Embed Size (px)
Citation preview

A u s t r a l i a n a n d N e w Z e a l a n d C o n t i n e n c e J o u r n a l
76 Vol. 14, No. 3 • Spring 2008
Peer reviewed
A guideline for the nursing assessment and management of urinary retention in elderly hospitalised patients
Abstract
The objective of this project was to develop a guideline for the nursing assessment and management of urinary retention in hospitalised older adults. The guideline was developed from a review of the literature and from consultation with a multidisciplinary expert panel. These experts provided feedback through a structured process known as the Delphi technique. Based on findings from both sources, a final guideline was developed which provides a framework for the nursing assessment and management of urinary retention in hospitalised older adults. This foundational work provides the basis for further research and evaluation of the management of urinary retention.
Introduction
Urinary retention commonly affects older people, and disproportionately more men than women 1-3. Early detection is important as the adverse outcomes associated with delayed response to an overly distended bladder are significant and include urinary tract infection and renal complications 4. on the other hand, catheter insertion that is premature or inappropriate exposes patients to unnecessary catheter associated infection and urethral trauma. one of the dilemmas for clinicians is that urinary retention is not always a straightforward diagnosis as symptoms can be masked, particularly in patients with neurological disorders, or in patients with cognitive impairment, i.e. delirium or dementia.
Joan OstaszkiewiczRN, MNurs Research Fellow, Deakin University-Southern Health Nursing Research Centre, Melbourne VIC
Professor Beverly O’ConnellRN, MSc, PhD, FRCNA Chair in Nursing, Deakin University-Southern Health, Melbourne VIC Australian and New Zealand Continence Journal Editorial Committee member
Dr Chantal skiBA, Hons, PhD Research Fellow, St Vincent’s Health, Melbourne VIC
Correspondence to:Ms Joan Ostaszkiewicz Deakin University-Southern Health Nursing Research Centre, Monash Medical Centre, Clayton VIC Email: [email protected]
Having diagnosed urinary retention, the other critical issue for
clinicians is to differentiate between those patients who require
immediate bladder decompression and those who do not.
Many clinicians are guided in this decision by protocols that
prescribe a threshold post void residual urine volume (PVR) or
a range of PVR values as the basis for determining whether or
not to catheterise a patient. There is some evidence to suggest,
however, that reliance on PVR as the basis for determining the
appropriateness of urinary catheterisation for older adults is
limited 2.
An Australian survey conducted in 2006 on current assessment
and management practice for urinary retention completed by
medical and nursing staff in an aged care rehabilitation facility,
confirmed anomalies in practice 5. Specifically, this study revealed
that clinicians in the aged care setting commonly encountered
patients with undiagnosed urinary retention and that there were
no guidelines to inform their practice.
To fill this gap, our project was to review the literature on the
management of urinary retention and to develop a guideline for
the initial management of this condition in hospitalised older
adults. As nurses are usually the first point of care for patients
with this condition in hospital settings, the guide was developed
for this group. This paper describes the process used to develop
the guideline and details the guideline for further discussion and
research.
Method
To develop the guideline, we searched for and reviewed
the literature on urinary retention to form the basis of a
draft guideline. This was then peer reviewed by an expert
multidisciplinary panel in an iterative consultation process.
© Continence Foundation of Australia

A u s t r a l i a n a n d N e w Z e a l a n d C o n t i n e n c e J o u r n a l
77Vol. 14, No. 3 • Spring 2008
review of the literature
The literature was searched using the database EBSCohost
and included CINAHL, Health Source: / Academic Edition
and MEDLINE. Keywords were identified from a preliminary
review of the literature. Topic relevant keywords included:
‘urinary retention’, ‘acute urinary retention’, ‘chronic urinary
retention’, ‘bladder scan’ and ‘post-void residual urine volume’,
‘older adults’, ‘hospital’, ‘guidelines’, ‘protocols’ and ‘clinical
pathways’. The reference lists of topic relevant publications were
reviewed for additional publications. No arbitrary limitation
was placed on the age of the data and, hence, data were located
between 1981 and 2005. The full documents of all abstracts
considered potentially relevant were retrieved and the main
issues were summarised.
Searches in websites of peak national and international
organisations with expertise in continence or urology were
also used to collect information on definitions, assessment and
management recommendations and guidelines pertaining to
urinary retention.
