Embed Size (px)
Citation preview

Pediatric Pediatric Neurology Neurology
EmergenciesEmergenciesGraham ThompsonGraham Thompson
Cheri Nijssen-JordanCheri Nijssen-Jordan
2003/11/062003/11/06

ObjectivesObjectives
Approach to H/A in PediatricsApproach to H/A in Pediatrics DDx of Pediatric H/ADDx of Pediatric H/A Migraines in PediatricsMigraines in Pediatrics
Febrile SeizuresFebrile Seizures AAP recommendationsAAP recommendations prophylaxisprophylaxis
Status EpilepticusStatus Epilepticus Idiopathic Facial Nerve ParalysisIdiopathic Facial Nerve Paralysis
treatmenttreatment

Case#1Case#1 14 yo girl with headache for past 2 wks14 yo girl with headache for past 2 wks Started intermitent but now always there Started intermitent but now always there
(2-3/10), sometimes throbs more (8/10) (2-3/10), sometimes throbs more (8/10) across front of headacross front of head
Started to feel nauseated, no emesisStarted to feel nauseated, no emesis Has been taking tylenol with minimal helpHas been taking tylenol with minimal help Has had previous H/A but only last few Has had previous H/A but only last few
hrshrs Dosen’t wake from sleep, doesn’t wake Dosen’t wake from sleep, doesn’t wake
with H/Awith H/A

Case #1 cont.Case #1 cont.
No fevers, but feels stuffy/congested at No fevers, but feels stuffy/congested at timestimes
No FHx migraineNo FHx migraine No motion sicknessNo motion sickness Had concussion playing hockey (AAA Had concussion playing hockey (AAA
boys league) 8 months ago, no change to boys league) 8 months ago, no change to current playcurrent play
No behaviour/school changesNo behaviour/school changes Took minocycline x 3-4 days then stoppedTook minocycline x 3-4 days then stopped

HeadacheHeadache
Pain sensitive structures around the Pain sensitive structures around the headhead Vessels, dura, meningesVessels, dura, meninges Sinuses, teethSinuses, teeth MusclulatureMusclulature
In general (but not a rule!!!)In general (but not a rule!!!) frontal pain- supratentorial structures and frontal pain- supratentorial structures and
vessels via trigeminal nvvessels via trigeminal nv Occipital pain – posterior fossa via cranial nvsOccipital pain – posterior fossa via cranial nvs
H/A patternsH/A patterns AcuteAcute
Single episodeSingle episode URTI, dental pain, bleed, initial migraine, URTI, dental pain, bleed, initial migraine,
cocaine/amphetaminescocaine/amphetamines Acute-recurrentAcute-recurrent
Episodic pain with symptom-free intervalsEpisodic pain with symptom-free intervals Migraine, tension, cluster, substance abuse, HTNMigraine, tension, cluster, substance abuse, HTN
Chronic progressiveChronic progressive Gradual increase in frequency and severity with worrisome Gradual increase in frequency and severity with worrisome
featuresfeatures Space occupying lesion, chronic meningitis, IIH, hydro, HTNSpace occupying lesion, chronic meningitis, IIH, hydro, HTN
Chronic nonprogressiveChronic nonprogressive > 15 H/A per month, > 4 months, > 4hrs> 15 H/A per month, > 4 months, > 4hrs
MixedMixed Migraine or analgesic abuseMigraine or analgesic abuse
Headache - EpidemiologyHeadache - Epidemiology
PrevalencePrevalence 7-9 yo - 60-69%7-9 yo - 60-69% 15 yo – 75%15 yo – 75%
Chief complaint in 0.7-1.3% of PED Chief complaint in 0.7-1.3% of PED visitsvisits

Etiology of Heache in the PED
0
10
20
30
40
50
Type of Headache
Per
cen
tag
e
Viral Illness
Sinusitis
Migraine
Post-traumatic
Viral Meningitis
Strep Pharyngitis
Tension
Other
Headache in the PEDHeadache in the PED
Serious etiologySerious etiology 19/288 (6.6%)19/288 (6.6%)
15 – viral meningitis15 – viral meningitis 1 - Shunt malfunction1 - Shunt malfunction 1 – oncology1 – oncology 1 – hydrocephalus1 – hydrocephalus 1 – punctate hemorrhage1 – punctate hemorrhage
All had abnormal hx or pxAll had abnormal hx or px

H/A in PEDH/A in PED Viral URTIViral URTI 28.5 – 39%28.5 – 39% MigraineMigraine 8.5 – 21%8.5 – 21% TensionTension 1.5 - 29% 1.5 - 29% TraumaTrauma 1.3 - 20% 1.3 - 20% TumorTumor 1.5 - 4% 1.5 - 4% ShuntShunt 2 – 11.5% 2 – 11.5% OtherOther
Serious etiology – 6.6 – 15%Serious etiology – 6.6 – 15% All but 1 child in all 4 studies - abN Hx or PxAll but 1 child in all 4 studies - abN Hx or Px Lewis DW Lewis DW Sem in Ped NeuroSem in Ped Neuro 2001 8(1):46 2001 8(1):46

