Embed Size (px)
DESCRIPTION
osce in pediatric neurology to help DNB exam
Citation preview

NEUROLOGY
Post Graduate CME Neurology
Bai Jerbai Wadia Hospital for Chidren, Mumbai

1) 4 yrs old, boy , FTND, Normal motor, mental and language milestones. Complaints from school – aggressive, cant sit in one place, restless, forgetful and impatient, problems with friends, fights
• Diagnosis?
• 3 cardinal features of this condition
• 2 treatment options

• ADHD
• Inattention, hyperactivity and impulsivity
• Medications (methyl phenidate, amphetamines, fluoxitine, atomoxitine), Behavior therapy

2)This child has epilepsy, MR, ataxia, unprovoked laughter, severe speech delay
• Diagnosis?• Chromosome involved• Inheritance• Name a syndrome with
the same chromosomal abnormality

• Angelman syndrome
• 15q11.2-12
• Uniparental disomy – usually maternal (60-75%)
- occ. paternal - normal chromosome ? Dominant mutations• Prader Willi – 15q11-13 (paternal origin)

3) 2 yrs old child born prematurely [28wks] comes with complaint of delayed achievement of motor milestones. Examination shows hypertonia with brisk reflexes in all 4 limbs more marked in lower limbs.
• What is the diagnosis? Define. • What is the MRI picture?• What is the treatment and when do you start it?• Name 2 conditions this child will be at risk for?

• Spastic Diplegia. Increased tone in all 4 extremities and face. LL>UL> face
• Periventricular leukomalacia
• Early intervention
• Learning disabilities,• Visual concerns• Epilepsy• Delayed mental development• Behavior concerns

4.A full term ,male child develops jaundice on day 3 of life, (S. bilirubin –34 mg%)and undergoes an exchange transfusion .
• What is the immediate complication likely to occur?
• Where is the anatomical abnormality? • What are the long term complications?• Name 1 investigations you would insist on
after discharge?

• Kernicterus
• Globus pallidus, dentate nucleus, cerebellar vermis, cochlear nuclei
• Choreoathetoid cerebral palsy, dystonic / dyskinetic CP, Sensorineural deafness,
• Audiometry testing

5. A child with apparently normal birth history :MS- social smile at 3 mths, Sitting at 8 months, rt hand preference at 9 mths, walking independently at 1.6 yrs.
• What is your diagnosis?
• What investigation will you do?
• What relevant maternal history will you ask for?

• Congenital hemiplegia
• MRI brain
• Maternal injury, threatened abortion, APC resistance, coagulation problem


6. Diagnosis
• 3 Differential diagnosis
• 3 differentiating features

• Ring enhancing lesion
• NCC, tuberculoma, toxoplasma, • abscess, tumor
• Peripheral vs central • single vs multiple• perilesional edema • smooth vs irregular• Scolex seen• Wall thickness• Intensity of cystic material


7. Diagnosis
• Name 2 other skin lesions
• Inheritance
• Other systems you would examine
• Name 3 lesions seen in the brain

• Ash leaf macule in Tuberous sclerosis
• Adenoma sebaceum , shagreen patch, café au lait spots
• Autosomal dominant
• Eyes, heart, kidneys, brain
• Tubers, subependymal nodules, subependymal giant cell astrocytomas

8. This 5 yr old comes with unsteadiness of gait with recurrent respiratory infections.
• Diagnose the conditionInheritance 3 salient features
2 lab investigations

• Ataxia Telangiectasia
• Autosomal recessive
• Ataxia, telangiectasia, immunodeficiency, recurrent sinopulmonary infections, X ray hypersensitivity, malignancies
• Alpha feto proteins, Immunoglobulins,(low IgA, IgG, high IgM), chromosomal breaks with exposure to radiation.

9. 8 yr old boy with headache, vomiting, ataxia, diplopia.
• Clinical diagnosis?
• MRI shows SOL
• .Name 2 supra and infra tentorial SOLs
• For this SOL what other abnormalities will you expect

• Raised ICT
• Supra- Craniopharyngioma, astrocytoma, Gliomas, ganglioglioma
• Infra- meduloblastoma, glioma• Craniopharygioma
• Panhypopitutarism, Hypothyroidism, GH deficiency, Gonadotrophin deficiency, cortisol def.

