Embed Size (px)
Citation preview

Pediatric Neurology
Dr. Kristen JohnsonDr. Adam OsterApril 14, 2011

In 60 minutes….
What we will try to cover.• Seizures• Common seizure mimics• Hydrocephalus and VP
shunts• A few other interesting
cases….
What we will not.• Headache• Stroke• Intracranial mass lesions• Lower motor neuron
weakness

18 month old girl arrives at the PLCRunny nose and cough Seizure this afternoon lasting 1 minute
Temp 39C, VSSNormal neuro exam

DIAGNOSIS?

What are the criteria to diagnose a febrile seizure?
Simple febrile
• < 15 minutes in duration• Generalized• Occur once in a 24 hr period
Complex febrile
• Prolonged• Focal• Occur more than once in a
24 hour period
✓6-60 months of age✓No evidence of intracranial infection✓Neurologically normal child✓No history of afebrile seizures

WHAT INVESTIGATIONS WOULD YOU LIKE TO ORDER?

NO ROLE
American Academy of Pediatrics – Clinical Practice Guideline 2011
CBCDLytesCaMgPO4glucose

. A lumbar puncture should be performed if:A. signs and symptoms of meningitis B. in an infant between 6-12mo who is considered deficient in Hib or S. pneumo immunizations (option)
C. in a child who has been pretreated with antibiotics (option)
American Academy of Pediatrics – Clinical Practice Guideline 2011

THE PARENTS NOW HAVE A LIST OF QUESTIONS FOR YOU….

What are the chances that this will happen again?
• Children < 12mo at the time of their first febrile seizure– 50% probability of recurrence
• Children > 12mo at the time of their first febrile seizure– 30% probability of recurrence
• Those who have a second febrile seizure have 50% chance of at least 1 additional recurrence

What are the chances my child will have epilepsy?
• Baseline risk of epilepsy in the population• 1%
• Risk of epilepsy in those with simple febrile seizures
• 2%
• Risk increases slightly if:– Multiple febrile seizures– < 12mo old at time of first febrile seizure– Complex febrile seizure– Family history of epilepsy

Is there anything I can do to prevent this in the future?
• NO

American Academy of Pediatrics – Clinical Practice Guideline 2008
• 1. Neither continuous or intermittent anticonvulsant therapy is recommended.– Adverse effects outweigh benefits
• 2. Antipyretics do not reduce the recurrence risk and are therefore not recommended.

Same child except….
AfebrileVomiting and diarrhea for 2dHad 4 brief seizures in a row
Does this change your thoughts?

4 year old boy presents to ACH with his first episode of seizure
•Well prior to event
•GTC seizure shortly after waking; • lasted 3 minutes;• post-ictal for 20 minutes;• back to baseline now
•No history of fever or viral sx•No history of head trauma or toxic ingestion•Developmentally normal•Normal neurological exam

WHAT INVESTIGATIONS WOULD YOU LIKE TO ORDER?
1st unprovoked seizure…

• 1. Lab tests should be ordered based on individual clinical circumstances– i.e. Vomiting, diarrhea, dehydration– Higher incidence of abnormalities (hypoNa+) in <
6mo
• 2. Consider toxicology screening if clinical suspicion
• 3. LP is of limited value in absence of clinical signs and symptoms of meningitis/encephalitis– Consider in < 6mo age group
American Academy of Neurology – Practice Parameter 2000

• 4. EEG should be part of standard workup– Helps determine seizure type, epilepsy syndromes,
risk of recurrence– Recurrence rate of 54% with abnormal EEG vs. 25% with normal
EEG
• 5. If neuroimaging is obtained, MRI is preferred modality– Emergent neuroimaging
• postictal focal deficit (Todd’s paresis) or slow return to baseline
– Nonurgent MRI should be considered in • Children < 1yo• Those with focal seizures• Those with EEG not in keeping with a benign epilepsy of
childhood• Those with developmental delays
American Academy of Neurology – Practice Parameter 2000

– EMS has just arrived with a 2 yo girl who is having a generalized tonic clonic seizure
– Seizure began 20 minutes ago– EMS unable to gain IV access• Given diastat 5mg PR x 1 dose
You are called STAT to the trauma room