Headache in the PEDHeadache in the PED
When to worry….When to worry…. Chronic progressive patternChronic progressive pattern H/A or vomiting on awakeningH/A or vomiting on awakening Age < 3yoAge < 3yo ““thunderclap headache”thunderclap headache” Focal neuro signsFocal neuro signs VP shuntVP shunt Neurocutaneous syndrome (NF, TS)Neurocutaneous syndrome (NF, TS)
Headache and TumorsHeadache and Tumors Childhood Brain Tumor Consortium (Childhood Brain Tumor Consortium (JNeurooncolJNeurooncol
1991 10:31)1991 10:31) 3291 tumors3291 tumors 62% had H/A 62% had H/A 98% of these had at least 1 problem on Hx/Px (50% 98% of these had at least 1 problem on Hx/Px (50%
had >3)had >3) HxHx
N/V, changes in gait, strength, personality, speech, schoolN/V, changes in gait, strength, personality, speech, school PxPx
Papilledema, ataxia, abN EOM, DTR, Visual acuity Papilledema, ataxia, abN EOM, DTR, Visual acuity
““THERE IS NO CLASSIC BRAIN TUMOR THERE IS NO CLASSIC BRAIN TUMOR HEADACHE”HEADACHE”

Pediatric Migraine – IHS Pediatric Migraine – IHS DefinitionDefinition

Pediatric Migraine - Pediatric Migraine - ClassificationClassification
Migraine without auraMigraine without aura Migraine with aura (classic)Migraine with aura (classic) Migraine equivalentsMigraine equivalents

Pediatric Migraine - Pediatric Migraine - EpidemiologyEpidemiology
3-5% of school-aged children - M>F3-5% of school-aged children - M>F Up to 20% of adolescents - M<FUp to 20% of adolescents - M<F Highest frequence Mon,Tues,Wed, Highest frequence Mon,Tues,Wed,
daytimedaytime

Pediatric Migraine – Tx Pediatric Migraine – Tx OptionsOptions
Non-medicinalNon-medicinal NSAIDsNSAIDs
IbuprofenIbuprofen KetorolacKetorolac
Dopamine AntagonistsDopamine Antagonists phenothiazinesphenothiazines
5-HT agonists5-HT agonists ErgotsErgots TriptansTriptans
Novel TherapiesNovel Therapies ValproateValproate

Migraine - NSAIDsMigraine - NSAIDs RDBPC study of 6-12 yo using 7.5 mg RDBPC study of 6-12 yo using 7.5 mg
IbuprofenIbuprofen Significant reduction in pain, nausea, need for Significant reduction in pain, nausea, need for
rescue med, significant increase in pain free status rescue med, significant increase in pain free status @ 2 hrs@ 2 hrs
Lewis et al Lewis et al HeadacheHeadache 2002 42:780 2002 42:780 RDBCO study of Ibuprofen 10mg/kg, RDBCO study of Ibuprofen 10mg/kg,
acetaminophen 15 mg/kg and placeboacetaminophen 15 mg/kg and placebo Significant reduction in pain @ 2 hrs. Significant reduction in pain @ 2 hrs. Ibuprofen 2X as likely as acet (OR 2.2 CI 1.1-40)Ibuprofen 2X as likely as acet (OR 2.2 CI 1.1-40) Hamlainen et al Hamlainen et al Neuro Neuro 1997 48:1031997 48:103
KetorolacKetorolac No good peds studiesNo good peds studies Advantage - not PO intakeAdvantage - not PO intake
Migraine – Dopamine Migraine – Dopamine AntagonistsAntagonists
Metoclopramide, prochlorperazine, Metoclopramide, prochlorperazine, promethazinepromethazine
Antiemetic effect helpful in gastric Antiemetic effect helpful in gastric stasis & delayed absorptionseen in stasis & delayed absorptionseen in migrainesmigraines
Drowsiness, hypotension, Drowsiness, hypotension, extrapyramidal effectsextrapyramidal effects
Migraine – 5-HT AgonistsMigraine – 5-HT Agonists
TriptansTriptans 50 6-8 yo 0.06 mg/kg SC sumatriptan50 6-8 yo 0.06 mg/kg SC sumatriptan
78% red. in pain (mod-sev to none-mild) in 78% red. in pain (mod-sev to none-mild) in 60 min60 min
Recurrence 6%Recurrence 6% Flushing, dizziness, tingling, chest pain, Flushing, dizziness, tingling, chest pain,
neck stiffnessneck stiffness

Triptans in TeensTriptans in Teens 1 yr study of 437 adolescents treated 3273 1 yr study of 437 adolescents treated 3273
migraines (10 mg nasal sumatriptan)migraines (10 mg nasal sumatriptan) 76% pain relief in 2 hrs, 43% pain free by 2 76% pain relief in 2 hrs, 43% pain free by 2
hrshrs IN dosing ranging from 5-20 mg IN dosing ranging from 5-20 mg
Improvement in VAS @ 2 hours, and has low rates Improvement in VAS @ 2 hours, and has low rates of recurrence (6%)of recurrence (6%)
Note: adolescent had huge placebo effect (up Note: adolescent had huge placebo effect (up to 57%)to 57%)
Winner et al Winner et al HeadacheHeadache 2002 42:675 2002 42:675 Winner et al Winner et al HeadacheHeadache 2003 43:451 2003 43:451

