Embed Size (px)
Citation preview
Pediatric VoiceUseful References
LSHSS issues dedicated to voice disorders
July 1996
October 2004
Pediatric voice disorders Brief survey of congenital problems Anatomical differences in children Occurrence of voice disorders in children Therapy considerations
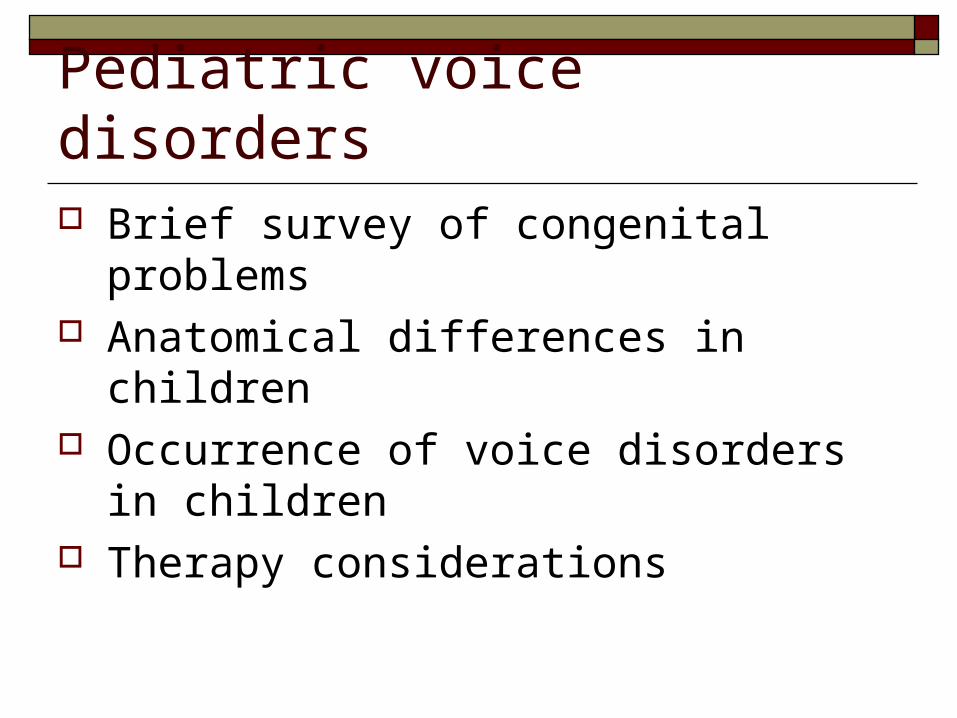
Laryngomalacia Soft larynx Collapse of laryngeal
structures during breathing
Partial airway obstruction
Stridor Often resolves w/o
intervention
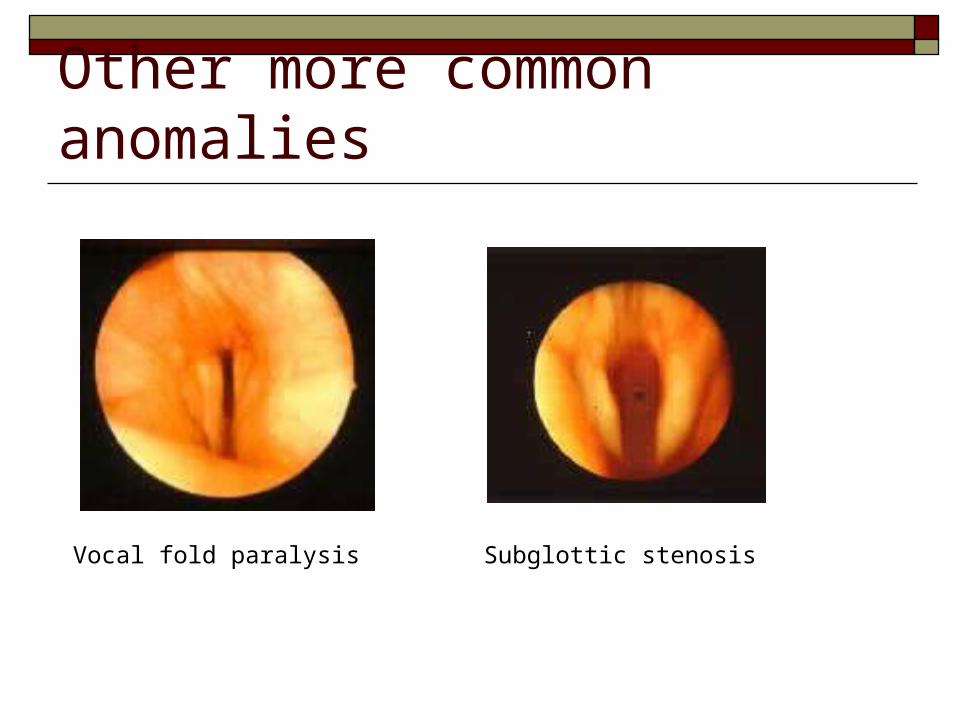
Other more common anomalies
Vocal fold paralysis Subglottic stenosis

Congenital Laryngeal Web
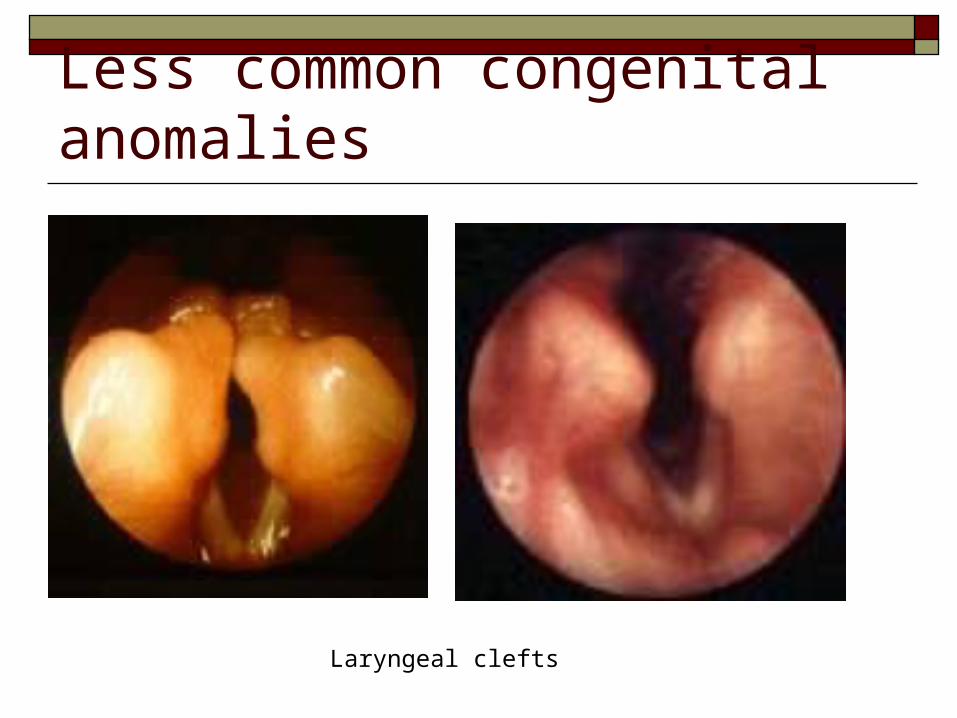
Less common congenital anomalies
Laryngeal clefts
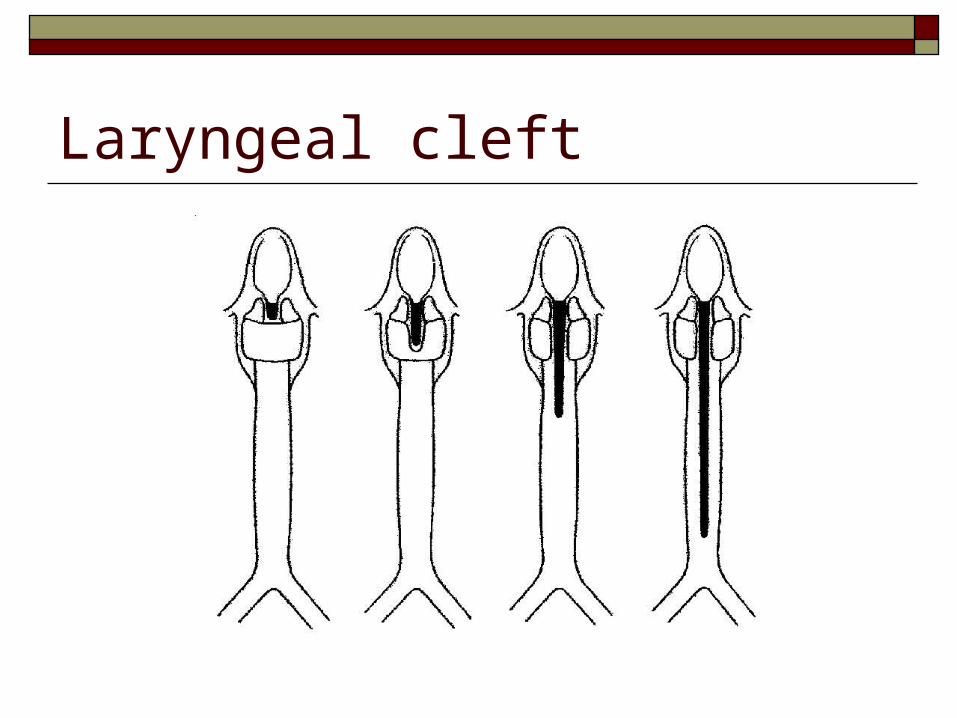
Laryngeal cleft
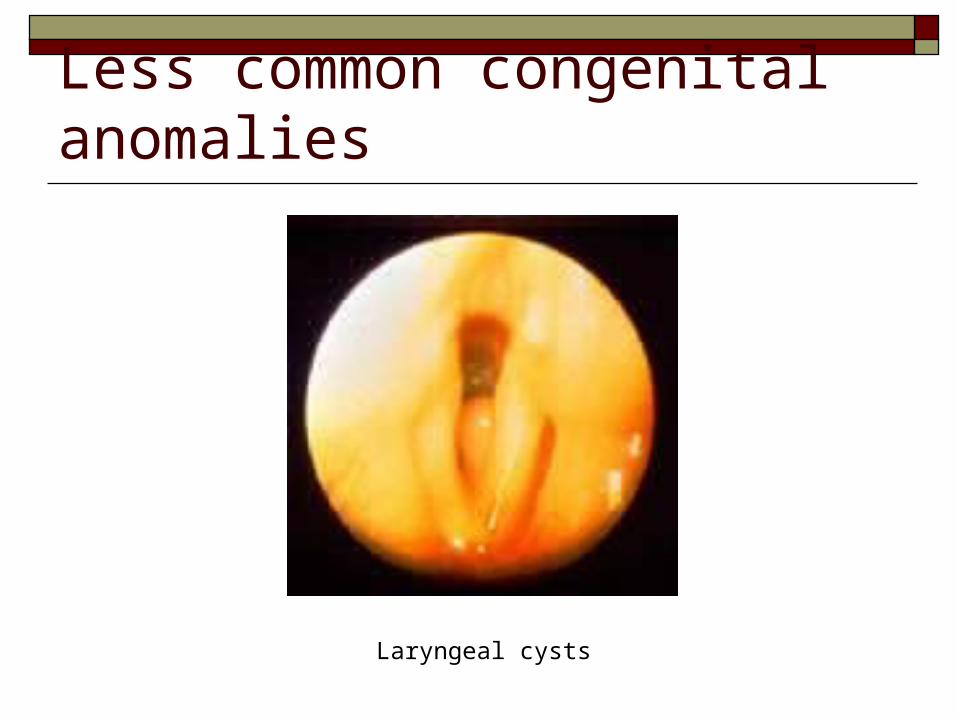
