Embed Size (px)
Citation preview

Pediatric Oncology
Nuts & Bolts
2008-9 (CURRENT VERSION AS OF 11/21/2011)

2
Goal #1: Common Malignancies Understand the presentation, pathophysiology, and prognosis of important malignancies in children and adolescents. Objective 1: Identify the presenting complaints, principles of current therapy, prognosis, and long-term complications due to the disease or therapy for these conditions: Leukemia (ALL, AML) Know the incidence of acute lymphoblastic leukemia and acute myelogenous leukemia, and the peak age at which these occur. Know which constitutional and genetic conditions predispose to the development of leukemia Know the clinical and laboratory features of acute lymphoblastic leukemia Recognize the clinical complications related to the hematologic abnormalities in acute leukemia Know the significance of an enlarged testis in acute lymphoblastic leukemia Know the clinical and laboratory findings that influence prognosis in acute lymphoblastic leukemia Recognize age as a significant risk factor in acute lymphoblastic leukemia prognosis, especially infants Know that the prognosis for acute lymphoblastic leukemia is partly related to cytogenetic findings Recognize and manage the myeloproliferative syndrome in infants with Down syndrome and differentiate it from acute myelogenous leukemia Recognize chloroma as a manifestation of acute myelogenous leukemia Brain Tumors Recognize the association between brain tumors and heritable syndromes (eg, neurofibromatosis, tuberous sclerosis) Recognize the clinical presentation of brain tumors by anatomic site (with specific attention to the most common tumors including: pilocytic astrocytoma, fibrillary astrocytomas, medulloblastoma/PNET, ependymoma, brain stem glioma Understand the role of surgery, radiation therapy and chemotherapy in the treatment of brain tumors Hodgkin’s and Non-Hodgkin’s lymphoma Know the differential diagnosis of acute lymphadenopathy and chronic lymphadenopathy simulating malignant lymphoma Know the criteria for "B" staging in patients with Hodgkin disease Know the association of Epstein-Barr virus and human immunodeficiency virus with non-Hodgkin lymphoma Know that the African type Burkitt lymphoma is associated with Epstein-Barr virus Recognize the superior vena cava syndrome as a presentation of lymphoblastic lymphoma Know the emergency management of a large mediastinal mass in non-Hodgkin lymphoma Know the emergency management of tumor lysis syndrome in non-Hodgkin lymphoma Neuroblastoma Recognize the clinical presentation of metastatic and nonmetastatic neuroblastoma Know the initial evaluation of a patient with neuroblastoma

3
Wilms’ Tumor Recognize the clinical presentation of Wilms tumor Bone tumors (osteosarcoma and Ewing’s sarcoma) Recognize the predilection of osteosarcoma for the metaphysis of long bones Know the role of surgery in the treatment of osteosarcoma Recognize the clinical presentation of Ewing sarcoma by anatomic site Recognize the radiologic findings of Ewing sarcoma Bone marrow transplantation Recognize the clinical indications for bone marrow transplantation Recognize the types of conditions amenable to this type of treatment Know the common complications related to bone marrow transplantation (e.g. graft-versus-host disease) Objective 2: For the common pediatric signs and symptoms, describe clinical findings that would warrant screening for malignancy Adenopathy – recognize the features of a pathologic node including size, texture, fixed, and location Headache - recognize symptoms associated with raised intracranial pressure including associated vomiting, papilledema, Parinaud’s syndrome, and cranial nerve abnormalities Limb pain – recognize common locations for limb pain associated with sarcomas (e.g. distal femur), as well as the absence of trauma associated with limb pain. In addition, recognize limb pain associated with swelling as a potential presenting symptom of a sarcoma Hepatomegaly and/or splenomegaly – learn the proper way to palpate an abdomen with attention to contour, texture, size and associated findings Persistent fever and malaise – recognize this as a common finding of hematologic malignancies and the association with Hodgkin’s lymphoma Seizures – recognize seizures as a rare complication of brain tumors in children due to the infratentorial predominance of these tumors in children Weight loss – recognize weight loss as a potentially subtle sign of an occult malignancy and the association with Hodgkin’s lymphoma Objective 3: Describe common acute side effects of commonly used chemotherapeutic drugs Specific agents covered include: Vincristine Cyclophosphamide Anthracyclines Methotrexate Cisplatin New targeted therapies Immune-based therapies

4
Objective 4: Describe common late complications of childhood cancer treatment that may present in childhood or adolescents Specific late effects covered include: Neuro-developmental morbidity related to radiation therapy and intrathecal chemotherapy Endocrine dysfunction related to radiation therapy or surgical ablation Secondary malignancies related to genetic risk and therapy associated malignancies Cardiac dysfunction related to anthracycline exposure Sterility related to high-dose therapy Goal #2: Conditions generally referred to an oncologist. Understand how to diagnose and initiate management of potential oncologic disorders which generally need referral Specific disorders include: Pancytopenia An abdominal mass A mediastinal mass Symptoms in patients predisposed to malignancy (e.g. neurofibromatosis, Downs syndrome) Goal #3 Psychosocial Aspects of Cancer Care Understand how to manage issues related to the psychosocial aspects of cancer care Specific issues include: Issues centering around end-of-life care decisions Pain control in children with life-limiting conditions Presenting “bad news” to patients and families Ethical considerations in the treatment of children with malignancies

5
Initial Work-up of Newly Diagnosed Pediatric Oncology Patients by Diagnosis I. Acute Leukemia (ALL or AML) Bone Marrow Aspirate (BM) – Needed for diagnosis in all cases, except for patients with extremely high WBC (>100K with >75% blasts), in which case peripheral blood (PB) can be substituted. Bone marrow biopsy is generally not necessary for diagnosis of leukemia. Morphology – Flow cytometry – 2 ml BM in green top and/or 5 ml PB in purple top to flow lab. NOTE: Send a peripheral blood sample to flow lab as soon as leukemia diagnosis is suspected- this is the most important diagnostic test to quickly establish how to treat the patient. They will do immunuophenotyping (surface marker expression) to distinguish ALL from AML (more reliable than morphology). They will also perform minimal residual disease (MRD) studies. Results available in hours Cytogenetics –They will determine ploidy and presence of specific cytogenetic translocations, which of diagnostic and prognostic value. Results take approx. 2 wks, Molecular diagnostics – 2 ml BM (or 5 ml PB) in purple top They will perform PCR to identify specific molecular abnormalities. For suspected ALL, request TEL-AML1, BCR-ABL and MLL testing. For suspected AML, request FLT3 mutation analysis. These are each important prognostic factors. Also, request appropriate test on suspected relapsed patients where specific molecular abnormality is known (BCR-ABL, e.g.). Clinical trial biology studies Cerebrospinal Fluid (CSF) – Obtained via lumbar puncture for all newly diagnosed leukemia patients to establish CNS stage (CNS-1: WBC < 5/hpf, no blasts on cytospin; CNS-2: WBC < 5/hpf, leukemic blasts present on cytospin; CNS-3: WBC >= 5/hpf, leukemic blasts present on cytospin). First dose of intrathecal chemotherapy is often given with diagnostic LP if diagnosis (ALL vs. AML) is already known. Cytospin – at least 2 ml CSF in sterile tube. Will do cytospin and Wright-Giemsa stain to look for leukemic blasts in CSF. . Cell count, differential, glucose, protein – at least 1 ml CSF in 2 sterile tubes to core lab Laboratory Tests CBC/diff – determine transfusion needs, assess for neutropenia, prognostic information from WBC Chemistries (CMP, uric acid, LDH) – assess for tumor lysis (high K, PO4, uric acid, LDH), renal insufficiency (from tumor lysis, hyperuricemia, leukemic infiltration of kidneys) PT/PTT, DIC panel – assess for coagulopathy (common in M3 AML) Type and cross – prepare for transfusions (don’t forget transfusion consents!) Cultures (blood, urine, etc.) – obtain if febrile, especially if also neutropenic Serologies – consider documenting serologic status for HSV and VZV, since reactivations common during chemotherapy

6
HLA typing – consider for high risk leukemia (AML, high risk ALL), since transplant in first remission possible Other Studies/Consults Echocardiogram/EKG – needed for AML or high risk ALL, since both will receive anthracyclines during induction CXR/chest CT – consider for respiratory symptoms and/or T-cell ALL to rule out presence of mediastinal mass Renal consult – consider if uric acid high at diagnosis, particularly if creatinine is elevated, since dialysis may be required. Usually, they prefer to be called early in the diagnostic process. Head CT – consider for mental status changes or focal neuro signs/symptoms to rule out CNS bleed (high risk in M3 AML) or CNS chloromas (rare) Ophtho exam – consider for visual changes to rule out retinal hemorrhages (high risk in M3 AML) Radiation oncology consult – consider if CNS positive and/or high risk ALL since CNS radiation may be needed

7
Workup of other common diagnoses:
HD NHL NBL RMS OS EWS CNS WT GCT RB Staging CT neck CXR/CT chest CT abd/pelvis MRI (or CT) 1o site(s) 3 MRI brain 6 10 12 13
MRI spine 4 8 LP for CSF analysis 5 6 8 Plain x-ray 1o site Bone scan 1 1 10 PET Bilat. BMA/Bx 2 10 MIBG scan Gallium scan Thallium scan 7 Abd u/s (incl. Doppler) Baseline Organ Function Echo/EKG 11 PFT’s 9 CrCl (24hr urine or
nuclear med study) 9 14
Audiology 9 Tumor markers Serum -HCG, AFP Urine catecholamines
(HVA, VMA)
Ferritin LDH ESR Uric acid
Diagnosis abbreviations: HD- Hodgkin disease, NHL- non-Hodgkin lymphoma, NBL- neuroblastoma, RMS- rhabdomyosarcoma, OS- osteosarcoma, EWS- Ewing’s sarcoma, CNS- brain tumor, WT- Wilm’s tumor, GCT-germ cell tumor , RB- retinoblastoma Footnotes 1 Obtain if “B” symptoms or bony pain present 2 Obtain BMA for flow, cytogenetics in case BM involved 3 Obtain brain MRI if opsoclonus/myoclonus present 4 For paraspinal tumors to evaluate for cord compression 5 If opsoclonus/myoclonus present 6 For cranial parameningeal tumors only 7 Recommended, but not routinely done at JHH 8 For CNS tumors with propensity for CSF metastasis (e.g., medulloblastoma, ependymoma, germ cell tumor, AT/RT, PNET). Send CSF for -HCG, AFP for CNS germ cell tumors. 9 For patients who will receive chemo (PFT’s if will receive CCNU, audiology/CrCl if will receive cisplatin or carboplatin) 10 For clear cell sarcoma of kidney only11 Not needed for low stage disease since won’t receive anthracyclines (consult protocol)12 Only if neurologic symptoms present (to rule out concomitant CNS GCT) 13 To assess evidence of extraorbital spread and to rule out metastasis to pineal gland (so-called “trilateral retinoblastoma”)14 For patients who will receive carboplatin as part of a chemoreduction regimen

8
General Considerations:
1. Sperm banking- All pubertal males should be offered sperm banking prior to treatment for their cancer. 2. Biology studies- If there is an open clinical trial in which a patient will be enrolled, check the protocol for any additional samples to be sent for biology studies. 3. Radiation oncology consults- These should be obtained early in the diagnostic process for most of the diagnoses in the table, since radiation will be at least considered as therapy. The only exception is osteosarcoma, where radiation is rarely used. 4. Access- The surgeons should be called early in the diagnostic process to schedule central line placement, when needed. Type of line (Infusaport vs. Hickman, number of lumens) will be dependent upon therapy to be given 5. Pregnancy test- Don’t forget this for all females even close to reproductive age. 6. Serologies- Consider viral serologies prior to starting therapy. HIV can be associated with NHL, EBV with HD or nasopharyngeal carcinoma, e.g. Also, documentation of HSV and VZV serologic status can be helpful in diagnosis and management of exposures and suspected cases of reactivation (which are common in patients receiving chemotherapy).