ErgotsErgots
DHE – less side effects that DHE – less side effects that Ergotamine (N/V, hypertension, Ergotamine (N/V, hypertension, flushing, angina-like episodes)flushing, angina-like episodes)
0.1-0.5 mg IV0.1-0.5 mg IV Rarely used in ED setting in childrenRarely used in ED setting in children
ValproateValproate
No pediatric studiesNo pediatric studies Annals EM June 2003Annals EM June 2003 40 pts received 500 cc NS then 40 pts received 500 cc NS then
randomized to 500 mg VPA vs 10 mg randomized to 500 mg VPA vs 10 mg prochlorperazineprochlorperazine
VAS score q 15 min x 1 hrVAS score q 15 min x 1 hr VPA had poor response in terms of VPA had poor response in terms of
pain and nauseapain and nausea

Drugs in Pediatric Drugs in Pediatric MigraineMigraine
DrugDrug DoseDose RouteRoute
IbuprofenIbuprofen 10 mg/kg 10 mg/kg POPO
NaproxenNaproxen 5 mg/kg5 mg/kg POPO
KetorolacKetorolac 0.5 mg/kg (max 0.5 mg/kg (max 30mg/dose)30mg/dose)
IV/IMIV/IM
MetoclopramideMetoclopramide 1-2 mg/kg (max 1-2 mg/kg (max 10mg/dose)10mg/dose)
PO/IV/IMPO/IV/IM
ProchlorperazinProchlorperazinee
0.1 mg/kg0.1 mg/kg PO/IV/IMPO/IV/IM
SumatriptanSumatriptan Child -0.06 Child -0.06 mg/kgmg/kg
Adol 6mgAdol 6mg
Adol 5-20mgAdol 5-20mg
SCSC
SCSC
ININ
DHEDHE 0.1 – 0.5 mg0.1 – 0.5 mg IV/IMIV/IM
Migraine EquivalentsMigraine Equivalents Benign paroxysmal torticollis Benign paroxysmal torticollis
Infancy, torticollis, pallor, vomiting, Infancy, torticollis, pallor, vomiting, behaviour, bilat, 4hrs – 4 days, resolve by behaviour, bilat, 4hrs – 4 days, resolve by mid childhoodmid childhood
Benign paroxysmal vertigo (38%)Benign paroxysmal vertigo (38%) Unsteadiness, pallor, fear, spinning, 1-5 Unsteadiness, pallor, fear, spinning, 1-5
min. 1-3 yo, usually leaves within 2-3 yrsmin. 1-3 yo, usually leaves within 2-3 yrs Abdominal migraine vs cyclical Abdominal migraine vs cyclical
vomiting (18.5%)vomiting (18.5%) Crampy, periumbilical, nausea, vomiting, Crampy, periumbilical, nausea, vomiting,
pallor, 4 - 10 yo, may develop classic pallor, 4 - 10 yo, may develop classic migrainesmigraines

Migraine EquivalentsMigraine Equivalents
Acephalgic migraine (28.7%)Acephalgic migraine (28.7%) Visual auras without H/A, < 10 min, 5-12 yoVisual auras without H/A, < 10 min, 5-12 yo ““alice in wonderland”alice in wonderland”
Acute confusional migraineAcute confusional migraine Confusion, agitiation, memory loss, Confusion, agitiation, memory loss,
adolescenceadolescence Retrospective!!!!!!Retrospective!!!!!!
Made up 9.9% of migraine visits to Made up 9.9% of migraine visits to neurologistneurologist

Pediatric H/A ReviewsPediatric H/A Reviews
Qureshi F Lewis D Managing Qureshi F Lewis D Managing headache in the Pediatric headache in the Pediatric Emergency Department Emergency Department Clinical Clinical Pediatric Emergency MedicinePediatric Emergency Medicine 2003 2003 4(3)4(3)
Lewis D Headache in the Pediatric Lewis D Headache in the Pediatric Emergency Department Emergency Department Seminars in Seminars in Pediatric NeurologyPediatric Neurology 2001 8(1):46 2001 8(1):46

Case #2Case #2
16 mo boy previously well brought 16 mo boy previously well brought by EMS because of sz at homeby EMS because of sz at home
Lasted 1 minLasted 1 min Eyes rolled back, arms twitchingEyes rolled back, arms twitching Crying ++ afterCrying ++ after Has had URTI over past 2-3 daysHas had URTI over past 2-3 days

Simple Febrile Seizures - Simple Febrile Seizures - DefinitionDefinition
Normal preceding neuro and dvt statusNormal preceding neuro and dvt status Age 6 mo – 5 yrsAge 6 mo – 5 yrs brief (<15 minutes) brief (<15 minutes) generalized seizure generalized seizure only once in a 24 hour periodonly once in a 24 hour period febrile child who did not have either febrile child who did not have either
central nervous system infection or a central nervous system infection or a severe metabolic disturbance.severe metabolic disturbance.