Consultation with multidisciplinary expert panel
Clinical experts specialising in gerontology, urology and
continence medical and nursing practice were approached by the
project team and invited to participate in the multidisciplinary
expert panel. Using a Delphi technique 6, they were invited to
comment on information obtained from the literature and on
drafts of the developing guideline. The purpose of the Delphi
technique is to elicit information and expert comments from
participants in an iterative way so as to facilitate problem solving,
planning and decision-making until a consensus is reached 7. In
order to reach consensus about the guideline, the experts were
consulted on three separate occasions. Where clinical expert
opinion varied, we consulted the research literature.
In addition to consulting multidisciplinary experts, the
penultimate draft of the guideline was circulated among a
group of nurses working in an aged care rehabilitation facility
and feedback was sought on its clinical usefulness. Comments
obtained from this group were incorporated into the design of
the final draft of the guideline.
Findings
results of review of the literature
The review of literature revealed the following three main
definitions:
• Urinary retention is a failure to empty thebladder totally – a
condition that is clinically diagnosed as either acute or chronic 8.
• “Acuteurinaryretentionisapainful,palpableorpercussible
bladder, when the patient is unable to pass any urine” 9(p.176).
• Chronicurinaryretention is“anon-painfulbladder,which
remains palpable or percussible after the patient has passed
urine” 9(p.176).
The International Consultation on Incontinence further
recommends that transient voiding difficulty in older adults
be differentiated from chronic urinary retention 9. The need
to differentiate patients with urinary retention combined with
high pressures (i.e. hydronephrosis, kidney back pressure and
congestion and an elevated serum creatinine) from patients with
urinary retention combined with low pressures is also advised 10.
The literature search yielded no specific clinical management
guidelines on the topic of urinary retention. There were a
number of guidelines published on disease processes where
urinary retention may present as a symptom (i.e. benign prostatic
hypertrophy, or spinal cord disease) and on the issues of urinary
catheterisation and intermittent catheterisation.
Although there were no specific guidelines on urinary retention,
there was a large volume of related literature; this was grouped
according to the key issue or theme addressed by each
publication. The first theme centred on prevalence, and the
impact and management of acute urinary retention as a symptom
of disorders such as benign prostatic hypertrophy, or following
pelvic surgery. This literature revealed important information
on risk factors for urinary retention in older adults such as
faecal impaction, impaired mobility, neurological disorders (i.e.
stroke, Parkinson’s Disease, Multiple Sclerosis), longstanding
diabetes, medicines (i.e. antihypertensives, anticholinergics,
antispasmodics, atropine, sedatives), urethral obstruction, spinal
cord injury or disease, spinal anaesthesia and surgical disturbance
of bladder innervation. These risk factors were included in the
guideline.
Another major topic area gleaned from the literature focused
on the physiological effects of ageing on bladder function.
Studies showed that, as people age, their bladder contractility
decreases 11, 12; factors that may explain this change include
detrusor fibrosis 13, increased collagen deposition 14 and a loss
of acetylcholinesterase-positive nerve terminals 15. Not only
do many older people have reduced bladder contractility,
but many frail older adults also have a concurrent overactive
bladder, a condition termed detrusor hyperactivity with impaired
contractility (DHIC) 16-18. This condition can cause frail older
adults to have a large PVR and concurrent lower urinary tract
symptoms such as urinary incontinence.
In light of these findings, one of the challenges for clinicians
is that many older adults with impaired bladder contractility
or DHIC may have few or no symptoms. Where symptoms
are limited to urinary incontinence, this can be erroneously
© Continence Foundation of Australia

A u s t r a l i a n a n d N e w Z e a l a n d C o n t i n e n c e J o u r n a l
79Vol. 14, No. 3 • Spring 2008
attributed to other factors. The condition can be further
concealed by the presence of other conditions, for example
dementia. Cognisant of the potential for clinically unsuspected
urinary retention in certain groups, some researchers have
recommended routine screening for PVR for all patients
admitted to general rehabilitation units 19, for incontinent
nursing home residents 20, 21 and for all patients with lower
urinary tract symptoms 22.
