Embed Size (px)
Citation preview
Pediatric Traumatic Brain Injury
Janice L. Cockrell MD
Medical Director, Pediatric Rehabilitation
Legacy Emanuel Children’s Hospital
Incidence
• Annual incidence 180/100,000 in 1-15 year olds (Kraus, 1995)
• Most common cause of mortality
Pediatric TBI
• 81% mild
• 8% moderate
• 6% severe
• 5% fatal
Injury Severity
• Mild – unconscious <15 min; GCS 13-15
• Mod – unconscious >15 min; GCS 9-12
• Severe – unconscious >6hr; GCS 3-8
Etiology
• Non-accidental trauma in infants
• Falls in toddlers
• Ped vs. MVA in school-age children
• MVA in >16 year olds
Types of Injuries
• Trauma– Focal– Diffuse
• Stroke
• Hypoxia
Trauma
• Focal injuries– Prefrontal regions– Intracranial hematomas
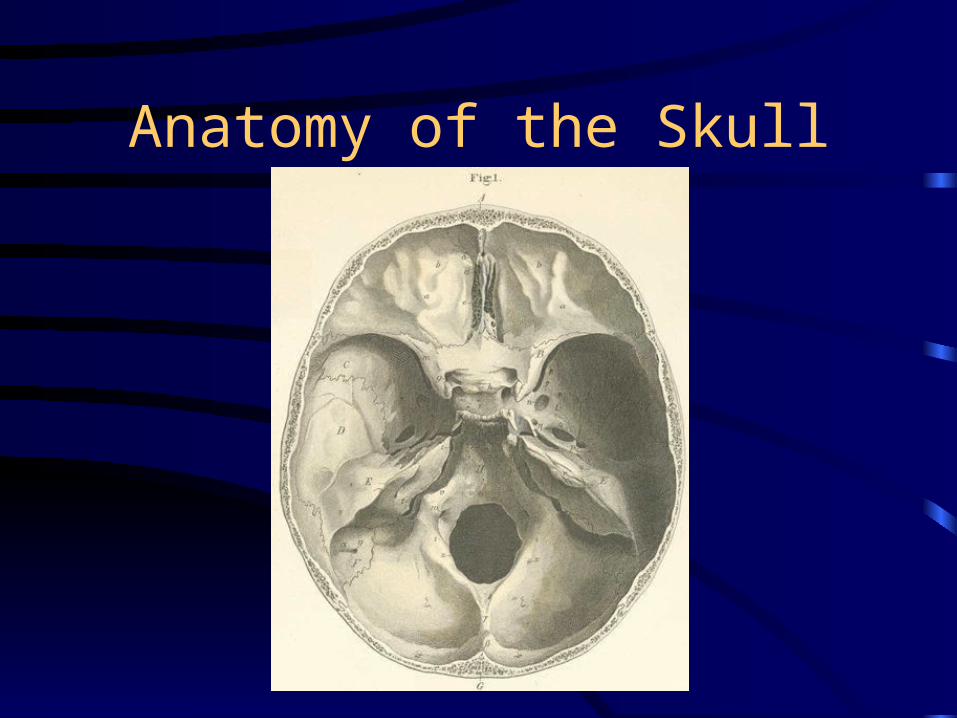
Anatomy of the Skull
Trauma
• Focal injuries– Prefrontal regions– Intracranial hematomas
• Diffuse injuries– Diffuse axonal injury (DAI)– Hypoperfusion– Excitatory cascades of neurotransmitters
producing free radicals
Risk Factors
• Age
• Previous TBI
• Socioeconomic deprivation
• Premorbid behavior problems only a minor risk factor
• (Demellweek et al, 2002)
Effect of AANS Trauma Protocols
• Implementation of the AANS protocols for TBI resulted in a 9.13 times higher odds ratio of a good outcome compared to prior outcomes in a community hospital.