10. CSF picture
Protein 1640mg% ,
sugar 45/92 , cells 150 P40 L60
• Identify the condition
• 3 pathological etiologies
• 3 features on CT scan
• Treatment options
• TBM
• Ischaemia, edema, exudates
• Infarct, basal exudates, hydrocephalus ( communicating /non communcating) tuberculomas,
• 4 drug AKT, steroids, anti edema, shunt surgery,

11. Child with fever, headache , vomiting and altered sensorium.
• CSF picture :proteins 130,
sugar 40/90,
cells 240 P40 L 60
• Give 3 differentials
• Give 2 other investigations
• Treatment options

• Partially treated pyogenic meningitis, early TBM, aseptic, viral meningitis
• Latex agglutination, HSV DNA PCR, CT scan with contrast, EEG
• Antibiotics, acyclovir 10 mg/kg 8 hrly for 14 days, AKT, supportive

12.Child with fever , convulsions, altered sensorium
CSF picture : protein 62,
cells 95 P10 L90,
sugars 45/80,
RBCs 80/ hpf
• Additional 2 investigations of choice
• Treatment with dose

• EEG - PLEDS-periodic lateralizing epileptiform discharges
• HSV PCR,( ? HSV IgG, IgM ), CT scan / MRI with contrast – bi/ uni temporal hyperintensities
• Acyclovir 10mg/kg/dose 8 hrly for 14 -21 days

13)1.5 yrs old child with fever and convulsions.
CSF picture : proteins 80, sugar 20 /60, cells 500 , P 90 L 10.
• Diagnose / 3 common organisms• Child develops tense AF with focal
convulsions on day 8. Probable causes?• 3 Long term sequelae

• Pyogenic meningitis; pneumococci, H influenza, meningococci
• Subdural empyema, cerebral absess, infarction.
• Sensorineural deafness, hydrocephalus, CP, MR, Epilepsy, behavioural problems

14)11 months old comes with neuroregression from 5 months of age. He is hypotonic on examination.
• Name 3 systems you would like to examine?
• Differentials
• Give 4 DDs of cherry red spots
• Investigation of choice

• CNS, abdominal, ophthalmology,
• Krabbes, GSD [Pompes], Tay sachs, gangliosidosis
• GM 1Gangliosidosis, sialidosis, tay sachs, niemann picks, sandhoffs, MLD,
mucolipidosis
• Leucocyte enzymes, fibroblast culture

15)18 months old child comes with recurrent strokes , ptosis , ataxia and myopathy.
• Diagnosis
• Investigation of choice
• Inheritance
• Name 2 more conditions of the same metabolic category

• MELAS
• Mitochondrial deletion study MRI with spectroscopy CSF Lactate, Blood Lactate. ABG-Anion Gap Metabolic Screen
• Maternal transmission• MERRFS, Kearn Sayers, Leighs, Alpers

16) 6 months old female child, FTND, has asymmetric infantile spasms, developmental retardation and choroidal lacunae. MRI clinches the diagnosis.
• What is the diagnosis?
• What is the MRI picture?
• What is the inheritance pattern?

• Aicardi syndrome
• Corpus callosum agenesis
• Posterior choroidal cysts,
• choroidal lacunae
• X linked Dominant

17) A boy presents with this skin lesion-
Give 4 differential diagnosis
When and how much would you investigate?
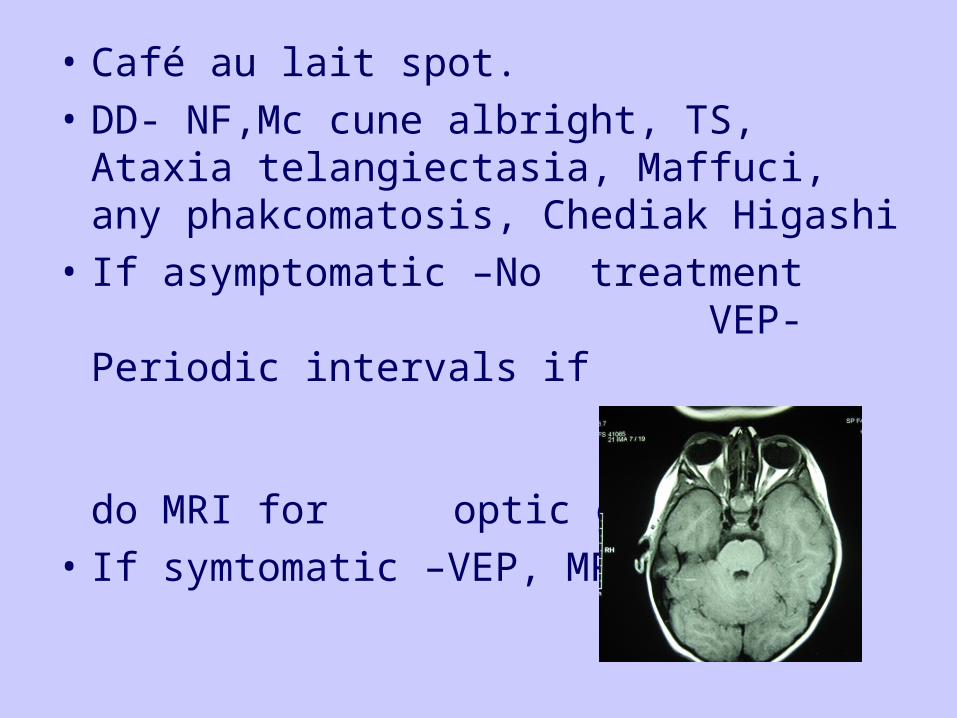
• Café au lait spot.
• DD- NF,Mc cune albright, TS, Ataxia telangiectasia, Maffuci, any phakcomatosis, Chediak Higashi
• If asymptomatic –No treatment VEP-Periodic intervals if abnormal do MRI for optic glioma
• If symtomatic –VEP, MRI,
EEG

