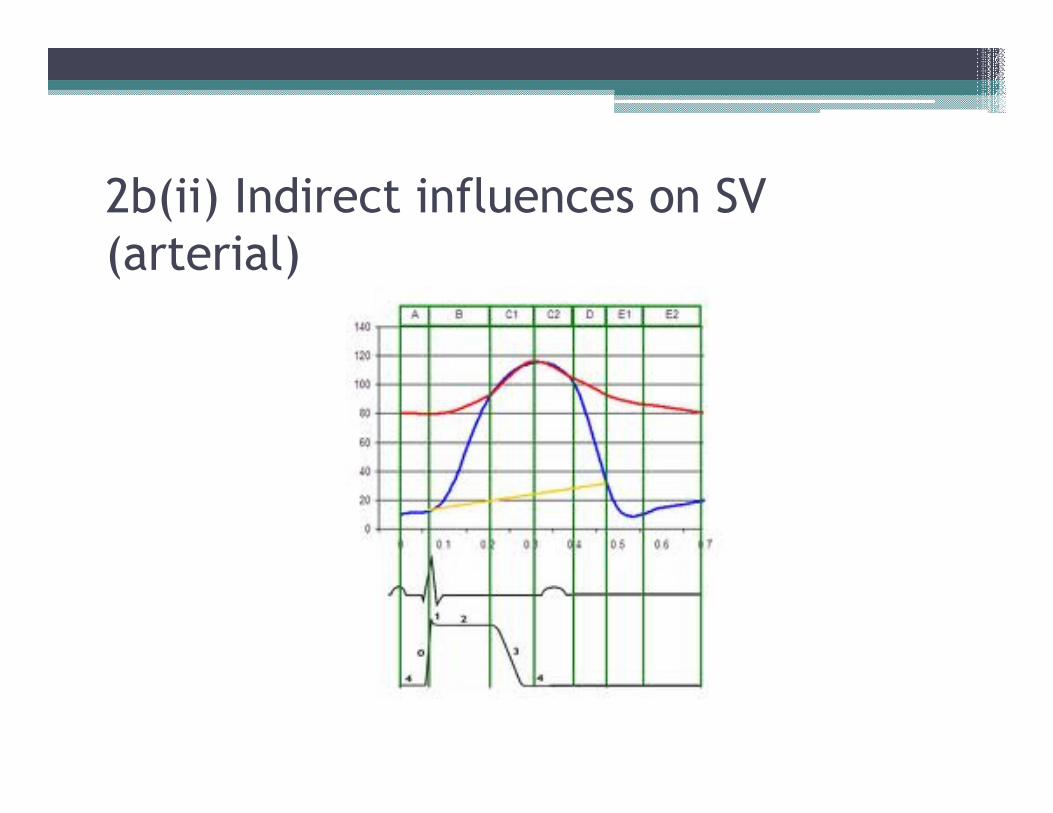
2b(ii) Indirect influences on SV
(arterial)
3. What determines TPR?
• Resistance to blood flow is essential for maintenance of normal BP
• Receptors:
▫ α 1 adrenoceptors -contraction of smooth muscle (dominant action)
▫ β2 adrenoceptors – relaxation

Renin-Aldosterone-Angiotensin System
Problem!!!
• BP = HR x SV x TPR
• Role of baroreceptors in controlling BP
‘Andrew’ has arrived at A & E
•BP 220/140 mm Hg•Pulse 60 beats/ min (normal)•Sodium = 142 mMol/L (135-145)•Potassium = 4.2 mMol/L (3.5-5.5)
•BP = HR x SV x TPR
BP = HR x SV x TPR
• BP = elevated (220/140 mm Hg)
• HR = normal (60 beats / min)
• SV = reduced
• Hence, TPR must be raised??
• Inc (BP) = norm (HR) x red (SV) x inc (TPR)
Quick quiz!!!
• Measure BP
▫ Think about HOW this can be done in your pharmacy – who, where etc??
▫ What things do you need to discuss / question with the patient
Antihypertensive Drugs
• 1. Drugs that act on RAAS
▫ ACE inhibitors
▫ Angiotensin II antagonists
▫ Aldosterone antagonists
• 2. Diuretics
• 3. Calcium Channel blockers
• 4. α-adrenoceptor antagonists
• 5. β-adrenoceptor antagonists
• 6. others
1. ACE Inhibitors
• Reduces
▫ vasoncontriction of Angiotensin II, and
▫ Na retention / water retention
• Causes accumulation of bradykinin
• Potentially serious interaction - ‘triple whammy’
▫ ACE inhibitors
▫ NSAIDS
▫ Diuretics
Angiotensin II antagonists
• Prescribed to patients who can’t tolerate the cough with ACEI
• Similar side effects as ACEI
• Like ACEI cause a down regulation of vasoconstriction and Aldosterone effects