• Hospital charges increased by more than $97,000 per patient. (Palmer, Bader, Qureshi et al, 2001)
Most Common Physical Problems (Hawley, 2003)
• Headache• Blurred vision• Difficulty sleeping• Fatigue• Clumsiness• Seizures• Hearing problems• Change in appetite

Sensory Problems
• Blurry vision
• Visual field cuts
• Cortical blindness
• Diplopia
• Hearing loss/central auditory processing problems
• Loss of smell
Motor Problems
• Spasticity
• Ataxia
• Clumsiness
• Tend to improve markedly over time
Outcomes measurement
• Glasgow Outcome Score
• IQ
• Academic achievement
• Motor skills
• Adaptive skills
• Problem solving
• Executive function
Glasgow Outcome Score
• 1 - Expired
• 2 - Vegetative
• 3 - Severe disability
• 4 - Moderate disability
• 5 - Good outcome
Most Common Sequelae
• Intellectual
• Academic
• Personality/behavioral
Cognitive Outcomes
• Declines in– IQ– Attention and concentration– Memory– Language– Non-verbal skills– Executive functions
Behavioral Outcomes
• Impulsivity
• Irritability
• Agitation (overstimulation)
• Apathy
• Emotional lability

Academic Outcomes
• Declines in achievement
• Declines in school performance
• Decreased adaptability

Problems Which Resolve Mild TBI
• Clumsiness
• Speech
• Hearing
Problems Which ResolveMod-Severe TBI
• Sleep
• Epilepsy
Problems Which PersistMild
• Attitude to siblings
• Nightmares
• Lost hobbies
• Personality change
• Temper
Problems Which PersistModerate/Severe
• Attitude toward siblings
• Clumsiness
• Concentration
• Hearing
• Mood fluctuations
• Temper
Adult Outcomes
• Difficulty maintaining employment
• Marital problems
• Social isolation (adults described as less likable, less interesting, less socially skilled)
• Involvement with criminal justice system
Long-term Neuropsychological Outcomes
• Family factors influence behavior and academic outcomes