18)• Name the sign• 3 DDs• 3 investigations in
sequence of importance
• Inheritance/ locus

• Gowers Sign
• Duchenne, SMA III, Limb girdle dystrophy, BMD, myopathy
• Dystrophin gene study, EMG /NCV, CPK levels
• X linked recessive/ Xp 21

19)• Diagnosis
• 2 associated abnormalities
• Classical CNS picture in CT scan and is described as
• Inheritance

• Sturge Weber syndrome
• Glaucoma, intracranial calcification, intractable epilepsy, hemangioma
• Tram track calcification
• Sporadic inheritance

• 20)
• Identify
• 2 salient features
• Criteria for diagnosis in newborn period are called:
• Child develops spastic quadriparesis.What will you suspect?
• Downs syndrome
• Facies, congenital heart defects, hypothyroidism ,deafness, hypotonia
• Halls Criteria
• Atlanto-axial dislocation

• 22)
• Diagnose
• Inheritance
• 2 associated abnormalities
• Investigation for Raised ICT

• Apert syndrome
• Autosomal dominant
• Proptosis, syndactyly, MR
• 3 D CTScan

• 23)
• This child came with neuroregression from 7 months of age with abn hand movts
• Diagnosis / DD• 3 salient features• Which milestones
are delayed?

• Retts syndrome / Autism
• Autism, stereotypies, microcephaly, loss of
fine purposeful hand movements
• Social, language

24) 10 month old , male, presents with progressive decreased activity since 3 months of age, breathing difficulty since 8 mths and pneumonia. Examination shows alert child with hypotonia and absent reflexes.
• What is the diagnosis ?• How do you confirm?• What is the inheritance? • Name 3 antenatal / natal features to ask for?

• SMA 1
• EMG/NCV, Gene studies
• SMA- AR,
• Decreased fetal kick count, polyhydramnious, previous fetal loses, weak cry, resp problems at birth.

25) 3 yrs old girl comes with drooping of both eyelids and squint noticed since 15 days. Abnormality seems to increase in the evenings.
• Diagnosis?
• Any 2 relevant questions?
• How do you confirm? Name 2 relevant investigations.
• Drug of choice.

• Myasthenia gravis
• Any other activity tires with time eg. Eating, walking, speech,
• Edrophonium test / Neostigmine test• Anticholinesterase antibody, EMG with
repititive stimulation, CTScan chest
• Pyridostigmine

• • 26 ) Label the
parts shown

• Corpus callosum
• Lateral ventricle
• 4 th ventrricle
• Pons
• medulla

EPILEPSY

1)4 Yrs old boy with normal motor and mental development becomes aphasic for last 15 days. He had a single GTC at 3.6 yrs.CNS examination is normal.
• Investigation of choice
• Diagnosis
• Treatment options

• EEG
• Landau Kleffner syndrome
• IV Ig , Steroids, AEDs

2) 6 yrs old girl with delayed development. Perinatal hypoglycemia. Symptomatic infantile spasms at 7 mths. Then focal seizures, generalised, myoclonic and now tonic.
• Diagnosis?• Drugs used?• AEDs to be avoided?• Non pharmacological treatment modalities

• Lennox Gastaut syndrome
• Valproate, Lamotrigine, Topiramate, clobazam
• Carbamazepine, phenobarbitone
• Corpus callosotomy, Ketogenic diet, vagal nerve stimulation

3) 10 yrs old boy presents with lip smacking, facial and eye deviation on left lasting 2 minutes after falling asleep. Similar history 3 and 6 months back.
• Investigation of choice?• Diagnosis?• Which investigation you need not do?• Prognosis?• Drug of choice?