The literature on PVR presented variable �ndings that challenge
the reliability of using PVR as a measure for diagnosing clinically
signi�cant urinary retention For example, even in healthy older
adults, the presence of retained urine (i.e. PVR) may represent
normal ageing as Bonde and colleagues 1 identi�ed in a normative
sample of 140 older adults aged over 75 years, who had PVRs
ranging from 0-150mls, and averaged 45mls for women and
90mls for men. Another study of healthy community dwelling
people, over 55 years of age, found that detrusor contractions
declined signi�cantly with age and this decline was associated
with lower urine �ow rates and a small increase (generally
≤50mls) in PVR 23.
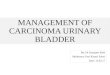
The critical question is: at what volume does a residual volume
become clinically signi�cant? This was not answered as the
literature revealed a wide range of PVR values that require
attention. (Table 1).
After reviewing urinary retention in 100 elderly hospitalised
individuals, Grosshans and colleagues claimed that, “… no
one value is considered signi�cant as a normal or pathological
value” 2(p.637) and have called for further research in order to
better de�ne what may constitute a normal PVR value among
elderly persons, and to determine its signi�cance. To further
illustrate the proposition that proper bladder emptying and
the clinical signi�cance of PVR varies from one person to the
next, Taylor and Kuchel 35(p.1923) state that “repeated PVR values
of 250mls in an older woman who is asymptomatic without
urinary frequency or recurrent urinary tract infections probably
requires no further action, whereas, the same individual
who is symptomatic and has renal failure, or evidence of
hydronephrosis on ultrasound, requires a urology referral”.
A �nal consideration for clinicians is that there is some doubt
in the research literature about the test-retest reliability of
PVR itself, even within a 24-hour period 36-38 . Gri�ths and
colleagues 38 measured residual urine in each of the geriatric
patients in their study at three di�erent times of day, during
two visits at 2-4 week intervals and found large within-patient
variability within that study group.
R esults of consultation with expert panel
The multidisciplinary expert panel was provided with a summary
of the major points found in the literature and panel members
© Continence Foundation of Australia

A u s t r a l i a n a n d N e w Z e a l a n d C o n t i n e n c e J o u r n a l
80 Vol. 14, No. 3 • Spring 2008
were invited to agree, disagree or comment on these points. The
findings from this process revealed that they agreed with most of
the proposed content that formed the basis of the draft guideline.
They identified some limitations with the definitions of acute and
chronic urinary retention found in the review of literature. For
example, the definition of acute urinary retention as “a painful,
palpable or percussible bladder, when the patient is unable to
pass urine” 9 does not accommodate patients with acute urinary
retention who have few or none of these symptoms. Similarly,
the definition of chronic urinary retention as “a non-painful
bladder, which remains palpable or percussible after the patient
has passed urine” 9, does not account for patients with chronic
urinary retention whose bladders are not able to be palpated or
percussed. Hence, reliance on the review of literature definitions
for acute and chronic retention as the basis for diagnosing the
type of urinary retention was seen as problematic.
There was no professional consensus in the literature on what
constitutes a threshold PVR and none of the studies reviewed
provided a formula for practice. Members of the expert panel
also expressed varied opinions about what information should
be included in the guidelines to assist healthcare professionals
to interpret PVR. Despite this variability, the expert panel
emphasised that any interpretation of the clinical significance
of PVR should be done in conjunction with other clinical
information. A key message from the expert panel was that the
knowledge and skills required for identifying and managing
urinary retention were highly specialised and that, “… the
management of urinary retention should be underpinned by
specialised individualised clinical decision-making and is context
specific”.
The panel also identified the different factors that underpin
clinical decision making, including:
• Thepersonandtheircarer’spreferencesfortreatment.
• Theirpsychosocialstatusandqualityoflife.
• Thepotentialforuppertractdamage.
• Anyunderlyingpathology.
• Thetypeandseverityofsymptoms.
• Theresultsofinvestigations.
• Whetherornotthepersonneedsandhasassistancetocarry
out treatment for their condition.
Therefore, all these factors were included in the guideline. In
addition, we included information on the major risk factors and
key signs and symptoms for urinary retention in hospitalised older
adults to alert users of the guide to the fact that multiple factors
need to be considered when interpreting PVR in older adults.
