Embed Size (px)
Citation preview

Pediatric TumorsPediatric Tumors
Pamela Simon R.N., C.P.N.P, Pamela Simon R.N., C.P.N.P, MSNMSN
Lucile Packard Children’s HospitalLucile Packard Children’s Hospital

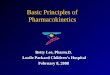
Distribution of Childhood CancerDistribution of Childhood Cancer
CNS18%
Liver1%
Other8%
Leukemia33%Retina
3%Germ Cell3%
Bone5%
Wilm's Tumor
6%
Hodgkin's5% NHL
3%
NBL8%
Soft Tissue Sarcoma
7%

Abdominal massesAbdominal masses
HistoryHistory SymptomsSymptoms
– abdominal discomfort, increased abdominal abdominal discomfort, increased abdominal size or assymptomaticsize or assymptomatic
– Presence of systemic symptomsPresence of systemic symptoms bone pain, limping, malaise, feverbone pain, limping, malaise, fever
– Other symptomsOther symptoms hematuriahematuria

Abdominal massesAbdominal masses
Physical findingsPhysical findings Presence of abdominal massPresence of abdominal mass
– upper abdomen or lower abdomenupper abdomen or lower abdomen
Other associated physical findingsOther associated physical findings– other masses: orbitalother masses: orbital– bruisesbruises– hypertensionhypertension– painpain

Abdominal MassAbdominal Mass
Differential diagnosis Differential diagnosis depends on locationdepends on location
Upper abdominal Upper abdominal massmass– NeuroblastomaNeuroblastoma– Wilm’s tumorWilm’s tumor– HepatoblastomaHepatoblastoma– RhabdomyosarcomaRhabdomyosarcoma– Germ cell tumorGerm cell tumor– LymphomaLymphoma

Abdominal MassAbdominal Mass
Differential diagnosis Differential diagnosis (cont)(cont)
Lower Lower abdominal/pelvic abdominal/pelvic massmass– NeuroblastomaNeuroblastoma– RhabdomyosarcomaRhabdomyosarcoma– Germ cell tumorGerm cell tumor– LymphomaLymphoma– Ewing’s sarcomaEwing’s sarcoma

Abdominal MassesAbdominal MassesLaboratory evaluationLaboratory evaluation Bone marrow aspirateBone marrow aspirate
– neuroblastoma, lymphoma, neuroblastoma, lymphoma, rhabdomyosarcoma or rhabdomyosarcoma or Ewing’s sarcoma Ewing’s sarcoma
CSF tapCSF tap– if lymphoma is a if lymphoma is a
considerationconsideration

Abdominal massesAbdominal massesRadiologic work-upRadiologic work-up Abdominal/pelvic ultrasoundAbdominal/pelvic ultrasound
– useful screening test: helps define location and useful screening test: helps define location and quality (solid or cystic)quality (solid or cystic)
– not useful to assess for retroperitoneal adenopathynot useful to assess for retroperitoneal adenopathy
Computed tomographyComputed tomography – location of masslocation of mass– presence of calcificationpresence of calcification– obstructive signs obstructive signs

Wilm’s TumorWilm’s Tumor
Accounts for 6% childhood malignanciesAccounts for 6% childhood malignancies Median age at diagnosis 3 yearsMedian age at diagnosis 3 years Metastasizes to lung and lymph nodesMetastasizes to lung and lymph nodes
– 70% patients present with localized disease70% patients present with localized disease

Wilm’s Tumor: Signs & SymptomsWilm’s Tumor: Signs & Symptoms
Most commonly Most commonly presents as painless presents as painless abdominal massabdominal mass
Hypertension (20-30%)Hypertension (20-30%) Pain (20-30%)Pain (20-30%) Hematuria (25%)Hematuria (25%)