Aldosterone Antagonists
• Not routinely used for hypertension
• Used mainly for HF
• Potassium sparing diuretics
2. Diuretics
• Thiazides - stimulate Na/water excretion
• Act on distal tubule
• Reduces blood volume and cardiac output (& BP)
• Thiazides are weaker than loop diuretics
• Thiazides also have a direct vasodilator effect

3. Calcium Channel Blockers
• Drugs used in Hypertension act on L-type channel
▫ Dihydropyridines (eg Amlodipine)
▫ Verapamil
▫ Diltiazem
• Act in 3 sites
▫ Conducting system of heart – reduces HR
▫ Contractile myocytes – reduces SV
▫ Vascular smooth muscle – reduces TPR

4. α-adrenoceptor antagonists
• Receptors found in smooth muscle –vasoconstriction
• Reduction in BP due to reduction in TPR leads to a compensatory increase in NA (affecting βadrenoceptors in heart) – thus reducing effectiveness as drugs – usually used in combination
5. β-adrenoceptor antagonists
• Not now routinely used for hypertension
• Stimulation of β1 adrenoceptors in heart
▫ Increases heart rate
▫ Increases force of contraction
▫ Increases cardiac output
▫ INCREASES BLOOD PRESSURE
• Problem – Baroreceptors/ feedback mechanism

Β – adrenoceptors antagonists
• Work on:
▫ Heart : reduce CO
▫ Kidney: reduce renin release
▫ Brain: reduce sympathetic nervous system activity
6. Other antihypertensive drugs
• Vasodilators
▫ Sodium Nitroprusside
▫ Minoxidil
▫ Hydralazine
• Centrally acting sympatholytics
▫ Methyldopa
▫ Clonidine
▫ Moxonidine
‘Andrew’ needs rapid reduction of BP
•BP 220/140 mm Hg
•Two options:•Sodium nitroprusside 1/v•Oral labetolol
•After 24 hours: BP 175/100 mm Hg
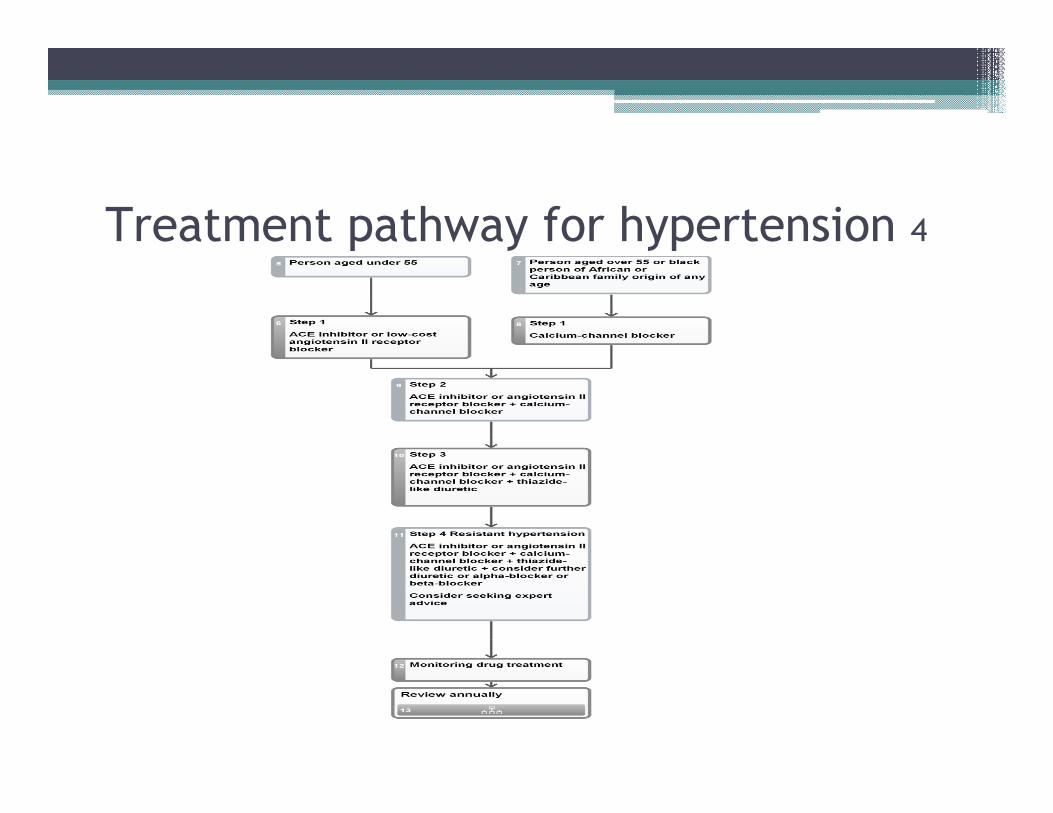
Treatment pathway for hypertension 4