Discussion
Retention of urine is widely experienced by older adults and is
often difficult to detect and diagnose. Its management in this
group of patients poses challenges for clinicians as previously
Table 1. PVR values that require attention.
study PVr values study population
Agency for Health Care Policy and Research (1996) 24 >200mls Elderly patients
Borrie et al. (2001) 25 2 consecutive scans ≥150mls Elderly rehabilitation patients
Dromerick & Edwards (2003) 26 150mls Stroke patients
Fonda et al. (2005) 27 >100mls for men Elderly and frail patients >200mls for women
Gray (2000) 28 150-200mls or more Not stated
Grosshans, Passadori & Peter (1993) 2 >50mls Elderly patients on acute care wards
Hilton & Stanton (1981) 29 20-300mls Elderly patients
Mainprize & Drutz (1989) 30 >30mls Women with chronic persistent urinary tract symptoms
ouslander (1981) 31 20-300mls Elderly patients
Resnick (1984) 32 20-300mls Elderly patients
Starer & Libow (1987) 17 300mls Elderly incontinent nursing home residents
Smith & Albazzaz (1996) 33 >300mls Elderly women post surgery for proximal hip fracture
Tam, Wong & Yip (2005) 34 100mls Elderly patients transferred from acute hospital
Wu & Baguley (2005) 19 150mls Geriatric rehabilitation patients
© Continence Foundation of Australia

A u s t r a l i a n a n d N e w Z e a l a n d C o n t i n e n c e J o u r n a l
81Vol. 14, No. 3 • Spring 2008
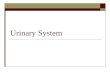
Figure I. Guidelines for nursing assessment and management of urinary retention in elderly hospitalised patients.
Guidelines for nursing assessment and management of urinary retention in elderly hospitalised patients
Urinary retention manifests either acutely or chronically and is
characterised by......
Please note: These guidelines may accompany, but do not replace, local guidelines and/or sound clinical judgement. There may be individuals with more complex conditions (i.e. multiple sclerosis, spinal patients, etc) for whom these guidelines do not apply.
List of abbreviationsPost void residual – PVRIndwelling catheter – IDCIntermittent catheter – IC
Urinary retention symptoms that warrant attention
> Lower abdominal pain and/or discomfort (this may present as distress or agitation in people who are cognitively impaired), and/or
> Urinary incontinence, and/or> Inability or difficulty to void and/or empty the bladder (see facts about
bladder emptying)
Conduct a nursing assessment
> Brief patient history> Review urinary retention risk factors > Conduct a physical assessment of lower abdomen (inspect, palpate, percuss)> Urinalysis (if possible)> Bladder scan to determine the PVR
Modify and monitor risk factors as medically advised (i.e. improve
mobility, bowel management program, relieve pain, administer
prescribed medications etc)
Modify and monitor risk factors as medically advised (i.e. improve
mobility, bowel management program, relieve pain, administer
prescribed medications etc)
Clinically significant
Not clinically significant
Relieve bladder
distension as medically
advised (i.e. IDC / IC)
Monitor for clinical signs
and symptoms (i.e. observe urine output)
Modify and Monitor Common Risk Factors
> faecal impaction> impaired mobility> neurological conditions
(i.e. multiple sclerosis, stroke, Parkinson’s disease)
> longstanding diabetes> drugs (antihypertensives,
anticholinergics, antispasmodics, atropine, sedatives)
> urethral obstruction (i.e. benign prostatic hypertrophy, urethral stricture, prostate cancer, tumours)
> spinal injury or disease> spinal anaesthesia> surgical manipulation of the bladder
nerves
Facts about Bladder Emptying
> Bladder emptying can be affected by:- a lack of privacy- voiding in unfamiliar places- voiding on command- voiding with a partially or
overfilled bladder- pain
> It is also affected by the above mentioned risk factors
*The Clinical Significance of PVR
There is no professional consensus on the PVR that constitutes an upper or lower threshold
The PVR measurement is one of many factors to be considered in determining treatment options
Other factors to consider include:
> The person’s preferences for treatment
> Psychosocial status, quality of life> The potential for upper tract
damage> The type and severity of symptoms> The results of investigations> Comorbidities, prognosis> Underlying pathology
This project was undertaken by Professor Bev O’Connell and Ms Joan Ostaszkiewicz, Deakin—Southern Health Nursing Research Centre, School of Nursing, Deakin University, Melbourne and Dr Chantal Ski, Hobsons Australia. It was funded by The National Continence Management Strategy: an initiative of The Australian Government Department of Health and Ageing (2006).