The nurses cannot get an IV… what are your options?
– Rectal diazepam 0.5mg/kg– Buccal midazolam 0.5mg/kg– Intranasal midazolam 0.2mg/kg
– Intramuscular midazolam 0.2mg/kg– Intranasal lorazepam 0.1mg/kg– Sublingual lorazepam 0.1mg/kg

Is one first line agent better than the others?
• Buccal midazolam is better than rectal diazepam– 56% versus 27%
• IV lorazepam is better than IV diazepam– At least as effective (70% versus 65%) – Fewer side effects
• Bottom line: 1. when IV access is unavailable buccal midazolam is the treatment of choice; 2. IV lorazepam should replace IV diazepam in initial management
Appleton et al. Cochrane 2008

What next?• Second line agents
– Phenytoin 20mg/kg (1mg/kg/min)
– Fosphenytoin (3mg PE/kg/min)
• Third line agents– Phenobarbital (20mg/kg)– Valproic acid (20-30mg/kg)– Keppra/Levetiracetam
• Infusions– Midazolam (1-30mcg/kg/min)– Thiopental– Pentobarbital (5mg/kg then 1-
3mg/kg/hr)– Ketamine– Propofol
• Intubation– Propofol (1-3mg/kg)– Thiopental (3-5mg/kg)

Would your management change if this was a neonate?
• 1st line agent– Phenobarbital
• Pyridoxine trial

Convulsive Status Epilepticus

Convulsive Status Epilepticus
• Incidence 38/100 000/year in age 1-19– Higher incidence < 1yo – 135/100 000/year– 9-27% of children with epilepsy will have an
episode of status epilepticus– 12% present with status on 1st episode of seizure
• Outcomes mainly dependent on cause – Mortality 4%

The importance of treating early…
Status aborted in 100%who received 3rd AED within 60 minutes of 1st
versus
Only 22% who received 3rd AED > 60 minutes fromthe 1st

Etiology of Convulsive Status Epilepticus
Acute sy
mptomati
c
Remote sympto
matic
Remote sympto
matic w
ith ac
ute trigg
er
Progre
ssive
encephalo
pathy
Febrile
Crypto
genic
0%
10%
20%
30%

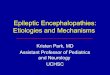
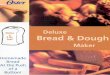
Diagnostic yield of investigations
electrolyt
es
blood cultu
re
lumbar punctu
re
AED leve
ls
toxic
ology sc
reen
inborn erro
rs metab
olism EEG
neuroim
aging
6.00% 2.50%13.00%
32.00%
4.00% 4.00%
90.00%
8.00%

NOW ON TO RANDOM CASES…SPOT
DIAGNOSES

2 mo boy with jerky movements
• Mom notices that he flinches and tenses up periodically
• Occurs during awake periods• Becoming more and more frequent• She has brought a video in for you to see

See video
http://www.youtube.com/watch?v=AQ3ZbWPSx1g

Infantile spasms
Cryptogenic (1/3)• Normal development• No known etiology
– Normal exam– Normal EEG– Normal MRI
Symptomatic (2/3)• Known etiology
– Tuberous Sclerosis most common
– CNS malformations– IEMs– Congenital infections
• Developmental delay

18 month old boy presenting with ? seizure
• He was crying and all of the sudden he turned blue, fell over and had a few twitches
• He was awake 1 minute later and now seems fine
• Otherwise healthy boy• Mom recorded the episode for you

See video
http://www.youtube.com/watch?v=2bKVHSe6hVQ

Breath-holding spells6 months – 4 years old
associated with Fe deficiency
Cyanotic• Most common• Child crying +++, holds
breath, rapidly cyanotic, becomes rigid
• Transient LOC with brief twitching of extremities
• Return to baseline quickly
Pallid• Less common• Preceded by minor trauma• Child turns pale and
collapses• Apnea and limpness
followed by rapid recovery

4 month old with recurrent episodes of stiffening and arching back
Sandifer’s Syndrome

3 wk old girl with jerky movements during sleep
• Video clip
http://www.youtube.com/watch?v=7z2FXVtxgaI

