Embed Size (px)
Citation preview

1
Pennine Acute Hospitals NHS
Trust:
Improvement Journey

2
Nursing establishments increased by circa
20 wte (£682k) – full by end Sep 17 – FGH
FGH Consultant Medical staff full, 4
remaining middle grades recruited -await
start date
UCC – RN vacancy reduced 30% to 8%
AMU skill mix review – vacancies decreased
from circa 45% to less than 5% (RN)
AMU redesign plus further 10 beds Q3
17/18
Zero 12 hour ED waits since 02.17
Sepsis training above 95%
Medicine Workforce - £1.3 m 17/18 –
additional 14 RNs & 30 HCAs
FGH/RI – ED/Medicine
Site based
leadership

TROH Urgent Care
• Only ED with Green NAAS
• Investment in 25wte nurses and
additional Band 6 posts in ED/AMU
to strengthen leadership
• Expansion of Ambulatory
Care
• Additional CT scanner
• Frailty model expanded to ED/AEC
Primary care Streaming gaining
traction
Speciality response to
ED improving
Increasing use of AEC

4
Improvements on 4 hr performance
trajectory - ahead of STP agreed
trajectory by 1.22%
Significant reduction/elimination of 12
trolley waits
Escalation policy established and in place.
Moving towards recognised OPEL
ACU: National award for ambulatory care
service from NHS England
Ambulance arrivals to assess 14%
improvement, 24% improvement in time to
treatment
Quality Improvement strategy: PDSA
ongoing: See and treat in ED/ 2 hourly
Quality rounds
Unstable and unsafe
system stabilised and
improving NMGH - ED

5
AMU redesign
• Additional 8 beds opened July
2017
• Full expansion to 50 beds October
2017
• Pathway redesign based on SAM
guidance with focus on frailty and
full MDT working
• Improvements in LOS
• 94% compliance with mandatory
training
Fragile Service - AMU

6
£1.2m investment in midwives to achieve Birth rate +
9 consultants recruited with clinical directors in post
at both NMGH and ROH
Bi- weekly practice review meetings in place
Increased incident reporting
Improved Governance processes
- improved culture of incident reporting
- managing incidents in real time
- weekly complaints an incidents meeting to identify learning
93% Mandatory training compliance
84% Essential training compliance
Maternity services

Maternity services
• CTG central monitoring now live and working well with a clear reduction in CTG related incidence upon audit
• CTG training at 94%
• 50% reduction general anaesthetic at non-elective caesarian section
• Significant reduction in blood loss during post-partum haemorrhage
• Reduction seen in trauma post C Section and general anaesthetic emergency section down from 30% to 15%
• Early warning score assessment for mothers significantly improved and a reduction in critical care admissions
• Trust part of wave 1 for the NHSI maternity and neonatal safety collaborative
7

Paediatrics
• Strengthened clinical leadership
teams – consultants, ward
leaders, matrons
• 26 new nurse starters
• Attention to risk and governance
systems with weekly review
meetings, joint boards rounds,
annual education programmes,
risk register reviews.
• Reliably staffing HDU beds and
sustained reduction in transfers
out of area
• Training to support identification
and support of the unwell child
• Paed O&A expansion to create
additional capacity and reduce
LOS
8

9
C&YP Experience
0%20%40%60%80%
100%
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
Dec
-15
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
No
v-1
6
Dec
-16
Jan
-17
Feb
-17
Mar
-17
Ap
r-1
7
May
-17
Jun
-17
Jul-
17 -
Friends & Family Test
Friends & Family Test Negative
Feedback Cloud Where word occurrs at least 10 times

Critical Care
• ROH HDU rota – increased from 5
hours a day of a consultant Intensivist
and a speciality doctor, progressing to
10 hours a day 7 days a week.
• Speciality Doctors - 3 wte overseas
recruits with a further 2 to join the
service by the end of the year.
• Advanced Critical Care Practitioner
(ACCP) training commenced in
February 2017 – two underway and two
further trainees from February 2018.
• An ICM trainee has started with the
Trust based at ROH
• Supernumerary shift leader recruitment
is on-going, with steady improvement
• Recorded handover from ROH HDU
to parent teams with a structured
ward round document with safety
checklist
• Daily joint multidisciplinary handover
of the unit at the ROH in the morning
• Ventilator Acquired and Associated
Pneumonia (VAP) screening done
daily process for recording rates
under development
• Procedural checklists introduced –
CVC, tracheostomy, bronchoscopy,
intubation
• Monthly joint M&M/MDT between
ROH/FGH meetings and bi weekly
M&M/MDT at the ROH
10

