Embed Size (px)
Citation preview

Mary Andrus, BA, RN, CICMary Andrus, BA, RN, CICInfection Preventionist ConsultantInfection Preventionist Consultant
APIC CONSULTING SERVICES, INC.APIC CONSULTING SERVICES, INC.
Pennsylvania Department of Pennsylvania Department of Health (PADOH) Health (PADOH) –– CLABSI, CLABSI,
CAUTI, and SSI AuditCAUTI, and SSI Audit
Provisional CLABSI ResultsProvisional CLABSI Results
Provisional CLABSI ResultsProvisional CLABSI Results
A total of 120 records were
reviewed

Provisional CLABSI ResultsProvisional CLABSI Results
Auditors reviewed 23 patients that had been
reported to NHSN
Provisional CLABSI ResultsProvisional CLABSI Results
Bloodstream infections that
were reported by hospitals and confirmed by
auditors
Provisional CLABSI ResultsProvisional CLABSI Results
Bloodstream infections that
were reported by hospitals and not
confirmed by auditors

Provisional CLABSI ResultsProvisional CLABSI Results
Total number of positive blood cultures reviewed
by audit.
Provisional CLABSI ResultsProvisional CLABSI Results
Bloodstream infections that
were identified as CLABSI by audit
but were not reported to NHSN
Provisional CLABSI ResultsProvisional CLABSI Results
Positive blood cultures that were not identified
as CLABSI by audit and were not reported
by the hospital to NHSN

CLABSI Misreported CasesCLABSI Misreported Cases
• Under-reported (5)– 3 cases were not reported because the hospital identified the
BSI as secondary to another infection. In each case, the criteria for the primary infection were not met
– 2 cases were missed by the hospital
• Over-reported (4)– 2 cases were reported as a primary BSI (CLABSI) when criteria
for an infection at another site with the same organism was identified by the auditor
– 1 case was reported by the hospital, but it appears to be associated with a CLABSI on an earlier date
– 1 case was reported as CLABSI, but no corresponding blood culture was identified by the auditor
LaboratoryLaboratory --confirmed Bloodstream Infection (LCBI) confirmed Bloodstream Infection (LCBI)
LCBI Criterion 1
Notes about Criterion 1Notes about Criterion 1

� Common commensal� Diphtheroids
(Corynebacterium spp.)
� Bacillus spp. (not B.anthracis)
� Proprionibacterium spp.
� Coagulase-negative staphylococci (including S. epidermidis)
� Viridans group streptococci
� Aerococcus spp.� Micrococcus spp.
LaboratoryLaboratory --confirmed bloodstream infection confirmed bloodstream infection (LCBI)(LCBI)
LCBI Criterion 2
commensal
Two or more blood cultures on separate occasionsTwo or more blood cultures on separate occasions
“Two or more blood cultures drawn on separate occasions”means
1.Blood from at least 2 blood draws were collected within two days of each other and
2.At least one bottle from each draw is reported as having grown the same common commensal
““ SamenessSameness ”” of organismof organism
If the common skin contaminant is
identified to the species level from one culture, and a companion culture
is identified with only a descriptive name (i.e., to the genus level), this it
is assumed that the organisms are the
same
Example: If a culture grows Staphlycoccus epidermidis
and a companion culture grows Coagulase-negative staphyloccocci, then you can report that the common
skin contaminants are the same and that they are S. epidermidis

““ SamenessSameness ”” of organismof organism
If common skin contaminants from the
two cultures are speciated (e.g., both are Bacillus spp.) but no antibiograms
are done or they are done for only one of the isolates, assume that the
organisms are the same
Blood Culture Specimen CollectionBlood Culture Specimen Collection
Ideally, blood specimens for culture should be
obtained from two to four blood draws from separate venipuncture sites, not through the
vascular catheter.
These blood draws should be performed
simultaneously or over a very short period of time (i.e., within a few hours).
If your facility does not currently obtain
specimens using this technique, you may still report BSIs using these criteria, but you should
work with appropriate personnel to facilitate better specimen collection practices for blood
cultures
� Common commensals� Diphtheroids
(Corynebacterium spp.)� Bacillus spp. (not
B.anthracis)� Proprionibacterium spp.� Coagulase-negative
staphylococci (including S. epidermidis)
� Viridans group streptococci
� Aerococcus spp.� Micrococcus spp.
LaboratoryLaboratory --confirmed bloodstream infection confirmed bloodstream infection (LCBI)(LCBI)
LCBI Criterion 3
commensal

