Embed Size (px)
Citation preview
Pediatric Grand Rounds 6/4/10
1
PEDIATRIC GRAND ROUNDS JUNE 4TH, 2010 PEDIATRIC ECMO: OLD DOG
OR NEW TRICK? Curt Froehlich, MD Pediatric ECMO Director
CHRISTUS Santa Rosa ECMO Program
Disclosures
• I have NO financial rela:onships with commercial interest to disclose
• I WILL be discussing off label use of FDA approved equipment
• I WILL BRIEFLY introduce equipment NOT FDA approved and will acknowledge when doing so
Learning ObjecNves
1. Describe the basics of ECMO, basic contraindica:ons to ECMO, and the theory behind which ECMO can be used to treat disease.
2. Describe briefly the early applica:ons of ECMO on neonatal and adult pa:ents and how these pa:ent popula:ons have changed throughout the years.
Learning ObjecNves
3. Describe the cost of ECMO as it compares to other therapies such as organ transplanta:on and bone marrow transplanta:on.
4. Describe briefly some of the future applica:ons of ECMO and its technologies including resuscita:on, transport, prematurity and organ transplanta:on and how these advances alter future pa:ent selec:on.
Diseases desperate grown By desperate appliance are relieved, Or not at all.
-‐Claudius, King of Denmark In Hamlet Act IV Scene 3 W. Shakespeare
Pediatric ECMO
Borrowed from Jim Fortenberry, MD. Children's Healthcare of Atlanta at Egleston