11
Quality Improvement Strategy
Quality improvement strategy
launched mid 2017
Staffing investment has allowed
greater involvement and
engagement in projects
Expansion of QI team enables
facilitation of collaborative events
and greater focus on
improvement

12
AIM: To reduce the cardiac arrest rate (per 1000 admissions) by 50% on
collaborative wards by 31st November 2017
Deteriorating Patient Collaborative
For collaborative wards, the chart
is within statistical control. If you
compare baseline with
intervention period then there has
been a 14% decrease.
For collaborative wards,
the chart is within
statistical control. If you
compare baseline with
intervention period then
there has been a 9%
decrease.
Highlighting sick patients at
the start of each shift
Trust-wide roll out of NEWS observation
chart
Roll-out of Patientrack e-
obs system commenced
Cardiac arrest role allocation
Using manual observations
for more accurate
identification of
deterioration
Code red- escalating
clinical intuition and
empowering staff
Weekend plan/escalation
stamp

13
AIM: To ensure 90% of all Red Flag Sepsis patients to receive antibiotics within 1
hour of arrival (in A&E) or within 1 hour of sepsis screening (inpatients) by 31st
March 2018
Sepsis
CQC MD 12: Ensure that staff are always escalating patients who
trigger the sepsis pathway for immediate medical review
In-Patient Sepsis Screening and Action Tool launched 10th
April with NEWS Observation Chart across all sites
‘Screen for Sepsis’ visual prompt included in NEWS
Observation Chart to ensure staff complete the Sepsis
Screening Tool if any Sepsis triggers are identified
If staff identify ‘Red Flag Sepsis’ using the Sepsis Screening
and Action Tool, then the ‘Sepsis Six’ pathway is available to
follow immediately
CQC MD 41: Ensure that staff complete training in ‘Sepsis six’ so
staff are aware of the process to follow when a patient is put on a
‘Sepsis six’ treatment pathway
Adult Sepsis E-Learning Module now included within Essential
Job Related Training for all nursing, midwifery and medical
staff working with adults
Clinical microsystems established for each Care
Organisation to focus improvement work locally
within all A&E departments with the aim of improvement the
early identification and timely management of sepsis.
13

14
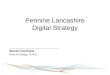
NAAS
30%
49%
21%
Across all 4 sites 50 areas in total to be
assessed 47 undertaken 3 outstanding
Red wards Amber wards
Green wards
45%
33%
22%
NMGH 18 areas in total to be
assessed 18 undertaken 0 outstanding
Red wards Amber wards Green wards
22%
64%
14%
TROH 16 areas in total to be
assessed 14 undertaken 2 outstanding
Red ward Amber ward Green ward
13%
54%
33%
FGH / RI 16 areas in total to be
assessed 15 undertaken 1 outstanding
Red ward Amber ward
Green ward
Investment in 3 corporate quality
Matrons ( introduced June 2017
Still significant work to be done
but steady improvements in
outcomes
Far greater visibility of ward
quality and performance
November 2017 roll out of
paediatric NAAS
70% of all wards
assessed at Green or
Amber. 21% at Green

15
Actions and initiatives implemented to support
improvement to Trustwide Falls are as follows;
The roll out Pennine wide of the RCP bundle
Introduction of Falls Steering Group
Intensive training for areas with high falls levels
Introduction of falls panel which looks at learning from
falls across Pennine
Introduction of a distinct falls team
Collaboration with Alliance colleagues at Salford
Harm Free Care - Falls

16
Pennine Acute per 1000 bed days
There are 8 points below the mean from Sept 2017 which indicates special
cause. There are an average of 5.34 falls per 1000 bed days per month
across Pennine Acute.
Statistically
significant
improvement
correlates with the
introduction of the
RCP bundle

17
Pennine Acute Count of Falls
There is an astronomical data point in January 2016 with the rest of the data
points in statistical control. There are an average of 187.97 falls per month
at Pennine Acute.

18
The Infection Prevention Improvement plan 2017/18.
90 Quality Improvement programme completed for an innovative
patient hand hygiene project and adoption now in progress across
Pennine Care Organisations
NE sector collaborative E.Coli improvement programme initiated
with CCGs
“SIGHT “ CDI educational video completed
Implementation of both Care Organisation and Group Infection
Prevention Committee chaired by each Care Organisation DIPC.
Re-launch of IP Link Nurses programme with 2 successful study
days completed
Hand hygiene mandatory annual assessment compliance above
90% for all Care Organisations .
Harm Free Care – Infection Prevention

19
CDI: The Trust position compared to monthly reported cases in
2016/17, has improved and is in a position to meet the annual
objectives.