9
Management of Hyperleukocytosis and Tumor Lysis Syndrome General Introduction Acute leukemia often presents with an elevated white blood cell count 1. Hyperleukocytosis becomes a potential problem when the white blood cell count rises above 100,000 2. Consequences of an elevated white blood cell count include: a. Hyperviscosity i. Sludging of viscous blood in the brain causes decreased level of consciousness, ranging from confusion to lethargy to coma and is fatal if not relieved ii. Sludging of viscous blood in the lungs causes hypoxia and can be fatal if not relieved iii. Sludging of viscous blood in the kidneys can contribute to acute renal insufficiency b. Increased risk of acute tumor lysis syndrome 3. The risk of hyperviscosity is greater with AML than with ALL (myeloid cells are “stickier” than lymphoid cells), but the risk of tumor lysis syndrome is greater with ALL than with AML. These are TENDENCIES, though. One can see symptomatic hyperviscosity with ALL, and AML patients have tumor lysis syndrome. Hyperleukocytosis 1. Signs of hyperleukocytosis/hyperviscosity: a. Hypoxia with increased pulmonary markings diffusely on chest x-ray b. Altered mental status c. Renal insufficiency d. The above must be in the context of a white blood cell count >100,000 e. These findings can occur individually or collectively Any of the above findings in the context of a white blood cell count >100,000 must be treated as evidence of hyperviscosity caused by hyperleukocytosis, but DO NOT FORGET a differential diagnosis. Patients can present with pneumonia, congestive heart failure, renal infiltration with leukemia or lymphoma cells, infection, intoxication, or other etiologies for each of the signs listed above, and these alternatives need to be considered 1. Management of hyperleukocytosis: a. Exchange transfusion vs. leukapheresis The choice between exchange transfusion and leukapheresis depends in part on patient size and in part on physician preference. b. Contact surgery IMMEDIATELY upon learning of a patient with an elevated white blood cell count and any of the above signs of hyperviscosity c. Encourage the surgeon to place the largest caliber central line possible, to facilitate leukapheresis d. Very small children and infants may not tolerate the fluid shifts associated with leukapheresis and will require exchange transfusion instead e. Exchange transfusion can be accomplished with an arterial line and a large caliber peripheral iv, and may therefore be more expedient (no need for sedation/anesthesia for the placement of a central line)

10
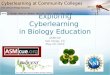
f. Treat the disease: The vast majority of the tumor cells are present in the bone marrow, even in patients with peripheral white blood cell counts exceeding 500,000 g. No study has demonstrated a benefit, in terms of long term outcome, for leukapheresis or exchange transfusion i. The decreased white blood cell count in the peripheral blood is temporary, and reverses within hours ii. Dropping the peripheral white blood cell count does NOT alter the risk of tumor lysis syndrome. Therefore, the role of leukapheresis and exchange transfusion is in the management of symptomatic hyperviscosity. In the absence of symptoms, these interventions are not necessary. h. Regardless of the decision to institute leukapheresis or exchange transfusion, INTIATE DEFINITIVE THERAPY AS SOON AS POSSIBLE Acute Tumor Lysis Syndrome 1. Seen not only in leukemia, but also in other diseases, the classic being Burkitt’s lymphoma 2. Results from rapid lysis of tumor cells, releasing intracellular contents into the bloodstream 3. Characteristic triad of hyperuricemia, hyperkalemia, hyperphosphatemia. Hypocalcemia also seen. Hyperuricemia 1. Results from breakdown of purines released from dying cells 2. Purines are eventually metabolized to uric acid which is excreted by the kidneys 3. At a high enough concentration, uric acid crystallizes in the kidneys. These crystals are nephrotoxic 4. Symptoms depend on uric acid level in the blood: a. Lethargy, nausea, vomiting and renal colic can be seen between 10-15 mg/dl b. Above 20 mg/dl, renal toxicity and severe CNS dysfunction (coma) can occur 5. Treatment of hyperuricemia: a. Decrease production i. Allopurinol blocks the production of uric acid by inhibiting xanthine oxidase ii. Rasburicase is recombinant urate oxidase and catalyzes the conversion of uric acid to allantoin. This drug works almost instantaneously to reduce uric acid levels to almost undetectable.
Nucleotide Precursors
Hypoxanthine Xanthine Uric Acid
Allantoin
xanthine oxidase
Urate
xanthine oxidase
pH~7.3
X X
X = site of action of allopurinol
= site of action of rasburicase
Urate Oxidase

11
b. Promote solubility by alkalinizing the urine using NaBicarb in iv fluids c. Decrease concentration by volume expansion (2x maintenance fluids) Hyperkalemia 1. Results from lysis of tumor cells and release of intracellular potassium 2. Compounded by renal insufficiency Hyperphosphatemia 1. Results from release of intracellular phosphate from dying tumor cells 2. Lymphoblasts have 4x more intracellular phosphate than lymphocytes 3. Compounded by renal insufficiency 4. Treat with diuretics to promote renal excretion Hypocalcemia 1. Related to hyperphosphatemia 2. Worry about calcium phosphate crystal formation and precipitation when Ca x PO4 >60 mg/dl 3. Avoid alkalosis (decreases solubility of CaPO4 crystals) STANDARD INITIAL APPROACH TO ACUTE TUMOR LYSIS SYNDROME IVF D5 1/2NS +40 meq/L NaHCO3 at 2x maintenance Adjust fluids to maintain urine pH 7.0-7.5 Frequent monitoring of electrolytes (as frequent as every 2 hours) Allopurinol or rasburicase (there are specific eligibility criteria for rasburicase) Dialyze for the usual indications Monitor for other metabolic complications (hyponatremia, hypomagnesemia)

12
Spinal Cord Compression, Increased ICP, CVA, SMS/SVC, Typhlitis
Spinal Cord Compression 1. ETIOLOGY: most often epidural compression from extension of paravertebral tumor through the intervertebral foramina or extension of tumor in the vertebral column. 2. PRESENTATION: back pain (localized/radicular) in 80%, weakness, sensory loss, change in bowel/bladder function. Prognosis for recovery based on duration and level of disability at presentation. 3.DIAGNOSIS/MANAGEMENT: With normal neuro exam, may start dexamethasone 0.25 to 0.5 mg/kg/day PO divided q 6 hrs and perform MRI of spine within 24 hours. With abnormal neuro exam,start dexamethasone 1 -2 mg.kg.day IV and obtain emergent MRI of spine. **Note:steroids may prevent diagnosis of lymphoma- plan diagnostic procedure as soon as possible. If cause of tunor is known: emergent radiotherapy or chemotherapy for sensitive tumors, otherwise plan emergent neurosurgical consultation. If cause of tumor is unknown: immediate surgery to decompress the spine. Increased Intracranial Pressure 1.ETIOLOGY: ventricular obstruction, obstruction of CSF flow 2. PRESENTATION: Varies according to age. Headache, vomiting, lethargy, seizures, personality changes, loss of skills. 3. DIAGNOSIS: Head CT or brain MRI. MRI is more sensitive for diagnosis of posterior fossa tumors. 4. MANAGEMENT: Immediate neurosurgical consultation. Elevate head of bed 30 degrees, avoid hypoosmolar IV solutions. Consider use of mannitol. If tumor is identified, add dexamethasone 2 mg/kg/day IV divided q6 hrs. Cerebrovascular Accident 1. ETIOLOGY: hyperleukocytosis, thrombocytopenia, coagulopathy, treatment related (ex L-asparaginase, methotrexate, radiation induced fibrosis). 2. PRESENTATION: usually a sudden change in motor skills or speech, may also have seizures or severe mental status changes. 3. DIAGNOSIS: Head CT with contrast, brain MRI, MRA/MRV. 4. MANAGEMENT: If factors depleted by L-asparaginase, platelet transfusions and FFP as needed. For thrombosis, administer heparin. Avoid L-asparaginase and consider new threshold for transfusing platelets. Superior Mediastinal/Superior Vena Cava Syndrome 1. ETIOLOGY: Hodgkin’s disease, non-Hodgkin’s lymphoma, T-cell ALL, germ cell tumors, occlusion of central venous catheter. 2. PRESENTATION: Orthopnea, headaches, facial swelling, dizziness, plethora 3. DIAGNOSIS/MANAGEMENT: CXR. Consider CT or MRI scan to asses airway. CONTROL AIRWAY! Attempt diagnosis of malignancy by least invasive method possible before beginning treatment. Empiric therapy to possibly include radiotherapy, steroids, cyclophosphamide. Typhlitis 1. ETIOLOGY: Neutropenic enterocolitis. Inflammation of the bowel wall, usually localized to the cecum.

13
2. PRESENTATION: right lower quadrant abdominal pain, nausea, fever, diarrhea. Most common in patients being treated for leukemia and lymphoma, especially when Ara-C is used. (ex AML). At worst, can perforate. 3. DIAGNOSIS/MANAGEMENT: careful abdominal exam, AXR may show pneumatosis, paucity of air, bowel wall edema. Likely follow with CT to confirm diagnosis. Make patient NPO, add anaerobic and gram-negative coverage. Alert GPS and follow closely with serial abdominal exams. .

14
Fever and Neutropenia .
A patient with fever and neutropenia should be considered an emergency, never a routine admission. Patients often deteriorate rapidly and sometimes worsen even after initial doses of antibiotics. Even with appropriate care, 5-10% of cancer patients will die from infectious complications. The degree and duration of neutropenia are important risk factors. Along with neutropenia, oncology patients have many other factors that make them susceptible including altered phagocyte function, cellular immunity, and humoral immunity. Altered physical defense barriers such as mucositis permit changes in colonization and are often points of entry for systemic invasion. For all of these reasons, oncology patients with neutropenia are much more vulnerable than patients with cyclic neutropenia, viral-induced neutropenia, etc. The cornerstone of treatment is empiric antibiotics. This concept was developed in the 1970s. Studies in the late 1970s/early 1980s led to the practice of continuing antibiotics until resolution of neutropenia, even if all cultures remain negative. Definitions: Absolute neutrophil count (ANC): total WBC x (% neutrophils + % bands) Fever and Neutropenia: ANC < 500 or falling toward this level with fever >38.30C (orally) or two temperatures > 38.00C twice in a 24 hour period. ** Note that patients with low grade fevers on steroids or who appear ill in the absence of fever require a similar evaluation. Evaluation: 1. History: attention to development of symptoms in relation to flushing the line, chills/rigors, mental status changes, respiratory symptoms, and pain with bowel movements. Note any prior infections and organisms involved. 2. PE: Carefully note vital signs! Assess perfusion status. Tachycardia +/- hypotension may be early signs of sepsis. Detailed PE including examination of oropharynx for mucositis and/or lesions, line site for erythema, discharge, or tenderness, and perirectal area for erythema or tenderness. Do not do a digital rectal exam due to the risk of translocating bacteria. Note that signs of inflammatory response may be minimal with neutropenia. 3. Labs: CBC with differential, comprehensive metabolic panel, blood cultures from all central line lumens, UA and culture (do not catheterize), blood T & S. CXR only if respiratory symptoms present. Surveillance cultures (throat, urine, and stool) are controversial, but we do obtain them. Studies have shown no utility of obtaining peripheral blood cultures in our patient population. 4. Antibiotic Therapy (Note: All dosing should be based on the guidelines in Nuts & Bolts, NOT The Harriet Lane Handbook). A.) If patient is not ill appearing and has no apparent focus of infection, start antibiotics with both gram-negative and gram-positive coverage. We typically start with piperacillin/tazobactam. B.) If patient appears ill, provide double coverage for Pseudomonas. We typically start with piperacillin/tazobactam and amikacin. C.) If blood cultures remain negative and patient is afebrile, continue broad spectrum coverage until evidence of marrow recovery (rising ANC). D.) If patient is persistently febrile after 48-72 hours, consider broader gram-negative coverage and also consider adding oxacillin or vancomycin for better gram-positive coverage. E.) If patient is persistently febrile after 4-7 days, add amphotericin at 0.5 mg/kg/day and work-up for fungal infection (Sinus, chest, abd/pelvis CT). **See The Harriet Lane Handbook for pre-medications used with amphotericin. If fever persists > 72 hrs on this dose of

15
amphotericin, increase to 1 mg/kg/day. For patients with severe infusion related reactions unresponsive to interventions and/or renal compromise, discuss the use of Abelcet with the oncology team and ID. F.) Note: Patients with continued fever and/or recurrence of fever need prompt, thorough physical exams. Further Evaluation and Modifications Based on Focus of Infections: Site Presentation Evaluation Treatment Modification
Central Line Erythema, warmth, discharge
Blood Cxs from all lumens
Additional gram-positive coverage. Removal of line for tunnel infection, fungal, or prolonged infection.
HEENT Gingivitis Vesicles or ulcerative lesions Sinus tenderness
HSV cultures, PCR, Tzanck test CT scan
Add anaerobic coverage Add acyclovir Consider fungal coverage
Respiratory Inc WOB, cough, tachypnea, hypoxia
CXR, likely CT also. Sputum for culture, PCP, fungal stain. HSV, CMV serology. CMV early antigen, cx. Consider early BAL.
Consider coverage for: fugus, PCP, Mycoplasma, CMV, HSV. Consider early steroids for suspected PCP- contraindicated in fungal infection.
Gastrointestinal Retrosternal pain Acute abdominal pain Diarrhea Perianal tenderness
Consider endoscopy or upper GI AXR, likely also CT Stool cxs, C. difficile toxin
Consider fungal and/or HSV coverage, H2 blocker. If suspect typhlitis, add anaerobic and gram-negative coverage. Add anaerobic coverage.

16
Chemotherapy . The principle of chemotherapy is a simple one, stop growing cells from dividing. Since cancer cells are dividing at a higher rate than normal ones, the theory goes, cancer will die before all of the normal tissue. With very few exceptions, the drugs in pediatric oncology are used according to this principle. Since chemotherapeutic agents following this principle are only relatively selective for cancer cells, many of the side effects are related to the activity of drugs on normal tissue, Chemotherapy is usually given in combinations of agents. Often these combinations are given cute nicknames, to allow for discussion without listing all the drugs to be used. Unfortunately, in order to fit the drugs into one of these easy-to-remember nicknames, alternate or archaic names of some of the drugs are used. For example, DCTER (“Doctor’) is a regimen of Dexamethasone, Cytarabine, Thioguanine (6-TG), Etoposide, and Rubidomycin (daunomycin). This is the only regimen where the anthracycline daunomycin is called rubidomycin. Memorizing these mnemonics is a function of experience only. This section will provide a brief discussion the major classes of anti-neoplastic agents and an alphabetically organized chart for easy reference of the most commonly used drugs in pediatric oncology. Since chemotherapy pharmacology is an active science, the information here will limited as new agents are developed and more is known about the activities of these drugs. Alkylators e.g. Busulfan, Cyclophosphamide, Melphalan, Nitrosureas, Thiotepa These drugs act by covalently binding to DNA inducing DNA damage and DNA-DNA or DNA-protein crosslinks. Although some drugs act in a cell cycle non-specific manner, cell kill occurs in rapidly prolferating cells. Cyclophosphamide (cytoxan) and Ifosfamide are metabolized to active compounds including acrolein. Acrolein and other metabolites bind to and destroy bladder epithelium leading to hemorrhagic cystitis. 2-mercaptoethanesulphonic acid, or Mesna, is a uroprotectant that binds to the alkylator metabolites and allows their safe excretion through the urine. Mesna dose must be 60% or greater of the dose of the chemotherapy drug to be used. Given the complications of hemorrhagic cystitis, hydration is usually prescribed with the oxazophosphorine alkylators (cyclo- and ifosfamide). This hydration can be problematic since SIADH is another possible complication of these drugs. Anti-metabolites e.g. 5-FU, 6-MP, 6-TG, Ara-C, Cladribine, Fludarabine, (Methotrexate discussed separately below) The anti-metabolites are agents that resemble nucleosides, but with chemical modifications rendering them functionally inactive. Depending on their exact targets, they may block DNA polymerase and inhibit chain elongation, or they may act on other enzymes and block nucleic acid synthesis. These drugs, thus, kill only cells in active states of growth and division. Ara-C (cytarabine) when given at high doses is excreted in tears and can result in a local conjunctivitis. Eye drops should be administered prophylactically to any patient receiving high dose Ara-C.