Complex Febrile SeizureComplex Febrile Seizure
FocalFocal > 15 minutes> 15 minutes >1 in 24 hrs>1 in 24 hrs Post-ictal involvementPost-ictal involvement
Febrile Seizures - Risk Febrile Seizures - Risk FactorsFactors
Height of temperattureHeight of temperatture MaleMale Family Hx of febrile seizuresFamily Hx of febrile seizures

Febrile Seizures - Febrile Seizures - EpidemiologyEpidemiology
2-5% of children 2-5% of children Peak onset is 1 yo, mean = 19 – 23 moPeak onset is 1 yo, mean = 19 – 23 mo Sz is 1Sz is 1stst sign of illness in 25-50% of cases sign of illness in 25-50% of cases FHx in 25-40%FHx in 25-40%
1 parent – 4.4X risk1 parent – 4.4X risk 2 parents – 20X risk2 parents – 20X risk Sibling – 3.6X riskSibling – 3.6X risk 22ndnd degree relatives 2.7X risk degree relatives 2.7X risk
Infections?Infections? Of 445 cases 34% AOM, 12% URTI, 6% viral exanthem Of 445 cases 34% AOM, 12% URTI, 6% viral exanthem
6% pneumonia6% pneumonia HHV 6/7 – may not be as common as previously thoughtHHV 6/7 – may not be as common as previously thought HSV & influenza AHSV & influenza A Same baseline risk for invasive bacteremia (1%)Same baseline risk for invasive bacteremia (1%)

Febrile Seizures and Febrile Seizures and ImmunizationsImmunizations
Increased inIncreased in Day of DPTP-HibDay of DPTP-Hib 8-14 days post MMR8-14 days post MMR
NO long term consequencesNO long term consequences

Febrile Seizures – AAP Febrile Seizures – AAP GuidelinesGuidelines
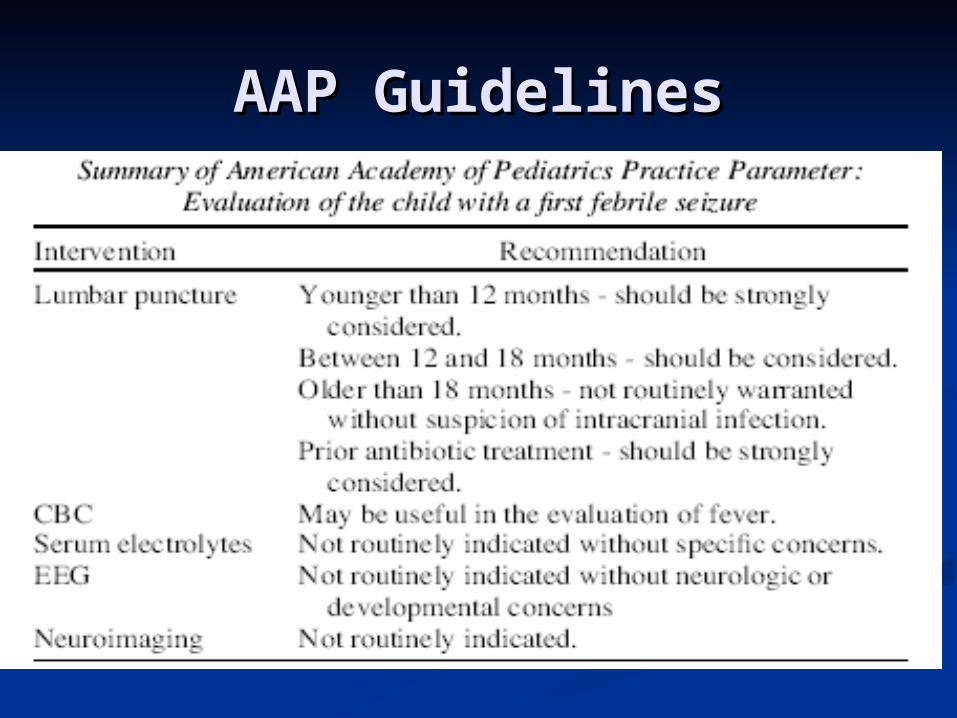
AAP GuidelinesAAP Guidelines

To LP or not?To LP or not?
All studies are retrospectiveAll studies are retrospective 503 pts with meningitis (V&B) age 2mo – 15 503 pts with meningitis (V&B) age 2mo – 15
yy 115 had sz but none were isolated sz115 had sz but none were isolated sz
452 6mo-5yo with fever and sz452 6mo-5yo with fever and sz 15 meningitis, all had septic appearance, 15 meningitis, all had septic appearance,
photophobia, stiff neck or Kernig (+)photophobia, stiff neck or Kernig (+) 241 6 mo-5yo with fever and sz241 6 mo-5yo with fever and sz
All had LP, 11 bacteria menngitis, all had one of All had LP, 11 bacteria menngitis, all had one of following 1)seen MD in past 48hrs 2)sz recurring following 1)seen MD in past 48hrs 2)sz recurring in ED 3)focal sz 4) abN neuro examin ED 3)focal sz 4) abN neuro exam