CDI Rate per 100,000 bed days has reduced from 14.31 in 2016/17 to
13.89 in first quarter of 2017/18.

The graphs below highlight post 48hr MSSA rate per 100,000 bed days
benchmarked with North of England Trusts. Pennine Acute continues to
report low a rate of 2.9. The majority of cases relate to soft tissue
infection and cellulitis.

0.00
10.00
20.00
30.00
40.00
50.00
60.00
70.00
E.Coli bacteraemias (Trust apportioned) rate per 100,000 Bed days Benchmark data for North England Trusts: Apr to Jun 2017
REN
RFF
RBS
RP5
RTX
RNL
RWY
RXL
RFR
RAE
RM2
RRF
RXP
RR7
RVY
RE9
RCF

23
A review of the Thromboprophylaxis policy is underway and following a pilot
on F11 at ROH VTE assessments. The prescription of thromboprophylaxis
will be linked via the EPMA from October 2017 to improve the compliance of
assessment and prescription for all new admissions.
Following the pilot 91% of newly admitted adults had VTE risk assessments
completed.
A check list has been introduced to all the wards at TROH for the ward
rounds, as a reminder to assess a patient’s VTE need. It will be monitored
by undertaking an audit of this from November 17 onwards This will help in
reducing the incidents of hospital associated VTE.
NMGH are looking at processes to increase compliance with risk
assessment as part of their MAU redesign work. The learning from this work
will be spread to other care organisation as part of their MAU redesign work
A group HA-VTE project is to be established as part of the Pennine QI
strategy.
Harm Free Care – VTE

24
VTE Assessment Compliance within 24
hours NMGH

25
Pressure Ulcers Collaborative
The aims of this
collaborative are: • A 30% reduction of Stage 2
Pressure Ulcers in pilot areas
by 1st April 2018
• Zero tolerance of Stage 3&4
(including unstageable pressure
ulcers) Pressure Ulcers in pilot
areas by 1st April 2018
• A 20% reduction in pressure
ulcers in the community pilot
areas by 1st April 2018.
Driver Diagram

26
Pressure Ulcers - Pilot Areas

27
Pressure Ulcers - Tests of change
Designed a flow chart explaining
what to do/next steps for pressure
ulcer care as a hand held pocket
device
Protected time for skin checks
and equipment checks
Standardised handover with
designated section for skin care,
skin check frequency, equipment
and mobility.
Body maps as part of intentional
rounding tool
Qualified staff aim to complete
skin inspections on AMU within
4 hours of arrival.
Welcome pack at every
bedside to educate patients on
pressure ulcer prevention.
End of bed handover on the
late/night shifts.
Bedside checklists as a visual
prompt on the bay for pressure
relieving equipment.
Review of fractured neck of
femur pathway from A&E and
focus on pressure ulcer
prevention earlier on.
To complete hourly
assessment of all medical
devices which risk damage to
skin
Education leaflets around skin
integrity handed out at pre-op
Educate and update staff on
correct use of slide sheet
CCU SKIN Bundle
Body maps as part of
intentional rounding tool
FGH/RI Pilot TROH Pilot NMGH Pilot
Supported with
• Site based learning sets throughout August & September
• Pressure Ulcer Pledge – to highlight importance
• NHS Model for Improvement
• Quality Improvement Team

End Of Life & Bereavement
• EOL Resource boxes on all wards and departments
• Dedicated Bereavement Offices with Bereavement Clerks, separate to General Office
• SWAN bereavement suites on all sites & in A&E
• celebration packs, comfort packs and z-beds for relatives staying overnight with loved ones.
• Tissue Donation process improved
• 3 Dedicated Bereavement Nurses, EOL Support Volunteers and investment in training and education days

29
February 2016
Monthly Mortality Case reviews were – under resourced, with delays
in analysis and reports
Speciality M&M reviews – Meetings not multi-disciplinary for
richness of feedback
Speciality M&M reviews - No formal agreed structure for
implementing and monitoring improvement actions from learning
Mortality Performance Report HSMR/SHMI and Dr Foster analysis -
Mortality performance and Mortality review findings reported via
different routes
Coding and Mortality validation - Variable practice of mortality
validation tool
The Hospital Standardised Mortality Ratio (HSMR) performance for
the Trust for the period June 2015 to May 2016 at 102.47
Morbidity & Mortality