5 month old girl with jerky movements
• Come in clusters• Often around mealtime• Otherwise developing normally• Normal examination
• Watch video• http://www.youtube.com/watch?
v=KI7JTnQodGE

2 mo boy presenting with irritability and vomiting

Infants = 50mL CSFAdults = 150mL CSF

Hydrocephalus– Blockage
• Aqueductal stenosis– Congenital– Intrauterine infection
• Tumor• Congenital malformation
– Myelomeningocele – Chiari malformations– Dandy-Walker malformations
– Impaired absorption• Hemorrhage
– Ex-prem with IVH
• Meningitis
– Oversecretion• Choroid plexus tumors

Ventriculoperitoneal shunt

Same infant returns 6 weeks later with vomiting
• Low grade fever for the past 2 days• Has been more irritable than usual
• Hr 140, rr28, BP 85/50, T 38.2 C• Fontanel feels slightly full• Full EOM, PERL, no facial asymmetry• Mild increased tone in extremities

VP shunt complications
Infection• Usually within first 2
months• Staph epi and Staph aureus
most common• Late infections are usually
gram negative organisms• Treat with vancomycin and
cefotaxime
Obstruction• Most common within first 6
months; over half within first 2 years
• Investigations– Shunt series– Fast MRI– CT

Shunt series



6 year old girl •Previously healthy•Woke this am with a facial droop
•Remainder of neurologic examination is normal

What is your differential diagnosis?
• Bell’s palsy• Lyme disease• HIV infection• Otitis media• Cholesteatoma

How are you going to treat her?
Lacri-lube eye ointment
? Corticosteroids
? Antiviral Therapy

2 year old boy with dizzy spells
Episodes are brief where he falls to one sideCompletely well in betweenNormal neurological examination

Benign paroxysmal vertigo
• Children between 1 and 4 years of age• Acute episodes of dizziness and imbalance
which last seconds to minutes• No loss of consciousness• May have nausea and vomiting• Normal examination– +/- nystagmus
• Migraine variant

3 year old presents with difficulty walking
Abrupt onsetNo headacheVomit x 1 only
No constitutional symptomsHad chicken pox 2 weeks ago
Neuro exam: + ataxia, nystagmus

Acute Ataxia
• Life Threatening– Tumor– Hemorrhage– Stroke– Infection
• Common– Cerebellar ataxia– Guillain-barre syndrome– Labyrinthitis– Toxins– migraine


Acute cerebellar ataxia
• Acute onset of unsteadiness in a previously well child
• Most common cause of ataxia in a young child• Usually between 1-4 years old• Parainfectious or postinfectious demyelinating
phenomenon– Varicella (5-10 days after onset of illness; rarely up
to 3 weeks)– EBV, HSV, Mycoplasma, Influenza, Enteroviruses

Acute Cerebellar Ataxia
• Diagnosis– When illness follows typical course and there are
no other neurological findings, diagnosis may be made on clinical grounds
– If atypical features then do CT or MRI• Prognosis– Most cases resolve within 2 weeks of onset

6 year old girl presents with funny movements and irritability
• Watch video
http://www.youtube.com/watch?v=RsIQFeYOkAg

Sydenham’s Chorea
• Primarily between 3-13 years of age• Post-streptococcal disease– Major diagnostic criteria for rheumatic fever
• Initially affects face and hands• Involuntary movements disappear during sleep• Do streptococcal serology and complete workup for
rheumatic fever (ECG, echo)• Treat with penicillin• Alleviate movements with haldol, VPA, or
carbamazepine

3mo girl presenting with hypotonia
• Poor feeding and poor suck over the past few days
• Change in bowel movements
• Parents notice she is limp when they hold her
• Previously a healthy baby

Infant Botulism
• Clostridium botulinum toxin– Binds presynaptic receptors and disrupts ACh
release• Occurs between 1wk-12mo (usually 2-8mo)• Ingestion of raw honey or environmental dust– Utah, Pennsylvania, California
• Constipation cranial nerve dysfunction (poor suck/gag, ptosis, decreased eye movements) hypotonia/weakness respiratory failure

Infant botulism
• Diagnosis is clinical– Check for spores and toxin in stool
• Treatment– Human botulism Immunoglobulin– Supportive

Thanks!
Questions?