17
Intercalators e.g. Actinomycin-D, Bleomycin, Daunorubicin, Doxorubicin, Mitoxantrone, Platinum compounds These drugs work by inserting themselves in between the base pairs of the double-stranded DNA molecule (intercalation). This action can have a number of effects, ranging from inhibition of the enzymes that unwind DNA during replication (topoisomerase) to induction of DNA strand cleavage. Different drugs have different specific mechanisms of action. Lung damage is a potential complication of treatment with bleomycin. This complication is rare in the acute setting, but may manifest as dyspnea, cough, and low oxygen saturation anytime after receiving bleomycin. Fever is common within the first 24 hours after bleomycin treatment. Anthracycline and related drugs (dauno- and doxorubicin and mitoxantrone) can cause cardiac effects, most notable as electrocardiographic changes or arrhythmias, within 48 hours of administration. The majority of these effects are usually asymptomatic and transient, lasting 72 hours or less. Over the long term, though, these drugs can lead to cardiomyopathy and heart failure. These drugs also lead to urine discoloration, with dauno- and doxorubicin causing pink urine. Since these drugs are often co-administered with alkylators, differentiating anthracycline-colored from blood tinged urine is important. In addition to causing the most profound nausea and vomiting of any chemotherapy agents, the platinum compounds have strong effects on the kidneys. Most commonly, magnesium wasting is found, but other electrolyte abnormalities can occur. Renal insufficiency can occur both acutely and chronically. Ototoxicity, manifesting as high frequency hearing loss, is another frequent complication of platinum therapy. With these side effects, carboplatin is usually dosed according to the Calvert formula, which uses measured GFR and creatinine clearance to dose the drug. Topoisomerase Inhibitors e.g. Etoposide, Irinotecan, Topotecan These drugs act on the topoisomerases, enzymes required for unwinding DNA during replication. Etoposide forms a covalent bond with topoisomerase II, resulting in DNA breakage, while the others inhibit topoisomerase I. As such, these drugs only work against replicating cells. Diarrhea is the most serious side effect of irinotecan. In patients not following an anti-diarrhea regimen, this side effect occurs in 50%; with an anti-diarrheal regimen, the incidence remains above 10%. The diarrhea, once started, can be intractable requiring hospitalization and IV hydration. At the first sign of increased frequency or loose stools, patients should take start loperamide, and continue up to every 2 hours until normal bowel pattern is established. Neomycin has shown some benefit in irinotecan-induced diarrhea.

18
Asparaginase Asparaginase acts by depleting asparagine and thus blocking protein synthesis. In normal cells, asparagine is a non-essential amino acid, unlike tumor cells which require increased amounts of asparagine. Since it affects protein synthesis, liver damage is a potential problem of asparaginase administration. This liver damage may present as coagulopathy, since clotting factors are also rapidly synthesized and degraded. Additionally, pancreatitis is a complication which can present in the range from abdominal pain to pseudocyst with pancreatic insufficiency. Allergic reactions to asparaginase are common, ranging from rash to anaphylaxis. Multiple forms of asparaginase exist to allow delivery of this drug to patients who have a reaction to the E. coli derived L-asparaginase. Methotrexate Methotrexate inhibits dihydrofolate reductase (DHFR), reducing the level of folate synthesis and, therefore, the amount of nucleic acid and protein synthesis. Methotrexate administration results in an acute, transient transaminitis very rarely leading to more serious liver problems. Mucositis, myelosuppression, nephrotoxicity, and pulmonary toxicity are the most common side effects of methotrexate administration. With the exception of mucositis, these other side effects are related to prolonged exposure to methotrexate. As such, Leucovorin (folinic acid) is given to “rescue” the anti-folate effects of methotrexate by bypassing the need for DHFR in folate synthesis. Methotrexate levels are monitored during leucovorin administration with discharge held until an appropriately low serum level are reached. Other anti-folate drugs like trimethoprim (Bactrim) can potentiate the effects of methotrexate. DRUG TABLE Below are listed 30 of the most common chemotherapy drugs used in Pediatric oncology. This is not a comprehensive list, but a ready-reference. “Immediate Toxicities” are those that occur within minutes to 72 hours after drug infusion. The interventions listed are guidelines. Obviously, patient care is most directly tailored to the clinical appearance and needs of the individual patient. “Delayed Toxicities” can be from one week to many years later, and are considerations for the outpatient or ambulatory setting. MicroMedex and other resources provide more detailed information.
Drug Other Names
Mechanism of Action
Immediate Toxicities
Intervention Delayed Toxicities
5-Fluorouracil 5-FU Nucleoside analog
Diarrhea Neuro changes
(cerebellar ataxia, mood changes)
Supportive Discontinue 5-FU
Myelosuppression Dacrocystitis (Rx is topical
steroids)
6-Mercaptopurine 6-MP Nucleoside analog
Nausea/vomiting Anti-emetics
Myelosuppression Hyperbiluribinemia
6-Thioguanine 6-TG Nucleoside analog
Nausea/vomiting Anti-emetics
Myelosuppression Hyperbiluribinemia
Actinomycin-D Dactinomycin DNA intercalater
Transaminitis Nausea/vomiting
None Anti-emetics
Myelosuppression
Ara-C Cytarabine Nucleoside analog
Conjunctivitis
Eyedrops
Myelosuppression

19
Mucositis Neuro changes
(ataxia, lethargy, confusion)
Supportive Hydration
Asparaginase Elspar (also derivatives: PEG-asparaginase, Erwinia asparaginase)
Protein synthesis inhibitor
Hypersensitivity/ anaphylaxis
Liver dysfunction Coagulopathy Pancreatitis
Supportive Supportive Supportive Supportive
Pancreatitis Pancreatic
insufficiency
Bleomycin DNA intercalater
Hypersensitivity/ anaphylaxis
Fever (in first 12-
24 hours)
Supportive Anti-pyretics
Pulmonary Fibrosis
Busulfan Alkylator Seizures Nausea/vomiting
Phenytoin prophylaxis Anti-emetics
Myelosuppression
Carboplatin CBDCA DNA intercalater
Hypomagnesemia Mucositis
Magnesium Supportive
Myelosuppression Renal Insufficiency
High Frequency hearing loss
Peripheral neuropathy
Cisplatin CCDP DNA intercalater
Hypomagnesemia Renal
insufficiency Mucositis
Magnesium Saline hydration Supportive
Myelosuppression Renal Insufficiency
High Frequency hearing loss
Periph. neuropathy
Cladrabine 2-CDA Nucleoside analog
Myelosuppression Lymphopenia
Cyclophosphamide Cytoxan Alkylator Hemorrhagic cystitis
SIADH Nausea/vomiting Mucositis Cardiomyopathy
Hydration, MESNA, urology consult NOT decreased hydration, electrolyte balance Anti-emetics Supportive Supportive
Myelosuppression
Daunorubicin Rubidomycin DNA intercalater
Nausea/vomiting Arrhythmia
Anti-emetics Monitor and
Myelosuppression Heart Failure

20
Colored urine
support (usually transient ~72h) None
Doxorubicin Adriamycin Hydroxydaun-omycin
DNA intercalater
Nausea/vomiting Arrhythmia Colored urine Mucositis
Anti-emetics Monitor and support (usually transient ~72h) None Supportive
Myelosuppression Heart Failure
Etoposide VP-16 Topoisomerase II inhibitor
Hypotension Nausea/vomiting Cortical blindness
Hydration Anti-emetics None (transient)
Myelosuppression Peripheral
neuropathy
Fludarabine Nucleoside analog
Neuro changes (encephalopathy, seizures)
Nausea/vomiting Capillary leak
Anti-convulsives Anti-emetics Colloid
Myelosuppression
Gleevec Imatinib Kinase inhibitor
Heartburn Myalgia Edema Nausea/vomiting
Antacids Supportive Supportive Anti-emetics
Myelosuppression Fatigue Pigmentation
changes
Hydroxyurea Hydrea DNA synthesis inhibitor
Nausea/vomiting Anti-emetics
Myelosuppression

21
Ifosfamide Alkylator Hemorrhagic cystitis
SIADH Nausea/vomiting Mucosiitis Mental status
changes Renal tubular
acidosis
Hydration, MESNA, urology consult NOT decreased hydration, electrolyte balance Anti-emetics Supportive Slow Ifos infusion Electrolyte balance
Myelosuppression
Irinotecan Topoisomerase I inhibitor
Diarrhea Transaminitis Microscopic
hematuria
Loperamide (at first sign of loose stool) none none
Myelosuppression
Melphalan Alkylator Nausea/vomiting Anti-emetics
Myelosuppression
Methotrexate MTX Anti-metabolite (DHFR inhibitor)
Mucositis Renal failure Acute
pneumonitis
Supportive Saline hydration Steroids
Myelosuppression
Mitoxantrone DNA intercalater, Topoisomerase II inhibitor
Nausea/vomiting Colored urine
Anti-emetics None
Myelosuppression Heart Failure
Nitrosurea CCNU or BCNU Lomustine Carmustine
Alkylator Nausea/vomiting Encephalopathy Liver dysfunction
Anti-emetics d/c nitrosurea Supportive
Myelosuppression Interstitial
pneumonitis
Temozolomide TMZ Temodar
Alkylator Nausea/vomiting Neuro changes
(confusion, ataxia)
Anti-emetics Supportive
Myelosuppression Selective
thrombocytopenia
Thiotepa Alkylator Nausea/vomiting Mucositis
Anti-emetics Supportive
Myelosuppression

22
Topotecan Topoisomerase I inhibitor
Nausea/vomiting Microscopic
hematuria Fever
Anti-emetics None Anti-pyretics
Myelosuppression
Vinblastine Velban Microtubule polymerization inhibitor
Peripheral neuropathy (jaw pain, paresthesia, foot drop)
Constipation
Lower dose Stool softening regimen
Myelosuppression
Vincristine Oncovin Microtubule polymerization inhibitor
Peripheral neuropathy (jaw pain, paresthesia, foot drop)
Constipation
Lower dose Stool softeners

23
Antiemetic Management in Pediatric Oncology I. Types of Emesis Acute: Emesis occurring within 24 hours of chemotherapy administration. Occurs in 1/3 of patients despite treatment. Delayed: Emesis occurring > 24 hours after chemotherapy administration. Risk factors include: female sex, certain agents (e.g. cisplatin), prior acute emesis. High frequency of occurrence. Anticipatory: Prior to administration of chemotherapy. II. Physiology Major neurologic structures involved in chemotherapy induced nausea and vomiting (CINV) include: vomiting center (VC) in the lateral reticular formation of the medulla; chemoreceptor trigger zone (CTZ) in the area postrema of the medulla; cerebral cortex; and vagal and splanchnic afferents from the gut to the vomiting center at the CTZ.
The VC receives input from several areas including the limbic system, the chemoreceptor trigger zone, the vestibular system, and the gastrointestinal tract. Presumed sequence of events includes:
1. Chemotherapy or radiation irritates enterochromaffin cells in the gut mucosa. 2. Enterochromaffin cells are stimulated to release serotonin. 3. Serotonin activates 5-hydroxytryptamine-3 (5-HT3) receptors that have a neuronal
connection with the VC. 4. The 5-HT3 receptors stimulate either vagal afferent nerves or central receptors associated
with the VC.