Febrile Seizures – Febrile Seizures – Recurrence RiskRecurrence Risk
1/3 will have recurrence, ½ of these 1/3 will have recurrence, ½ of these will have mutiple episodeswill have mutiple episodes
Highest inHighest in Young at 1Young at 1stst presentation presentation FHxFHx Low feverLow fever Short duration between start of fever Short duration between start of fever
and sz (<24 hrs)and sz (<24 hrs) Up to ½ of recurrences occur in 1Up to ½ of recurrences occur in 1stst 2 2
hrshrs

Febrile Seizures – Febrile Seizures – Recurrence RiskRecurrence Risk
Meta-analysis of recurrence riskMeta-analysis of recurrence risk Onset younger than 12 moOnset younger than 12 mo Febrile or afebrile seizure in 1Febrile or afebrile seizure in 1stst degree degree
relativerelative Rectal temp < 40 C during 1Rectal temp < 40 C during 1stst sz sz
Offringa et alOffringa et al
Consequences of Febrile Consequences of Febrile Seizures?Seizures?
EpilepsyEpilepsy General population – 1%General population – 1% Simple febrile szs – risk of afebrile szs Simple febrile szs – risk of afebrile szs
by age 25 increases to 2.4%by age 25 increases to 2.4% >1 focal complex febrile sz – may by up >1 focal complex febrile sz – may by up
to 30%to 30% Cognitive OutcomeCognitive Outcome
No changes in several american and No changes in several american and british studiesbritish studies

Febrile Seizures – Febrile Seizures – Prevention?Prevention?
AntipyreticsAntipyretics No evidence to support use No evidence to support use Uhari et al Uhari et al J pedsJ peds 1995 126:991 180 kids 1995 126:991 180 kids
RDBPC (plac + plac, plac + acet, diaz + acet, RDBPC (plac + plac, plac + acet, diaz + acet, diaz + plac) no difference in recurrence x2yrsdiaz + plac) no difference in recurrence x2yrs
Schnaiderman et al Schnaiderman et al Eur J PedsEur J Peds 1993 152:747 1993 152:747 104 kids RCT acet q4h or prn, no difference104 kids RCT acet q4h or prn, no difference
Van Stuijvenberg et al Van Stuijvenberg et al PedsPeds 1998 102:1 230 1998 102:1 230 kids RDBPC ibuprofen to plac no diff X1yrkids RDBPC ibuprofen to plac no diff X1yr
Meremikwa et al Meremikwa et al Cochrane DatabaseCochrane Database 2002:4 2002:4 no evidence supporting use of acet to prevent no evidence supporting use of acet to prevent Febrile SzFebrile Sz
Febrile Seizures – Febrile Seizures – Prevention?Prevention?
AntiepilepticsAntiepileptics Phenobarb – definite reduction in recurrences (OR Phenobarb – definite reduction in recurrences (OR
0.54 NNT = 8) if taken continuously, no difference 0.54 NNT = 8) if taken continuously, no difference if intermitentif intermitent
Hyperactivity, irritability, bld levels, sleep d/o, SJSHyperactivity, irritability, bld levels, sleep d/o, SJS VPA – definite reduction in recurrences (OR = 0.09 VPA – definite reduction in recurrences (OR = 0.09
NNT = 4) also if continousNNT = 4) also if continous Hepatotoxicity, thrombocytopenia, pancreatitis, wt changeHepatotoxicity, thrombocytopenia, pancreatitis, wt change
Intermitent diazepam – reduction by 44% per Intermitent diazepam – reduction by 44% per person per yearperson per year
Ataxia, lethary, irritibility, sleep d/oAtaxia, lethary, irritibility, sleep d/o Pheytoin, carbamazepine – no differencePheytoin, carbamazepine – no difference
Febrile Sz papersFebrile Sz papers
Warden CR et al Evaluation and Warden CR et al Evaluation and Management of febrile seizures in Management of febrile seizures in the Out-of-hospital and emergency the Out-of-hospital and emergency department setting department setting Annals of Annals of Emergency MedicineEmergency Medicine 2003 41(2) 2003 41(2)
Baumann RJ et al Treatment of Baumann RJ et al Treatment of Children with Simple Febrile Children with Simple Febrile Seizures: the AAP Practice Parameter Seizures: the AAP Practice Parameter Pediatric NeurologyPediatric Neurology 2000 23:11 2000 23:11
Case #3Case #3 18 mo girl started seizing @ home 2 hours ago18 mo girl started seizing @ home 2 hours ago Stiffened, unresponsive, R arm twitching the L Stiffened, unresponsive, R arm twitching the L
startingstarting Lasted about 4 minutesLasted about 4 minutes Very sleepy post ictal, not responding to parentsVery sleepy post ictal, not responding to parents Had 2 more similar szs in past 1hr so brought in by Had 2 more similar szs in past 1hr so brought in by
EMS, still not responding to voice (but maintaining EMS, still not responding to voice (but maintaining airway!!)airway!!)
Szs again just as you walk in the roomSzs again just as you walk in the room Currently on tegretol because other meds didn’t Currently on tegretol because other meds didn’t
workwork No fevers, no intercurrent illnessNo fevers, no intercurrent illness Last sz 3 months agoLast sz 3 months ago

Status Epilepticus Status Epilepticus
WHO DefinitionWHO Definition ““a condition characterized by and a condition characterized by and
epileptic sz that is sufficitnely prolonged epileptic sz that is sufficitnely prolonged or repeated at sufficiently brief intervals or repeated at sufficiently brief intervals so as to produce an unvaring or enduring so as to produce an unvaring or enduring epileptic condition”epileptic condition”
RealityReality Continuous or repetitive seizure activity of Continuous or repetitive seizure activity of
at least 30 minutes with failure to regain at least 30 minutes with failure to regain consciousness between convulsions.consciousness between convulsions.

