-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
1/10
DOI: 10.1542/peds.2012-0177; originally published online
November 5, 2012;2012;130;e1567PediatricsKathleen Gallagher
Elizabeth Rausch-Phung, Cynthia Schulte, Barbara Valure, Gregory
L. Armstrong andAbedi, Stephen Goodell, Jacqueline Lawler, Huong Q.
McLean, Lynn Pollock,Ikechukwu U. Ogbuanu, Preeta K. Kutty, Jean M.
Hudson, Debra Blog, Glen R.
OutbreakImpact of a Third Dose of Measles-Mumps-Rubella Vaccine
on a Mumps
http://pediatrics.aappublications.org/content/130/6/e1567.full.html
located on the World Wide Web at:The online version of this
article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005.
Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois,
60007. Copyright 2012 by the American Academypublished, and
trademarked by the American Academy of Pediatrics, 141 Northwest
Point
publication, it has been published continuously since 1948.
PEDIATRICS is owned,PEDIATRICS is the official journal of the
American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/130/6/e1567.full.htmlhttp://pediatrics.aappublications.org/content/130/6/e1567.full.htmlhttp://pediatrics.aappublications.org/content/130/6/e1567.full.htmlhttp://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/content/130/6/e1567.full.html
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
2/10
Impact of a Third Dose of Measles-Mumps-Rubella
Vaccine on a Mumps Outbreak
WHATS KNOWN ON THIS SUBJECT: Mumps outbreaks continue to
occur among unvaccinated and highly vaccinated populations.
In
highly vaccinated populations, options for outbreak control
are
limited. No previous study has documented the impact of a
third
measles-mumps-rubella (MMR) vaccine dose on a mumps
outbreak.
WHAT THIS STUDY ADDS: Our study assessed the use of a third
MMR vaccine dose for mumps outbreak control in a setting
with
preexisting high 2-dose vaccine coverage. The findings
suggest
a potential role of MMR vaccine for outbreak control in such
limited settings.
abstractBACKGROUND AND OBJECTIVE: During 20092010, a
northeastern US
religious community experienced a large mumps outbreak
despite
high 2-dose measles-mumps-rubella (MMR) vaccine coverage. A
third dose of MMR vaccine was offered to students in an
affected
community in an effort to control the outbreak.
METHODS: Eligible sixth- to 12th-grade students in 3 schools
were
offered a third dose of MMR vaccine. Baseline and follow-up
surveys and physician case reports were used to monitor
mumps
attack rates (ARs). We calculated ARs for defined 3-week
periods
before and after the intervention.
RESULTS: Of 2265 eligible students, 2178 (96.2%) provided
documen-
tation of having received 2 previous doses of MMR vaccine, and a
high
proportion (1755 or 80.6%) chose to receive an additional
vaccine dose.
The overall AR for all sixth- to 12th-grade students declined
from 4.93%
in the prevaccination period to 0.13% after vaccination (P,
.001).
Villagewide, overall AR declined by 75.6% after the
intervention. A
decline occurred in all age groups but was significantly
greater
(96.0%) among 11- to 17-year-olds, the age group targeted
for
vaccination, than among all other age groups. The proportions
of
adverse events reported were lower than or within the range
of
those in previous reports of first- and second-dose MMR
vaccine
studies.
CONCLUSIONS: This is the first study to assess the impact of a
third
MMR vaccine dose for mumps outbreak control. The decline in
in-
cidence shortly after the intervention suggests that a third
dose
of MMR vaccine may help control mumps outbreaks among popu-
lations with preexisting high 2-dose vaccine coverage.
Pediatrics
2012;130:e1567e1574
AUTHORS: Ikechukwu U. Ogbuanu, MD, MPH, PhD,
a,b
PreetaK. Kutty, MD, MPH,b Jean M. Hudson, MD, MPH,c Debra
Blog,
MD, MPH,d Glen R. Abedi, MPH,b Stephen Goodell, RN, BSN,
MPH,c Jacqueline Lawler, MPH, CPH,c Huong Q. McLean,
MPH, PhD,b Lynn Pollock, RN, MSN,d Elizabeth Rausch-
Phung, MD, MPH,d Cynthia Schulte, RN, BSN,d Barbara
Valure, RN, BSN,c Gregory L. Armstrong, MD,b and Kathleen
Gallagher, MPH, DScb
aEpidemic Intelligence Service, Centers for Disease Control
and
Prevention, Atlanta, Georgia; bNational Center for
Immunization
and Respiratory Diseases, Atlanta, Georgia; cOrange County
Health Department, Goshen, New York; and dBureau of
Immunization, New York State Department of Health, Albany,
New York
KEY WORDS
measles-mumps-rubella (MMR) vaccine, mumps, outbreak, third
dose
ABBREVIATIONS
ACIPAdvisory Committee on Immunization Practices
ARattack rate
CIconfidence interval
MMRmeasles-mumps-rubella
OCHDOrange County Health Department
RRrelative risk
This work was presented in part at the 2010 International
Conference for Emerging Infectious Diseases; July 1114,
2010;
Atlanta, GA.
The findings and conclusions in this article are those of
theauthors and do not necessarily represent the views of the
Centers for Disease Control and Prevention.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-0177
doi:10.1542/peds.2012-0177
Accepted for publication Jul 12, 2012
Address correspondence to Preeta K. Kutty, MD, MPH, 1600
Clifton
Rd, NE, MS A34, Centers for Disease Control and Prevention,
Atlanta, GA 30333. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have
no financial relationships relevant to this article to
disclose.