CDC/NHSN Surveillance Definition of HealthcareCDC/NHSN Surveillance Definition of Healthcare --Associated Infection and Criteria for Specific Type s of Associated Infection and Criteria for Specific Type s of Infections in the Acute Care SettingInfections in the Acute Care Setting
This chapter contains the CDC/NHSN surveillance definition of healthcare-associated infection (HAI) and criteria for all specific types of HAI. These criteria include those for the “Big Four” infection types (surgical site infection [SSI], pneumonia [PNEU], bloodstream infection [BSI] and urinary tract infection [UTI]), outlined in earlier chapters of this manual, as well as criteria for other types of HAI. Of particular importance, this chapter provides further required criteria for the specific event types that constitute organ/space SSIs (e.g., mediastinitis [MED] that may follow a coronary artery bypass graft, intra-abdominal abscess[IAB] after colon surgery). Additionally, it is necessary to refer to the criteria in this chapter when determining whether a positive bl ood culture represents a primary BSI or is secondary to a different type o f HAI. A BSI that is identified as secondary to another site of infectio n must meet one of the criteria of HAI detailed in this chapter. Secondary BSIs are not reported as separate events in NHSN, nor can nor should they be associated with a central line.
Secondary BSISecondary BSI• A culture-confirmed BSI associated with a documented
HAI at another site• If a primary infection is cultured, the Secondary BSI must
yield culture of same organism as the primary HAI site
Example: Mrs. Jones has a fever and grows E. coli in her urine (>100,000 col/cc) and in her blood. She has both a femoral central line and an indwelling urinary catheter. A CAUTI (SUTI) is reported with a secondary BSI.
Example: Mr. Smith grows A. baumanii in his surgical wound which is resistant to amikacin and levofloxin but sensitive to other tested antimicrobials. He is also growing A. baumanii in his blood, but it is susceptible to amikacin. The SSI is reported with a secondary BSI.
When determining if a bloodstream infection is
the primary infection site or secondary to an
infection at another site, there will be no
requirement for the antibiograms of the blood
culture isolate(s) and antibiograms of the
isolate(s) from the primary infection site culture
to match. The isolate(s) must only match at the
genus/species level for the bloodstream
infection to be considered secondary to the
primary infection site.

Secondary BSI (cont.)Secondary BSI (cont.)
• If an infection is identified and no culture is used to meet the infection criteria and a blood culture is positive, then the first infection is considered primary and the bloodstream infection is reported as secondary. The organism cultured from the blood is reported as the organism for the primary site.
Example: 6 days postoperatively, Miss Green has an abdominal abscess, confirmed by CT scan. On the same day, her blood is drawn and grows Bacteroides fragilis. The infection is reported as an SSI-GIT (organ space SSI) with a secondary BSI. The organism is reported as B. fragilis
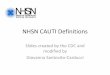
Positive blood culture
Does patient meet the criteria for HAI at another site? (If infection is CA, or if NHSN criteria for the specific site HAI has not been met, answer “No”.)
No Yes
CA or HA
Is blood isolate a common pathogen for this site?
HA CA
This CA infection with secondary BSI is not reported through NHSN nor is the BSI.
Primary BSI
NoYes
Site infection with secondary BSI
Primary BSI
QUESTIONS?QUESTIONS?