30
Reliable system for multidisciplinary M&M reviews,
engaging Ward staff, Bereavement Nurses and EOL and
palliative care teams.
Adapting the SRFT Mortality Review Policy to provide a
standardised review process and governance structure for
escalation and reporting by the Care Organisations
Moving to a 3 step process to align with SRFT policy with
the creation of a new electronic Death Summary and
Coding form
Structured Judgement Review adopted as corporate review
methodology with overlap period during training.
Focus on learning with robust collation, communication and
education process being developed to provide assurance
around learning from avoidable factors. (incl. M&M, Clinical
Audit reports, Dr Foster, Grand Rounds, Coroners, themed
harms data, SI’s, Claims, Complaints etc.)
On-going data analysis and review of Dr Foster intelligence
to determine improvement actions within areas Trustwide
and at Care Organisation level.
Bereavement teams involved in liaising with relatives of
patients to support their involvement with mortality case
reviews, and investigations, and to keep informed of
progress and outcomes.
Morbidity & Mortality

31
The Trusts HSMR has
continued to reduce,
against a rolling 12
month trend, to the
period June 16 to May
17. HSMR is now
statistically less than
expected at 95.3.
The improved position,
against the risk
adjusted mortality
indictors is multi
faceted; reduction in in-
hospital deaths and
crude rate; increase in
the expected number
of deaths due to
improvements in
documentation, coding
and the introduction of
new coding guidance
for Septicaemia.
Morbidity & Mortality
Dr Foster Mortality Dashboard Period Jun-16 - May-17

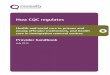
32
Morbidity & Mortality
The Trusts HSMR has
continued to reduce,
against a rolling 12
month trend, to the
period June 16 to May
17. HSMR is now
statistically less than
expected at 95.3.
The improved position,
against the risk
adjusted mortality
indictors is multi
faceted; reduction in in-
hospital deaths and
crude rate; increase in
the expected number
of deaths due to
improvements in
documentation, coding
and the introduction of
new coding guidance
for Septicaemia.

Complaints
33
Complaints reduction and earlier response
rate less dissatisfied complainants with
introduction of new head of complaints and
investment in 4 Complaints handlers posts
and administration support
Eradication of +100 days open
complaints

Incidents, Claims and Coroners
• Care Organisation incident
reporting increased by 10%
• Serious Untoward Incident
investigation backlog reduced
from 102 to 4
• Reduction in SUI related
deaths
• Duty of Candour for Serious
Untoward Incidents –
increased from 20% to 100%
(Director or Deputy led
process)
• Coronial information request
data backlog Aug 2016 n=1000
– Aug 2017
• Prevention of Future deaths
notices reduced
• Legal representation at
inquests reduced from 44% to
5%
34

Claims
The Trust has been notified of 163 claims within the last year. There has been an decline in the
number of claims received. (caveat - claimant’s have three years from the date of incident or the
date of knowledge
Improvements to continue the reduction of claims include; changing Trust solicitors to Hill Dickinson;
a claims focus at meetings; training sessions to promote expedited processes.
Two new permanent members of staff within the department and a legal assistant who handles the
release of medical records.
Non clinical claims
Detailed analysis of EL/PL claims presented to H&S Committee to inform plans for targeted training
• Needlestick
• Slips/trips/falls
• Manual handling
0
2
4
6
8
10
12
14
16
18
20
Claims Received
Linear (Claims Received)

Claims
The above graph highlights the specialities of those claims which we have been notified of within the
last year, confirming hot-spots within: A&E, General Medicine, Obstetrics and Orthopaedic Surgery.
Regular meetings with the Governance Managers for Women & Children’s to investigate how we can
attempt to decrease the number of claims; often with the highest damages payments.
Further clinical training sessions are to take place following feedback to Orthopaedic Surgery due to the
high number of claims relating to missed fractures.
Clinical Negligence Claims
Analysis of NHSR scorecard to inform a planned programme of review with MD/CD's for each Care
Organisation and Division
Detailed review of high cost/high volume claims to support targeted training of clinicians
Further consideration to establish a clinically led Litigation Review Group. ( Group wide), to review new
claims received, to assess risk, lessons learned and potential early settlement.
0
5
10
15
20
25
30

Delays and Outliers
Medical outliers reduced from peak of 50 in Feb 2016 to
less than 10
MOATs and DTOCs still largely
unchanged
90 improvement cycles and clinical microsystem
coaching

38
Data Quality - ED
Point prevalence analysis of clock
stops between 3hour 30 and 3
hours 59.
• Auditors independent of the site
analysed, were trained in the
methodology for validation.
• Clinical input was provided by an
ED Consultant and information
support from the Divisional
Information Manager.