24
5. The chemoreceptor trigger zone (CTZ) also sends impulses to the VC. 6. When a threshold is reached in the VC, nerve impulses travel by the vagus to stimulate
emesis.
The CTZ can be stimulated by substances either in the blood or in the cerebrospinal fluid. Input from the CTZ is fed into the VC, thereby causing neuronal activity in the periphery that result in vomiting. The cerebral cortex plays a major role in anticipatory nausea. Previous experience will influence the incidence of this type of nausea and vomiting (Adapted from Bradbury, RP, Chemotherapy Induced Nausea and Vomiting: Rationale for Cost Effective Management. Cancer Control Journal; Volume 3 (3), 1996.)
III. Listing of Agents
Antiemetic Agents
Antihistamines Dimenhydrinate (Dramamine) Diphenhydramine (Benadryl) Meclizine (Antivert) Anticholinergic agent Scopolamine (Transderm Scop) Dopamine antagonists Chlorpromazine (Thorazine) Droperidol (Inapsine) Metoclopramide (Reglan) Prochlorperazine (Compazine) Promethazine (Phenergan) Serotonin antagonists Dolasetron (Anzemet) Granisetron (Kytril) Ondansetron (Zofran) Palonosetron (Aloxi) Substance P receptor antagonist Aprepitant (Emend) Other agents Dexamethasone Methylprednisolone (Medrol) Trimethobenzamide (Tigan)
Major Adverse Effects/Other Issues of Antiemetic Agents
Antiemetic class Adverse effects/other issues
Antihistamines and anticholinergics
Sedation, urinary retention, blurred vision, exacerbation of narrow-angle glaucoma
Dopamine antagonists
Sedation, extrapyramidal effects, QT prolongation, severe hypotension; rarely, seizures, agranulocytosis, neuroleptic malignant syndrome, blood dyscrasias
Serotonin antagonists
QT prolongation, QRS widening; rarely, hypersensitivity reactions
Substance P receptor antagonists
Use in caution with agents metabolized by CYP3A4
IV. Management

25
Author’s note: Antiemetic management is not a “one size fits all” proposition. It is imperative that you think carefully about the likely etiology of nausea in the patient you’re treating. For example, CINV has an entirely different physiology from anticipatory nausea and each should be treated differently. Many of the agents utilized for CINV are extremely expensive and should be utilized thoughtfully.
Dosing guidelines are for days of chemotherapy administration only. a. Identify the most emetogeneic agent in the combination b. Assess the relative contribution of the other agents to the emetogenicity of the combination. c. When considering other agents the following rules apply: Level 1 agents do not contribute to the emetogenicity of a given regimen Level 2 agents (regardless of number) increase emetogenicity of most emetogenic agent one level Level 3 or 4 agents increase the emetogenicity of the combination by one level per agent. Numerically: 2 + 2 = 3 2 + 2 + 2 = 3 3 + 2 = 4 3 + 2 + 2 = 4 3 + 3 + 3 = 5 4 + 4 = 5 Examples: VAC: Vincristine (Level 1) Actinomycin (0.015 mg/kg, Level 3) Cytoxan (2.2 gm/m2, Level 5) Emetogenic rating: (5+3) = 5 IE: Ifosphamide (Level 3) Etoposide (Level 2) Emetogenic rating: (3+2) = 4 HD MTX: MTX (12 gm/m2, Level 4) Emetogenic rating: 4 ID Dose MTX MTX (1 gm/m2, Level 3) Emetogenic rating: 3
Emetogenicity of Common Chemotherapeutic Agents Level Frequency of Emesis (%) Agent

26
5 >90% Busulfan (BMT dosing) Carmustine >250 mg/m2 Cisplatin >50 mg/m2 Cyclophosphamide >1500 mg/m2 Dacarbazine Mechlorethamine Pentostatin Streptozocin 4 60-90 Carboplatin Carmustine < 250 mg/m2 Cisplatin <50 mg/m2 Cyclophosphamide > 750 mg/m2 to < 1500 mg/m2 Cytarabine > 1000 mg/m2 Dactinomycin > 1.5 mg/m2 Doxorubicin > 60 mg/m2 Irinotecan Melphalan (IV) Methotrexate > 1000 mg/m2 Mitoxantrone >15 mg/m2 Procarbazine (oral) 3 30-60 Aldesleukin Cyclophosphamide < 750 mg/m2 Cyclophosphamide (oral) Dactinomycin < 1.5 mg/m2 Daunorubicin Doxorubicin 20-59 mg/m2 Epirubicin Estramustine Idarubicin Ifosfamide (Level 4 if 1.5 gm/m2 or above) Methenamine (oral) Methotrexate 250-1000 mg/m2 Mitoxantrone Temozolomide (any dose) 2 10-30 Asparaginase Capecitabine Cytarabine <1000 mg/m2 Doxetaxel Doxorubicin <20 mg/m2 Etoposide Fluorouracil <10000 mg/m2 Gemcitabine Methotrexate >50 mg/m2 to < 250 mg/m2 Mitomycin Paclitaxel Teniposide

27
Thiotepa Topotecan 1 <10 Androgens Bleomycin Busulfan (low dose – not BMT) Chlorambucil (oral) Cladribine Fludarabine Hydroxyurea Interferon Melphalan (oral) Mercaptopurine Thioguanine (oral) Tretinoin Vinblastine Vincristine Vinorelbine Other non 5-HT3 antiemetics can be added as required (in particular consider Ativan) Level 5: Dexamethasone 10 mg/m2 (20 mg max dose) 30 minutes prior to Dolasetron or Ondansetron (note decadron is given once every 24 hour period) then: Dolasetron 1.8 mg/kg (100 mg max dose) IVP 30 minutes prior to chemo q24 or: Ondansetron 0.45 mg/kg (16 mg max dose) 30 minutes prior to chemotherapy then Ondansetron
0.15 mg/kg/dose at T = 6, 12, and 18 hrs. Consider aprepitant for patients refractory to the above regimen. Level 4 (including BMT patients receiving chemotherapy or TBI): Agents used for BMT dosing, despite being Level 5, are included in this category to avoid the automatic inclusion of steroids. BMT patients must be treated with Zofran to avoid QT prolongation seen with Dolasetron at high dose Dolasetron 1.8 mg/kg (100 mg max dose) IVP 30 minutes prior to chemo q24 or: Ondansetron 0.45 mg/kg (16 mg max dose) 30 minutes prior to chemotherapy then Ondansetron
0.15 mg/kg/dose at T = 6, 12, and 18 hrs (these dose may be given prn) Dexamethasone should be reserved for treatment failures. Level 3:

28
Either: Dolasetron 1.8 mg/kg (100 mg max dose) IVP 30 minutes prior to chemo q24 or: Ondansetron 0.45 mg/kg (16 mg max dose) 30 minutes prior to chemotherapy Or: Ondansetron 0.15 mg/kg (8 mg max dose) at T = -30 and then q6 hours prn Level 2 (including intrathecal chemotherapy): If required: Dolasetron 0.9 mg/kg (50 mg max dose) IVP 30 minutes prior to chemo q24 or: Ondansetron 0.15 mg/kg (8 mg max dose) T = -30 minutes only Level 1: No antiemetic routinely provided, or utilize alternate antiemetics. Non-chemotherapy associated nausea/vomiting: Dolasetron 0.35 mg/kg (12.5 mg max dose) IVP prn q8hrs

29
Pain Management in Pediatric Oncology An important component of treating pain in children is to recognize that children do have pain and that when compared to adults, children are commonly under-medicated for their pain. Many factors such as age, developmental level, fear or anxiety complicate the assessment and treatment of pain in children. Assessment Pain is defined as “whatever the experiencing person says it is, existing whenever he says it does” (McCaffery, 1968), and for the older, verbal child, self-reports of pain can be used. But for pre-verbal and neurologically impaired children, one must rely on behavioral assessments, and on parent/caregiver input. ”Soft signs” such as irritability, restlessness, poor feeding, poor sleep, decreased play, and withdrawn behaviors may signal the existence of pain in infants. For slightly older children (ages 2-6), lack of cooperation, decreased play and withdrawal may also occur with pain. Children commonly use distraction, sleep, or lying very still to avoid feeling pain, which then may lead caretakers to the erroneous conclusion that the child is not having pain. Physical signs such as tachycardia, hypertension, diaphoresis, and nausea may also be symptoms of pain, although these are not always reliable indicators as they can be associated with other variables such as fever, anxiety, etc. For children above the age of four or five, it is most important to get the child’s input using self-report pain scales. There are self-report assessment tools, such as FACES and number scales, available to measure pain in older children. In non-verbal children, caregivers can use the Observational Pain Scale or Behavioral Pain Assessment Scale, available on nursing units. Etiology Both acute and chronic pain may be present in the pediatric oncology patient. Acute pain occurs in children undergoing diagnostic procedures and treatment. Chronic pain may occur in long term survivors or in those with progression of the disease/tumor. In children, therapy-related pain is reported more commonly than cancer-related pain. Tumor related causes of pain Tumor-related pain commonly results in somatic, visceral, and neuropathic pain. Somatic pain is usually well localized and described as aching or gnawing. Examples of somatic pain include pain associated with either primary or metastatic bone disease or postoperative incisional pain. Visceral pain results from the infiltration, compression, distension, or stretching of thoracic and abdominal viscera by primary or metastatic tumor. This pain is poorly localized, often described as deep, squeezing, or pressure. It may be associated with nausea, vomiting, and diaphoresis. An example is pain associated with tumors of the liver (e.g. , hepatoblastoma) Neuropathic pain most commonly results from tumor compression, infiltration of peripheral nerves, and/or infiltration of the spinal cord. Clinical manifestations include dysesthesias with a burning and/or electrical quality, paroxysmal brief shooting or stabbing qualities, allodynia or pain that is induced by stimuli which are not normally painful. Treatment related causes of pain Postoperative pain: many oncology patients have surgery as part of their diagnosis and treatment, or to obtain central venous access. This pain is best treated with systemic opioids, or with epidural infusions of local anesthetics mixed with opioids. Phantom sensations and phantom limb pain are common in children after an amputation, and may occur days to weeks following the surgery. Drugs such as Gabapentin and/or tricyclic antidepressants may be helpful in treating phantom pain. Evidence suggests that regional

30
anesthesia prior to the amputation can prevent phantom limb pain. TENS (transcutaneous electrical nerve stimulation) has also been reported to be helpful in treating this type of pain. Therapy related toxicities: radiation and chemotherapy can cause significant mucositis. Mucositis can range from one small mouth ulcer to severe mouth, throat, and rectal sores with perianal abcess. These may also be symptoms of infection (e.g. herpetic stomatitis) and require appropriate treatment as well as pain management. The pain caused by minimal oral mucositis can be treated with a topical solution such as Larry’s solution (a mixture of viscous lidocaine, Maalox, and benadryl prepared in the pharmacy). Moderate to severe mucositis (e.g. when patients refuse to eat , cannot swallow their own secretions, or are having pain with bowel movements) is best treated with systemic opioids. A PCA pump (patient controlled analgesia) can provide a continous infusion to take the edge off the pain, with a bolus capability for exacerbations caused by mouth care, swallowing, or having a BM. Hemorrhagic cystitis: can be a complication of cytoxan or ifosfamide, associated with severe pain as blood clots are passed with the urine. Systemic pain medications along with bladder irrigation are used to treat this type of pain. Peripheral neuropathies: can occur as a result of administration of vincristine, vinblastine, cisplatin, and continuous infusion Ara-C and 5 FU. Treatment includes rest and modification of the chemotherapy. This is normally a reversible phenomenon although it may reoccur when the drug is restarted. Medications such as neurontin and tricyclic antidepressants are usually helpful in treating neuropathic pain. Medications for neuropathic pain usually require several days to start to become effective and need to be titrated to effect, usually starting with a low dose to prevent side effects like sedation. Intrathecal chemotherapy has been associated with arachnoiditis and meningeal irritation syndrome (headache, nuchal rigidity, fever, nausea, vomiting) Graft versus host disease may be associated with severe abdominal pain and cramping. Another manifestation is skin breakdown which leaves the child with pain similar to a first degree burn and may progress to sloughing of the skin. Procedure Related Pain Survivors of childhood cancer vividly recall the difficulties in experiencing repeated painful procedures. It is important to proactively manage painful procedures in children who can be expected to have repeated procedures in the course of their treatment. Adequate pain relief and sedation with initial procedures during diagnosis will set the stage for subsequent painful procedures. Needle puncture: what often does not seem like a big deal to adult caregivers is a major source of distress for children. Children need adequate preparation before their first needle stick to minimize fear and anxiety. Child life specialists are trained to provide support and coping mechanisms for children and families. Medical professionals who are accustomed to obtaining blood samples and starting IV’s on children should provide the initial needle punctures. The use of topical local anesthetic creams may be helpful for the child. Lumbar puncture: pain related to LP’s is mainly from the skin puncture and the possible inadvertent encounter with the periosteum. Topical local anesthetics may be applied as well as infiltrating local anesthetics. The main distress to the child is often related to the positioning and requirement to remain still. There is also the potential for a CSF leak to occur leaving the child with a postdural puncture headache, usually relieved with analgesics, caffeine, hydration, and positioning. Bone Marrow aspiration/biopsy: this pain is related to the insertion of a large needle into the posterior iliac space and to the unpleasant sensation experienced at the time of marrow aspiration. It is not uncommon for children to require conscious sedation or general anesthesia.