Distinguishing Symptoms
PVR / PAIN /
DISTRESS / AGITATION
PVR / NO PAIN /
NO DISTRESS / NO AGITATION
Plan of Care Plan of Care
Notify Medical Practitioner In collaboration with Medical Practitioner, establish the clinical
significance of the PVR*
Relieve bladder distension as medically advised (i.e. IDC / IC)
© Continence Foundation of Australia

A u s t r a l i a n a n d N e w Z e a l a n d C o n t i n e n c e J o u r n a l
82 Vol. 14, No. 3 • Spring 2008
there has been a lack of clear guidance on which to base current
practice. An ongoing dilemma is the lack of consensus about
the clinical signi�cance of PVR in older adults. This absence
of evidence has important implications for nurses who are
often required to make judgements about when to intervene
and seek more specialised advice. The survey of clinicians
that was conducted prior to the development of the guideline
revealed considerable variability in practice in relation to the
management of this condition.
In order to assist nurses’ clinical decision making on this issue,
this research resulted in a guideline that provides a framework for
the nursing assessment and management of urinary retention in
hospitalised older adults. It is based on the best available evidence
at the time it was created and was developed in consultation with
a multidisciplinary expert panel. Information is included on key
signs and symptoms for urinary retention in hospitalised older
adults, risk factors that need to be considered in the decision
making process, factors that a�ect normal bladder emptying,
and on the gap in evidence on the clinical importance of PVR
in older adults. As such, it recommends that nurses interpret the
�nding of PVR in collaboration with a medical practitioner and
in context with other factors (Figure 1).
Although the guideline was developed for the nursing care of
older people in acute and subacute settings, it may also be useful
to other healthcare professionals who are involved in the initial
management of this condition and in other healthcare settings.
It is important that this research be viewed as foundational and
that further trial and evaluation of the guideline is undertaken in
a range of populations and settings.
Acknowledgements
This project was funded by the Department of Health and
Ageing as part of the National Continence Management Strategy.
The authors would like to thank the experts for their valuable
input to the development of the guideline and colleagues who
provided feedback on drafts of the manuscript.
R eferences1. Bonde HT et al. Residual urine in 75-year-old men and women: a
normative population study. Scand J Urol Nephrol 1996; 30(2):89-91.
2. Grosshans CL, Passadori Y & Peter P. Urinary retention in the elderly: a study of 100 hospitalised patients. J Am Geriat Soc 1993; 41:633-638.
3. Jacobsen SJ et al. Natural history of prostatism: risk factors for acute urinary retention. J Urol 1997; 158:481-487.
4. Munstonen S, Ala-Houhala I O & Tammela TL. Long-term renal dysfunction in patients with acute urinary retention. Scand J Urol Nephrol 2001; 35:44-48
5. O ’Connell B, O staszkiewicz J & Ski C. Development and trial of best practice protocol for management of urinary retention in elderly patients in acute and sub-acute settings. Deakin University, Australia, 2006, p.1-103.
© Continence Foundation of Australia

A u s t r a l i a n a n d N e w Z e a l a n d C o n t i n e n c e J o u r n a l
83Vol. 14, No. 3 • Spring 2008
6. Adler M & Ziglio E. Gazing into the O racle. Jessica Kingsley Publishers: Bristol, PA, 1996.
7. Dunham RB. The Delphi technique, 1998. Retrieved from http://www.medsch.wisc.edu/adminmed/2002/orgbehav/delphi.pdf20.10.07.
8. American Urological Association, 2004. Retrieved from http://www.urologyhealth.org/glossary/index.cfm?letter=U 20.04.06.
9. Abrams P et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002; 21:167-178.
10. Wareing M. Urinary retention: issues of management and care. Emerg Nurse 2003; 11(8):24-27.
11. Resnick NM, Elbadawi AE & Yalla SV. Age and the lower urinary tract: what is normal? Neurourol Urodyn 1995; 14:1657.
12. P�sterer MH, Gri�ths DJ, Schaefer W & Resnick NM. The e�ect of age on lower urinary tract function: a study in women. J Am Geriat Soc 2006; 54(3):405-412.
13. Lepor H, Sunaryade L, Hartanto V & Shapiro E. Quantitative morphology of the adult human bladder. J Urol 1992; 148:414-417.