Wilm’s Tumor: Staging SystemWilm’s Tumor: Staging System
StageStage DefinitionDefinition
II Tumor limited to kidney, completely excisedTumor limited to kidney, completely excised
IIII Tumor extends beyond the kidney, completely resected; Tumor extends beyond the kidney, completely resected; no residual tumor beyond resection marginsno residual tumor beyond resection margins
IIIIII Residual non-hematogenous tumor confined to abdomenResidual non-hematogenous tumor confined to abdomen
IVIV Hematogenous metastasesHematogenous metastases
VV Bilateral renal involvementBilateral renal involvement

Bilateral Wilm’sBilateral Wilm’s

Survival by Stage and HistologySurvival by Stage and Histology
Histology/stage # pts 2 yr-s* 4 yr-s*
FH/I 546 98 97
II 281 96 94
III 290 91 88
IV 126 88 82
UH/I 20 89 89
UH/II-IV 40 56 54* survival

Wilms Tumor: Prognosis & Future DirectionsWilms Tumor: Prognosis & Future Directions
Prognostic factors: stage and histologyPrognostic factors: stage and histology Future directionsFuture directions
– Minimize therapy for favorable histology Minimize therapy for favorable histology patientspatients
– Identify biologic factors predictive of outcomeIdentify biologic factors predictive of outcome– Intensify therapy for patients with unfavorable Intensify therapy for patients with unfavorable
histologyhistology

Osteosarcoma: DistributionOsteosarcoma: Distribution by Age and Site by Age and Site

Clinical presentationClinical presentation Pain and swelling usually lasting 3-4 Pain and swelling usually lasting 3-4
months months – Duration: sometimes > 6 monthsDuration: sometimes > 6 months
Occurs around metaphysis of long Occurs around metaphysis of long bonesbones– Most common primary sites: distal femur, Most common primary sites: distal femur,
proximal tibia and proximal humerusproximal tibia and proximal humerus– 50-70% around the knee joint50-70% around the knee joint
Metastases: ~15-20% patientsMetastases: ~15-20% patients– Sites: lung and other bonesSites: lung and other bones

Most Common Metastatic SitesMost Common Metastatic Sites

Diagnostic workupDiagnostic workup
Imaging Work-up: Plain Imaging Work-up: Plain X ray, MRI of primaryX ray, MRI of primary
Metastatic workupMetastatic workup– Chest CT Chest CT – Bone scanBone scan– PET scanPET scan
BiopsyBiopsy

Imaging Evaluation Imaging Evaluation

Metastatic Work-Up: Chest X-RayMetastatic Work-Up: Chest X-Ray

Metastatic Work-Up: Chest CTMetastatic Work-Up: Chest CT

Metastatic Work-Up: Bone ScanMetastatic Work-Up: Bone Scan

PathologyPathology
Intramedullary high-grade Intramedullary high-grade sarcoma sarcoma – Malignant mesenchymal Malignant mesenchymal
cells producing osteoid cells producing osteoid
The World Health The World Health Organization (WHO) Organization (WHO) recognizes three major recognizes three major subtypes: based on subtypes: based on matrix: matrix: – OsteoblasticOsteoblastic– ChondroblasticChondroblastic– fibroblasticfibroblastic

Osteosarcoma: PathologyOsteosarcoma: Pathology

Osteosarcoma: TherapyOsteosarcoma: Therapy
Historically, 2-year Historically, 2-year survival < 20% for survival < 20% for patients treated with patients treated with surgery and/or surgery and/or radiotherapyradiotherapy
Uncontrolled trials of Uncontrolled trials of adjuvant chemotherapy adjuvant chemotherapy resulted in EFS of 45-resulted in EFS of 45-60% suggesting 60% suggesting chemotherapy improved chemotherapy improved outcomeoutcome

Multi-Institutional Osteosarcoma Multi-Institutional Osteosarcoma Study:Study: Design Design
BIOPSY
SURGERY
RANDOMIZE
Adjuvant Chemotherapy
No Adjuvant Chemotherapy

Osteosarcoma: TreatmentOsteosarcoma: Treatment
Current therapy: multi-Current therapy: multi-agent chemotherapy agent chemotherapy usually including usually including cisplatin, doxorubicin cisplatin, doxorubicin and methotrexate.and methotrexate.
Complete surgical Complete surgical resection for local resection for local control.control.