Desperate but Reasonable?
Borrowed from Jim Fortenberry, MD. Children's Healthcare of Atlanta at Egleston
Pediatric Grand Rounds 6/4/10
2
Pediatric ECMO Outline
• History • Basic Principles/Mechanics
• 3 Types of ECMO
– Respiratory ECMO
– Cardiac ECMO
– “Rescue” ECMO
Pediatric ECMO Outline
• Future evolu:on and applica:ons
• “Cost” of ECMO
• CSRCH ECMO program
• Success Story
What is ECMO? • Stands for: Extra-‐Corporeal Membrane Oxygena:on? • Should it stand for Extremely Costly Midnight Opera:on? • What is it? – A way in which the lungs or the heart and lungs can be ar:ficially supported for prolonged periods of :me
ECMO History • Technology is not “new” • Reports of first pa:ents supported in 1972
• First Study 1972 in Adults: – Lots of new centers performing ECMO
– Showed no benefit – ConvenNonal therapy beRer than Bad ECMO!
ECMO History • Bartled et al, Esperanza first neonatal case 1976
• Bartled et al 1982 45 newborns, 90% predicted mortality >50% survival
• O’Rourke 1989 randomized neonatal trial: Stopped early due to ECMO benefit
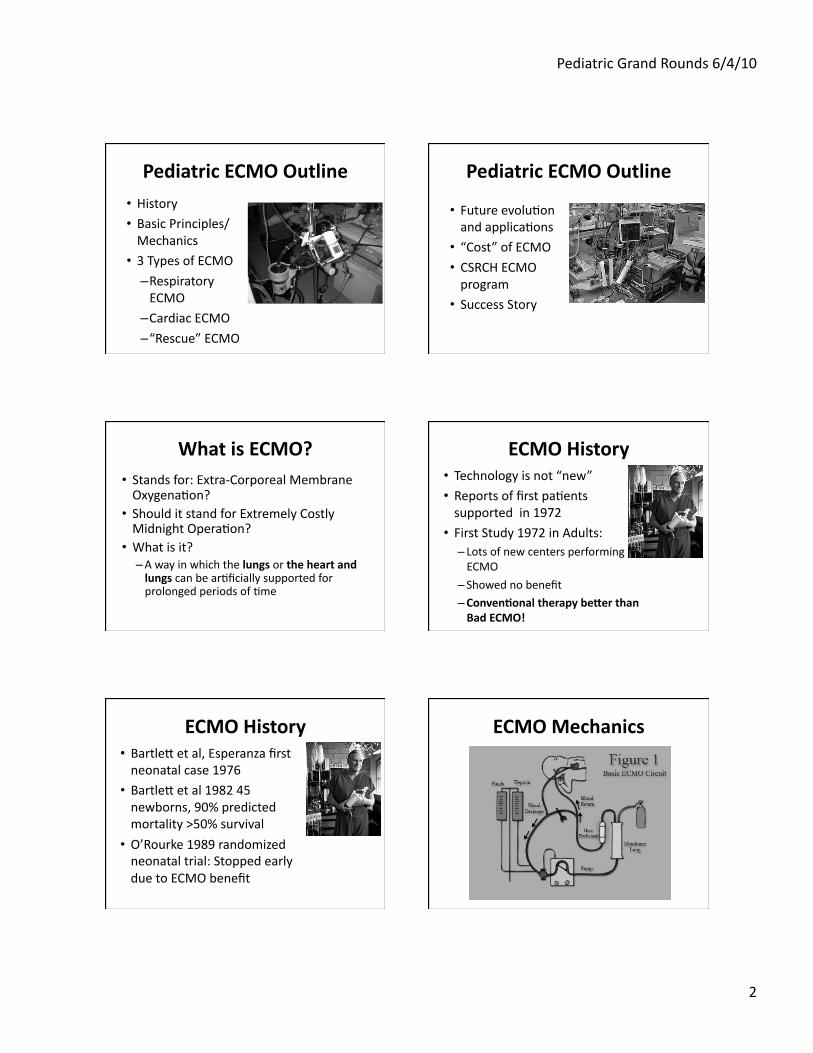
ECMO Mechanics
Pediatric Grand Rounds 6/4/10
3
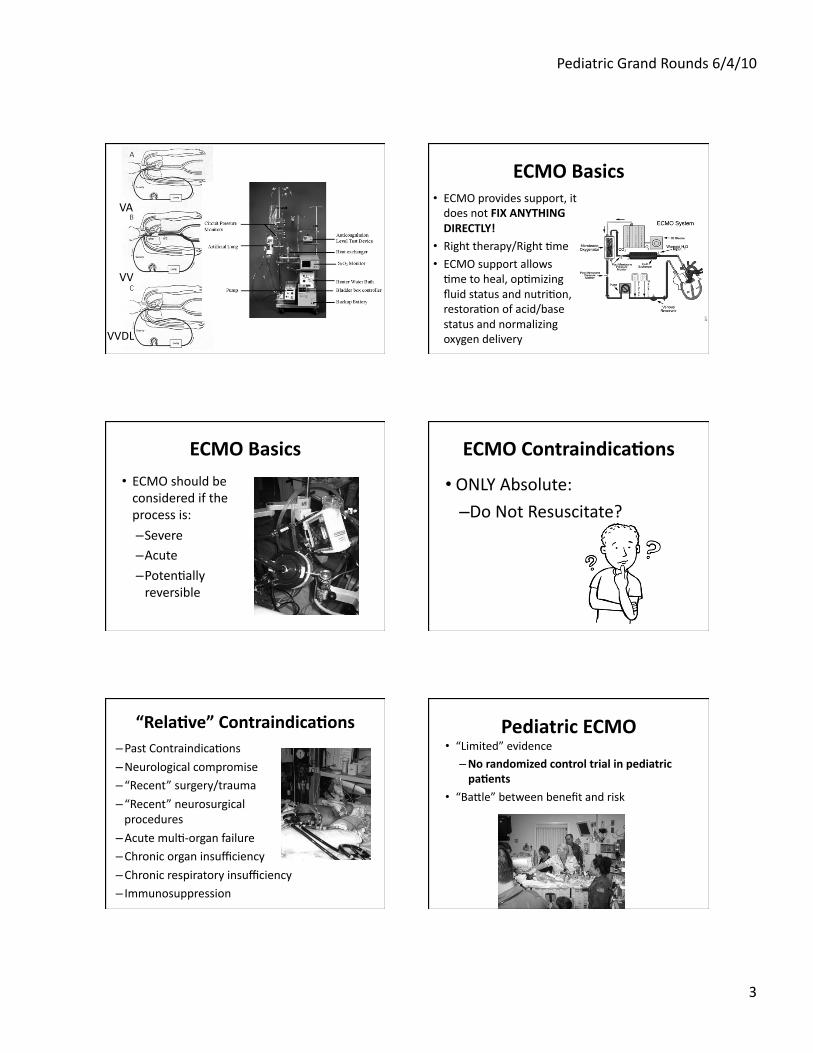
VA
VV
VVDL
ECMO Basics • ECMO provides support, it does not FIX ANYTHING DIRECTLY!