FUNDING: No external funding.
PEDIATRICS Volume 130, Number 6, December 2012 e1567
ARTICLE
at Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
mailto:[email protected]://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/mailto:[email protected]
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
3/10
Before the introduction of mumps
vaccine, epidemics of mumps occurred
throughout the United States, fre-
quently in crowded settings such
as prisons, orphanages, schools, and
military facilities.1 In 1967, a live
mumps virus vaccine was licensed inthe United States. In 1977,
the Advisory
Committee on Immunization Practices
(ACIP) recommended 1 dose of mumps
vaccine for all children aged 12 months
or older.2 After this, mumps incidence
declined rapidly from 50 to 251 reported
cases/100 000 persons before 1967
to 2/100 000 persons in 1988.3 In
1989, to enhance measles control,
ACIP recommended a second dose of
measles-mumps-rubella (MMR) vaccine;widespread use of 2 doses of
MMR
vaccine resulted in further declines in
mumps incidence.4 During 20002005, his-
toric annual lows of,300 mumps cases
were reported (incidence 0.1/100 000
persons). Coverage with at least 1 dose
of MMR vaccine was between 90.5%
and 91.5% nationwide among children
aged 19 to 35 months.5,6 In 2006,
according to the National Immunization
Survey, provider-verified 2-dose cover-age for MMR vaccine among
adoles-
cents aged 13 to 17 years was 87.0%.7
Mumps outbreaks in 2006 and 2009
2010 represented outbreaks in high
2-dose populations, with the latter pro-
viding a unique opportunity to study
the use of a third dose for mumps
outbreak control. In 2006, despite con-
tinued high MMR vaccine coverage, the
United States experienced the largest
mumps outbreak in 2 decades, with6584 reported cases (incidence
2.2/
100 000 persons). The highest inci-
dence occurred among persons aged
18 to 24 years (incidence 31.1/100 000
persons versus 8.4/100 000 persons
among all other age groups combined),
many of whom were midwestern col-
lege students who had received 2
doses of mumps-containing vaccine.8
In 2007 and 2008, there were 800
(incidence 0.27/100 000 persons) and 454
(0.15/100 000 persons) reported mumps
cases, respectively.9 In both years, the
1-dose coverage with MMR vaccine
among children aged 19 to 35 months
was 92.1% to 92.3%,5 and the 2-dose
coverage among adolescents aged 13to 17 years was 88.9% to
89.3%.10
In 2009, the United States experienced
the next largest mumps outbreak in 2
decades among highly vaccinated
populations. On June 28, an 11-year-old
US resident with a history of receiving 2
doses of MMR vaccine developed par-
otitis after returning from the United
Kingdom, where a mumps outbreak
was ongoing.11 During his infectious
period, he attended a summer campfor Orthodox Jewish boys in New
York
state; subsequently, 25 cases occurred
at the camp. When the camp ended and
attendees returned to their homes,
community transmission occurred,
resulting in mumps outbreaks in mul-
tiple locations in northeastern United
States, including Orange County, New
York. Most cases were among mem-
bers of Orthodox Jewish communities
who had received 2 previous doses ofMMR vaccine.
In Orange County, mumps cases were
first reported in September 2009. By
December 31, 2009, 392 mumps cases
were reported to the Orange County
Health Department (OCHD); 290 (74%)
had received 2 doses of MMR vaccine.
Adolescents aged 11 to 17 years
accounted for 72% of cases; 92% had
received 2 age-appropriate doses of
MMR vaccine. Reported cases wereconcentrated in a singlevillage
that had
its own schools. Village members had
limited contact with neighboring vil-
lages. The high average household size
in the affected community (5.7 versus
the US national average of 2.6)12 cre-
ated an environment for possible aug-
mentation of transmission. As a result,
the outbreak continued despite stan-
dard outbreak control measures (eg,
isolation of cases and ensuring ap-
propriate vaccination of contacts). The
characteristics of the village and on-
going mumps transmission in a setting
of high 2-dose MMR vaccine coverage
provided a unique opportunity to eval-
uate the use of a third dose of MMRvaccine for mumps outbreak
control.
This report describes the impact of the
third dose of MMR vaccine on the
mumps outbreak.
METHODS
The affected village in Orange County
had a population of 20 363 in 2010 and
a median age of 10.6 years.13 The vil-
lage is served by 4 schools. Health care
is provided mainly by 4 physician
practices.
Because a high proportion of the
mumps cases were among students in
grades 6 to 12, a school-based vacci-
nation interventionwas proposed.To be
eligible, a school needed to provide
evidence of ongoing mumps trans-
mission in the 2 weeks preceding the
vaccination intervention, conducted
from January 19 to February 2, 2010,
and to document high 2-dose mumpsvaccine coverage among the
students
by using the Comprehensive Clinical
Assessment Software Application.14
As part of standard mumps outbreak
control, a dose of MMR vaccine was
offered to all students who had 0 or 1
previous MMR doses. However, eligi-
bility for the third dose study was de-
termined by documented evidence of
previous receipt of 2 MMR vaccine
doses. Students were eligible to receivea third dose of MMR
vaccine if they
reported no history of mumps during
the current outbreak and provided
a signed consent from their parent or
guardian and their own written assent
before vaccination. Validation of receipt
of 2 previous doses of MMRvaccinewas
conducted by reviewing school vacci-
nation records and, if missing, by
contacting the students physician.
e1568 OGBUANU et alat Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
4/10
Because a third dose of MMR vaccine is
not recommended by the ACIP, this
study was reviewed and approved by
the Institutional Review Boards at the
Centers for Disease Control and Pre-
vention and the New York State De-
partment of Health.