31
Children may be sedated for a painful procedure following the Children’s Center conscious sedation protocol. For children who require a deeper level of sedation, there is also a designated operating room which may be scheduled for short procedures. This room may be scheduled through the Department of Anesthesia, the phone number is 7-2637 and the contact person is Kym. Treatment Drug therapy represents the major modality in pain treatment, and may be used in conjunction with other therapies such as heat, distraction, and relaxation. For mild pain, one can start with non-opioid agents such as Acetaminophen (10 – 15 mg/kg/dose every 4 hours) or Trilisate (magnesium choline salicylate). NSAID’s are not used in oncology patients because of concerns about anti-platelet effects. Trilisate does not affect platelets. The dose of Trilisate is 30-60mg/kg/24 hours divided tid-qid. More severe pain may require the addition of opioids to the treatment regimen. Whenever possible, the oral route should be the first choice. Commonly used oral opioids include codeine and oxycodone. There are several problems with codeine – it is very nauseating for many people and 10 % of people lack the enzyme to convert it to morphine, making it ineffective in this group of patients. Oxycodone tends to cause less nausea and vomiting, so it is often the first line choice for pain that is unrelieved by peripheral agents. Both oxycodone and codeine are available in combination with Acetaminophen or as single agents. Moderate to severe pain may require treatment with stronger opioids such as morphine, dilaudid, or fentanyl. Administration of these medications by patient controlled analgesia (PCA) occurs when patients are unable to take oral meds. PCA provides the advantage of continuous low dose infusions which provide steady blood levels of opioids, therefore avoiding the peaks (sedation) and valleys (pain) associated with prn boluses of opioids. The PCA also provides bolus dosing, allowing the patient to treat episodes of “breakthrough pain” and self-medicate prior to painful events. Patients younger than 5 years may have a PCA pump, enabling parents or nurses to push the button for exacerbations of pain or prior to painful procedures. It is important to instruct parents to only push the PCA bolus when the child is awake. Pushing the bolus for a sleeping child can be unsafe. Opioids can be associated with annoying side effects: itching, nausea, vomiting, drowsiness, and urinary retention. Usually, these side effects lessen over time. Other medications, dose reduction, or opioid switch may be used to treat these side effects. Studies have shown that low dose Naloxone (Narcan) infusions are effective in decreasing itching and nausea/vomiting. Constipation is the side effect that does not improve with time or dose reduction. Constipation with opioid use must be anticipated and best treated with prevention. Therefore, opioids and stool softeners/laxatives should be prescribed together. Alternatively, patients with diarrhea will benefit from the constipating effects of opioids. An alternative method to provide analgesia is to use an epidural catheter for the delivery of extradural opioids and/or local anesthetics to treat surgical pain, and some types of cancer pain that are unresponsive to standard opioid analgesia. In terminally ill children, an epidural catheter can be tunneled subcutaneously to allow for the catheter to remain in place for long term use. Patients with tunneled catheters may be discharged to home. General Guidelines: 1. Determine the cause/source of pain in order to choose the correct treatment or medication.

32
2. Remember that marked individual variations exist in dosing requirements 3. Doses should be titrated to clinical effectiveness or as limited by side effects such as sedation, respiratory depression, vomiting, or pruritis. 4. When converting from one medication to another, or one route to another, equipotent analgesic conversions should be used. There are conversion tables available to do this (two are included with this handout). 5. When appropriate, give medications “around the clock (ATC)” rather than “prn”. Try not to get behind, as the best method of pain control utilizes prevention. Long term chronic pain or pain associated with terminal illness is also found in the pediatric oncology population. There are other medications that may be used to treat this type of pain. Sustained release opioid preparations are useful when severe ongoing pain is anticipated. Medications such as Oxycontin and MScontin can be administered BID or TID to provide for easier dosing at home, and allow an uninterrupted night of sleep. These sustained release forms may be supplemented with short-acting opioids for breakthrough pain. The patient must be able to swallow an intact pill to be able to use sustained release medications as they cannot be broken, crushed, or chewed for reasons of safety. These opioids must be titrated to effect with a minimum of side effects, and as pain improves, they can be weaned. Methadone is a very effective long-acting opioid. Unfortunately, because methadone use is associated with drug addiction and maintenance programs, some people are hesitant to use it in appropriate chronic pain patients. Methadone use in cancer pain is both advocated and discouraged. Unlike many other opioids, methadone is an opioid agonist and an NMDA receptor antagonist. This dual activity may improve pain control and may be effective in treating neuropathic pain, reducing opioid requirements and tolerance. It can be used for severe ongoing pain, is usually effective BID or TID, comes both orally and parenterally, and is available in liquid and pill form. Therefore, it can be taken by children who are unable to swallow pills. The disadvantage of methadone is its long and variable elimination half-life which may result in drug accumulation and make titration difficult. It is important to discuss the social stigma of methadone use with patients and families. Another available alternative in certain patient populations is the Fentanyl transdermal patch (Duragesic). Fentanyl patches are useful in situations where the oral route is unavailable. Fentanyl patches provide continuous release of analgesic over a 72 hour period. Because of concerns regarding overdosage, it is recommended that they not be used in opioid naïve patients. The disadvantage of the Fentanyl patches is that the smallest dose available is 25 mcg which dispenses 25 mcg per hour for 72 hours, and the patches can not be cut. Therefore, it may be impossible to dose pediatric patients who do not meet the weight requirement, although opioid tolerant children may be able to use the patches. Additionally, weaning off the patches may be difficult in patients who are extremely opioid sensitive. OPIOID DEPENDENCE All opioids used consistently over extended periods of time can cause physical dependence and tolerance. In many situations, patients may need to be weaned from the medication or may need higher doses to achieve the same effect. This does not mean that they are psychologically “addicted” to opioids. The Pediatric Pain Service can provide weaning schedules or guidance

33
for weaning as needed. Typically, when clinical conditions improve and the patient’s pain is decreasing, the opioid can be weaned approximately 10-20% every other day, depending on how long they were on the opioid. If the patient is not weaned, they can experience unpleasant withdrawal symptoms including abdominal pain, vomiting, diarrhea, tremors, irritability, sweating, sneezing, rhinorhea, fever, difficulty sleeping, poor feeding, inability to keep still, and potential seizures. Withdrawal symptoms may also occur if benzodiazepines are abruptly stopped. These symptoms are similar to opioid withdrawal but may be life-threatening. Table 8-2 Commonly Prescribed Liquid Analgesics Drug How supplied Dose Mg/kg Acetaminophen drops 80 mg/0.8 ml 10-15 Acetaminophen solution 160 mg/ml 10-15 Acetaminophen elixir 80, 120, 130, 160, 325 mg/5ml 10-15 Codeine syrup 10, 60 mg/5ml 0.5-1.2 Codeine Solution 15 mg/5ml 0.5-1.2 Acetaminophen + codeine elixir or solution
120 mg acetaminophen +12 mg codeine/5 ml
Based on codeine
Acetaminophen + hydrocodone suspension
120 mg acetaminophen + 2.5 mg hydrocodone/5ml
Based on hyrocodone
Ibuprofen suspension 100 mg/5ml 4-10 Meperidine elixir 50mg/5ml 1-1.5 Methadone solution 5, 10 mg/5ml 0.1 Morphine solution 10, 20, 100 mg/5ml 0.1
Table 3-4. Equianalgesic Opioid Doses Name
Equipotent IV Dose (mg/kg)
Equipotent PO Dose (mg/kg)
Parenteral/ Oral Ratio
Alfentanil • 0.05 - -
Butorphanol 0.01-0.02 0.05* 25%
Codeine 1.2 2.0 66%
Fentanyl
0.001
0.01-0.015t transmucosal
25-50% of transmucosal doset
Hydromorphon 0.015 0.02-0.1 20-70%
Meperidine 1.0 1.5-2.0 50-60%
Methadone 0.1 0.1 100%
Morphine 0.1 0.3-0.5 20-33 %
Nalbuphine 0.1 0.5 20%
Oxycodqne - 0.1 -
Sufentanil 0.0001 - .

34
Table 8-1 Relative potencies of Intravenous Opioids Drug IV dose (mg/kg/) Frequency (hours) Ratio of equivalence
to morphine Morphine 0.1 2-4 1 Fentanyl 0.001 1-2 80-100 Hydromorphone 0.0015 3-4 5-7 Meperidine 1.0 2-4 0.1 Methadone 0.1 4-12 1 From- Pediatric Pain Management and Sedation Handbook Editors Myron Yaster MD, Elliot Krane MD, Richard Kaplan MD, Charles Cote MD, and Dorothy Lappe RN, MS, MBA

PEDIATRIC ONCOLOGY 2008-2009 PHARMACOTHERAPY DOSING GUIDELINES
Pharmacotherapy in pediatric oncology and stem cell transplant patients can differ from the established standards due to the variability of pharmacokinetic and pharmacodynamic properties in immunocompromised patients. The following dosing guidelines are specific for the pediatric oncology population at the Johns Hopkins Hospital and have been reviewed by pharmacy and pediatric oncology. Please make every effort to update these recommendations as new information becomes available. Guidelines do not contain doses for medications in organ dysfunction. Please contact pharmacy for dosing recommendations.
KEY: * All doses are intravenous unless otherwise indicated Underlined drugs = pharmacokinetically monitored drugs †: Indicates drugs that require ID approval for inpatient pediatric oncology use NF: nonformulary medications ELIM = primary route of elimination R= renal excretion H= hepatic excretion U= unknown route of elimination O= other

36
ANTIBIOTICS
DRUG DOSE USE ELIM MONITORING PARAMETERS
Amikacin < 12 yo: 7.5 mg/kg/dose IVq8h > 12 yo: 5 mg/kg/dose IV q8h
Gram - R BUN/creatinine, peak (20-30 mcg/ml) and trough (< 10 mcg/ml) obtained per therapeutic drug monitoring nomogram, trough weekly to check for toxicity Extended interval dosing: trough ONLY ; < 4 mcg/ml
Extended interval dosing*: 15-22.5 mg/kg/dose IV every 24 hours *not appropriate for patients with renal impairment; verify appropriateness prior to initiating therapy
Atovaquone 1-3 mo and >24 mo: 30 mg/kg/day po daily 4-24 mo: 45 mg/kg/day po daily Adolescents/adults: 1500 mg po daily
PCP prophylaxis- Alternative to Bactrim
R Rash, pruritis, hyponatremia, n/v/d, elevated amylase, neutropenia, elevated LFT’s
Azithromycin † 5-10mg/kg/dose IV/po q24h Atypicals, anaerobes, Some gram +/-
H Drug interactions with other cytochrome P450 medications
Aztreonam† 50 mg/kg/dose IV q8h max = 8 grams/24 hours
Gram - R BUN/creatinine, LFT
Cefepime† 50 mg/kg/dose IV q8h max = 6 g / 24 hours
Gram +/- R BUN/creatinine, LFT
Cefixime† 4 mg/kg/dose po bid max = 400 mg/day
Gram +/- R BUN/creatinine, LFT
Cefpodoxime†,NF 5 mg/kg/dose po BID max = 800mg/24 hours
Gram +/- R CBC/diff, PT/PTT, LFT, BUN/creatinine
Ceftriaxone 75 mg/kg/dose IV/IM q24h max = 2 g/dose and 4 g / 24 hours
Gram +/- R BUN/creatinine, LFT, CBC/diff
Clindamycin 10 mg/kg/dose IV q6h max = 4.8 g / 24 hours
Gram +, anaerobes H BP, skin rash, CBC/diff, LFT
Dapsone ≥ 1 mo: 2 mg/kg/day po daily (max dose = 100 mg/day) OR 4 mg/kg/dose po once weekly (max dose = 200mg) Adolescents/adults: 100 mg po daily
PCP prophylaxis- Alternative to Bactrim
R Hemolytic anemia, methemoglobinemia, neutropenia, N/V, LFT elevations, ATN, photosensitivity Caution in patients with G-6-PD deficiency
Gentamicin > 50 kg: 2 mg/kg/dose IV q8h < 50 kg: 2.5 mg/kg/dose IV q8 hours
Gram - R BUN/creatinine, peak (6-10 mcg/ml) and trough (< 2mcg/ml) obtained per therapeutic drug monitoring nomogram, trough weekly to check for toxicity
Imipenem/cilastatin†,NF (Primaxin)
60-100 mg/kg/day IV divided q6-8h Max = 1 gram/dose or 4gram/24 hours
Gram - R BUN/creatinine, seizures
Linezolid † < 12 yo: 10 mg/kg/dose po/IV q8h >12 yo: 600 mg po/IV q12h
VRE R/U LFT, CBC/diff, lactic acidosis
Meropenem† 20-40 mg/kg/dose IV q8h Max = 6 gram/24 hours
Gram +/-, anaerobes R BUN/creatinine, LFT
Metronidazole 7.5 mg/kg/dose IV/po q6h max = 4 grams/24 hrs
Anaerobes R/O CBC, discoloration of urine
Norfloxacin > 12 yo: 400 mg po BID (<12 yo: 9 mg/kg/day po divided BID; not to be used for routine BMT prophylaxis)
Gram – (BMT prophylaxis)
R
Oxacillin 50 mg/kg/dose IVq6h Gram + R BUN/creatinine, LFT, Serum sodium, CBC/diff

37
max = 12 gram/24 hours Penicillin 50,000 units/kg/dose IV q6h Gram + (BMT
prophylaxis) R BUN/creatinine, electrolytes
Pentamidine 4 mg/kg/dose IV every month (LAST LINE) PCP prophylaxis R BUN/creatinine, CBC, BP Piperacillin/tazobactam 100 mg/kg/dose IVq6-8h
Max = 4.5 grams/dose or 18 grams/24 hrs Gram +/- R BUN/creatinine, electrolytes, CBC
Sulfamethoxazole/ trimethoprim
5 mg TMP/kg/day po divided BID x 3days/wk Post-BMT = 5 mg TMP/kg/day po divided BID x 2days/wk Max = 320 mg TMP and 1600 mg SMZ / 24 hours
PCP prophylaxis- GOLD STANDARD
R BUN/creatinine, CBC, LFT
5 mg TMP/kg/dose IV q6-8h (treatment) Gram - Tobramycin > 50 kg: 2 mg/kg/dose IV q8h
< 50 kg: 2.5 mg/kg/dose IV q8h Gram - R BUN/creatinine, peak (6-10 mcg/ml) and trough (<2
mcg/ml) obtained per therapeutic drug monitoring nomogram, trough weekly to check for toxicity
Vancomycin† 12.5 mg/kg/dose IV q8h Gram + R BUN/creatinine, trough (5-20 mcg/ml) obtained per therapeutic drug monitoring nomogram then weekly; peaks not recommended unless meningitis