• Right therapy/Right :me
• ECMO support allows :me to heal, op:mizing fluid status and nutri:on, restora:on of acid/base status and normalizing oxygen delivery
ECMO Basics
• ECMO should be considered if the process is:
– Severe – Acute – Poten:ally reversible
ECMO ContraindicaNons
• ONLY Absolute: – Do Not Resuscitate?
“RelaNve” ContraindicaNons – Past Contraindica:ons – Neurological compromise – “Recent” surgery/trauma
– “Recent” neurosurgical procedures
– Acute mul:-‐organ failure – Chronic organ insufficiency
– Chronic respiratory insufficiency – Immunosuppression
Pediatric ECMO • “Limited” evidence – No randomized control trial in pediatric paNents
• “Badle” between benefit and risk
Pediatric Grand Rounds 6/4/10
4
All who drink of this treatment recover within a short :me, except in those
who do not.
Therefore, it fails only in incurable cases -‐Galen
Borrowed from Jim Fortenberry, MD. Children's Healthcare of Atlanta at Egleston
Problems In Study of ECMO
• Small popula:ons • Omen selec:ng the sickest pa:ents-‐nonresponders
• Loss of equipoise before demonstra:on of effect
• Difficul:es in RCTs-‐hard to randomize within a center
• “Can’t we use the machine?” Borrowed from Jim Fortenberry, MD. Children's Healthcare of Atlanta at Egleston
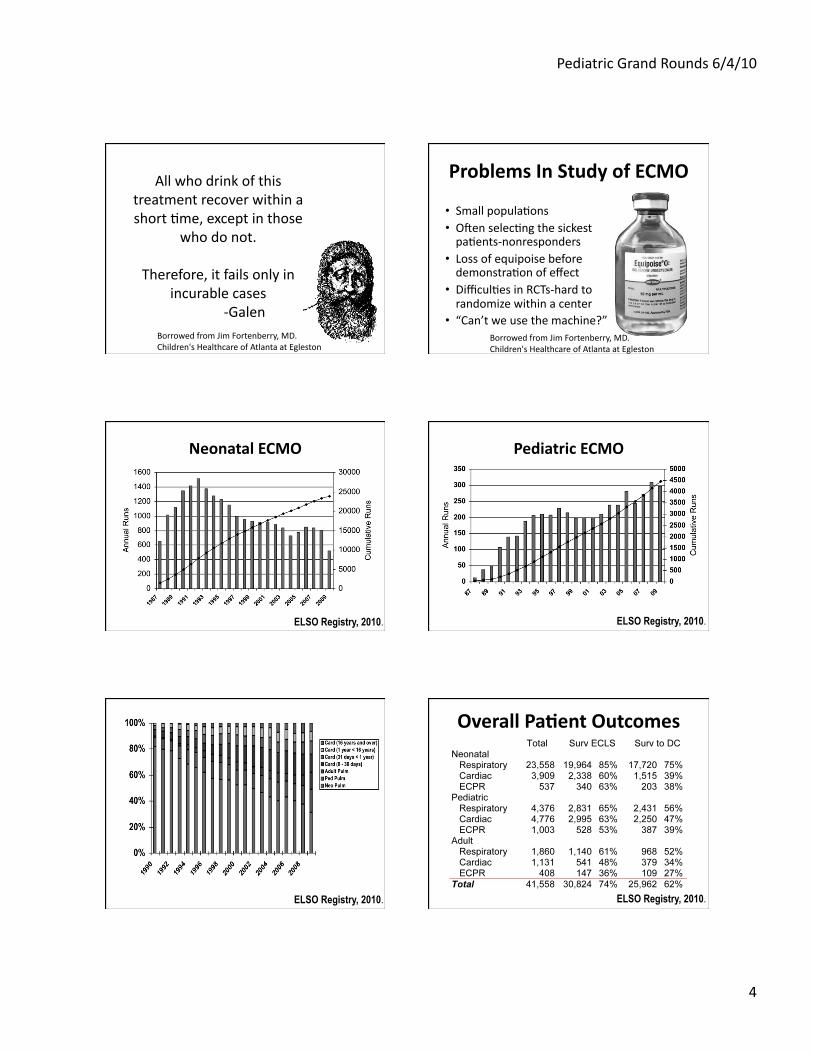
Neonatal ECMO
ELSO Registry, 2010.
Pediatric ECMO
ELSO Registry, 2010.