Mumps Case Ascertainment and
Estimation of Third Dose
Vaccination Coverage
Mumps reporting is mandatory in New
York.15 We ascertained mumps cases
from 2 sources: notifications to OCHD
and surveys of parents and guardians
in the eligible schools. Reported cases
were investigated to obtain additional
epidemiological, clinical, laboratory,
and vaccination information. Only
mumps cases with onset dates during
the outbreak (September 1, 2009 to
June 30, 2010) were included in our
analyses. Mumps cases were classified
by using the 2008 Council of State
and Territorial Epidemiologists defi-
nitions.16 We checked for duplicate
reports of cases in OCHD registry and
our surveys. There were 3 participants
in OCHD registry who did not report
having mumps in the surveys; thesewere considered mumps cases in
the
analysis.
A baseline survey was distributed to all
sixth- to 12th-grade students to collect
information on demographic charac-
teristics, vaccination history, mumps
history, clinical features and compli-
cations of recent episodes of mumps,
and health care provider information.
Two months (ie, .2 incubation peri-
ods) after the vaccination intervention,we distributed a
follow-up survey to all
sixth- to 12th-grade students at par-
ticipating schools, whether or not they
had completed the baseline survey or
received vaccine during the interven-
tion. The self-report follow-up survey
collected information on symptoms as-
sociated with mumps that occurred
after the intervention, as well as lo-
cal and systemic adverse events
after the receipt of the third dose
MMR vaccine.
Statistical Analysis
Mumps attack rates (ARs) were calcu-
lated for students who participated in
the study and received a third dose.
Three time periods were defined in
relation to each students date of re-
ceipt of the third dose of MMR vaccine.
We also calculated mumps ARs for the
entire village. For the village analysis,
3 time periods were defined for all
persons, irrespective of vaccination
status. Because the vaccination in-
tervention was limited to schools,
dates of vaccination were not available
for other village residents. Therefore,the 2-week vaccination
period, January
19 to February 2, 2010, was excluded
from the periods defined to analyze
villagewide ARs. Data from the surveys
were entered into Microsoft Access
2003 (Microsoft Corp, Redmond, WA)
and deidentified data were analyzed in
SAS 9.2 (SAS Institute Inc, Cary, NC).
P values of,.05 were considered to
indicate statistical significance.
Mumps ARs Among Sixth- to 12th-
Grade Students in the Participating
Schools
Among students in the participating
schools who were eligible for vaccina-
tion and completed the survey, we
calculated ARs during three 21-day time
periods based on each students vac-
cination date; the 21-day time periods
were based on the average mumps
incubation period of 16 to 18 days,
range, 12 to 25 days.17 The 3 timeperiods were: (1)
prevaccination, the
21-day period before vaccination; (2)
postvaccination phase 1, 21 days af-
ter the day of vaccination; and (3)
postvaccination phase 2, the 21 days
after postvaccination phase 1. We as-
sumed that some of the cases in post-
vaccination phase 1 were among
students who had been incubating
the virus at the time of vaccination,
whereas cases in postvaccination
phase 2 were a result of exposures
occurring after vaccination. For the
purpose of this analysis, students who
did not receive the vaccine were
assigned a vaccination date, based
on the vaccination dates of students ofthe same class, gender,
and age. ARs
were calculated as the number of new
mumps cases occurring in each of the
specified time periods, divided by the
number of susceptible students. Sus-
ceptible students included only those
who did not have mumps at the be-
ginning of the specified time period of
analysis. Relative risks (RRs) and 95%
confidence intervals (CIs) were calcu-
lated. Among students eligible fora third-dose MMR vaccination,
we also
calculated the incremental vaccine ef-
fectiveness (ie, the decline in risk of
disease among students who received
the third dose of MMR vaccine in
comparison with students who had
only received 2 doses) by using the
formula (vaccine effectiveness = 1 2
rate ratio).
Mumps ARs Among All Age Groups
VillagewideVillagewide ARs among residents were
calculated by using OCHD mumps reg-
istry for three 21-day time periods de-
fined around the vaccine intervention
period (January 19 to February 2): (1)
preintervention, the 21 days before
the intervention period; (2) post-
intervention phase 1, 21 days after
intervention period; and (3) postin-
tervention phase 2, the 21 days after
the postintervention phase 1.Because most of thesixth- to
12th-grade
students were aged 11 to 17 years, ARs
were calculated for this age group and
other age groups defined as,5 years,
5 to 10 years, 18 to 24 years, and $25
years. ARs for each age group were
calculated by using the village pop-
ulation of 20 363, according to the 2010
US Census.13 Relative declines in ARs
after the intervention were compared
ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1569at
Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
5/10
between age groups with Poisson re-
gression.
RESULTS
From June 1, 2009 through June 30,
2010, 3502 mumps cases related to theNortheast mumps outbreak
were re-
ported to the Centers for Disease Control
and Prevention, of which 790 (22.6%)
were from Orange County, New York.
Threeofthe4schoolsinthevillagewere
eligible for this study; the fourth school
reportednomumpstransmissioninthe
2 weeks preceding the intervention.
Ninety-eight percent of schoolchildren
in the village attended these 3 schools.