14. Hald T & Horn T. The human urinary bladder in aging. Br J Urol 1998; 82(suppl 1):59-64.
15. Gosling JA. Modi�cation of bladder structure in response to out�ow obstruction and aging. Eur Urol 1997; 32(suppl 1):9-14.
16. Resnick NM & Yalla SV. Detrusor hyperactivity with impaired contractile function. An unrecognized but common cause of incontinence in elderly patients. J Am Med Assoc 1987; 257:3076-3081.
17. Starer P & Libow LS. The measurement of residual urine in the evaluation of incontinent nursing home residents. Arch Gerontol Geriat 1988; 7:75-81.
18. Malone-Lee J & Wahedna L. Characteristics of detrusor contractile function in relation to old age. Br J Urol 1993; 72:873-880.
19. Wu J & Baguley IJ. Urinary retention in a general rehabilitation unit. Arch Phys Med Rehab 2005; 86(9):1772-1777.
20. O uslander JG & Schnelle JF. Incontinence in the nursing home. Ann Int Med 1995; 122(6):438-449.
21. Resnick B. A bladder scan trial in geriatric rehabilitation. Rehab Nurs 1995; 20(4):194-203.
22. Kelly CE. Evaluation of voiding dysfunction and measurement of bladder volume. Rev Urol 2004; 6(Suppl 1):S32-S37.
23. Nordling J. The aging bladder: a signi�cant but underestimated role in the development of lower urinary tract symptoms. Exp Gerontol 2002; 37:990.
24. Agency for Health Care Policy and Research (AHCPR). Urinary Incontinence in Adults: Acute and Chronic Management. Clinical Practice Guideline No. 2, 1996 update. US Department of Health and Human Services. Public Health Service, Agency for Health Care Policy and Research. AHCPR publication No. 96-0682. March 1996.
25. Borrie MJ et al. Urinary retention in patients in a geriatric rehabilitation unit: prevalence, risk factors and validity of bladder scan evaluation. Rehab Nurs 2001; 26(5):186-191.
26. Dromerick AW & Edwards DF. Relation of post void residual to urinary tract infection during stroke rehabilitation. Arch Phys Med Rehab 2003; 84:1369-1372.
27. Fonda D et al. Incontinence in the frail elderly. In: Abrams P et al. (Eds). 3rd International Consultation on Incontinence: Recommendations of the International Scienti�c Committee. Plymouth, UK: Plymouth Distributors Ltd, 2005, p.1163-1239.
28. Gray M. Urinary retention. Management in the acute setting. Part 2. Am J Nurs 2000; 100(8):36-44.
29. Hilton P & Stanton SL. Algorithmic method for assessing urinary incontinence in elderly women. Br Med J [Clin Res Ed] 1981; 282:940-992.
30. Mainprize TC & Drutz HP. Accuracy of total bladder volume and residual urine measurements: comparison between real-time ultrasonography and catheterization. Am J O bstet Gynecol 1989; 160:1013-1016.
31. O uslander JG. Urinary incontinence in the elderly. West J Med 1981; 135(6):482-491.
32. Resnick NM. Noninvasive diagnosis of the patient with complex incontinence. Gerontology 1990; 36(suppl 2):8-18.
33. Smith NKG & Albazzaz MK. A prospective study of urinary retention and risk of death after proximal femoral fracture. Age Ageing 1996; 25:150-154.
34. Tam C, Wong K & Yip W. Incomplete bladder emptying in elderly wards. Conference Abstracts of the 35th Annual Meeting International Continence Society. Neurourol Urodyn 2005.
35. Taylor JA & Kuchel GA. Detrusor underactivity: clinical features and pathogenesis of an under diagnosed geriatric condition. J Am Geriat Soc 2006; 54(12):1920-1932.
36. Birch NC, Hurst G & Doyle PT. Serial residual volumes in men with prostatic hypertrophy. Br J Urol 1998; 62:571.
37. Dunsmuir WD et al. The day-to-day variation (test-retest reliability) of residual urine measurement. Br J Urol 1996; 77:192-193.
38. Gri�ths DJ, Harrison G, Moore K & McCracken P. Variability of post-void residual urine volume in the elderly. Urolog Res 1996; 24(1):23-26.
© Continence Foundation of Australia