Application: tMURs and NMS
Application: tMURs and NMS
se /complianceressure measurement*
ifestyle*
moking status*ncouragement
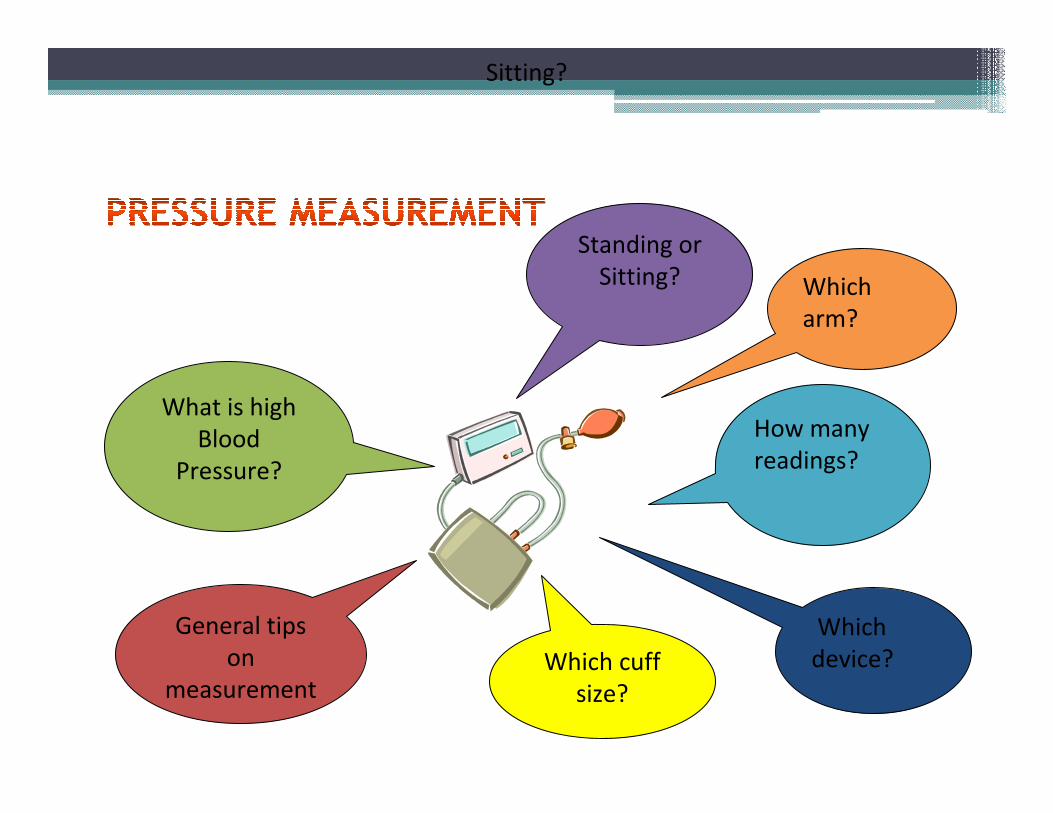
Which
arm?
How many
readings?
Which
device?Which cuff
size?
General tips
on
measurement
What is high
Blood
Pressure?
Sitting?
Standing or
Sitting?
• “Having high blood pressure increases the risk of having a heart attack or stroke….”
• “taking xxx medicine, helps to reduce BP and so reduces this risk”
• “xxx medicine works best if you use them regularly”
• Diet / exercise programs
• Alcohol consumption
• Salt intake
• Local initiatives

• Ask patient if they smoke – add info to form
• Offer smoking cessation advice / support or referral to specialist service if necessary
• NHS choices website www.nhs.uk
• Other websites
▫ British Hypertension Society. www.bhsoc.org
▫ Blood pressure UK. www.bloodpressureuk.org
• Local initiatives
▫ Byou. www.b-you.co.uk
▫ Healthy lifestyle hub. www.dchs.nhs.uk/your_health_useful_info/
References
1. William H. Updated hypertension guideline: What pharmacists need to know. Clinical Pharmacist. 2011.3.254-256
2. Sherwood J, Ashton M, Ferriman H. Current and future options for the management of hypertension. Pharmaceutical Journal. 2011. 286. 48-9
3. Boarder M, Newby, Navti P. Pharmacology for pharmacy and the health sciences. Oxford. Oxford University Press. 2010
4. National Institute for Health and Clinical Excellence. Clinicalguideline 127. Hypertension: clinical management of primary hypertension in adults
5. Shannon R, Davies E. How motivational interviewing can help patients change their lifestyles. Clinical pharmacist. 2010. 2.28
6. Broomhead C. Hypertension targets: improving control and concordance. Prescriber. 2009. 50-53