Among the eligible schools, theweighted2-dose MMR vaccine
coverage
based on the Comprehensive Clinical
Assessment Software Application was
94.3%; vaccination records were in-
complete for the remaining 5.7% of
students. The baseline survey was
conducted concurrently with the vac-
cine intervention, whereas the follow-
up survey was conducted April 5 to 18,
2010. Of the 2688 sixth- to 12th-grade
students in the eligible schools, 2537
(94.4%) returned the baseline surveys
and 2356 (87.7%) returned the follow-
up surveys. Of the 2688 students, 2265
(84.2%) were offered an additional
dose of MMR vaccine (either as a part
of standard outbreak control or as part
of the third-dose intervention; Fig 1);
1258 (55.5%) were females. Of the
2265 students, 2178 (96.2%) had a vali-
dated history of receiving 2 previous
doses of MMR vaccine and were eligi-
ble for the third-dose intervention.Of the 2178 eligible
students, 1755
(80.6%) received a third dose of MMR
vaccine during the intervention. In the
comparisonof those whoreceived a third
dose of MMR vaccine and those who did
not, the proportion of male students was
similar, but vaccinated students were
more likely to be from school B (the
largest school) and slightly more likely to
be in the upper grades (Table 1).
Mumps ARs Among Sixth- to 12th-
Grade Students in the 3 Eligible
Schools
Among sixth- to 12th-grade students
who had no previous history of mumps,
the overall AR during the 3-week pre-
vaccination period was 4.9%; ARs werehigher among males (6.99%)
than
females (3.25%, P, .001 for compari-
son; Table 2). Rates were higher in
schools A (5.1%) and B (5.3%) than in
school C (2.8%). The overall AR declined
significantly (P, .001) from 4.9% in
the prevaccination period to 1.55%
during the postvaccination phase 1.
The decline in the overall AR from
postvaccination phase 1 to the post-
vaccination phase 2 was also statisti-cally significant (P ,
.001; Table 2).
There were no significant differences
in ARs between males and females
during the postvaccination phase 2
(0.00% for males versus 0.24% for
females; Fisher exact P = .26).
During the postvaccination phase 1, the
overall AR wassimilarin both vaccinated
and unvaccinated students (1.60% and
1.67%, respectively) (Table 2). However,
during the postvaccination phase 2, theAR was eightfold lower
among vacci-
nated students (Table 2), although the
difference was not statistically signifi-
cant (0.06% vs 0.48%, respectively; RR:
0.12; 95% CI: 0.011.32; P = .097). The
incremental effectiveness of the third
dose of vaccine (vaccine effectiveness)
was 88.0%, with a large CI that included
0 (95% CI: 231.9% to 98.9%).
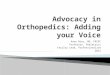
Mumps ARs Among All Age GroupsVillagewide
After the third-dose intervention, ARs
fell substantially among all age groups
in the village (Fig 2). Overall, ARs vil-
lagewide declined from 0.86% during
the 3-week preintervention period to
0.21% during the 3-week postinterven-
tion phase 2, a 75.6% relative decline
(Table 3). This decline was statistically
significant only among 11- to 17-year-
olds (96.0% relative decline) and
among 5- to 10-year-olds (72.9% rela-
tive decline). The relative decline in ARs
in the 11- to 17-year age group was
significantly greater (P, .005) than
that in any of the other 4 age groups.
Self-reported Adverse Events After
Immunization
Of the1755individuals whoreceived the
third dose of MMR vaccine, 1597 (91.0%)
returned the follow-up survey.18 Of
those, 115 (7.2%) reported at least 1
local or systemic adverse event in the
2 weeks after vaccination. The most
commonly reported adverse events
were pain, redness, or swelling at the
injection site
(3.6%) andjoint or mus-
cle aches (1.8%). No serious adverse
events were reported in the survey, and
a search of local physician records re-
vealed no serious adverse events among
the affected age groups.
DISCUSSION
This is the first documented study to
assess the impact of a third dose of
MMR vaccine on the course of a mumps
outbreak in a highly vaccinated pop-ulation, in which standard
outbreak
response measures had not been ef-
fective in halting theoutbreak. After the
intervention, there was a reduction in
cases in all age groups, but this decline
was particularly prominent and rapid
among the older students (1117 years
of age) targeted for vaccination. The
proportions of adverse events reported
in this study were lower than or within
the range of those in previous reportsoffirst- and second-dose
MMR vaccine
studies.
The circumstances of this outbreak
response did not allow for the ideal
evaluation of the effect of a third dose
of vaccine, a randomized, placebo-
controlled clinical trial. In addition,
the intervention occurred immediately
after the peak of the outbreak. For this
reason, it is not possible to exclude the
e1570 OGBUANU et alat Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
6/10
possibility that the rapid decline in in-
cidence after the intervention was en-tirely unrelated to our
intervention.
Declines in incidence were seen among
19.4% of students eligible for vaccina-
tion (but not vaccinated) after the in-
tervention as well as among age groups
not eligible for vaccination. However,
the decline observed in the vaccinated
age group (96.2% among 11- to 17-year-
olds) was statistically significant,
greater than that seen in any other age
group. Furthermore, because trans-
mission was particularly intenseamong the 11-to 17-year-olds,
and such
a large proportion of this group was
vaccinated during the intervention, it is
reasonable to expect the intervention to
provide herd-immunity effects that
would decrease incidence in nonvac-
cinated individuals. One would expect
these effects to be most prominent
among unvaccinated students in the
same classes as the vaccinated students,
as well as among 5- to 10-year-olds, the
only other age group attending the same
schools as the vaccinated children. After
the intervention, incidence of mumps in
this latter group fell by 72.8%, less thanthat observed in the
vaccinated age
group but more than that observed in
any other age group.