ELSO Registry, 2010.
Overall PaNent Outcomes
ELSO Registry, 2010.
Pediatric Grand Rounds 6/4/10
5
3 Types of ECMO
• Respiratory ECMO
• Cardiac ECMO
• “Rescue” ECMO
Pediatric Respiratory ECMO
• Remember: – Acute – Severe – Poten:ally reversible
• All mechanical ven:la:on causes acute lung injury (pressure, volume, jet, APRV, HFOV)
– Earlier is beRer! (before irreversible lung injury)
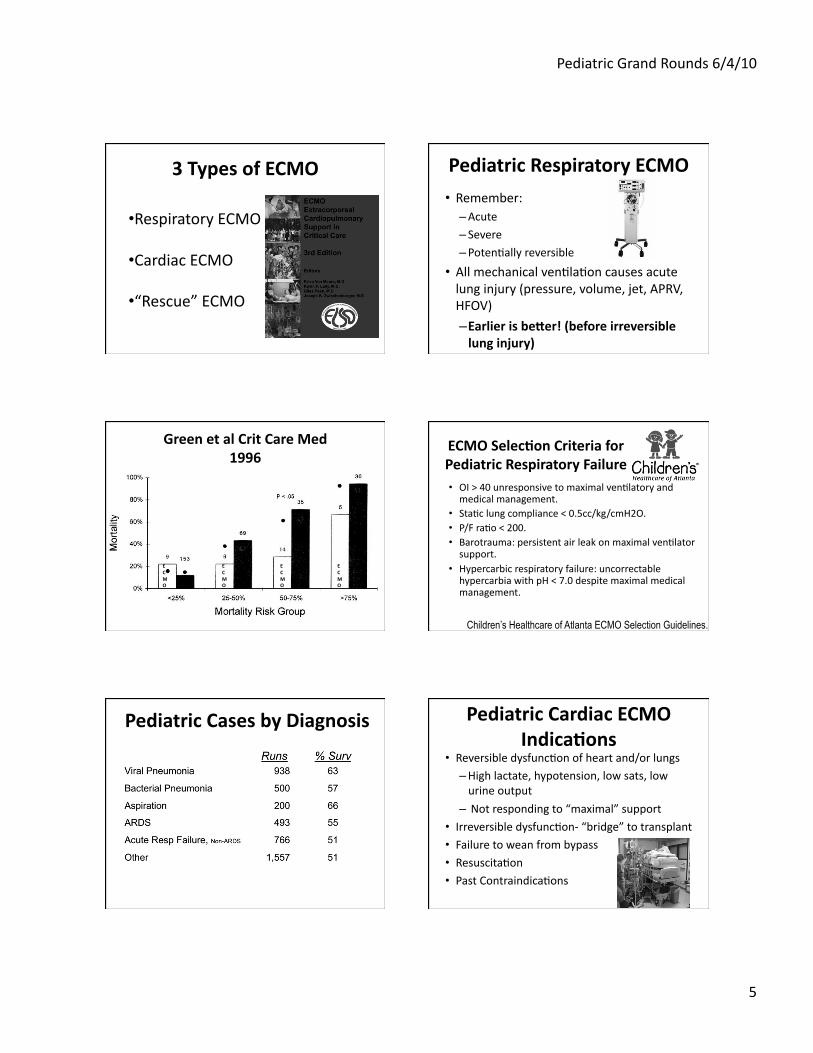
Green et al Crit Care Med 1996
ECMO
ECMO
ECMO
ECMO
ECMO SelecNon Criteria for Pediatric Respiratory Failure • OI > 40 unresponsive to maximal ven:latory and medical management.
• Sta:c lung compliance < 0.5cc/kg/cmH2O. • P/F ra:o < 200. • Barotrauma: persistent air leak on maximal ven:lator support.
• Hypercarbic respiratory failure: uncorrectable hypercarbia with pH < 7.0 despite maximal medical management.
Children’s Healthcare of Atlanta ECMO Selection Guidelines.
