Embed Size (px)
Citation preview

J Shoulder Elbow Surg (2009) 18, e11-e13
www.elsevier.com/locate/ymse
Peg-in-socket nonunion of the radial neck: Case reportand review of the literature
Amol Tambe, MBBS, MS, FRCS (Trauma and Orth)*,Michael J. Hayton, BSc(Hons), MBChB, FRCS(Trauma and Orth)
Wrightington Upper Limb Unit, Wrightington Hospital, Wrightington, United Kingdom
Radial neck fractures are uncommon in children, and themanagement of completely displaced fractures of the radialneck can pose considerable difficulty. Both conservativeand surgical techniques have been described in the treat-ment of these injuries in children.4,5,7,8
Complications arising from these fractures in the pedi-atric population include malunion, nonunion, avascularnecrosis, radioulnar synostosis, premature closure of thephyses, stiffness of the elbow, and increased carryingangle.1 Nonunion of a radial neck fracture has beenrecognized as a rare outcome of this fracture type in chil-dren.1,9 We describe a case of a ‘‘peg-in-socket’’ type ofnonunion in a radial neck fracture in a young girl. Thisunusual type of nonunion required surgical fixation toalleviate symptoms of pain and clicking at the elbow.
Case report
A 12-year-old girl sustained a direct injury to her left elbow aftera fall. At presentation, her radiographs revealed a completelydisplaced Salter Harris type I fracture of the radial neck, with theradial head having rotated 90� and lying parallel to the radial neck.She had no associated neurologic injury at presentation. She wastreated at a pediatric orthopedic unit, where the fracture under-went open reduction with a miniopen approach to the radial headand stabilization of the fracture with an intramedullary pin along
*Reprint requests: Amol Tambe, Upper Limb Fellow, Wrightington
Upper Limb Unit, Wrightington Hospital, Hall Lane, Appley Bridge,
Wigan WN6 9EP United Kingdom.
E-mail address: [email protected] (A. Tambe).
1058-2746/2009/$36.00 - see front matter � 2009 Journal of Shoulder and E
doi:10.1016/j.jse.2008.04.001
the radial shaft, engaging the radial head in the subchondral plate.The fracture reduced well and was stable.
The intramedullary pin was removed at 3 months, when thefracture was deemed to be well on its way to union. However, thepatient continued to have ongoing pain and clicking in this area,which prompted another review with radiographs. This revealedan area of lucency in the radial headeneck junction, suggestive ofnonunion. At this initial review, it was decided to treat herexpectantly in the hope that the fracture might unite.
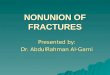
At 1 year from injury, the patient still had symptoms of pain inthe elbow and the forearm associated with a clicking sensation. Aradiograph of her elbow revealed an established nonunion with theappearance of sclerosis, rounding off of the radial neck, andhollowing within the radial head, thus giving a peg-in-socketconfiguration (Figure 1, A and B). A magnetic resonance image(Figure 2) suggested probable early avascular necrosis in theradial head. At this stage, the patient had constant pain in herelbow and forearm, which was now limiting her daily activity. Shehad a normal carrying angle, a 10� limitation in extension, and 40�
lack of full supination. Flexion and pronation were not signifi-cantly affected.
Fluoroscopy of the elbow was done to assess the radial headeneck junction. In flexion-extension, the rounded radial neck wasfound to piston into the hollow radial head so that they movedtogether as one unit. On forearm rotation, however, the radial neck(the peg) was seen to be rotating within the pseudoarthrosis withthe radial head (the socket). The radial head itself did not show anyrotatory movement while the radial neck was rotating within it.
After a detailed discussion with the patient and her parentsabout the fluoroscopic findings, it was decided to fix the nonunionsite with bone grafting. A standard Kocher approach was used toexpose the radial head and neck. The head was bound by adhe-sions, which were cleared to free the radial head within theannular ligament. The radial head articular cartilage appeared
lbow Surgery Board of Trustees.

e12 A. Tambe, M.J. Hayton
Figure 1 Nonunion of the radial neck is shown in (A) anteroposterior and (B) lateral radiographs of the elbow.
normal, and the operative appearance was not classic of avascularnecrosis. The nonunion site was entered and thoroughly debrided.
The cavity was then packed with an autograft from the distalradius. A 20-mm cannulated Herbert screw was inserted to engage
Figure 2 Magnetic resonance imaging of the nonunion site.
the head and shaft. The screw afforded good fixation, and care wastaken to ensure that the screw did not impinge into the articularsurface of the radial head. Lysis of adhesions improved herextension slightly, without any major improvement in supination.She was given a resting splint postoperatively.
There were no postoperative complications. The patient wasallowed flexion-extension movement out of her splint undersupervision, with gentle rotation after 4 weeks. She continued tomake good progress with the therapists, and at her latest review, 1year after surgery, had 10� to 130� of flexion and full pronationwith a 30� limitation of supination. Her latest radiographs showedthe Herbert screw to be in a good position, with evidence ofconsolidation of the graft (Figure 3, A and B). Of particular note,her symptoms of pain in the forearm and elbow, along withclicking, had resolved completely.
Discussion
Fractures of the radial neck account for about 1% of allchildren’s fractures.1 Nonunion is an extremely rareoutcome after radial neck fractures in children, which isevident by the paucity of literature relating to pediatricradial neck nonunions.
In the largest series of pediatric radial neck nonunions,Waters and Stewart 9 describe 9 patients with this compli-cation. These presented to the authors after primarysurgical management elsewhere. Although range of motionwas restricted in all 9 (especially in supination), 3 of thesepatients with nonunions had pain (intermittent or withforearm rotation) at presentation. According to the radio-graphic description of their nonunions, persistent angula-tion and translation were predominant. None of the 9patients appeared to have the peg-in-socket type ofnonunion that was seen in our patient.
The increased risk of nonunion has been attributed to theforce that caused the fracture also disrupting the blood