S.E. Etiology in S.E. Etiology in PediatricsPediatrics
26% acute CNS insult26% acute CNS insult Bleed/traumaBleed/trauma InfectionInfection
21% underlying sz D/O21% underlying sz D/O Sudden discontinuation of MedsSudden discontinuation of Meds FeverFever
53% unknown!!!53% unknown!!!
SE ProblemsSE Problems HypoxiaHypoxia
Impaired ventilation, increased secretions, increased Impaired ventilation, increased secretions, increased O2 consumption, impaired O2 delivery, metabolic and O2 consumption, impaired O2 delivery, metabolic and respiratory acidosisrespiratory acidosis
Brain injuryBrain injury Hypoxia and perfusion related (CBF unable to keep up Hypoxia and perfusion related (CBF unable to keep up
with demandswith demands may occur more frequently with younger age leading to may occur more frequently with younger age leading to
MR, behaviour changes, motor deficitsMR, behaviour changes, motor deficits MorbidityMorbidity
Age dependent, up to 30% in <1 yo, 6% in those > 3yoAge dependent, up to 30% in <1 yo, 6% in those > 3yo MortalityMortality
3%3%
S. E. - TherapiesS. E. - Therapies
BenzosBenzos Phenytoin/FosphenytoinPhenytoin/Fosphenytoin PhenobarbPhenobarb Refractory S.E. TxRefractory S.E. Tx

S.E. - BenzosS.E. - Benzos Lorazepam vs Diazepam vs MidazolamLorazepam vs Diazepam vs Midazolam Loraz has smaller volume of Loraz has smaller volume of
distribution, longer acting (12-24 hrs vs distribution, longer acting (12-24 hrs vs 5-30 min), less respiratory depression5-30 min), less respiratory depression Small study (n=86) loraz 3% vs diaz 31%Small study (n=86) loraz 3% vs diaz 31%
Rectal diaz has less resp depression Rectal diaz has less resp depression than IVthan IV
Midazolam not used in newborns as may Midazolam not used in newborns as may lower sz threshold lower sz threshold
Midaz may be used PO, IV, IM, INMidaz may be used PO, IV, IM, IN

S.E. – BenzosS.E. – Benzos
Cochrane Review August 2003Cochrane Review August 2003 Lorazepam vs other AED in the PEDLorazepam vs other AED in the PED Only one studyOnly one study No difference in stopping szs, recurrence No difference in stopping szs, recurrence
rate, respiratory depression rate or need rate, respiratory depression rate or need for rescue AED in IV lorazepam vs for rescue AED in IV lorazepam vs diazepamdiazepam
Statistically significant diff in rectal loraz Statistically significant diff in rectal loraz over diaz, but numbers too small to make over diaz, but numbers too small to make recomendationsrecomendations
S.E. – S.E. – Phenytoin/FosphenytoinPhenytoin/Fosphenytoin
FosphenytoinFosphenytoin Phosphate ester pro-drug of phenytoinPhosphate ester pro-drug of phenytoin
Advantages of FosphenytoinAdvantages of Fosphenytoin Not in propylene glycol base so less tissue toxicity and Not in propylene glycol base so less tissue toxicity and
cardiac side effects (hypotension, bradys, VF)cardiac side effects (hypotension, bradys, VF) pH =8 (phenytoin =12)pH =8 (phenytoin =12) Compatible with any IV solution including DextroseCompatible with any IV solution including Dextrose Rapid IV infusion rate (up to 3X faster)Rapid IV infusion rate (up to 3X faster) IM route possible, IM route possible,
Disadvantages Disadvantages Pruritis (usually face and perineum) in up to 50%Pruritis (usually face and perineum) in up to 50% paresthesiaparesthesia High cost – 1G = $90 compared to $6High cost – 1G = $90 compared to $6
Recent studies show may have overall institutional cost Recent studies show may have overall institutional cost savings because of less side effectssavings because of less side effects

S.E. - BarbituatesS.E. - Barbituates
PhenobarbitalPhenobarbital Drug of choice in neonatesDrug of choice in neonates High sedative and CR depression which High sedative and CR depression which
may be enhance with prior benzo Txmay be enhance with prior benzo Tx Prolonged start time (15-20 minutes)Prolonged start time (15-20 minutes)

Refractory S.E.Refractory S.E.
Failure to respond to sequential Failure to respond to sequential treatment with benzo, phenytoin, treatment with benzo, phenytoin, phenobarbphenobarb
Midazolam infusionMidazolam infusion Propofol infusionPropofol infusion VPA infusionVPA infusion