38
ANTIFUNGALS
DRUG DOSE ELIM MONITORING PARAMETERS
Amphotericin B 0.5-1.5 mg/kg/dose IV q24h R BUN/creatinine, potassium, magnesium, LFT, CBC AmBisome† 3 mg/kg/dose IV q24h (empiric)
5 mg/kg/dose IV q24h (treatment) Prophylactic regimen: 1-3 mg/kg/dose IV three days/week
Caspofungin† 70 mg/m2/dose x 1 on day 1, max 70 mg then 50 mg/m2/dose IV q24h, max 50 mg
H Hepatic function
Fluconazole
Prophylaxis: 5 mg/kg/day IV/po q24h max = 400 mg Treatment: 10 mg/kg/day IV/po q24h Max = 800 mg
H BUN/creatinine, LFT, CBC
Itraconazole 5-10 mg/kg/day po Q24h or divided BID Max = 600 mg/day in 3 divided doses
H LFT, bilirubin, BUN/creatinine
Voriconazole † IV: 6 mg/kg/dose IV q12h X 2 doses, then 4 mg/kg/dose IV q12h PO: <15 kg = 50 mg po BID 15-25 kg = 100 mg po BID 25-40 kg = 150 mg po BID >40 kg = 200 mg po BID
H LFT, bilirubin, BUN/creatinine (IV), vision changes

39
ANTIVIRALS
DRUG USE DOSE ELIM MONITORING PARAMETERS
Acyclovir CMV prophylaxis 500 mg/m2/dose IV q8h 800-3200 mg/24 hr po divided q6 hours
R BUN/creatinine, LFT, CBC, phlebitis
HSV prophylaxis 250 mg/m2/dose IV q12h 80 mg/kg/day po divided q6 hours
HSV infection IV: 250 mg/m2/dose IV q8h PO: 200 mg q4h while awake (5X/day)
VZV infection IV: 500 mg/m2/dose IV q8h PO: 20 mg/kg/dose q6h Max = 3200 mg/day
Cidofovir Adenovirus infection 5 mg/kg/dose IV once weekly until PCR negative *Must give probenecid to decrease nephrotoxicity **Dose can be decreased based upon renal function Alternative regimen in renal dysfunction: 1 mg/kg/dose IV three times weekly
R BUN/creatinine, adenoviral cultures/PCR,
CMV Immune Globulin † CMV infection (use with ganciclovir)
400 mg/kg IV on days 1, 2, and 7, then 200 mg/kg IV on days 14 and 21
U CMV quantitative PCR, BP, HR, temp
Famciclovir † HSV infection >12 yo: 500 mg po q8h < 12 yo: 6 mg/kg/dose po q8h (max 500 mg po q8h)
R Resolution of rash, BUN/creatinine
Ganciclovir † CMV infection Induction: 5 mg/kg/dose IV q12h x 14-21days Maintenance: 5 mg/kg/day IV q24h
R CBC/diff, UOP, BUN/creatinine
Oseltamivir (ID approval required if outside of influenza season)
Influenza treatment ≤ 15kg: 2 mg/kg/dose (max dose: 30mg) po BID x 5 days > 15 kg-23 kg: 45 mg po BID x 5 days > 23 kg-40 kg: 60 mg po BID x 5 days > 40 kg: 75 mg po BID x 5 days
R Influenza culture, rash, CBC, LFT
Palivizumab † RSV prophylaxis 15 mg/kg IM once monthly during RSV season (indicated for those patients ≤ 2 yo with high risk features)
U LFT, rash
Ribavirin † RSV treatment 2g inhaled over 2 hrs three times daily H/R RSV positivity, BP, rash, CBC Valacyclovir † HSV infection To mimic an IV acyclovir regimen of 250 mg/m2/dose:
30 mg/kg/dose po TID (max = 1000 mg po TID) To mimic a PO acyclovir regimen of 20 mg/kg/dose 4 or 5X/day: 20 mg/kg/dose po TID (max = 750 mg po TID)
R BUN/creatinine, CBC, UA, LFT
Valganciclovir † CMV prophylaxis 15 – 18 mg/kg/dose po daily, max dose = 900 mg po daily (One case report suggests 15 mg/kg/dose po BID for treatment)
R

40
OTHER DRUGS
DRUG DOSE USE MONITORING PARAMETERS Allopurinol PO (preferred): 10 mg/kg/day in 3 divided doses
Max dose = 800 mg/day Decreases uric acid Renal function, uric acid, calcium, phosphate, CBC, LFT
IV: 200-400 mg/m2/day in 3 divided doses Max dose = 600 mg/day
Aminocaproic acid Load: 100-200 mg/kg/dose po/IV Maintenance: 100 mg/kg/dose q6h Max dose = 30 grams per day
Hemostatic Fibrinogen, fibrin split products, potassium, renal function
Amlodipine Initial: 0.1 mg/kg/day, titrate to response Max dose = 10 mg/day
Antihypertensive BP, headache, rash, CBC, LFT’s
Aprepitant 125 mg po on day 1 given one hr prior to chemo, then 80 mg given one hr prior to chemo on days 2 and 3 *not appropriate for every patient **Should be used in combination with dolasetron/ondansetron/granisetron AND dexamethasone
Prevention of chemotherapy-induced nausea and vomiting with highly emetogenic regimens
Drug interactions, LFT’s, nausea and vomiting, somnolence and fatigue Check chemotherapy protocol before using to see if aprepitant is contraindicated
Beclomethasone 4 mg po q6h Gastrointestinal GvHD Not readily absorbed (topical administration in the gut)
Cyclosporine IV/PO: per patient specific roadmap and based upon serum cyclosporine levels **Brands are NOT INTERCHANGEABLE** Sandimmune is the product dispensed when cyclosporine is written unless MD specifies Neoral in order; always specify Brand and write “Brand Necessary” on discharge prescriptions
Immunosuppressant Cyclosporine levels (trough, usual goal 150-300 ng/ml), renal function, bilirubin, potassium, magnesium, BP, tremors, seizures, headache, lipid panel
Darbepoetin Initial: 2.25 mcg/kg/dose SC q2wks (may titrate q 6 wks; max of 4.5 mcg/kg/dose)
Chemotherapy induced anemia
Hgb/Hct, BP, seizures, back pain, limb pain, flu-like symptoms
Dexamethasone Initial: 10 mg/m2/dose IV Maintenance: 5 mg/m2/dose IV q6h Max dose = 20 mg/dose
Antiemetic for chemotherapy-induced nausea and vomiting
BP, potassium, serum glucose, N/V
Dolasetron IV: 1.8 mg/kg/day 30 min before chemo Max dose = 100 mg
Antiemetic HR, headache, N/V
PO: 1.8 mg/kg PO within 1 hr before chemo Max dose = 100 mg
Enoxaparin Prophylaxis: 0.5 mg/kg/dose SC q12h Treatment: 1-1.5 mg/kg/dose SC q12h
Anticoagulant Antifactor Xa levels, CBC, LFT’s
Filgrastim (G-CSF) IV/SC: 5-10 mcg/kg/dose q24hours (protocol specific)
Colony stimulating factor CBC with differential, LFT, bone pain, fever
GranisetronNF IV: 10-20 mcg/kg/dose q 12 h Max dose = 2 mg/day
Antiemetic N/V, LFT’s, headache, BP, HR
Immune globulin 400-500 mg/kg/dose IV every 3-4 weeks BMT patients Infusion related reactions, n/v, BP, acute renal failure Leuprolide (Lupron) Monthly regimen:
Lupron Depot 3.75 mg IM q month Every 3 month regimen:
GnRh agonist (used in pediatric oncology for menstrual suppression)
Rash, acne, vaginal bleeding, gynecomastia, headache, fever, weight gain, skin striae

41
Lupron Depot 11.25 mg IM q 3 months Mycophenolate mofetil IV/PO: 600 mg/m2/dose Q12h
(Dose may be given as frequently as q6h based upon drug concentrations)
Immunosuppressant CBC, LFT, UA, renal function, BP, phosphate, potassium, N/V, GI upset, mycophenolate levels (trough)
Ondansetron IV: 0.15-0.45 mg/kg/dose 30 min before chemo then 0.15 mg/kg/dose q6h prn (max = 32mg/day)
Antiemetic HR, headache, N/V
PO: based on BSA <0.3 m2: 1 mg po TID prn 0.3-0.6 m2: 2 mg po TID prn 0.6-1m2: 3 mg po TID prn > 1m2: 4-8 mg po TID prn
Pamidronate Hypercalcemia of malignancy: 0.5-1 mg/kg/dose IV once (max dose = 90 mg) Dose may be repeated in 7 days if no effect Prevention of steroid induced osteoporosis: 1 mg/kg/dose IV q3months
Hypercalcemia of malignancy; prevention of steroid induced osteoporosis
HR, BP, seizures, electrolytes (Calcium, phosphate, potassium, magnesium), N/V, bone pain, osteonecrosis of the jaw
Probenecid 1-1.25g/m2/dose 3hrs before, and 1 and 8 hrs after end of cidofovir infusion **round dose to nearest 250mg Alternative dosing strategies: 2 g/m2 3 hrs before, then 1g/m2/dose at 1 and 8 hrs after infusion
Decreases nephrotoxicity a/w cidofovir
GI upset, CBC, BUN/creatinine, LFT, rash (avoid penicillins with probenecid use- increase seizure potential)
Rasburicase > 30 kg: 3 mg IV x 1 15-30 kg: 1.5 mg IV x 1 < 15 kg: 0.1 mg/kg IV x 1
Decreases uric acid Uric acid (must send on ice following rasburicase for 24-48 hours), SCr
Sirolimus 1 mg/m2/dose po q24h Immunosuppressant Sirolimus level (trough), BUN/creatinine, LFT, CBC, lipid panel, pulm function
SSKI drops (potassium iodide)
1 drop (1 drop = 50mg) po BID to start 24 hrs prior to MIBG scan and continue for 6 days post-MIBG scan
Prophylaxis for MIBG scan Diarrhea, skin rash, hypersensitivity reactions, nausea
Tacrolimus IV: 0.05-0.1mg/kg/day Immunosuppressant Tacrolimus levels (trough), LFT’s, BUN, serum creatinine, potassium, glucose, BP, neurotoxicity
PO: 0.15-0.4 mg/kg/day divided Q12H TOBI nebs ≥ 6 yo and adult: 300 mg INH q12h in repeated
cycles of 28 days on, 28 days off < 6yo: 40-80 mgh IN q12h in repeated cycles of 28 days on, 28 days off
Respiratory prophylaxis for high risk patients
Voice alteration, bronchospasm, dyspnea, increased cough, pharyngitis, hoarseness, tobramycin trough level (only if renal dysfunction)
Ursodiol 10 mg/kg/dose po TID TPN-induced cholestasis LFT, abdominal pain, rash
CONVERSION FACTORS (IV TO PO)
DRUG IV DOSE ORAL DOSE Cyclosporine 1 3-4 (Sandimmune)
2-3 (Neoral) Mesna 1 2 Mycophenolate mofetil 1 1 Tacrolimus 1 2

42
THERAPEUTIC DRUG MONITORING
DRUG WHAT TO DRAW WHEN TO DRAW
GOAL IN RELATION TO DOSE STEADY STATE LEVELS REACHED
Amikacin Peak 0.5 hours after completion of infusion
With third dose; not necessary to draw levels for empiric neutropenic fever unless renal dysfunction, positive culture for gram
negative organism, or amikacin therapy planned for more than 48 hours
20-30 mcg/ml
Trough Immediately prior to dose administration <10 mcg/ml
Busulfan Multiple levels drawn from
opposite lumen of drug administration
Per protocol n/a
Carbamazepine Trough Immediately prior to dose administration 1-3 days 4-12 mg/L
Cyclosporine
Trough, drawn from opposite lumen of drug administration
Immediately prior to dose administration
2-3 days after changes made
*150-300 ng/ml (*patient and protocol specific)
Random, drawn from opposite lumen of drug administration
Continuous infusion: Stop infusion, remove tubing. Wait 15 minutes; draw random cyclosporine level from OPPOSITE lumen. Resume new infusion through the infusion lumen.
300-400 ng/ml
Digoxin Trough Immediately prior to dose administration Variable, 5-7 days 0.8-2 ng/ml Enoxaparin Anti-Xa level 4-6 hours after SC injection 6-24 hours 0.5-1 unit/ml
Gentamicin Peak 0.5 hours after completion of infusion
With third dose; not necessary to draw levels for empiric neutropenic fever unless renal dysfunction, positive culture for gram
negative organism, or amikacin therapy planned for more than 48 hours
4-12 mcg/ml
Trough Immediately prior to dose administration 0.5-2 mcg/ml Phenobarbital Trough Immediately prior to dose administration 7-14 days 15-40 mcg/ml
Phenytoin Trough Immediately prior to dose administration 3-5 days Total 10-20 mcg-ml
Free 1-2 mcg/ml Sirolimus Trough Immediately prior to dose administration 3-10 ng/ml
Tacrolimus Trough, drawn from opposite lumen of drug administration
if IV Immediately prior to dose administration 24-48 hours 5-10 ng/ml
Methotrexate Multiple levels Per protocol Per protocol
Mycophenolate mofetil Trough, drawn from opposite lumen of drug administration
if IV Immediately prior to dose administration 48-72 hours
MPA 1.0-3.5 (active) MPAG 35-100
Tobramycin Peak 0.5 hours after completion of infusion
With third dose; not necessary to draw levels for empiric neutropenic fever unless renal dysfunction, positive culture for gram
negative organism, or amikacin therapy planned for more than 48 hours
4-12 mcg/ml
Trough Immediately prior to dose administration 0.5-2 mcg/ml
Vancomycin Peak
1 hour after completion of infusion (not necessary to check unless concerned about CNS
penetration, ie. meningitis) 24-48 hours, depending on renal function 25-40 mcg/ml
Trough Immediately prior to dose administration 5-15 mcg/ml Valproic Acid Trough Immediately prior to dose administration 48-72 hours 50-100 mcg/ml