Mumps-containing vaccines havebeen
used for outbreak control among
populations that were largely un-
vaccinated.1721 In 1976, mumps vac-
cine was administered to a proportion
of the population during an epidemic of
mumps on St. Paul Island, Alaska, and
transmission among vaccinees stop-ped approximately a month
earlier than
among those who were unvaccinated.19
Similarly, in 1986, at a time when only 1
dose of MMR vaccine was recom-
mended in the United States, mumps
vaccine was provided to 414 students
and staff of a high school experi-
encing a mumps outbreak primarily
among unvaccinated students.21 The
authors concluded that the vaccination
TABLE 1 Comparison of Demographic Characteristics of the Sixth-
to 12th-Grade Students Duringa School-Based Third-Dose MMR Vaccine
Intervention: Orange County, New York, 20092010
C haracteris tics S tud ents Who Did Not
Receive a Third Dose
(n= 423), n (%)
Students Who
Received a Third Dose
(n= 1755), n(%)
x2
P
School ,.0001
School A 88 (21) 170 (10)
School B 249 (59) 1329 (76)
School C 86 (20) 256 (15)
Gender .75
Females 234 (55) 986 (56)
Males 189 (45) 769 (44)
Grade category .042
68 201 (48) 738 (42)
912 222 (52) 1017 (58)
FIGURE 1Study enrollment, sixth- to 12th-grade students in the 3
eligible schools, Orange County, New York, 2009 2010.
ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1571at
Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
7/10
intervention may have had an impact on
controlling the outbreak (postinter-
vention RR = 0 [95% CI: 00.85]). Unlike
these previous studies, this article as-
sessed the use of a third MMR vaccine
dose for outbreak control among apopulation with preexisting
high 2-dose
vaccine coverage.
Previous estimates of mumps vaccine
effectiveness have ranged from 66% to
95%for 2 doses, consistently lower than
estimates for measles vaccine effec-
tiveness (95%100%).2229 No data are
available from this study regarding the
immune response after a third MMR
vaccine dose. Because of the high rate
of vaccine uptake (80.6%) and thesmall number of cases (2
among
the 413 unvaccinated students and 1
among the 1723 vaccinated students)
that occurred .1 incubation period
after vaccination, we are unable to
directly evaluate the vaccine effective-
ness. However, during this outbreak
intervention, the rapid decline in
incidence in the target age group
suggests a rapid immune response to
the third dose that resulted in relatively
high mumps vaccine effectiveness. This
finding is consistent with available data
that demonstrated that a third dose of
MMR vaccine administered to seroneg-
ative college students resulted in rapidmumps virus
immunoglobulin G re-
sponse, suggesting the capacity to
mount an anamnestic immune response
in previously vaccinated individuals.30
Thus, a gap in protective efficacy as
a result of suboptimal vaccine effec-
tiveness, coupled with the potential for
a rapid anamnestic immune response,
support thepotential role of a third dose
of a mumps-containing vaccine as an
effective strategy for outbreak control ina setting of high
2-dose coverage.
Future mumps outbreaks are likely to
occur among highly vaccinated pop-
ulations, as seen in recent outbreaks in
the United States and elsewhere.8,1720
Factors possibly contributing to these
outbreaks include crowding, primary
vaccine failure, suboptimal vaccine ef-
fectiveness, waning immunity, and the
lack of natural boosting of mumps im-
munity by wild-type virus.8,1720 The
susceptibility of our study population
was likely due to a high force of in-
fection secondary to crowding, al-
though waning immunity might be
a factor as well. It is possible that theunusually large
household size and
crowding in the study halls at the re-
ligious schools may have augmented
the transmission of mumps. A similar
trend has been noted in previous
mumps outbreaks in crowded prisons,
orphanages, schools, and military fa-
cilities,1 as well as in the 2006 mumps
outbreak, which affected mostly stu-
dents in college dormitories.8
While the use of a third dose of MMRvaccine may have been
effective in
limiting the size and duration of the
outbreak described here, this finding
should not support the routine use of
a third dose of mumps vaccine in na-
tional vaccination programs. Although
there were few mumps cases after the
intervention because of the highuptake
of thevaccine in thetargetedage group,
the results of our study suggest that
TABLE 2 Mumps ARs Among Sixth- to 12th-Grade Students During
Selected 3-Week Periods Before and After a School-Based Third-Dose
MMR VaccineIntervention During an Outbreak of Mumps, Orange County,
New York, 20092010
Prevacc ination (21 d ) Postvaccination
Phase 1a (21 d)
Postvaccination
Phase 2b (21 d)
Comparison of ARs in
Postvaccination Phase 2
and Postvaccination
Phase 1
No. of
MumpsCases
Population
at Risk
AR
(%)
No. of
MumpsCases
Population
at Risk
AR
(%)
No. of
MumpsCases
Population
at Risk
AR
(%)
RR (95% CI) P
All studentsc
All students 113 2291 4.93 35 2258 1.55 3 2223 0.13 0.06
(0.020.19) ,.001
Females 41 1261 3.25 15 1256 1.19 3 1241 0.24 0.21 (0.060.73)
.006
Males 72 1030 6.99 20 1002 2.00 0 982 0.00 NCd ,.001
Students with a validated history of 2 previous MMR vaccine
doses
Students who did not receive
a third dose of MMR vaccine
7 420 1.67 2 413 0.48 0.3 (0.061.40) .18e
Females 2 234 0.85 2 232 0.86 1.0 (0.147.10) 1.0e
Males 5 186 2.69 0 181 0.00 NCd .06e
Students who received a third
dose of MMR vaccine
28 1751 1.60 1 1723 0.06 0.04 (0.0050.27) ,.001
Females 13 984 1.32 1 971 0.10 0.08 (0.01
0.59) ,.001Males 15 767 1.96 0 752 0.00 NCd ,.001
a Day 1 to day 21 after the vaccination date.b Day 22 to day 42
after the vaccination date.c Refers to students in the eligible 3
schools who did not have a history of mumps and who had not
received a third dose of MMR vaccine before the vaccination date.d
NC: Could not be calculated because of empty cells.e P value
calculated by using the Fisher exact test.