Osteosarcoma TreatmentOsteosarcoma Treatment
Types of surgical techniquesTypes of surgical techniques
– AmputationAmputation– RotationplastyRotationplasty– ““growing’ prosthesisgrowing’ prosthesis– Total knee titanium replacementTotal knee titanium replacement

AmputationAmputation

RotationplastyRotationplasty

RotationplastyRotationplasty

Total knee titanium Total knee titanium replacementreplacement
(endoprosthesis)(endoprosthesis)

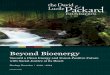
Prognostic Factors: MetastasesPrognostic Factors: Metastases

20
40
60
80
100
1 2 3 4 5
pre-chemo
SURVIVAL OF PATIENTS WITH LOCALIZED OSTEOSARCOMA
years
1980’s- combination chemo
1960’s – single agentchemo
2004 - chemo regimensmultiple intensified
% s
urv
ival

Osteosarcoma: Outcome Modern Osteosarcoma: Outcome Modern TrialsTrials

Osteosarcoma: OutcomeOsteosarcoma: Outcome
Reached a plateau in outcome for Reached a plateau in outcome for osteosarcoma patientsosteosarcoma patients– Further improvement will require large Further improvement will require large
cooperative studies: International collaborationcooperative studies: International collaboration– EURAMOS: EURAMOS:
North American Children’s Oncology Group (COG) North American Children’s Oncology Group (COG) German Austrian Swiss Cooperative German Austrian Swiss Cooperative
Osteosarcoma Study Group (COSS)Osteosarcoma Study Group (COSS) European Osteosarcoma Intergroup (EOI) European Osteosarcoma Intergroup (EOI) Scandinavian Sarcoma Group (SSG) Scandinavian Sarcoma Group (SSG)

Osteosarcoma: ConclusionsOsteosarcoma: Conclusions
We have made significant progress in the We have made significant progress in the treatment of osteosarcomatreatment of osteosarcoma
Therapy has reached a plateau and further Therapy has reached a plateau and further improvements will require large number of improvements will require large number of patientspatients– International collaboration: significant barriers International collaboration: significant barriers
but offers the best chance of increasing the but offers the best chance of increasing the number of patients availablenumber of patients available
– Biologic studies: essential for continued Biologic studies: essential for continued progressprogress

CNS TUMORSCNS TUMORS

CNS TUMORSCNS TUMORS
Most common solid tumors in childrenMost common solid tumors in children 22ndnd most frequent (16.6% of all childhood most frequent (16.6% of all childhood
malignancies)malignancies) Incidence has increased over the past 2 Incidence has increased over the past 2
decades decades Males > females, white> African AmericanMales > females, white> African American

CNS TUMORSCNS TUMORS
Signs & SymptomsSigns & Symptoms (related to the location, histologic grade of (related to the location, histologic grade of
tumor & age of child)tumor & age of child)GeneralGeneral-Headache-Headache-Seizures-Seizures-Mental status changes-Mental status changes-Increased intracranial Pressure (ICP)-Increased intracranial Pressure (ICP)

CNS TUMORSCNS TUMORS
Signs & Symptoms-Posterior FossaSigns & Symptoms-Posterior Fossa-Cerebellum--Cerebellum-
-nausea, vomiting, headache, papilledema, -nausea, vomiting, headache, papilledema, clumsy walk, double vision, dizzynessclumsy walk, double vision, dizzyness
-Brainstem--Brainstem- -vomiting, cranial nerve palsies, headache, -vomiting, cranial nerve palsies, headache,
head tilt, personality changes, hearing losshead tilt, personality changes, hearing loss