Transfusion Support and Complications Basic principles Transfusion support is an essential component of pediatric oncology care. The underlying disease, treatment, and even supportive care frequently cause anemia, thrombocytopenia, neutropenia, and, although less frequently, coagulopathy. Patients need a current type and screen (usually sent every three days) to receive red blood cells. Anemia Most patients receiving intensive chemotherapy will need transfusions of packed red blood cells (PRBC). Growth factor support (erythropoetin or darbopoetin) is used less frequently in pediatric oncology, but has been shown to reduce the frequency of transfusions in adult. All pediatric patients should receive leukoreduced, irradiated PRBC, typically 10 – 20 ml/kg. Each 5-6 ml/kg should raise the hemoglobin by about 1 g/dl. The amount of blood transfused should be rounded to the nearest unit (typically 250 to 350 ml) except in small children (<15 kg). Blood should be transfused at 1 to 4 ml/kg/hr depending on the degree of anemia and cardiac status of the patient The transfusion threshold varies from patient to patient. Patients may be transfused if they have symptoms attributed to anemia (headache, fatigue, shortness of breath, decreased exercise tolerance), but these symptoms are often multifactorial. Most patients will be transfused for a hemoglobin <7 g/dl and many for a hemoglobin <8 g/dl. Some patients after bone marrow transplant may need special products like CMV negative blood depending on their CMV status and specific treatment plans. Thrombocytopenia In general, stable patients are transfused for a platelets count of <10,000/ul, patients with fever, sepsis, severe mucositis, or on amphotericin B for a platelet count of <20,000/ul, and bleeding patients for a platelet count of <50,000/ul. Patients usually need to have a platelet count of >50,000/ul for lumbar puncture and >75,000/ul for surgery. All oncology patients receive single donor platelets. These platelets are collected by apheresis and should contain a minimum of 3.0 x 1011 platelets. This is equivalent to 4 or 5 units of platelets. The formula to calculate the expected increment in platelet count is units of platelets/ Body Surface Area (in m2) * 10,000 to 15,000. A simpler approach is to transfuse the equivalent of 1 unit of platelets per 10 kg of weight. A platelet count should be sent 1 hour after platelet transfusion at least once a week to evaluate the increment. The necessary frequency of platelet transfusion depends on a number of factors that affect platelet survival. Platelet survival is decreased in patients with fever, splenomegaly, bleeding, infection, disseminated intravascular coagulation, or HLA or platelet specific antibodies. Dr. Platelet will order an HLA quick screen once a week in hospitalized patients receiving platelets. This evaluates for HLA specific antibodies, a problem that can be overcome by selecting HLA matched platelets. Patients without these problems may only need platelets once or twice a week as the half-life of platelets is 4 to 5 days. However, many patients after bone marrow transplantation or with complications will need platelets on a daily basis. For patients with active bleeding and refractory to platelet transfusion other possible interventions include transfusing PRBC to increase the hematocrit >30%, epilson-aminocaproic acid (Amicar), corticosteroids, conjugated estrogens, progesterones, and activated Factor VIIa. These interventions are used infrequently. Coagulopathy Treatment of coagulopathy depends on the etiology. Some conditions, i.e. vitamin K deficiency, resolve with treatment of the underlying problem, but may still require blood product support in the short term. Fresh frozen plasma (FFP) contains 1 unit/ml of most coagulation

44
factors while cryoprecipitate contains high levels of fibrinogen, Factor VII and XIII, and von Willebrand’s Factor. FFP is usually dose at 10 to 15 ml/kg while cryoprecipitate is used mostly in patients with hypofibrinogenemia and bleeding. Each unit of cryoprecipitate per 10 kg will increase the fibrinogen by 40 to 50 mg/dl. Granulocytes Granulocyte transfusions are occasionally used as a bridge to neutrophil recovery in profoundly neutropenic patients with progressive infection on appropriate antibiotics. They are collected by apheresis from volunteer donors of the same blood type. The donors receive dexamethasone to increase the number of granulocytes in the peripheral blood and therefore collected. Some donors are collected after G-CSF stimulation of granulocytes on a research study. Granulocytes need to be transfused without 6 hours, so they are released before repeat infectious disease testing is completed. Reactions to granulocyte transfusions are common and include fever and chills in 10 to 50% and mild to moderate pulmonary edema in 5 to 10%. Severe pulmonary toxicity occurs in about 1% and may be related to concurrent administration of amphotericin B. Amphotericin B should not be administered within 6 hours of a granulocyte transfusion. Premedications are commonly used for granulocyte transfusions including acetaminophen, diphenhydramine, and hydrocortisone 1 mg/kg. A separate consent is needed for granulocyte transfusions. Adverse Reactions Transfusion reactions are the most common adverse effect from blood transfusion. Mild reactions include fever with febrile non-hemolytic transfusion reactions in 0.5% of RBC transfusions and 18% (2% severe reactions in oncology patients) of platelet transfusions. Allergic reactions occur with 0.1 to 0.2% of PRBC and 0.3 to 0.4% of platelet or plasma transfusions (per unit). These reactions cause urticaria and less frequently wheezing, respiratory distress, or hypotension. The blood bank should be contacted about reactions as well as treating the allergic reaction with antihistamines, corticosteroids, and if necessary inhaled albuterol and subcutaneous epinephrine. Other serious transfusion reactions and the most concerning infectious complications are described in the table. Other serious complications include graft versus host disease (prevented by irradiating all cellular blood products for oncology and other immunosuppressed patients), acquisition of CMV and EBV infection (reduced by leukodepletion of cellular blood products, and other rare infections (West Nile Virus, HTLV-1 & 2, malaria, babesiosis, leishmaniasis, lyme disease, brucellosis, toxoplasmosis, and Chagas disease.
Consent

45
A separate consent is needed for blood products and should be completed at the time of diagnosis of all pediatric oncology patients. It needs to be renewed on a yearly basis. The consent discussion should emphasize the risks (transfusion reactions, alloimmunization, and transmission of infections), alternatives (hematopoetic growth factors, pharmacological agents to decrease bleeding), and benefits (improved energy and activity, decreased risk of life threatening bleeding, ability to support more intensive therapy)

46
Pediatric BMT 1. Important distinctions in BMT The ideal one-line patient identification captures the following information plus the primary diagnosis, status of disease, and day post-transplant, and very efficiently gets everyone on the same page. Example: John is day +6 after non-ablative matched sibling BMT for CML in first chronic phase, or Sue is at day -3 before autologous PBSCT for stage IV neuroblastoma in first very good partial response. a. Ablative vs. non-ablative Traditional marrow transplants are myeloablative because the procedure starts with ablation of the recipient’s diseased marrow with high-dose chemotherapy or chemotherapy plus total body irradiation (TBI). A newer alternative approach is non-myeloablative (non-ablative for short), where the preparative regimen does not destroy the marrow, but provides sufficient immune suppression to prevent the recipient from rejecting the marrow graft; the marrow graft then must compete with the host marrow. Non-ablative preparative regimens are useful when the disease is not sensitive to high-dose chemotherapy or radiation (e.g. when the purpose of the transplant is to provide adoptive immunotherapy, or for non-malignant disease) and when the patient would not tolerate a standard ablative regimen (e.g. when there is organ dysfunction or uncontrolled infection). b. Autologous vs. allogeneic Autologous transplants are done by storing the patients own marrow stem cells and progenitor cells, and thawing and reinfusing them after the patient has received the high-dose therapy. This approach is allows dose escalation of effective chemotherapy (and/or radiation) to levels that would cause lethal marrow toxicity. Disadvantages include the possibility of contamination of the marrow graft with malignant cells and the lack of an immunologic graft vs. tumor effect. Advantages are no risk for graft rejection or life-threatening graft-vs-host disease (GVHD). Allogeneic transplants are done by harvesting the graft from a healthy donor. Unfortunately, many people do not have a well matched donor; for some diseases, the additional risks associated with allogeneic BMT offset any benefit of using cells from a healthy donor. Immune reconstitution is faster after autologous transplantation, and occurs in 4 – 6 months, as compared to 12 – 24 months after allogeneic BMT. Patients with active GVHD are at extremely high risk for opportunistic infection. c. HLA-identical vs. matched vs. mismatched The type of match is crucial for allogeneic transplant outcomes. The major histocompatibility antigens in humans are the HLA (human leukocyte antigens), which are encoded in a closely linked complex on chromosome 6. Therefore, people inherit HLA as haplotypes from each parent, with a recombination rate of ~1%, so each full sibling has a 25% chance of having inherited the same haplotypes from each parent as the patient. Such matches are called genotypically HLA identical. This is a favorable situation because these patients have a low risk of severe GVHD, but still have a significant graft-vs.-leukemia effect that reduces the risk of relapse compared with identical twins. Family members other than full siblings may be haploidentical, meaning that they inherited one haplotype in common with the recipient, and may match at additional HLA antigens by chance. Unrelated donors who are sufficiently well matched may be identified from among volunteer registries that have enrolled millions of people willing to donate marrow anonymously. Even when donors are fully phenotypically matched to the recipient, the risks of graft rejection and GVHD are higher than after genotypically HLA-identical BMT. Related donors who are mismatched for a single HLA antigen produce acceptable results that are indistinguishable from the results of fully phenotypically matched unrelated donors. d. PBSC vs. marrow vs. cord

47
The graft must contain stem cells (which give rise to all lineages of blood cells and last a lifetime), progenitor cells (which proliferate rapidly and provide rapid hematologic recovery), and lymphocytes (which provide more rapid immune reconstitution and help prevent rejection and relapse, but can cause GVHD). The traditional graft consists of marrow harvested by repeated aspiration from the hips. Alternatively, stem and progenitor cells can be mobilized from the marrow to the peripheral blood by chemotherapy or hematopoietic growth factors, such as G-CSF, where peripheral blood stem cells (PBSC) can be collected by leukapheresis, much like a platelet donation. PBSC are richer in progenitor cells and T cells than marrow, and therefore are associated with faster hematologic recovery but a greater risk of chronic GVHD in the allogeneic setting. Placental blood is rich in cells with tremendous marrow reconstituting activity per cell, and instead of being discarded, can be harvested from the cord at delivery and cryopreserved, either for private use or to supply unrelated cord blood registries. e. Processed vs. unprocessed The graft may be processed 1) to eliminate red blood cells or plasma to prevent hemolytic reactions if the donor is ABO mismatched; 2) to eliminate T cells to prevent GVHD, but then the pace of immune reconstitution is slower, and the risks of opportunistic infection and of relapse increase; or 3) to eliminate tumor cells, but it is possible that the risk of relapse is related more to tumor cells in the body than in the graft. 2. The expected course: common problems & when they occur a. Immediate preparative regimen toxicities Nausea & vomiting: BMT preparative regimens are highly emetogenic. For the first 3 wks after BMT, residual nausea & vomiting is frequently due to mucositis, as the tenacious mucus that is swallowed is nauseating. Hemorrhagic cystitis: associated with acrolein metabolite of cyclophosphamide, particularly in the presence of viral infection with adenovirus or BK virus, which have tropism for uroepithelium. Incidence is reduced to 10% by forced hydration combined with either Mesna (which binds the acrolein) or a 3-way irrigating foley catheter. SIADH: high-dose cyclophosphamide has a direct ADH effect that can be overcome by diuretic. Cardiotoxicity: The DLT of cyclophosphamide is cardiotoxicity, at twice the standard transplant dose. At transplant doses, there is a 0.5% chance of pancarditis, so before each dose of Cy, an EKG rhythm strip is obtained and must be approved as showing stable voltages. If the voltages have significantly decreased, an echocardiogram must be obtained stat to ascertain the safety of further cyclophosphamide. Sialitis: TBI can cause sialitis with markedly elevated salivary amylase. Ice packs and sour drops that increase saliva flow can help symptomatically. Skin toxicity: TBI, busulfan, and thiotepa all have significant skin toxicity. Patients must not have any oily or greasy emollients on their skin when they undergo TBI, or the absorption of TBI in the skin can be increased. Very frequent bathing (QID) is important to reduce the skin toxicity associated with thiotepa, because of excretion of active metabolites in perspiration. Acute tumor lysis syndrome: see Oncologic Emergencies section b. Graft infusion The graft must be infused promptly to minimize the loss of stem cells. In vitro cultivation conditions have to date resulted in loss of stem cell function. Minimal processing of the graft is desirable, but some grafts contain more volume than the patient would tolerate. Generally, grafts smaller than 15 ml/kg should not be volume reduced. In any case, the graft should be infused as rapidly as possible, even if the patient must be diuresed because of volume overload. In cases of ABO mismatch, the plasma and/or RBCs will be removed from the graft to prevent hemolysis. However, grafts that have been cryopreserved will have significant hemolysis of their RBC content as a result of freeze-thawing. To minimize nephrotoxicity from free hemoglobin, patients receive alkaline hydration and mannitol.

