Embed Size (px)
Citation preview

Peg-asparginase in the treatment protocol of Acute Lymphoblastic
Leukemia
Muhammad Qayash Khan
PhD in Zoology
Ist Semester 2013

Leukemia
Leukemia is a cancer of the marrow and blood.
---The four major types: Acute Myeloid Leukemia Chronic myeloid leukemia Acute Lymphoblastic
Leukemia Chronic lymphocytic
leukemia.
Acute leukemia
---A rapidly progressing disease that produces cells (blasts) that are not fully developed.

Epidemiology
Most common childhood cancer Demographics:
---Males more commonly than females
---Whites more than blacks
---More commonly in patients with Down Syndrome

Incidence

Etiology and Pathophysiology
ALL stems from mutations
–Radiation
–Chemicals
–Other Malignant immature white blood cells (WBCs).
–Lymphoblast crowd out the bone marrow.
–This includes crowding out of platelets, RBCs, and mature WBCs.

ALL Symptoms
Anemia Bleeding and bruising Bone and joint pain Fever Weight lossPetechia

Fonts - Bad
If you use a small font, your audience won’t be able to read what you have written
CAPITALIZE ONLY WHEN NECESSARY. IT IS DIFFICULT TO READ
Don’t use a complicated font

Blood and Bone Marrow hematology comparison in ALL

Bone Marrow Pathology

Etiology… stem cells

Symptoms

Diagnosis
Bone marrow biopsy
–>25% lymphoblast in the bone marrow Lumbar puncture
–CSF cytology Imaging/scans

Pegasparaginase (Oncaspar) for ALL
PEGylated L-asparaginase for the treatment of ALL in patients who are hypersensitive to the native unmodified form of L-asparaginase (obtained from Escherichia coli and Erwinia chrysanthemi). The drug was recently approved for front line use by FDA in 2007.

Oncaspar
Pegylated L-asparagine amidohydrolase from E. coli.
C1377H2208N382O442S17

Pharmacodynamics
The malignant cells are dependent on an exogenous source of asparagine for survival.
Normal cells, however, are able to synthesize asparagine and thus are affected less by the rapid depletion produced by treatment with the enzyme asparaginase. Oncaspar exploits a metabolic defect in asparagine synthesis of some malignant cells.

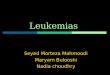
Mechanism of action
Pegaspargase, more effective than native asparaginase, converts asparagine to aspartic acid and ammonia. It facilitates production of oxaloacetate which is needed for general cellular metabolism. Some malignant cells lose the ability to produce asparagine and so the loss of exogenous sources of asparagine leads to cell death.

L-Asparaginase –Mechanism of Action
Catalyzes the conversion of L-asparagine to aspartic acid and ammonia.
Reversal of L-asparagine synthetase activity. Results in rapid and complete depletion of L-asparagine. Lack of intracellular asparagine results in decrease of protein
synthesis and apoptosis.

L-asparaginas in Normal Cells

L-asparaginase in Tumor Cells

L-asparginase action

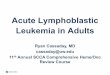
Protein PEGylation

Use of Different nanoparticles for drug delivery to the target

PEGylation, successful approachto drug delivery
PEGylation is the process of covalent attachment of polyethylene glycol (PEG) polymer chains to another molecule, normally a drug or therapeutic protein..

PEGylation
The molecular weight of a molecule increases which impart several significant pharmacological advantages over the unmodified form, such asImproved drug solubilityReduced dosage frequency, without diminished efficacy with potentially reduced toxicity.

PEGylation
Extended circulating life Increased drug stability Enhanced protection from proteolytic degradation
------PEGylated drugs have the following commercial advantages also:
Opportunities for new delivery formats and dosing regimens
Extended patent life of previously approved drugs

Different types of PEGylation

L-Asparaginase –Mechanisms of Resistance
Selective pressure of lymphoid cells that overexpress asparagine synthetase gene.
Increase in L-asparagine synthetase due to a decrease in intracellular levels of L-asparagine.
Formation of asparaginase antibodies that alter L-asparaginase pharmacokinetics.