CAUTICAUTI
Provisional CAUTI ResultsProvisional CAUTI Results
Provisional CAUTI ResultsProvisional CAUTI Results
Total number of records reviewed

Provisional CAUTI ResultsProvisional CAUTI Results
Auditors reviewed a total of 38 patients that were reported to
NHSN by the hospitals as CAUTI
Provisional CAUTI ResultsProvisional CAUTI Results
CAUTIs that were reported by hospitals
and confirmed by auditors
Provisional CAUTI ResultsProvisional CAUTI Results
CAUTIs that were reported by hospitals and not confirmed by auditors. These are
over-reported cases

Provisional CAUTI ResultsProvisional CAUTI Results
Total number of unreported positive urine cultures reviewed
by audit
Provisional CAUTI ResultsProvisional CAUTI Results
Urine cultures that were identified as
CAUTI by auditors. This is an under-reported case.
Provisional CAUTI ResultsProvisional CAUTI Results
Positive urine cultures that were not identified as
CAUTI by audit and were not reported
by the hospital

CAUTI Misreported CasesCAUTI Misreported Cases
• One case was under-reported. The hospital indicated that the UTI was pre-existing, but the evidence does not support this
• 12 cases were over-reported– 4 patients were reported as CAUTI when no indwelling catheter
was in place
– 4 patients were reported as CAUTI, but patients were asymptomatic
– 1 patient was asymptomatic and there was no culture on the date CAUTI reported
– 2 patients had no urine culture on the target date
– UTI on this date is not a new UTI, but an extension of a previous CAUTI


Patient with or without an indwelling urinary catheter
Patient of any age�None of the following:
•Fever (>38°C)•Urgency•Frequency•Dysuria•Suprapubic pain•Costovertebral angle pain or tenderness
Patient ≤ 1 year of age�None of the following:
•Fever (>38°C Core)•Hypothermia (<36°C)•apnea•bradycardia•lethargy•Vomiting
A positive urine culture of ≥105 CFU/ml with no more than 2 species of microorganism
A positive blood culture with at least 1 matching uropathogen microorganism to the urine culture
Asymptomatic Bacteremic Urinary Tract Infection (ABUTI)

CAUTICAUTI CriteriaCriteria
Provisional SSI ResultsProvisional SSI Results
* Differences in Specific Event not considered

Provisional SSI ResultsProvisional SSI Results
*
* Differences in Specific Event not considered
A total of 240 records were
reviewed
Provisional SSI ResultsProvisional SSI Results
* Differences in Specific Event not considered
70 patients were reported as having SSI
by the hospital
Provisional SSI ResultsProvisional SSI Results
*
60 of the SSI cases reported
by hospitals were also
identified as SSIby the audit
* Differences in Specific Event SSI not considered

Provisional SSI ResultsProvisional SSI Results
10 of the SSI cases reported by hospitals did
not meet SSI criteria during
the audit
* Differences in Specific Event SSI not considered
Provisional SSI ResultsProvisional SSI Results
* Differences in Specific Event are identified as “No SSI”
When the Specific SSI Event was evaluated, only 42/70 matched
Provisional SSI ResultsProvisional SSI Results
*
* Differences in Specific Event are identified as “No SSI”
28/70 records reviewed were
either over-reported or reported an
incorrect Specific SSI Event

Provisional SSI ResultsProvisional SSI Results
* Differences in Specific Event are identified as “No SSI”
170 operative procedures were
reviewed in cases where an
SSI was not reported
Provisional SSI ResultsProvisional SSI Results
* Differences in Specific Event are identified as “No SSI”
4/170 were identified as SSI
by the auditor (under-reported)
Provisional SSI ResultsProvisional SSI Results
* Differences in Specific Event are identified as “No SSI”
166/170 were not identified as SSI and were correctly not reported to
NHSN

SSI Misreported CasesSSI Misreported Cases
• Under-reported (4)– 1 not reported because case was infected at the time of surgery
– 3 cases were missed (undetermined)
• Over-reported (10)– 1 reported case should have been associated with a different
surgery date
– 8 cases were reported to NHSN where event criteria for SSI were not met
– 1 case reported as DIP was actually SIP, but it was >30 days so should not have been counted
Discrepancies to SSI Specific EventsDiscrepancies to SSI Specific Events
Hospital Determination Auditor Determination Number of Cases
SIP DIP 4
SIP Organ/Space 1
SIP DIS 1
SIS DIS 1
DIP Organ/Space 5
DIP DIS 1
Organ/Space SIP 1
Organ/Space DIP 1
Organ/Space Organ/Space (different O/S)
2
SSI DefinitionsSSI Definitions
Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. Infect Control Hosp Epidemiol 1992;13(10):606-8.