• Family factors did not moderate neuropsychological outcomes
(Yeates, Taylor, Wade, et al 2002)
Intellectual & Emotional Functioning in College Students
with Hx of Mild TBI
• Intellectually unimpaired
• Significantly higher level of emotional distress (Marschark et al, 2000)
Executive Functions
• Modulated by frontal lobe and prefrontal circuits
• Involve both monitoring and controlling behavior
• Interact with declarative memory and processing speed but are distinct abilities
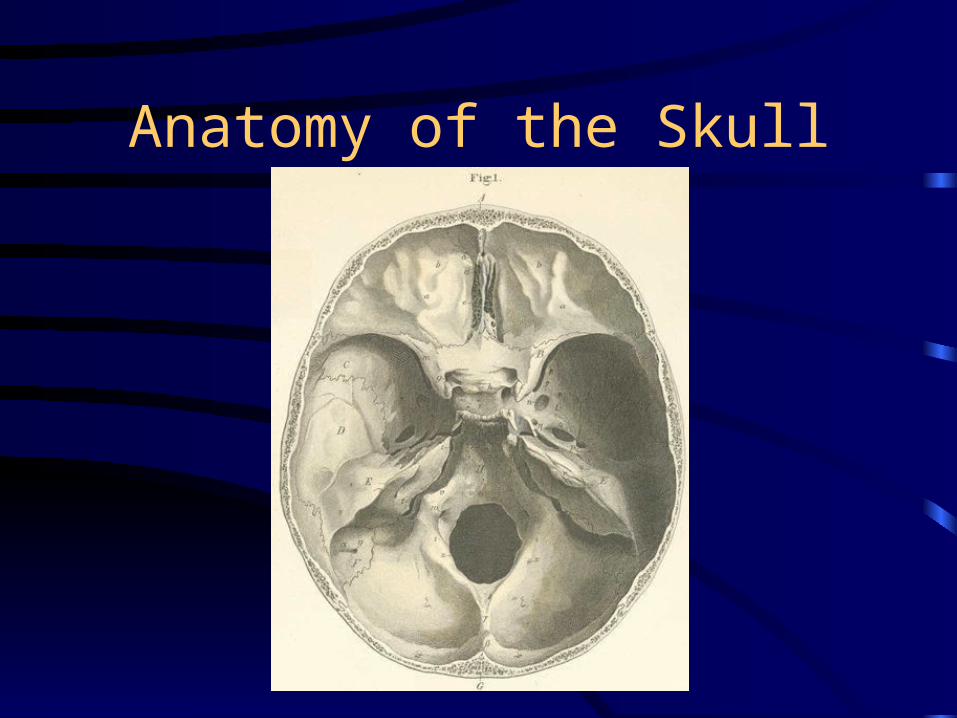
Anatomy of the Skull
Outcomes of Frontal Lesions
• Children with unilateral frontal lesions regardless of severity had a higher frequency of maladaptive behaviors than those without, even if there was no difference in cognition. (Levin, Zhang, Dennis et al 2004)
Mediating Factors
• Age
• Severity
• SEC– Family functioning– Education– Economic resources
• Premorbid personality
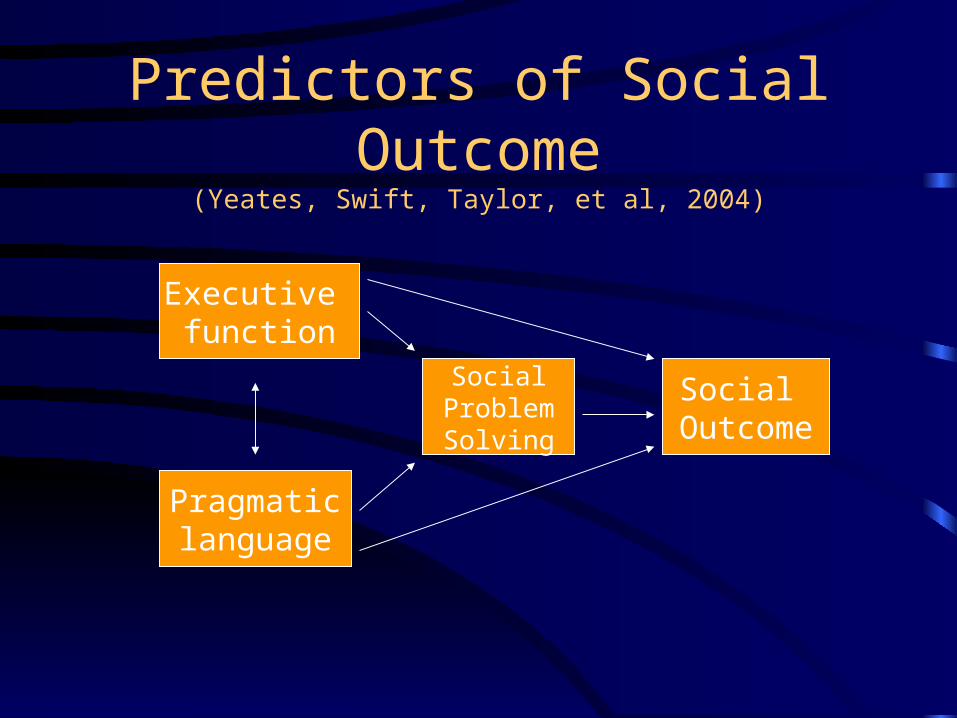
Predictors of Social Outcome(Yeates, Swift, Taylor, et al, 2004)
Executive function
Pragmaticlanguage
SocialProblemSolving
Social Outcome
SADHD
• Omission vs commission errors
• Omission errors immediately after TBI predicted SADHD
• Children with ADHD have a high number of commission errors
• SADHD is likely fundamentally different than ADHD. (Wassenberg, Max, Lindgren et al, 2004)
What can the treating physician do?
• Follow patient closely for the first few months
• Evaluate hearing and vision
• Monitor growth, nutrition
• Monitor and treat sleep disorders
• Educate patient and family regarding TBI
• Refer family for counseling if needed

Resources
• Brain Injury Association of Oregon 1-800-544-5243
• Brain Injury Support Group of Portland 1-503-413-7707
• Brain Injury Assoc of the US www.biausa.org
• Teaching Research, Western Oregon University 1-541-346-0573