Pediatric Cases by Diagnosis Pediatric Cardiac ECMO IndicaNons
• Reversible dysfunc:on of heart and/or lungs – High lactate, hypotension, low sats, low urine output
– Not responding to “maximal” support
• Irreversible dysfunc:on-‐ “bridge” to transplant • Failure to wean from bypass
• Resuscita:on • Past Contraindica:ons
Pediatric Grand Rounds 6/4/10
6
Cardiac ECLS by Diagnosis Under 16 years
Cardiomyopathy/MyocardiNs • 2 categories of non-‐surgical cardiac failure increasingly supported by ECLS
• Review of 15 pediatric viral myocardi:s – Overall survival was 80% – 60% recovered func:on to be weaned off with normal follow up func:on – Recovery for non-‐surgical paNent may occur aber prolonged cardiac support! – Median duraNon of cardiomyopathy support was 140 hrs!
Duncan et al. J Thorac Cardiovasc Surg 2001;122:440–8.
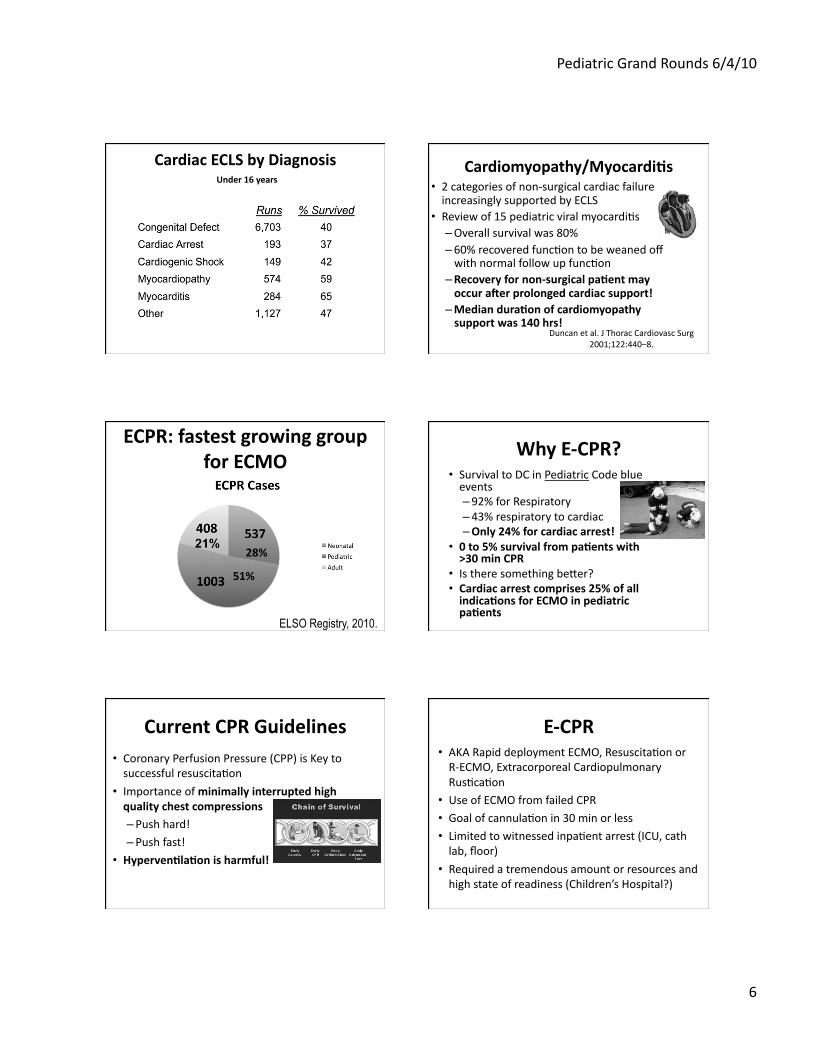
ECPR: fastest growing group for ECMO
ELSO Registry, 2010.
51%
28%
Why E-‐CPR? • Survival to DC in Pediatric Code blue events – 92% for Respiratory – 43% respiratory to cardiac – Only 24% for cardiac arrest!
• 0 to 5% survival from paNents with >30 min CPR
• Is there something beder? • Cardiac arrest comprises 25% of all indicaNons for ECMO in pediatric paNents
Current CPR Guidelines • Coronary Perfusion Pressure (CPP) is Key to successful resuscita:on
• Importance of minimally interrupted high quality chest compressions – Push hard! – Push fast!
• HypervenNlaNon is harmful!
E-‐CPR • AKA Rapid deployment ECMO, Resuscita:on or R-‐ECMO, Extracorporeal Cardiopulmonary Rus:ca:on
• Use of ECMO from failed CPR
• Goal of cannula:on in 30 min or less
• Limited to witnessed inpa:ent arrest (ICU, cath lab, floor)
• Required a tremendous amount or resources and high state of readiness (Children’s Hospital?)