e1572 OGBUANU et alat Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
8/10
administration of a third dose of MMR
vaccine may be an effective method of
controlling mumps outbreaks among
highly vaccinated populations in cer-
tain settings. With the changing mumps
epidemiology and limited options for
outbreak control, additional studies to
verify these findings in other settings
are warranted. In addition vaccine im-
munogenicity studies in a highly vac-
cinated population receiving a third
dose is of potential value to aid in un-
derstanding the kinetics of the immune
response. Future studies should also
attempt to better understand the dy-
namics of mumps immunity, as well as
the biological correlates of protection
afforded by the current vaccine.
ACKNOWLEDGMENTS
WethankHardeep S. Sandhu, MD,MBBS,
for supervisory guidance through-
out the study period; Kathleen A.
Wannemuehler, PhD and Aaron Curns,
FIGURE 2Villagewide mumps ARs by age group and by 2-week
intervals, Orange County, New York, June 1, 2009 through June 30,
2010 ( n = 790).
TABLE 3 Population-level Age-specific Mumps ARs in the Village,
Orange County, New York, 20092010a
Age
Group, y
Preintervention Periodb (21 d) Postintervent ion Phase 1c (21 d
) Postin tervention Ph ase 2d (21 d) Relative % Declin e
No. of Mumps
Cases
Population
at Risk
Age-specific
AR, %
No. of Mumps
Cases
Population
at Risk
Age-specific
AR, %
No. of Mumps
Cases
Population
at Risk
Age-specific
AR, %
All 172 19 993 0.86 87 19 717 0.44 41 19 630 0.21 75.6 (66.0 to
83.0)
,5 7 4592 0.15 11 4575 0.24 5 4564 0.11 26.7 (2126.0 to
77.0)
510 60 4316 1.40 40 4220 0.95 16 4180 0.38 72.9 (52.0 to
84.0)
1117 78 3210 2.40 8 3091 0.26 3 3083 0.10 96.0 (87.0 to
99.0)
1824 17 2355 0.72 7 2333 0.30 8 2326 0.34 52.8 (211.0 to
79.0)
$25 10 5521 0.18 21 5499 0.38 9 5478 0.16 11.1 (2123 to
63.0)
a Mumps cases reported to the OCHD and population for the
village based on the 2010 population census by the US Census
Bureau.b Preintervention period: 21 days before the third dose MMR
vaccine intervention period.
c Postintervention phase 1: 21 days after the intervention, that
is, day +1 to day +21.d Postintervention phase 2: 21 days after the
intervention period, that is, day +22 to day +42.
ARTICLE
PEDIATRICS Volume 130, Number 6, December 2012 e1573at
Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
9/10
MPH for statistical support; Jane
Seward, MBBS, MPH, Gregory Wallace,
MD, MPH, and Rafael Harpaz, MD,
MPH, for providing advice on the study
design and data interpretation and
comments on early versions of the
manuscript; and Mary McCauley, MS
for editorial support. We alsoespecially
thank all the students and their par-
ents who participated in the study;
the staff of the affected schools and
the medical clinics that serve the af-
fected community for providing assis-
tance with case finding/documentation
and access to vaccination records; and
the study staff from the New York State
and Orange County health departments
for providing logistical and clinical sup-
port during the school-based mass vac-
cination clinics (see the Supplemental
Information for a complete list).
REFERENCES
1. Hirsch A. Mumps (Parotitis epidemica s.
polymorpha). In: Handbook of Geographical
and Historical Pathology. Volume III. Lon-
don, UK: The New Sydenham Society; 1886:
277283
2. Center for Disease Control and Prevention.
Mumps vaccine. Recommendation of Public
Health Service Advisory Committee on Im-
munization Practices. Morbid Mortal WklyRep.
1977;26(48):393394
3. Barskey AE, Glasser JW, LeBaron CW.
Mumps resurgences in the United States:
a historical perspective on unexpected
elements. Vaccine. 2009;27(44):61866195
4. Watson JC, Hadler SC, Dykewicz CA, Reef S,
Phillips L; Centers for Disease Control and
Prevention. Measles, mumps, and rubella
vaccine use and strategies for elimination
of measles, rubella, and congenital rubella
syndrome and control of mumps: recom-
mendations of the Advisory Committee
on Immunization Practices (ACIP). MMWRRecomm Rep.
1998;47(RR-8):157
5. Centers for Disease Control and Prevention
(CDC). National, state, and local area vac-
cination coverage among children aged 19-
35 months United States, 2009. MMWR
Morb Mortal Wkly Rep. 2010;59(36):11711177
6. Centers for Disease Control and Pre-
vention. National Immunization Survey.