Less common congenital anomalies
Laryngeal cysts

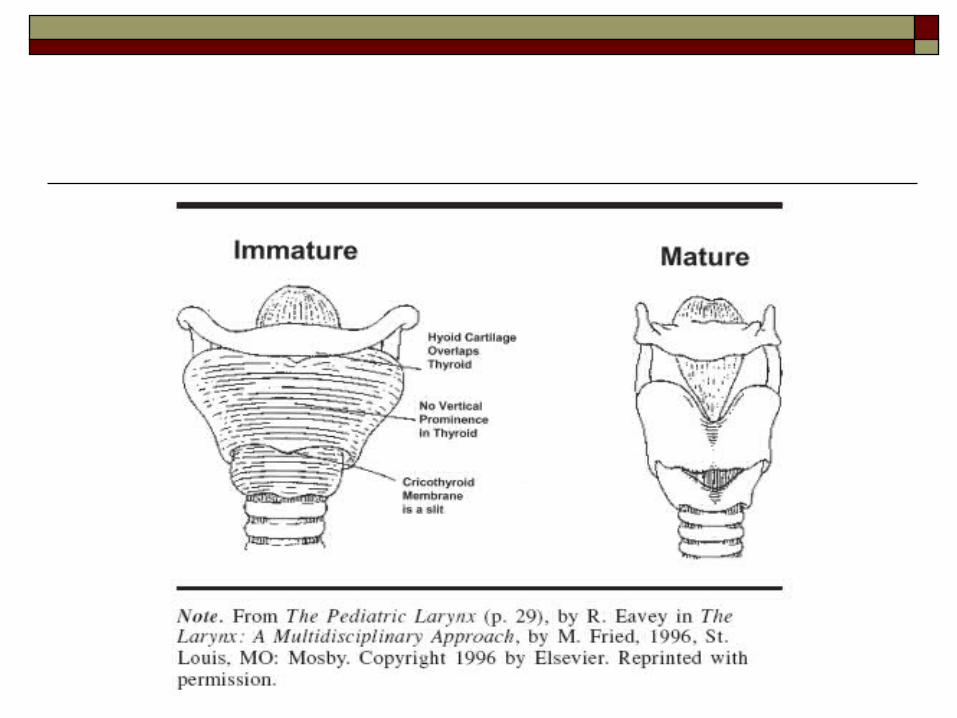
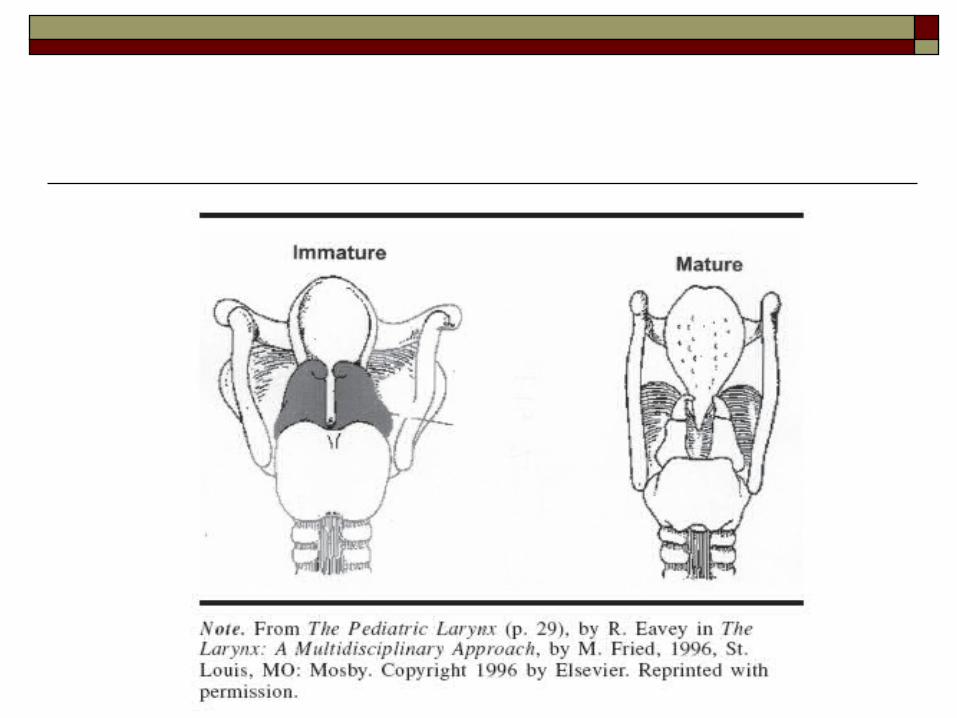
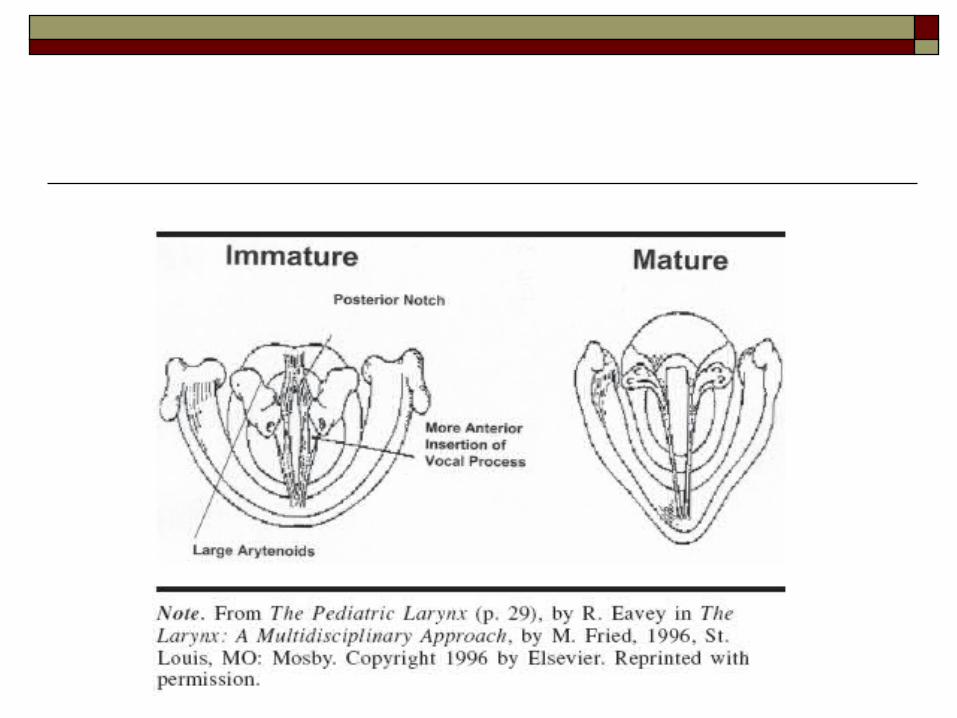
Pediatric larynx: Anatomical differences
Size Newborn 2.5-3.0 mm Adult female: 11-15 mm Adult male: 17-21 mm
Shorter membranous portion of vocal fold Lack of full layered structure Location in neck

Occurrence of voice disorders in children Occurrence data ranges from 6-23% of school
age children Adolescents may exceed general occurrence
estimates Good epidemiological studies clearly
stratified by age/group needs to be done
Types of voice problems typically reported in children
“Functional” voice problems Misuse/abuse related Presence of vocal nodules
Reflux related voice problems Paradoxical vocal fold motion Unidentified congenital problems