Pediatric Grand Rounds 6/4/10
7
E-‐CPR • Surgical availability – Level I trauma center?
• Pre-‐primed circuit
– ECMO specialist able to prime 24 hrs/day on site
• Blood bank • ICU physician, nursing staff • Early ECMO considera:on and ini:a:on
– <5 min into CPR
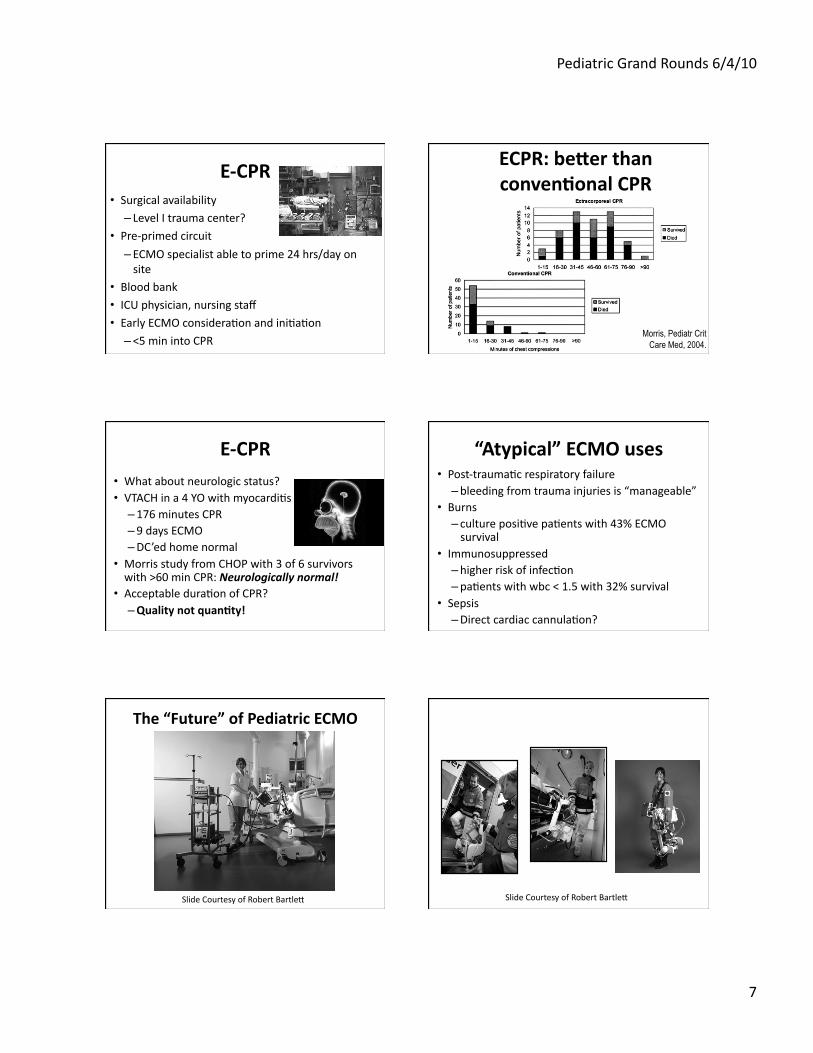
ECPR: beRer than convenNonal CPR
Morris, Pediatr Crit Care Med, 2004.
E-‐CPR • What about neurologic status? • VTACH in a 4 YO with myocardi:s – 176 minutes CPR – 9 days ECMO – DC’ed home normal
• Morris study from CHOP with 3 of 6 survivors with >60 min CPR: Neurologically normal!
• Acceptable dura:on of CPR? – Quality not quanNty!
“Atypical” ECMO uses • Post-‐trauma:c respiratory failure – bleeding from trauma injuries is “manageable”
• Burns – culture posi:ve pa:ents with 43% ECMO survival
• Immunosuppressed – higher risk of infec:on – pa:ents with wbc < 1.5 with 32% survival
• Sepsis – Direct cardiac cannula:on?