Superficial Incisional SSISuperficial Incisional SSI
Deep Incisional SSIDeep Incisional SSI
DIP and DISDIP and DIS
Deep incisional primary (DIP)
A deep incisional SSI that is identified in the primary incision in a patient that
has had an operation with one or more incisions
(e.g., C-section incision or chest incision for coronary artery bypass graft with a
donor site [CBGB])
Deep incisional primary (DIP)
A deep incisional SSI that is identified in the primary incision in a patient that
has had an operation with one or more incisions
(e.g., C-section incision or chest incision for coronary artery bypass graft with a
donor site [CBGB])
Deep incisional secondary (DIS)
A deep incisional SSI that is identified in the
secondary incision in a patient that has had an
operation with more than one incision (e.g., donor
site [leg] incision for coronary artery bypass graft with a donor site
[CBGB])
Deep incisional secondary (DIS)
A deep incisional SSI that is identified in the
secondary incision in a patient that has had an
operation with more than one incision (e.g., donor
site [leg] incision for coronary artery bypass graft with a donor site
[CBGB])

Organ/Space SSIOrgan/Space SSI
Specific event types that must
be used to differentiate
organ/space SSI
BONE Osteomyelitis JNT Joint or bursa
BRST Breast abscess/mastitis LUNG Other infections of respiratory tract
CARD Myocarditis/pericarditis
MED Mediastinitis
DISC Disc space ORAL Oral cavity
EAR Ear, mastoid OREP Other respiratory
EMET Endometritis OUTI Other urinary
ENDO Endocarditis SA Spinal abscess
EYE Eye, other than conjunctivitis
SINU Sinusitis
GIT GI tract UR Upper respiratory
IAB Intraabdominal, NOS VASC Arterial or venous
IC Intracranial VCUF Vaginal cuff
Organ/Space SSIOrgan/Space SSI

Denominator for Procedure Denominator for Procedure –– Wound ClassWound Class
C = CleanCC = Clean ContaminatedCO = ContaminatedD = DirtyU = Unknown
Wound class is an assessment of the likelihood and degree of contamination of a surgical wound at the time of the operation
Wound ClassWound Class
Clean
� Uninfected wound with no inflammation� Respiratory, alimentary, genital or uninfected urinary tract are notentered� Primarily closed� Closed drainage, if needed
Clean-Contaminated
� Respiratory, alimentary, genital, or urinary tracts entered under controlled conditions and without unusual contamination�Include operations on biliary tract, appendix, vagina, oropharynx if no evidence of infection or major break in technique
Wound ClassWound Class
Contaminated
� Open, fresh, accidental wounds�Major breaks in sterile technique or gross spillage from the GI tract�Includes incisions into acute, nonpurulent inflamed tissues
Dirty� Old traumatic wounds with retained devitalized tissue�Wounds involving existing clinical infection or perforated viscera

Procedure Details Procedure Details ––DurationDuration
Duration:Record the hours and minutes between the skin incision and skin closure.Do not record anesthesia time!
Duration:Record the hours and minutes between the skin incision and skin closure.Do not record anesthesia time!
Additional Rules about DurationAdditional Rules about Duration
• If more than one NHSN operative procedure is done through the same incision during the same trip to the OR, create a record for each procedure and use the total time for the duration of both
Example: Mr. Jones goes to the OR and has a coronary artery bypass graft with a [leg] donor site (CBGB) and also a mitral valve replacement (CARD). The time from the first incision until skin closure is 5 hours. A Denominator for Procedure record is completed for the CBGB and another for the CARD. The duration for each is recorded as 5 hours and 0 minutes.
Example: Mr. Jones goes to the OR and has a coronary artery bypass graft with a [leg] donor site (CBGB) and also a mitral valve replacement (CARD). The time from the first incision until skin closure is 5 hours. A Denominator for Procedure record is completed for the CBGB and another for the CARD. The duration for each is recorded as 5 hours and 0 minutes.
March 11-12, 2009
• If the patient goes to the OR more than once during the same admission and another procedure is performed through the same incision within 24 hours of the original incision, report the combined duration of operation for both procedures
Example: Fred Smith had a small bowel resection (SB) done on Tuesday morning which had a duration of 3 hours and 10 minutes. On Tuesday evening, he was returned to the OR where an exploratory laparotomy was done through the same incision to repair a leaking anastamosis. The cut time for this surgery was 1 hour and 10 minutes.
Report only one procedure – SB combining the two durations. The duration reported is 4 hours and 20 minutes
Example: Fred Smith had a small bowel resection (SB) done on Tuesday morning which had a duration of 3 hours and 10 minutes. On Tuesday evening, he was returned to the OR where an exploratory laparotomy was done through the same incision to repair a leaking anastamosis. The cut time for this surgery was 1 hour and 10 minutes.
Report only one procedure – SB combining the two durations. The duration reported is 4 hours and 20 minutes
Additional Rules about DurationAdditional Rules about Duration
March 11-12, 2009