Do children get voice services in schools? Voice problems constitute 2-4 % of school
SLP caseload Only about 1-4 % of dysphonic children
receive Tx (McNamara & Perry, 1994; Clark, 2003)
SLPs with larger caseloads more likely to provide voice services
Why are school SLPs reluctant to take voice disordered students onto caseloads?
Perceived lack of severity or priority of problem
Lack of experience Difficulty getting a laryngoscopic evaluation Concern about meeting service requirements
– see Ruddy and Sapienza (2004) for discussion
Hooper (2004)
As with adults, accurate diagnosis is critical for
appropriate decision making
Approaches to Treatment Prevention Therapy
Indirect Direct
“Children” are a large and varied group Preschoolers School age children (pre-adolescent) Adolescents
Role of Prevention 59 %* of school SLPs believe prevention is
an efficient way to deliver voice treatment 19 %* of schools SLPs perform such
practices
Prevention can be incorporated into the regular academic curriculum talk to the science/health teacher
*McNamara and Perry (1994)
Therapy Considerations Underlying treatment rationale for adults also
applies to children However, implementing the strategies need to
be tailored to the child Awareness and education are very important

Therapy Considerations Computer-based speech & voice programs are
quite appealing to children Many real-time feedback programs are freely
available for clinicians to download Good link to investigate
http://www.phon.ucl.ac.uk/resource/software.php
Therapy “phases” particularly important for children General awareness of vocal behaviors Specific awareness of behaviors to change Direct voice therapy or voice production
activities Generalization and carryover activities
(Andrews & Summers, 2002)
Therapy Considerations
“… These include the following:• parent/family involvement• teacher involvement in the school-age child• a component of child/family lifestyle education or vocal hygiene education• psychodynamic and interpersonal factors and related behavioral intervention or discussion• the incorporation of vocal behavior into good language and communication behavior• the use of age-appropriate activities if direct voice therapy is recommended” (Cooper, 2004)

Is voice therapy for children efficacious? Limited outcomes research Studies that suggest treatment effects lack
strong controls (e.g. Mori (1999))
Puberphonia What is it? Identification What can be done about it?