Available at: www.cdc.gov/vaccines/stats-
surv/nis/default.htm#nis. Accessed Sep-
tember 18, 2012
7. Centers for Disease Control and Pre-
vention. National Vaccination Coverage
Among Adolescents Aged 1317 Years
United States, 2006. MMWR. 2007;56(34):
885888. Available at: www.cdc.gov/mmwr/
preview/mmwrhtml/mm5634a3.htm?s_cid=
mm5634a3_e. Accessed September 18, 2012
8. Dayan GH, Quinlisk MP, Parker AA, et al. Re-
cent resurgence of mumps in the United
States. N Engl J Med. 2008;358(15):15801589
9. Centers for Disease Control and Prevention
(CDC). Summary of notifiable diseases:
United States, 2009. MMWR Morb Mortal
Wkly Rep. 2011;58(53):1100
10. Centers for Disease Control and Prevention
(CDC). National, state, and local area vac-
cination coverage among adolescents aged
13-17 yearsUnited States, 2008. MMWR
Morb Mortal Wkly Rep. 2009;58(36):9971001
11. Barskey AE, Schulte C, Rosen JB, et al. Mumps
Outbreak among Orthodox Jewish Communi-
ties in the United States. NEJM. In press
12. United States Census Bureau. AmericanCommunity Survey 5-year
estimates. Avail-
able at: http://factfinder.census.gov/main.
html. Accessed September 18, 2012
13. United States Census Bureau. 2010 Pop-
ulation estimates. Available at: http://
factfinder2.census.gov/main.html. Accessed
October 7, 2011
14. Centers for Disease Control and Pre-
vention. Comprehensive Clinic Assessment
Software Application (CoCASA). Available at:
www.cdc.gov/vaccines/programs/cocasa/
default.htm. Accessed October 8, 2011
15. Department of Health. New York State. NewYork codes, rules
and regulations, Title 10.
Available at: www.health.ny.gov/regulations/
nycrr/title_10/. Accessed September 18, 2012
16. Council of State and Territorial Epidemiol-
ogists. Revision of the Surveillance Case
Definition for Mumps. 2007. Available
at: www.cste.org/dnn/AnnualConference/
PositionStatements/tabid/191/Default.aspx.
Accessed September 18, 2012
17. Brockhoff HJ, Mollema L, Sonder GJ, et al.
Mumps outbreak in a highly vaccinated
student population, The Netherlands, 2004.
Vaccine. 2010;28(17):29322936
18. Abedi GR, Mutuc JD, Lawler J et al. Adverse
Events Following a Third Dose of Measles,
Mumps, and Rubella Vaccine in a Mumps
Outbreak. Vaccine. 2012, In press.
19. Whelan J, van Binnendijk R, Greenland K,
et al. Ongoing mumps outbreak in a stu-
dent population with high vaccination cov-
erage, Netherlands, 2010. Euro Surveill.
2010;15(17):19554
20. Stein-Zamir C, Shoob H, Abramson N, Tallen-
Gozani E, Sokolov I, Zentner G. Mumps
outbreak in Jerusalem affecting mainly
male adolescents. Euro Surveill. 2009;14
(50):19440
21. Wharton M, Cochi SL, Hutcheson RH, Bistowish
JM, Schaffner W. A large outbreak of mumps
in the postvaccine era. J Infect Dis. 1988;158
(6):12531260
22. Deeks SL, Lim GH, Simpson MA, et al. An
assessment of mumps vaccine effectiveness
by dose during an outbreak in Canada.CMAJ.
2011;183(9):10141020
23. McLean H, Hickman C, Seward J. Module 16:
Mumps. The Immunological Basis for Im-
munization Series. Geneva, Switzerland:
World Health Organization; 2010. Available
at: http://whqlibdoc.who.int/publications/
2010/9789241500661_eng.pdf. Accessed Sep-
tember 18, 2012
24. Marin M, Nguyen HQ, Langidrik JR, et al.
Measles transmission and vaccine effective-
ness during a large outbreak on a densely
populated island: implications for vaccina-
tion policy. Clin Infect Dis. 2006;42(3):315319
25. Dayan GH, Rubin S. Mumps outbreaks in
vaccinated populations: are available mumps
vaccines effective enough to prevent out-
breaks? Clin Infect Dis. 2008;47(11):14581467
26. Hviid A, Rubin S, Mhlemann K. Mumps.
Lancet. 2008;371(9616):932944
27. Marin M, Quinlisk P, Shimabukuro T,
Sawhney C, Brown C, Lebaron CW. Mumps
vaccination coverage and vaccine effec-
tiveness in a large outbreak among college
studentsIowa, 2006. Vaccine. 2008;26(29
30):36013607
28. Centers for Disease Control and Prevention
(CDC). Measles outbreak
SouthwesternUtah, 1996. MMWR Morb Mortal Wkly Rep.