Denominator for Procedure Denominator for Procedure –– ASA ClassASA Class
ASA Class :An assessment score by the anesthesiologist of the patient’s preoperative physical condition using the American Society of Anesthesiologists Classification of Physical Status schema
ASA Class :An assessment score by the anesthesiologist of the patient’s preoperative physical condition using the American Society of Anesthesiologists Classification of Physical Status schema
ASA ClassASA Class
1. Normally healthy patient2. Patient with mild systemic disease3. Patient with severe systemic disease
that is not incapacitating4. Patient with an incapacitating systemic
disease that is a constant threat to life5. Moribund patient who is not expected
to survive for 24 hours with or without operation
1. Normally healthy patient2. Patient with mild systemic disease3. Patient with severe systemic disease
that is not incapacitating4. Patient with an incapacitating systemic
disease that is a constant threat to life5. Moribund patient who is not expected
to survive for 24 hours with or without operation
March 11-12, 2009
NHSN Basic Risk IndexNHSN Basic Risk Index
The patient’s SSI risk category is simply the number of these factors present at the time of the operation

SSI RateSSI Rate* Stratify by:
•Type of NHSN operative procedure•Basic NHSN Risk Index
SSI Rates have been moved to the “advanced” section of the output options. Note that while these options are available, youwill only be able to obtain your facility’s SSI rates
Comparison to the previously-published NHSN pooled means will no longer be available
2008 NHSH Report 2008 NHSH Report –– SSI RatesSSI Rates
Standardized Infection Ratio (SIR)Standardized Infection Ratio (SIR)• The new SSI SIRs use risk adjustment
calculated through logistic regression modeling• Allows for all available risk factors to be
considered• Each risk factor’s “weight” will vary according to
its significant contribution to the risk for that SSI• For all NHSN procedures, the models predicted
SSI risk better than the basic risk index

Predictive Risk FactorsPredictive Risk FactorsNHSN Operative Procedure
Risk Factor(s) – All SSIs
AAA Duration
CBGB/C Age, ASA, duration, gender, number of beds*
COLO Age, anesthesia, ASA, duration, endoscope, medical school affiliation*, number of beds*, wound class
FUSN Approach, ASA, diabetes, duration, medical school affiliation*, spinal level, trauma, wound class
HPRO Age, anesthesia, ASA, duration, HPRO type, number of beds* trauma
HYST Age, anesthesia, ASA, duration, endoscope, number of beds*
KPRO Age, anesthesia, ASA, duration, gender, KPRO type, number of beds*, trauma
LAM Anesthesia, ASA, duration, endoscope
PVBY Age, ASA, duration, gender, medical school affiliation*
RFUSN Approach, diabetes, duration
VSHN Age, medical school affiliation*,number of beds*, wound class

Overall SSI SIROverall SSI SIR
• During 2009, there were 524 procedures performed an d 13 SSIs identified.
• Based on the NHSN 2006-2008 baseline data, 6.687 SS Is were expected.
• •This results in an SIR of 1.94 (13/6.687), signify ing that during this time period our facility identified 94% more SSIs than expected.
• The p-value and 95% Confidence Interval indicate th at the number of observed SSIs is significantly higher tha n the number of expected SSIs.