• EEG
• Rolandic epilepsy/ BECTS
• MRI/Neuroimaging
• Good,
• Carbamazepine /oxcarbamazepine

4)4 days old newborn, FTND presents with multiple multifocal seizures. He has a normal systemic examination.
• DD- 3 most imp
• If strong family history of neonatal seizures present, what will u think

• Hypocalcemia,
• hypomagnesemia,
• 5 th day fits,
• BFNS,
• hypoglycemia
• BFNS

5) 6 yrs old boy comes with left sided focal seizures preceded by aura of fearfulness. He has history of prolonged febrile seizures at 1 yr of age. EEG shows right temporal epileptiform activity.
• What MRI picture do you expect?• Which virus has been suspected for the
same lesion?• What are the treatment options?

• Mesial temporal sclerosis
• Human herpes virus 6
• Temporal lobectomy


6) What does this EEG show?
• What is the drug of choice?
• Prognosis?
• One OPD procedure to confirm diagnosis

• 3 Hz spike and wave activity in Absence seizure – childhood /Juvenile
• Valproate, Lamotrigine, clobazam
• Good in childhood, slightly less for juvenile
• Hyperventilation

Jerk jerk

7) Diagnosis
• Confirmatory test
• 3 therapeutic options

• SSPE –burst suppression pattern
• CSF measles IgG
• Ribavarine, interferons, inosiplex, amantidine


8) Diagnosis
• Commonest etiology
• Drug of choice

• PLEDS
• Herpes encephalitis
• Acyclovir

9) 6 yr old male admitted with prolonged generalised seizures.
• Immediate AEDs –name 2 with dose
• 2nd line AEDs –2 with dose
• 3rd line – name 2

• Lorazepam [0.05mg/kg], • Diazepam [0.3mg/kg],• midazolam[ 0.2mg/kg]
• Phenytoin[ 20mg/kg],• phenobarb[20/kg]
• Midazolam drip,• propofol,• thiopentol

10) 6 months old child with h/o perinatal insult comes with regression of social milestones and clusters of startles on awakening .
• Diagnosis
• Name 2 investigations you will ask for?

• Infantile spasms, West syndrome
• EEG, MRI
• Hypsarrhythmia
• ACTH / steroids, Vigabatrin, Valproate /Topiramate / Nitrazepam

11) SODIUM VALPROATE
• Each 5ml of syrup contains • Commonest 3 side effects• Contraindicated in• Synergistic activity with• Dosage range• With Lamotrigine what precautions Are
needed?

• 200 mg, or 40 mg/ml
• Weight gain, hair loss, hepatotoxic, PCOD, hirsutism, hyperammonemia
• Inherited Metabolic disorder, underlying liver dysfunction
• Lamotrigine
• 10-40 mg/kg/day
• Cut the dose of VPA when adding LMT

12) Topiramate
• 2 indications
• 2 side effects
• Contraindicated in
• Tablet strength? Syrup? Any other preparation known?

• Generalised, partial, Infantile spasms, LGS
• Wt loss, word finding difficulty – speech regression, blurred vision, renal calculi, hyperthermia
• thin children, speech concerns
• 25 / 50 / 100mg. No syrup. Sprinkle

13) Carbamazepine
• Commonest side effects
• Not used in
• Higher derivative with advantage
• Syrup strength

• Ataxia , diplopia, rash, hyponatremia, cognitive decline, behavior concerns
• Absence, myoclonic
• Oxcarbazepine, less side effects
• 5ml = 100mg

14)Lamotrigine
• Indication, Dose
• Synergistic with?
• What dosage modification done?
• Life threatening side effect?

• Partial, generalied, LGS, JME;
• 3-7 mg/kg/d
• Valproate,
• Reduce the dose of VPA prior to starting
• Steven Johnson syndrome

• 15)Name 3 newer AEDs
• Name a carbonic anhydrase inhibitor used as AED

• Ocarbamazepine, Topiramate, Lamotrigine, Vigabatrine, Gabapentine, Zonisamide, Leviteracetam, Felbamate, Tiagabine
• Acetazolamide, Topiramate

16) 3 months baby has intractable epilepsy since birth and delayed development
• Name 2 vitamins you can try
• Does not respond to them – what investigation next

• Pyridoxine
• Biotin
• Metabolic workup, MRI – dysplasia, metabolic

17) 1st unprovoked generalised seizure in a 2 yr old child
• Essential investigation
• Optional investigation
• Treatment of choice

• EEG
• MRI, biochemistry, CSF
• Nil , unless specific indication