The “Future” of Pediatric ECMO
Slide Courtesy of Robert Bartled Slide Courtesy of Robert Bartled
Pediatric Grand Rounds 6/4/10
8
Ambulatory Lung Assist with PA-‐LA implantaNon
5 weeks, bridging to transplant Regensberg, 2007
AALA bridge to XP: Hoopes, 2009
ECLS Research: ArNficial Placenta
Slide Courtesy of Robert Bartled
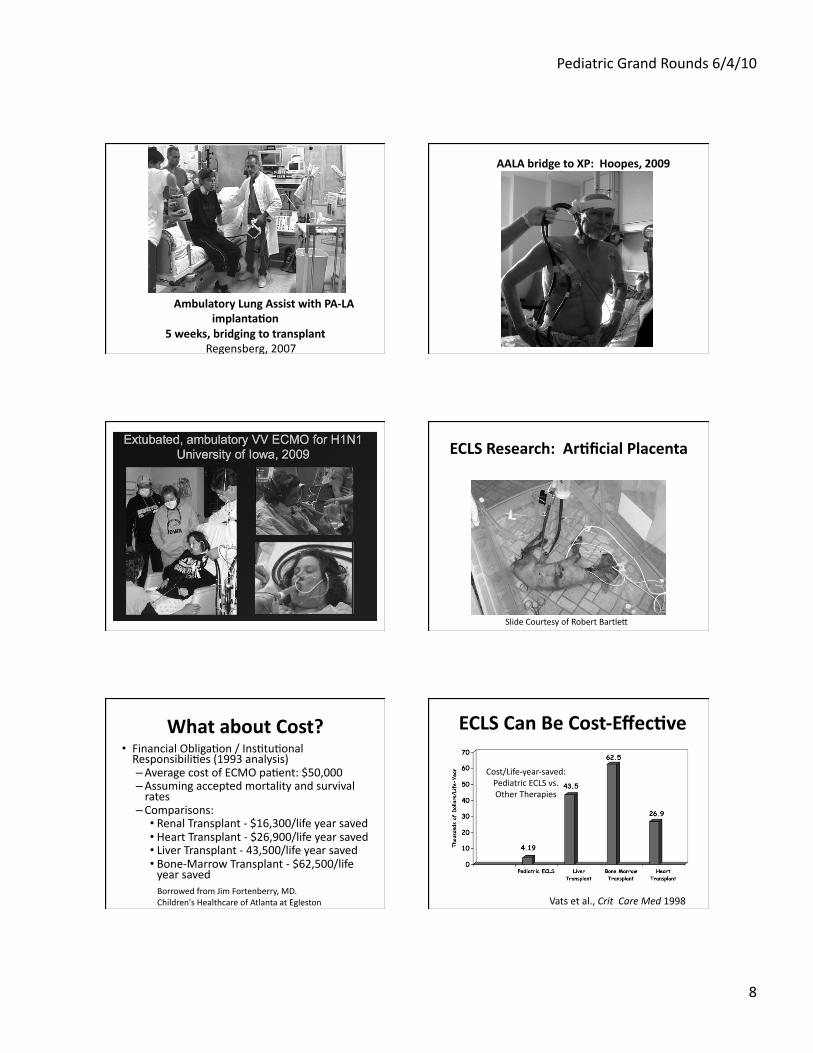
What about Cost? • Financial Obliga:on / Ins:tu:onal Responsibili:es (1993 analysis) – Average cost of ECMO pa:ent: $50,000 – Assuming accepted mortality and survival rates – Comparisons: • Renal Transplant -‐ $16,300/life year saved • Heart Transplant -‐ $26,900/life year saved • Liver Transplant -‐ 43,500/life year saved • Bone-‐Marrow Transplant -‐ $62,500/life year saved Borrowed from Jim Fortenberry, MD. Children's Healthcare of Atlanta at Egleston
ECLS Can Be Cost-‐EffecNve
Vats et al., Crit Care Med 1998
Cost/Life-‐year-‐saved: Pediatric ECLS vs. Other Therapies
Pediatric Grand Rounds 6/4/10
9
CHRISTUS Santa Rosa ECMO Program
• Neonatal Program began in 1989 – >100 pts
• In 2008 began a comprehensive pediatric program in conjunc:on with Wilford Hall
• Last year CSRCH supported 18 ECMO pa:ents
• >100 ECMO days in the pediatric ICU last year
• Program con:nues to grow
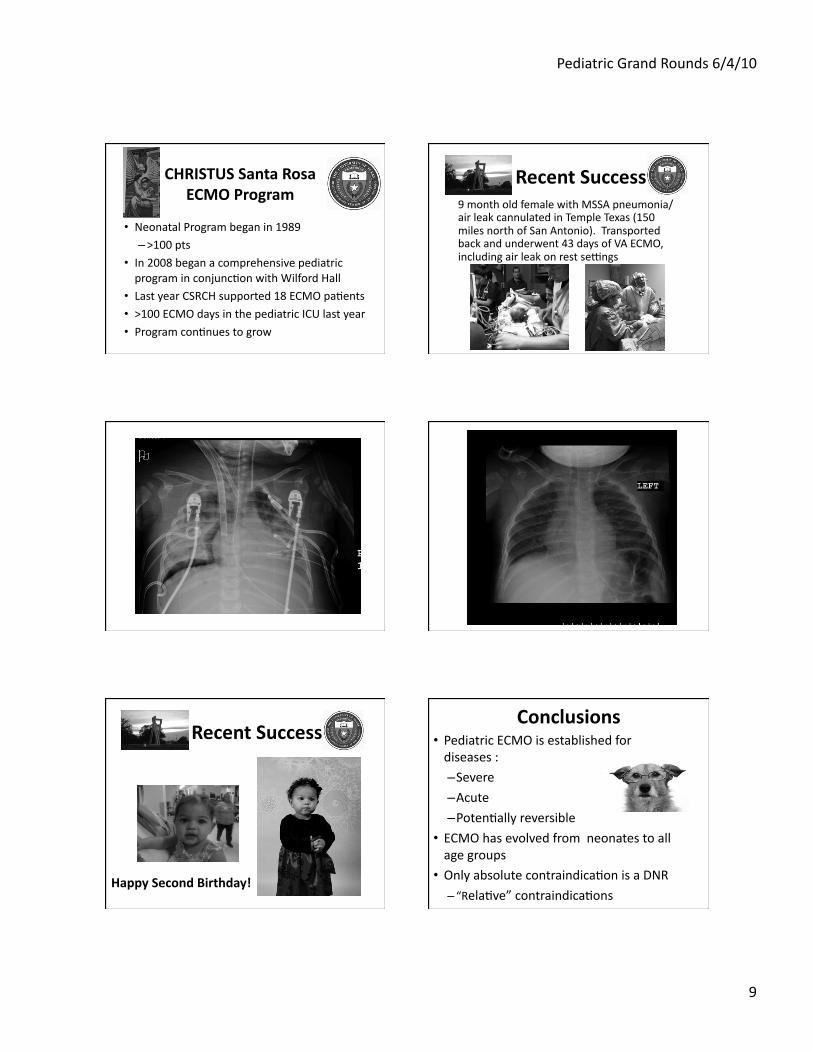