48
DMSO is used to protect cell membranes during cryopreservation. It is normally 90% renally excreted, so patients who develop renal failure before day 0 may require special intervention to prevent DMSO toxicity, including cardiac dysrhythmias and CNS toxicity. DMSO typically is associated with nausea, some bradycardia and hypertension, and a peculiar odor from exhaled dimethyl sulfide. c. Delayed preparative regimen toxicities Mucositis: Rapidly dividing cells line the GI tract, with turnover every 3 days in the mouth, every 5 days in the esophagus, and every 7 days more distally. The DLT of most preparative regimen agents beyond marrow toxicity is mucositis, which usually begins a week after the start of the preparative regimen and peaks about day +5. 90% of patients undergoing ablative BMT develop mucositis. When methotrexate is used as GVHD prophylaxis, mucositis usually continues to increase until day +15. In addition to painful mouth sores, residual nausea, vomiting, and diarrhea are common manifestations of mucositis until about day +14. VOD: Venoocclusive disease of the liver occurs in about 10% of children undergoing ablative BMT. The risk is increased 3x if transaminases are > 50 at the start of the preparative regimen. Fever during the preparative regimen is associated with increased risk of VOD, perhaps because Tylenol depletes glutathione, which is thought to be central to the pathophysiology of VOD in the hepatic sinusoidal endothelial cells. The first sign of VOD is usually weight gain, which typically begins around day 0. Jaundice and tender hepatomegaly typically follow a few days later, with a peak incidence at day +6, but VOD can begin as early as day 0 or as late as day +28. Once it begins, it can persist for weeks. It is generally clinically diagnosed, but abdominal ultrasound can be useful to confirm the diagnosis, and PAI-1 inhibitor levels are almost always elevated and tend to reflect severity. The severity ranges from a mild, self-limited disease to a life-threatening disorder with multiple organ failure. The earlier VOD begins, the more severe it is likely to be, and you can use the Bearman nomograms to estimate the risk of severe VOD on the basis of the day post BMT, % weight gain above baseline, and total bilirubin. HUS: Hemolytic-uremic syndrome occurs more commonly after BMT than after infectious diarrhea, and is diagnosed on the basis of microangiopathic hemolytic anemia with uremia. d. Engraftment Neutrophil recovery is one of the key requirements for discharge from the hospital after an ablative transplant. The day of engraftment is defined as the first of two consecutive days with an ANC above 500. The median time of engraftment is day +10 after PBSCT, +17 after allogeneic BMT, +25 after cord blood transplant, and day +40 after 4HC-purged autologous BMT. Pace of engraftment is a key risk factor for bacterial and fungal infections; for each week with an ANC < 100, there is a 10% incidence of fungal infection. Growth factors are not generally helpful after BMT except when the graft is suboptimal because of low counts, particularly with autologous BMT in heavily pre-treated patients. Transfusion independence usually occurs after neutrophil recovery, and is delayed until about 6 months after BMT in cases with a major ABO mismatch. e. Graft-vs.-host disease Acute GVHD affects the skin (90%), intestines (60%), and liver (30%). It may begin as soon as donor-derived lymphocytes begin to circulate, or many weeks later. Acute GVHD may begin later when prophylactic immune suppression is abruptly withdrawn (e.g. non-compliance, intentional discontinuation to induce GVL, or poor absorption due to diarrhea). Scoring is based on clinical staging by organ system, which are then combined into an overall clinical severity. Glucksberg grades are roman numerals I - IV, and IBMTR severity scores are capital letters A-D. Both scales have been validated as predicting non-relapse mortality after allogeneic BMT. Organ-specific clinical stage of acute GVHD

49
Glucksberg overall clinical grade of acute GVHD
IBMTR Severity Index for Acute GVHD
Skin Involvement Liver involvement Gastrointestinal involvement
Index* Stage (max.)
Extent of rash
Stage (max.)
Total bilirubin (μmol/l)
Stage (max.)
Volume of diarrhea (ml/day)
A 1 < 25% 0 < 34 (< 2 mg/dL) 0 < 500 B 2 25-50% Or 1-2 34-102 (2 – 5.9
mg/dL) or 1-2 500-1500
C 3 > 50% Or 3 103-255 (6 – 14.9 mg/dL)
or 3 > 1500
D 4 Bullae Or 4 > 255 (> 14.9 mg/dL) or 4 Severe pain and ileus
f. Immune reconstitution Even after neutrophil recovery, sepsis occurs frequently in BMT recipients due to persistent lymphoid dysfunction and functional asplenia. For the first 6 months after BMT, patients who develop fever are admitted for R/O sepsis and must promptly receive empiric broad-spectrum antibiotics. Patients with any history of chronic GVHD are functionally asplenic for life, and should be given pneumococcal prophylaxis. g. Relapse Relapse after BMT is usually fatal. However, after allogeneic BMT, withdrawal of immune suppression and/or donor lymphocyte infusions may produce remissions which may be durable. These approaches are much more likely to work when applied to minimal residual disease. h. Late effects
Stage Skin Liver Intestinal Tract
1 Maculopapular rash < 25% of body surface
Bilirubin 34-50 μmol/l (2 – 2.9 mg/dL)
> 500 ml diarrhea/day
2 Maculopapular rash 25-50% body surface
Bilirubin 51-102 μmol/l (3 – 5.9 mg/dL)
> 1000 ml diarrhea/day
3 Generalized erythroderma Bilirubin 103-255 μmol/l (6 – 14.9 mg/dL)
> 1500 ml diarrhea/day
4 Generalized erythroderma with bulla formation and desquamation
Bilirubin > 255 μmol/l (> 14.9 mg/dL)
Severe abdominal pain, with or without ileus
Grade Degree of organ involvement
I Stage 1-2 skin rash; no gut involvement; no liver involvement; no decrease in clinical performance
II Stage 1-3 skin rash; stage 1 gut involvement or stage 1 liver involvement (or both); mild decrease in clinical performance
III Stage 2-3 skin rash; stage 2-3 gut involvement or 2-4 liver involvement (or both); marked decrease in clinical performance
IV Similar to Grade III with stage 2-4 organ involvement and extreme decrease in clinical performance

50
Conceptually, late effects can relate to the primary disease and its initial therapy, the preparative regimen, and the graft. Secondary malignancies are usually ascribed to the preparative regimen, but all three categories may apply. There are three common syndromes: in the first year after transplant, EBV-associated lymphoproliferative disease occurs, usually in donor-derived B cells. The risk is 1% overall, but is increased ten-fold by T cell depletion of the graft and by ATG and monoclonal antibody therapy for GVHD. Therapy related MDS and AML associated with prior topoisomerase (e.g. etoposide) exposure occur with a relatively short latency of 2 – 5 years from therapy. Particularly high rates are observed after autologous PBSCT when the graft is mobilized by an etoposide-containing regimen. Therapy related MDS and AML associated with alkylating agents occurs with longer latency, typically 5 – 10 years. The latency for other second malignant neoplasms is longer, typically 10 – 20 years. Skin cancer and oral cancers are particularly common in long-term survivors of BMT. In children, a major concern is growth and development. Both chemotherapy-based and radiation-based preparative regimens are associated with reduced height velocity, but the effects of TBI tend to be greater. About ¼ of patients have diminished growth hormone levels, but even with growth hormone replacement, there tends to be diminished skeletal response, particularly during the time of the adolescent growth spurt. Other endocrine effects include hypothyroidism in about 25% and gonadal endocrine dysfunction, so some children will need endocrine replacement to acquire secondary sexual characteristics during puberty. Infertility is expected after myeloablative preparative regimens, but is not assured. Dozens of men who received BMT as children have fathered apparently normal children. Surprisingly, the number of reports of fertility after Busulfan-based preparative regimens is less than after TBI. Intellectual development is not usually significantly impaired by BMT regimens. On average, long-term survivors of TBI-based BMT have IQ scores 3 points lower than their normal siblings. However, this includes patients who have devastating leukoencephalopathy, particularly after extensive prior intrathecal chemotherapy and cranial irradiation. Verbal IQ tends to be better preserved than performance IQ, and executive function may be most sensitive to high-dose therapy. Chronic GVHD is classically defined as GVHD that occurs more than 100 days after BMT. However, we now recognize that cGVHD can occur earlier, and acute GVHD can occur later than day +100. The manifestations of cGVHD can affect nearly any organ system, and may mimic the findings of scleroderma. Nearly half of patients with cGVHD remain on immune suppressive therapy 5 years after the diagnosis. However, new onset of cGVHD is rare more than 2 years after BMT. Bony complications of BMT include avascular necrosis of bone, particularly among patients treated with steroids for cGVHD, and osteoporosis. Assuring sufficient dietary calcium and vitamin D are standard, and the use of bisphosphonates is being explored. Cataracts affect about a quarter of BMT recipients, particularly those who received TBI-based preparative regimens and were treated with corticosteroids for GVHD. Onset is between 1 – 6 years after BMT, but frequently, they do not affect central vision enough to warrant extraction.

51
How to manage common transplant complications i. Mucositis. Supportive care for mucositis includes bicarbonate rinses (to compensate for the loss of bicarb-rich saliva), TPN, and narcotics, usually as a PCA infusion. There is a PBMTC study of Traumeel, a homeopathic agent to prevent mucositis. j. F+N. See separate section on fever and neutropenia. The situation in BMT is often more severe because of the combination of mucocutaneous injury creating a portal of entry for infection, combined with more profound immune suppression and often prolonged neutropenia. Key aspects are searching diligently for a source of fever and promptly initiating broad-spectrum gram-positive and gram-negative coverage. Please be sure to cover organisms that have recently caused proven infections, since these infections frequently recrudesce, and use the data from surveillance cultures to cover the organisms with which the patient is colonized. k. FUO. For the first 6 months after BMT, patients who develop fever are admitted for R/O sepsis and must promptly receive empiric broad-spectrum antibiotics. For patients 6 – 12 months after BMT, fever should prompt an immediate ER visit, including counts and cultures; if there is any question about the patient’s appearance, admission for initiation of broad spectrum antibiotics is appropriate. Patients with any history of CGVHD should be treated as functionally asplenic. l. Viral infections. Zoster reactivates in 50% of allogeneic BMT recipients during the first year after transplantation, and typically is treated with acyclovir 500 mg/m2/dose IV Q8hr. Because immunocompromised patients can develop disseminated infection including zoster pneumonia, respiratory as well as contact isolation is indicated. Patients who are exposed to varicella before immunologic reconstitution should receive VZIG prophylaxis as early as possible within 96 hr of exposure. CMV reactivates in 25% of allogeneic BMT patients who are at risk because they or their donors have had CMV infection in the past. If untreated, CMV infection usually presents as pneumonitis in the second month after BMT with a course that rapidly progresses to respiratory failure and death within days. Fortunately, CMV reactivation is almost always detectable by blood PCR before pneumonia develops, and in this setting, pre-emptive therapy with ganciclovir, 10 mg/kg/day IV divided Q12hr is very effective as induction therapy, followed by maintenance therapy of 5 mg/kg/day IV once daily until day 100. In contrast, CMV pneumonia requires treatment with ganciclovir plus CMV immunoglobulin, and carries 50% mortality. Influenza is best prevented by immunization of the household, but when it occurs, oseltamivir is effective and has a favorable toxicity profile. Adenovirus infections are frequently fatal in patients in the first month after allogeneic BMT. Optimal therapy is not well defined, but our approach has been to treat severely immunocompromised patients with disseminated or symptomatic adenoviral disease with cidofovir, using hydration and probenecid to help prevent nephrotoxicity. RSV has also caused fatal outbreaks in BMT centers. We administer immunoglobulin prophylactically, and consider systemic antiviral therapy for patients with documented disease. m. VOD. Standard therapy is supportive care, avoiding additional hepatotoxic agents, maintaining intravascular volume with colloid, eliminating sodium from IV fluids because of extreme sodium avidity, (you can monitor FeNa as an index of severity), and avoidance of potent diuretics, which tend to deplete intravascular volume and convert the patient from pre-renal azotemia to intrinsic renal failure. We are conducting a trial of defibrotide, a mixture of single-stranded DNA oligonucleotides to treat severe VOD. n. HUS. Cyclosporine may contribute to HUS, so substituting other GVHD therapy is usually indicated. Occult infections frequently precipitate severe HUS. We have observed an association between fungal infections and HUS in children undergoing unrelated donor BMT, so we obtain CT scans and intiate empiric antifungal therapy in patients newly diagnosed as having HUS. o. Acute GVHD. Standard therapy of acute GVHD is the combination of either cyclosporine or tacrolimus with steroids (methylprednisolone at 2.5 mg/kg/day initially).

52
Progression after 2-3 days on steroids, failure to improve after a week on steroids, and failure to resolve after 2 weeks on steroids are very concerning. Steroid-refractory aGVHD carries at least 80% mortality. We have developed pentostatin as 2nd-line therapy for steroid-refractory GVHD. There is a CTN trial randomizing among 4 promising therapies for aGVHD. p. Chronic GVHD. The established standard therapy of cGVHD is corticosteroids, typically at least 1 mg/kg/day for at least a month, followed by a taper to alternate-day therapy for six months or more. In addition to causing disability, cGVHD is associated with impaired T-cell immune function and functional asplenia. Therefore, supportive care must include PCP prophylaxis, pneumococcal prophylaxis, and surveillance for invasive fungal infections and disseminated viral infections, both of which are major causes of mortality in patients with cGVHD.