L-Asparaginase –Pharmacokinetics
Absorption – Not given orally because of intestinal degradation– Intramuscular administration results in 50% lower peak blood
levels than IV route Distribution
– Primarily to intravascular space– Minimal blood-brain penetration
CSF levels are 1% of plasma concentration but depletion of plasma asparagine levels leads to an antileukemic effect in CNS
Metabolism – Not known

Half-lives of different L Asparaginase preparations Intramuscular
Elimination Asselin et al half-life (hours) Dose:25,000 IU i.m
– T ½ is variable with dose, disease status, renal or hepatic function, age, or gender
Depends on preparation PEG-Asparaginase(Oncaspar®) 137.5 ± 77.8 hours E.coli L-Asparaginase (Crasnitin®/Elspar®) 29.8 ± 4.1 hours E. chrysanthemi L-Aspa. (Erwinase®) 15.6 ± 3.1 hours

Half-lives of different L Asparaginase preparations intravenous IV
Werber et al. Elimination half life (hours) Dose:10,000IU PEG-Asparaginase(Oncaspar ®) no data E.coli L-Asparaginase (Crasnitin ®/Elspar ®) 17.7 ± 2.5 hours
E. chrysanthemi L-Aspa. (Erwinase ®) 7.2 ± 4.1 hours

L-Asparaginase –Dosage adjustment
Patients with hepatic impairment– Specific guidelines for dosage adjustments in
hepatic impairment are not available– These patients may be at increased risk for toxicity
Patients with renal impairment– Specific guidelines for dosage adjustments in renal
impairment are not available– No dosage adjustments are needed

L-Asparaginase –Impaired Protein Synthesis
Decreased production of insulin– Resultant hyperglycemia secondary to hypoinsulinemia– Hyperglycemia usually transient and resolves upon
discontinuation Fatal diabetic ketoacidosis has occurred
– Patients with diabetes mellitus at increased risk of adverse reactions due to alteration in insulin production or pancreatic insults
Blood sugar should be closely monitored Decreased production of albumin
– Hypoalbuminemia can be severe resulting in peripheral edema or ascites
Patients with limited hepatic synthetic function may be unable to tolerate the effects of L-asparaginase

L-Asparaginase –Impaired Protein Synthesis
Decreased production of vitamin K-dependent clotting factors and endogenous anticoagulants such as proteins C and S and antithrombin III
– Coagulopathies, thrombosis, or bleeding due to impaired protein synthesis may occur
– Monitor coagulation parameters during L-asparaginase therapy
– Use cautiously in patients with a preexisting coagulopathy (e.g. hemophilia) or hepatic disease
– Intramuscular injections may cause bleeding, bruising, or hematomas due to coagulopathy

L-Asparaginase –Toxicities
Mild nausea/vomiting– Anorexia, abdominal cramps, general malaise, weight loss
Tumor Lysis Syndrome (TLS)– Hyperkalemia, hyperphosphatemia, hyperuricemia, hypocalcemia,
and decreased urine output – severe renal insufficiency– Appropriate TLS measures must be taken following chemotherapy
administration in patients with large chemosensitive tumors Minor bone marrow suppression effects
– Generally transient– Greatest potential is for slight anemia to occur– Marked leukopenia has been reported and white blood cell counts
should be monitored

L-Asparaginase –Other Toxicities
Hepatic adverse reactions– Elevated AST, ALT, serum alkaline phosphatase, gamma
globulin, hyperammonemia, and hyperbilirubinemia or jaundice – Occurs within 2 weeks of starting therapy
Pancreatitis– Caused by necrosis and inflammation of pancreatic cells – Hemorrhagic and/or fatal pancreatitis can occur despite normal
amylase and lipase concentrations because of impaired protein synthesis
Pancreatic toxicity is dose-related Necessitates change of formulation or discontinuation of L-
asparaginase therapy

L-Asparaginase –Contraindications/Precautions
Contraindicated in patients with history of pancreatitis because of risk of acute pancreatitis.
E. coli preparation is contraindicated in patients with history of anaphylactic reactions to products derived from E. coli sources.