CNS TUMORSCNS TUMORS
S&S-Cerebral HemisphereS&S-Cerebral Hemisphere– Frontal lobe-one-sided paralysis, memory loss, Frontal lobe-one-sided paralysis, memory loss,
mental changes, urinary changesmental changes, urinary changes– Occipital lobe-visual changes, seizuresOccipital lobe-visual changes, seizures– Parietal lobe-Language disturbances, seizures, Parietal lobe-Language disturbances, seizures,
loss of reading, math loss of reading, math – Temporal lobe-seizures, unable to recognize Temporal lobe-seizures, unable to recognize
sounds, visual impairments sounds, visual impairments

CNS TUMORSCNS TUMORS
S&S-Midline TumorsS&S-Midline Tumors– Headache, nausea/vomiting, papilledema, Headache, nausea/vomiting, papilledema,
visual loss or abnormal eye movements, visual loss or abnormal eye movements, precocious puberty, diabetes insipidusprecocious puberty, diabetes insipidus
(impairment of hypothalmic/pituitary fx)(impairment of hypothalmic/pituitary fx)

CNS TUMORSCNS TUMORS
S&S- Spinal Cord-depends on locationS&S- Spinal Cord-depends on location– Thoracic-chest painThoracic-chest pain– Cervical or lumbar-neck, arm, back, leg Cervical or lumbar-neck, arm, back, leg
weakness, muscle spasms & wasting, altered weakness, muscle spasms & wasting, altered bowel, bladder functionbowel, bladder function
– Progression of symptoms can result in paralysisProgression of symptoms can result in paralysis

CNS TUMORSCNS TUMORS
Age & developmental stage are important factors Age & developmental stage are important factors in re: to symptomsin re: to symptoms
-infants-delay or loss of dev. Milestones-infants-delay or loss of dev. Milestones
-school age-personality changes, decline in -school age-personality changes, decline in school performance, change in handwritingschool performance, change in handwriting

CNS TUMORSCNS TUMORS
Diagnostic EvaluationDiagnostic Evaluation– MRI head-preferredMRI head-preferred
Add spine if requiredAdd spine if required
– CT headCT head– Lumbar punctureLumbar puncture– Lab work for “tumor markers” for germ cell Lab work for “tumor markers” for germ cell
tumors-AFP & B-hCGtumors-AFP & B-hCG– Pet Scan Pet Scan

CNS TUMORSCNS TUMORS
TREATMENTTREATMENT– SurgerySurgery
Most extensive resection feasibleMost extensive resection feasible
--Radiation Therapy--Radiation Therapy
--Chemotherapy--Chemotherapy

CNS TUMORSCNS TUMORS
PrognosisPrognosis– Varies greatly depending on type of tumor, Varies greatly depending on type of tumor,
resectability, resectability,

CNS TUMORSCNS TUMORS
AstrocytomaAstrocytoma– Occur at any age & various areas of brainOccur at any age & various areas of brain– Graded according to anaplasiaGraded according to anaplasia– Low grade cerebellar-pilocytic-85-95 % 5 year Low grade cerebellar-pilocytic-85-95 % 5 year
survival ratesurvival rate– Low grade cerebral-90% 5 year survival rateLow grade cerebral-90% 5 year survival rate– -High grade astrocytoma-29% for anaplastic -High grade astrocytoma-29% for anaplastic
astrocytoma & 18% -glioblastoma multiformeastrocytoma & 18% -glioblastoma multiforme

CNS TUMORSCNS TUMORS
Medulloblastoma (PNET)Medulloblastoma (PNET)– 20-25%of all brain tumors20-25%of all brain tumors– Small, round blue cell tumor-fast growingSmall, round blue cell tumor-fast growing– 30% metastasis30% metastasis– Surgery, radiation & chemotherapySurgery, radiation & chemotherapy– 5 yr survival rates 80%5 yr survival rates 80%