1997;46(33):766769
29. Yeung LF, Lurie P, Dayan G, et al. A limited
measles outbreak in a highly vaccinated US
boarding school. Pediatrics. 2005;116(6):
12871291
30. Date AA, Kyaw MH, Rue AM, et al. Long-term
persistence of mumps antibody after receipt
of 2 measles-mumps-rubella (MMR) vacci-
nations and antibody response after a third
MMR vaccination among a university pop-
ulation. J Infect Dis. 2008;197(12):16621668
e1574 OGBUANU et alat Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2012-0177/-/DCSupplementalhttp://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2012-0177/-/DCSupplementalhttp://www.cdc.gov/vaccines/stats-surv/nis/default.htm#nishttp://www.cdc.gov/vaccines/stats-surv/nis/default.htm#nishttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5634a3.htm?s_cid=mm5634a3_ehttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5634a3.htm?s_cid=mm5634a3_ehttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5634a3.htm?s_cid=mm5634a3_ehttp://factfinder.census.gov/main.htmlhttp://factfinder.census.gov/main.htmlhttp://factfinder.census.gov/main.htmlhttp://factfinder.census.gov/main.htmlhttp://factfinder2.census.gov/main.htmlhttp://factfinder2.census.gov/main.htmlhttp://factfinder2.census.gov/main.htmlhttp://factfinder2.census.gov/main.htmlhttp://www.cdc.gov/vaccines/programs/cocasa/default.htmhttp://www.cdc.gov/vaccines/programs/cocasa/default.htmhttp://www.health.ny.gov/regulations/nycrr/title_10/http://www.health.ny.gov/regulations/nycrr/title_10/http://www.cste.org/dnn/AnnualConference/PositionStatements/tabid/191/Default.aspxhttp://www.cste.org/dnn/AnnualConference/PositionStatements/tabid/191/Default.aspxhttp://whqlibdoc.who.int/publications/2010/9789241500661_eng.pdfhttp://whqlibdoc.who.int/publications/2010/9789241500661_eng.pdfhttp://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://whqlibdoc.who.int/publications/2010/9789241500661_eng.pdfhttp://whqlibdoc.who.int/publications/2010/9789241500661_eng.pdfhttp://www.cste.org/dnn/AnnualConference/PositionStatements/tabid/191/Default.aspxhttp://www.cste.org/dnn/AnnualConference/PositionStatements/tabid/191/Default.aspxhttp://www.health.ny.gov/regulations/nycrr/title_10/http://www.health.ny.gov/regulations/nycrr/title_10/http://www.cdc.gov/vaccines/programs/cocasa/default.htmhttp://www.cdc.gov/vaccines/programs/cocasa/default.htmhttp://factfinder2.census.gov/main.htmlhttp://factfinder2.census.gov/main.htmlhttp://factfinder.census.gov/main.htmlhttp://factfinder.census.gov/main.htmlhttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5634a3.htm?s_cid=mm5634a3_ehttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5634a3.htm?s_cid=mm5634a3_ehttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm5634a3.htm?s_cid=mm5634a3_ehttp://www.cdc.gov/vaccines/stats-surv/nis/default.htm#nishttp://www.cdc.gov/vaccines/stats-surv/nis/default.htm#nishttp://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2012-0177/-/DCSupplementalhttp://pediatrics.aappublications.org/lookup/suppl/doi:10.1542/peds.2012-0177/-/DCSupplemental
-
7/28/2019 Pediatrics-2012-Ogbuanu-e1567-74.pdf
10/10
DOI: 10.1542/peds.2012-0177; originally published online
November 5, 2012;2012;130;e1567PediatricsKathleen Gallagher
Elizabeth Rausch-Phung, Cynthia Schulte, Barbara Valure, Gregory
L. Armstrong and
Abedi, Stephen Goodell, Jacqueline Lawler, Huong Q. McLean, Lynn
Pollock,Ikechukwu U. Ogbuanu, Preeta K. Kutty, Jean M. Hudson,
Debra Blog, Glen R.
OutbreakImpact of a Third Dose of Measles-Mumps-Rubella Vaccine
on a Mumps
ServicesUpdated Information &
htmlhttp://pediatrics.aappublications.org/content/130/6/e1567.full.including
high resolution figures, can be found at:
Supplementary Material
0/peds.2012-0177.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2012/10/3Supplementary
material can be found at:
References
html#ref-list-1http://pediatrics.aappublications.org/content/130/6/e1567.full.at:
This article cites 20 articles, 6 of which can be accessed
free
Subspecialty Collections
_diseasehttp://pediatrics.aappublications.org/cgi/collection/infectiousInfectious
Disease & Immunitythe following collection(s):This article,
along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables)
or in its entirety can be found online at:Information about
reproducing this article in parts (figures,
Reprints
http://pediatrics.aappublications.org/site/misc/reprints.xhtmlInformation
about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN:
1098-4275.Grove Village, Illinois, 60007. Copyright 2012 by the
American Academy of Pediatrics. Alland trademarked by the American
Academy of Pediatrics, 141 Northwest Point Boulevard,
Elkpublication, it has been published continuously since 1948.
PEDIATRICS is owned, published,PEDIATRICS is the official journal
of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on December 10,
2012pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/content/130/6/e1567.full.htmlhttp://pediatrics.aappublications.org/content/130/6/e1567.full.htmlhttp://pediatrics.aappublications.org/content/130/6/e1567.full.htmlhttp://pediatrics.aappublications.org/content/suppl/2012/10/30/peds.2012-0177.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2012/10/30/peds.2012-0177.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2012/10/30/peds.2012-0177.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/130/6/e1567.full.html#ref-list-1http://pediatrics.aappublications.org/content/130/6/e1567.full.html#ref-list-1http://pediatrics.aappublications.org/content/130/6/e1567.full.html#ref-list-1http://pediatrics.aappublications.org/cgi/collection/infectious_diseasehttp://pediatrics.aappublications.org/cgi/collection/infectious_diseasehttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/cgi/collection/infectious_diseasehttp://pediatrics.aappublications.org/content/130/6/e1567.full.html#ref-list-1http://pediatrics.aappublications.org/content/suppl/2012/10/30/peds.2012-0177.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/130/6/e1567.full.html