AED Doses - PediatricAED Doses - PediatricDrugDrug DoseDose OnsetOnset
LorazepamLorazepam 0.05-0.1 0.05-0.1 mg/kg IV/PRmg/kg IV/PR
2-3 min2-3 min
DiazepamDiazepam 0.1-0.3 0.1-0.3 mg/kgIVmg/kgIV
0.5 mg/kg PR0.5 mg/kg PR
1-3 min1-3 min
PhenytoinPhenytoin 10-20 mg/kg 10-20 mg/kg IVIV
10-30 min10-30 min
FosphenytoinFosphenytoin 20 mgPE/kg20 mgPE/kg 10-30 min10-30 min
PhenobarbitalPhenobarbital 20 mg/kg20 mg/kg 10-20 min10-20 min
MidazolamMidazolam 0.1-0.2 mg/kg0.1-0.2 mg/kg Inf. 1-3 ug/kg/mInf. 1-3 ug/kg/m
PropofolPropofol 1-2 mg/kg1-2 mg/kg Inf. 25-100 Inf. 25-100 ug/kg/minug/kg/min
VPAVPA 15-20mg/kg15-20mg/kg Inf. 5 mg/kg/hrInf. 5 mg/kg/hr

Case #4Case #4
6 yo girl brought in by mother 6 yo girl brought in by mother because teacher said her face wasn’t because teacher said her face wasn’t working properlyworking properly
Can’t smile properly, L side doesn’t Can’t smile properly, L side doesn’t movemove
Had pain beside L ear yesterdayHad pain beside L ear yesterday Cough and runny nose 2 wks agoCough and runny nose 2 wks ago No fever, no rashNo fever, no rash

Bell’s PalsyBell’s Palsy(Idiopathic Facial Nerve Palsy)(Idiopathic Facial Nerve Palsy)
Unilateral facial nerve palsyUnilateral facial nerve palsy Sudden onset 1-2 wks post viral Sudden onset 1-2 wks post viral
infectioninfection Most common infectious Most common infectious
involvementinvolvement EBV, HSV, mumps, lyme disease, other EBV, HSV, mumps, lyme disease, other
viralviral ? Immune demyelination vs edema ? Immune demyelination vs edema

Bell’s PalsyBell’s Palsy DDxDDx
Lyme disaese (may be up to 50% in endemic areasa)Lyme disaese (may be up to 50% in endemic areasa) AOM, mastoiditisAOM, mastoiditis Ramsay Hunt (Herpes Zoster Oticus)Ramsay Hunt (Herpes Zoster Oticus) NMD (Myasthenia gravis)NMD (Myasthenia gravis) Tumor Tumor
Leukemia/lymphomaLeukemia/lymphoma SchwannomaSchwannoma parotidparotid
NeurofibromatosisNeurofibromatosis Brainstem infarctsBrainstem infarcts StrokeStroke TraumaTrauma

Bell’s PalsyBell’s Palsy
ClinicalClinical UnilateralUnilateral Pain may precedePain may precede Peripheral nerve weakness (lower motor Peripheral nerve weakness (lower motor
neuron) so involves upper and lower faceneuron) so involves upper and lower face Flat nasolabial foldFlat nasolabial fold Difficulty closing eye – exposure keratitisDifficulty closing eye – exposure keratitis Difficulty smilingDifficulty smiling ½ may loose taste on anterior ipsilat 2/3 of tongue ½ may loose taste on anterior ipsilat 2/3 of tongue
(dysgeusia)(dysgeusia) Decreased tearing vs crocodile tears (epiphoria)Decreased tearing vs crocodile tears (epiphoria) hyperacusishyperacusis

Bell’s Palsy - TreatmentBell’s Palsy - Treatment
Eye protectionEye protection 85-90% in children spontaneously 85-90% in children spontaneously
resolve with most occurring within 2 resolve with most occurring within 2 months of onsetmonths of onset

Bell’s Palsy - TreatmentBell’s Palsy - Treatment
Steroids?Steroids? Cochrane reviewCochrane review
3 studies, n = 117, not great randomization, 1 study 3 studies, n = 117, not great randomization, 1 study had no control grouphad no control group
No reduction in incomplete recovery or cosmetically No reduction in incomplete recovery or cosmetically disabling sequelaedisabling sequelae
Couldn’t recommendCouldn’t recommend Salman et al J child Neuro 2001 16:565Salman et al J child Neuro 2001 16:565
Systematic review of Bell’s Palsy in children <18Systematic review of Bell’s Palsy in children <18 8 trials, 1 exclusively children, 5 randomized, 5 8 trials, 1 exclusively children, 5 randomized, 5
blindedblinded No evidence for benefitNo evidence for benefit