39
Data Quality - RTT
Phase 1 – removing data no longer accurate, timely or up-to date
- 174 specialities removed from consultant masterfile
- cleanse of cancellation reason masterfile (21 codes deleted)
- 35 unused specialities deleted
- admissions and referrals - all entries mapped to data dictionary and cleansed , so
meaningful to end users
Phase 2 – Autoclosure
- 170,00+ pathways closed safely, remaining 56,000+ by Oct
- monthly automation of auto closure with SOPs in place to maintain cleansed system
- new Patient Tracking Lists currently being tested for go line Oct
Phase 3 – Training
- 379 staff via face to face training and passed RTT e-learning
Phase 4 – PAS Upgrade and Patient Centre Roll-out - TBC

New Workforce Strategy - Aims
40
Hig
h s
tan
dar
ds
of
care
, del
iver
ed r
elia
bly
an
d
pro
du
ctiv
ely
highly motivated people
highly competent people, working at the "top of their
licence"
A workforce of sufficent numbers

A workforce of sufficient
numbers
41
More work to be done on Medical
recruitment
104 RNs and 37 Midwives started Sept

A workforce of sufficient numbers
Key changes • Significant investment in recruitment activities • Leveraging of SRFT brand • Part way through implementing radical transformation of
recruitment activity from administration to assertive management
• Starting journey to develop and embed new employee value proposition
• Implementing NHSP across all functions (medical implemented in Nov 17)
• Revision to workforce planning – first phase medical rotas • HRD business partner model

Results • Overall most measures have improved significantly over the last twelve months. • The overall engagement score for the Trust has increased to 3.91 from 3.77.
• 63.92% of staff would recommend the Trust for care or treatment compared to 52.88% in
March 2016
• 56.36% would recommend it as a place to work compared to 45.51% in March 2016.
• Measure of Staff confidence in the future of the organisation increased (3.08 from 2.58)
• Staff feeling able to achieve their work objectives increased to 3.63
• Sickness absence reduced by one percentage point in year 2016/17 • Staff turnover rate stabilised
43
Highly motivated people – May 2017
results

Key Changes • CO Director leadership
– Shop floor presence
– 1000 voices
– Comms
• Increased appraisal coverage
• Roll out of Pioneer (Go Engage) programme
• Revision of grievance & disciplinary practice
• Revision of sickness management practice
• Revision of L&D and OD practice and leadership
• Launch of MES programme
• HRD Business Partner Model (inc changes to contracting out model)
44
Highly motivated people

45
Highly Competent People
Key Changes
• Launch of clinical leaders programme
• Prioritisation and review of clinical development programmes
• Working up new LNA aligned with Trust priorities and staff aspirations
• L&D & OD functions with new operating models
• Revision of Contribution Framework

A workforce of sufficient
numbers Key changes
• Significant investment in recruitment activities
• Leveraging of SRFT brand
• Part way through implementing radical transformation of recruitment activity from administration to assertive management
• Starting journey to develop and embed new employee value proposition
• Implementing NHSP across all functions (medical implemented in Nov 17)
• Revision to workforce planning – first phase medical rotas
• HRD business partner model
Results • Overall most measures have improved
significantly over the last twelve months.
• The overall engagement score for the Trust has increased to 3.91 from 3.77.
• 63.92% of staff would recommend the Trust for care or treatment compared to 52.88% in March 2016
• 56.36% would recommend it as a place to work compared to 45.51% in March 2016.
• Measure of Staff confidence in the future of the organisation increased (3.08 from 2.58)
• Staff feeling able to achieve their work objectives increased to 3.63
• Sickness absence reduced by one percentage point in year 2016/17
• Staff turnover rate stabilised

Highly Motivated & Competent
People Key Changes
• CO Director leadership – Shop floor presence
– 1000 voices
– Comms
• Increased appraisal coverage
• Roll out of Pioneer (Go Engage) programme
• Revision of grievance & disciplinary practice
• Revision of sickness management practice
• Revision of L&D and OD practice and leadership
• Launch of MES programme
• HRD Business Partner Model (inc changes to contracting out model)
Key Changes • Launch of clinical leaders
programme
• Prioritisation and review of clinical development programmes
• Working up new LNA aligned with Trust priorities and staff aspirations
• L&D & OD functions with new operating models
• Revision of Contribution Framework
47

Looking Ahead
• Reliable process to maintain fundamental
clinical & operational standards;
• Scale up and spread of QI change
packages and launch of QPID methods
• Establish robust and reliable learning
Framework
• Enhanced observation – appropriate use
of staff and interventions
• Workforce; alternative roles and reducing
reliance on agency staff
• A&E and UCC – maintaining progress
and maximising winter resilience
• Reducing harm caused by pressure
ulcers , falls and C-Diff
• Continue to be key stakeholder in
development of LCOs
• Engagement, Engagement, Engagement
48