Peg-in-socket nonunion e13
Figure 3 Healing of the radial neck nonunion is shown in (A) lateral and (B) anteroposterior radiographs of the elbow.
supply to the head and neck fragment in the process.3
Surgery in this compromised situation might add to thevascular insult and increase the potential for nonunion.2,3,5
Periosteal interposition at the fracture site has been citedas causing nonunion,6 although it is unlikely when openreduction has been done. Some have also suggested thatinadequate reduction and failure of fixation may be animportant cause of nonunion.1,9
Treatment options for nonunion broadly fall into 3categories: open reduction and internal fixation with a bonegraft, radial head excision, or observation alone inasymptomatic patients.9 Waters and Stewart advocatedrepeat open reduction with internal fixation to improveradiocapitellar alignment and range of motion, to reducepain, and to lessen the risk of future degenerative changesin the elbow joint.
It is difficult to understand why nonunion developed inour patient, although the severity of the initial trauma mighthave contributed. Certainly, the fracture was treated withoutdelay, and the reduction was stable and satisfactory. Onecan theorize that because the pseudarthrosis was behavingin the fashion of a rotating peg in a socket, it should nothave produced significant symptoms. We believe that theactivity-related pain in the forearm might have been due tothe proximal pistoning of the shaft inside the shell of theradial head.
The resolution of symptoms after fixation, especially ofthe forearm pain, might indicate that fixation prevented thispistoning of the radial shaft within the radial head, therebyproducing a stabilizing effect on the forearm. Supinationimproved only slightly, possibly due to slight incongruency
of the proximal radioulnar joint and formation of scar tissueafter the initial severe injury and subsequent surgery. Thepatient did not have any wrist-related pain, and we do notbelieve that she had an Essex-Lopresti injury.
We have not seen a nonunion of this nature aftera pediatric radial neck fracture and thus report it as a rareand interesting sequela of a radial neck injury.
References
1. Chambers HG. Fractures of the proximal radius. In: Beaty JH,
Kasser JR, editors. Rockwood and Wilkins’ fractures in children.
Philadelphia, PA: Lippincott Williams & Wilkins; 2001. p. 483-505.
2. D’Souza S, Vaishya R, Klenerman L. Management of radial neck
fractures in children: a retrospective analysis of one hundred patients. J
Pediatr Orthop 1993;13:232-8.
3. Evans MC, Graham HK. Radial neck fractures in children: a manage-
ment algorithm. J Pediatr Orthop 1999;8:93-9.
4. Kaufman B, Rinott MG, Tanzman M. Closed reduction of fractures of
the proximal radius in children. J Bone Joint Surg Br 1989;71:66-7.
5. Metaizeau JP, Lascombes P, Lemelle JL, Finlayson D, Prevot J.
Reduction and fixation of displaced radial neck fractures by closed
intramedullary pinning. J Pediatr Orthop 1993;13:355-60.
6. Pring M, Wenger D, Rang M. Elbow-Proximal Radius and Ulna. In:
Rang M, Wenger DR, Pring ME, editors. Rang’s children’s fractures.
Philadelphia, PA: Lippincott Williams & Wilkins; 2006. p. 119-34.
7. Rodriguez-Merchan EC. Percutaneous reduction of displaced radial
neck fractures in children. J Trauma 1994;37:812-4.
8. Vocke AK, Von Laer L. Displaced fractures of the radial neck in
children: long-term results and prognosis of conservative treatment. J
Pediatr Orthop B 1998;7:217-22.
9. Waters PM, Stewart SL. Radial neck fracture nonunion in children. J
Pediatr Orthop 2001;21:570-6.








![scaphoid nonunion panel Esfahan 16 ordibehesht 95.ppt · Microsoft PowerPoint - scaphoid nonunion panel Esfahan 16 ordibehesht 95.ppt [Compatibility Mode] Author: bahare Created Date:](https://img.pdfslide.us/doc/110x75/5f0c38017e708231d43452ac/scaphoid-nonunion-panel-esfahan-16-ordibehesht-95ppt-microsoft-powerpoint-scaphoid.jpg)