Bell’s Palsy - TreatmentBell’s Palsy - Treatment Acyclovir?Acyclovir?
Cochrane reviewCochrane review 2 studies Acyc + steroid vs Acyc, acyc vs steroid2 studies Acyc + steroid vs Acyc, acyc vs steroid Couldn’t comment on primary outcomes (reduction of Couldn’t comment on primary outcomes (reduction of
incomplete recovery @ 1 yr, adverse events, paralysis @ incomplete recovery @ 1 yr, adverse events, paralysis @ 6mo) as not enough data6mo) as not enough data
Couldn’t recommendCouldn’t recommend De Diego et al Laryngoscope 1998 108(4):573De Diego et al Laryngoscope 1998 108(4):573
101 pts randomized to prednisone 1mg/kg OD x10 vs 101 pts randomized to prednisone 1mg/kg OD x10 vs acyclovir 800 mg TID x10acyclovir 800 mg TID x10
Recovery @ 3 months using nv function tests higher in Recovery @ 3 months using nv function tests higher in steroid vs acyclovirsteroid vs acyclovir
Adour et al Ann Otol Rhinol Laryngol 1996 Adour et al Ann Otol Rhinol Laryngol 1996 105:371105:371
Quicker return to functional muscle control with Quicker return to functional muscle control with combined acyclovir and prednisonecombined acyclovir and prednisone

Case #5Case #5
2 mo infant brought in with lethargy and 2 mo infant brought in with lethargy and vomiting x 8 in last 4 hours this pmvomiting x 8 in last 4 hours this pm
Normal U/O and BMNormal U/O and BM Felt “warm” to touch @ homeFelt “warm” to touch @ home Had been crying all night for past 2 nightsHad been crying all night for past 2 nights Previously well, IUTD, had tylenol yest. to Previously well, IUTD, had tylenol yest. to
try to stop cryingtry to stop crying Term, uncomplicated G1 pregTerm, uncomplicated G1 preg Child @ day home with other kids, all well Child @ day home with other kids, all well

Case #5 contCase #5 cont 37.8 160 22 – poor effort37.8 160 22 – poor effort 94% BP – 94% BP –
UAUA Looks unwell, paleLooks unwell, pale Poor spont. movementPoor spont. movement Font slightly fullFont slightly full Pupils a bit sluggish, 4mmPupils a bit sluggish, 4mm No source for infection on examNo source for infection on exam
SWU doneSWU done LP grossly bloody, not clearing over 4 tubes LP grossly bloody, not clearing over 4 tubes started on A/Bstarted on A/B
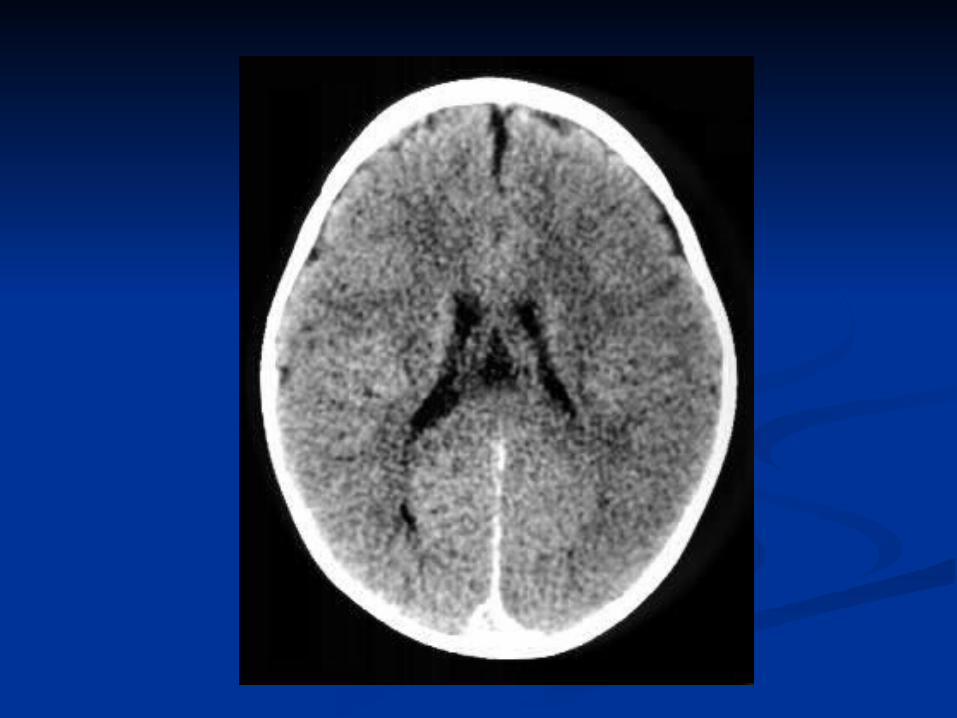

Non-Accidental TraumaNon-Accidental Trauma
DON’T FORGET IT IN DON’T FORGET IT IN YOUR YOUR DIFFERENTIALDIFFERENTIAL




























![1 CHERI Concentrate: Practical Compressed Capabilities · 2019. 5. 7. · 2.1 CHERI-256 The CHERI instruction-set architecture [1], [13] uses a large 256-bit capability format that](https://img.pdfslide.us/doc/110x75/5ff1164b0775fc50fc79755e/1-cheri-concentrate-practical-compressed-capabilities-2019-5-7-21-cheri-256.jpg)