Recent Success 9 month old female with MSSA pneumonia/air leak cannulated in Temple Texas (150 miles north of San Antonio). Transported back and underwent 43 days of VA ECMO, including air leak on rest sewngs
Recent Success
Happy Second Birthday!
Conclusions • Pediatric ECMO is established for diseases :
– Severe – Acute – Poten:ally reversible
• ECMO has evolved from neonates to all age groups
• Only absolute contraindica:on is a DNR – “Rela:ve” contraindica:ons
Pediatric Grand Rounds 6/4/10
10
Conclusions • ECMO can be cost effec:ve
• ECMO, ECMO equipment and applica:ons of ECMO con:nue to evolve
– Resuscita:on – Transport – “Bridge” to transplant – Prematurity
Plenty of new tricks!
Hopefully I have not led you astray…
Borrowed from Jim Fortenberry, MD. Children's Healthcare of Atlanta at Egleston
But remember! With great thanks… • En:re ECMO team… – Coordinators – Primers
– Specialists • CSRCH Neonatal Team
• UTHSCSA Perfusion Group
• Wilford Hall ECMO Program
• Jim Fortenberry
• Robert Bartled
With great thanks… QuesNons?





![[PPT]PCRRT in ECMO - Pediatric Continuous Renal … in ECMO.pptx · Web viewPCRRT in ECMO Indications/Role of CRRT in ECMO: Decrease fluid overload Management of fluid balance to](https://img.pdfslide.us/doc/110x75/5aef89b27f8b9a572b8e4544/pptpcrrt-in-ecmo-pediatric-continuous-renal-in-ecmopptxweb-viewpcrrt-in.jpg)