L-Asparaginase –Drug Interactions
L-Asparaginase and methotrexate– Therapeutic synergistic and antagonistic effects depend on the
schedule of administration If methotrexate is given 3—24 hours prior to L-asparaginase,
L-asparaginase decreases methotrexate toxicity– Due to blocking the antifolate effects of methotrexate
If methotrexate is given after L-asparaginase, the efficacy of methotrexate is decreased
– Due to: Inhibition of protein synthesis preventing progression to the S-phase of
the cell cycle Blocking of methotrexate polyglutamation
Recommended to give L-asparaginase at least 10—14 days prior to methotrexate or shortly after methotrexate administration
– Cells are refractory to methotrexate for up to 10 days following a single dose of L-asparaginase
– Period of increased DNA synthesis after L-asparaginase protein inhibition that leads to increased sensitivity to methotrexate

L-Asparaginase –Drug Interactions
L-asparaginase and vincristine– If L-asparaginase given concurrently or prior to vincristine, may result in
decreased hepatic metabolism of vincristine and cause additive neurotoxicity Vincristine should be given 12—24 hours prior to L-asparaginase
L-asparaginase and corticosteroids– Result in additive hyperglycemia because L-Asparaginase inhibits insulin
production Insulin therapy may be required in some cases
L-asparaginase and cytarabine– Acute pancreatitis with use of cytarabine in patients that have received prior
treatment with L-asparaginase Anticoagulants, platelet inhibitors, NSAIDs, or thrombolytic agents
– Due to the risk of bleeding and coagulopathy during L-asparaginase therapy patients should not receive other agents that may increase the risk of bleeding

L-Asparaginase –Monitoring Parameters
Blood glucose CBC with differential D-dimer Fibrinogen LFTs Prothrombin time Serum albumin Serum creatinine/BUN Serum uric acid

Conclusion and future perspective
Asparaginase is an important component of chemotherapy in ALL treatment protocol.
With pediatric patients the incidence of severeallergic reactions, thrombosis, pancreatitis and hepatic injury are prominent.
The incidence of these toxicities increases with age. Future perspective…… To reduce the toxicity level and drug efficiency
in Adult ALL.

References
Dinndorf PAF et al. 2007. DA drug approval summary: pegaspargase (oncaspar) for the first-line treatment of children with acute lymphoblastic leukemia (ALL). Oncologist. 2007 Aug;12(8):991-8.
AsselinBL,WhitinJC,CoppolaDJ,RuppIP,SallanSE,CohenHJ.Comparativepharmacokineticstudiesofthreeasparaginasepreparations.JClinOncol.1993;11:1780-1786.2
0.AlbertsenBK,JakobsenP,SchroderH,SchmiegelowK,CarlsenNT.PharmacokineticsofErwiniaasparaginaseafterintravenousandintramuscularadministration.CancerChemotherPharmacol.2001;48:77-82.2
1.WerberG.DrugmonitoringvonAsparaginaseimRahmendespädiatrischenTherapieprotokollsderALL/NHL-BFM90Studie.Inaugural-Dissertation,Münster.1995.2
2.HoDH,BrownNS,YenA,HolmesR,KeatingM,AbuchowskiA,etal.Clinicalpharmacologyofpolyethyleneglycol-L-asparaginase.DrugMetabDispos.1986;14:349-352.2
3.BoosJ,WerberG,AhlkeE,Schulze-WesthoffP,Nowak-GottlU,WurthweinG etal.Monitoringofasparaginaseactivityandasparaginelevelsinchildrenondifferentasparaginasepreparations.EurJCancer.1996;32A:1544-155