-
7/30/2019 Pediatric Medscape Lla
1/21
http://emedicine.medscape.com/article/990113-overview#showall
Updated: Feb 5, 2013
Pediatric Acute Lymphoblastic Leukemia
Author: Vikramjit S Kanwar, MD, MBA, MRCP(UK), FAAP; Chief
Editor: Robert J Arceci, MD,PhD more..
Practice Essentials
Signs and symptoms
Children with acute lymphoblastic leukemia (ALL) often present
with signs and symptoms that reflect
bone marrow infiltration and/or extramedullary disease. When
leukemic blasts replace the bone
marrow, patients present with signs of bone marrow failure,
including anemia, thrombocytopenia,
and neutropenia.
Other presenting signs and symptoms of pediatric ALL include the
following:
Patients with B-precursor ALL: Bone pain, arthritis, limping;
fevers (low or high);neutropenia; fatigue, pallor, petechiae, and
bleeding; lymphadenopathy and
hepatosplenomegaly
Patients with mature-B ALL: Extramedullary masses in the abdomen
or head/neck; CNSinvolvement (eg, headache, vomiting, lethargy,
nuchal rigidity)
Patients with T-lineage ALL: Respiratory distress/stridor due to
a mediastinal mass
Symptoms of CNS involvement are rarely noted at initial
diagnosis but are more common in T-
lineage and mature B cell ALL.[1]
Testicular involvement at diagnosis is also rare; if present, it
appears
as unilateral painless testicular enlargement.
SeeClinical Presentationfor more detail.
Diagnosis
Testing
Complete morphologic, immunologic, and genetic examination of
the leukemic cells is necessary to
establish the diagnosis of ALL.
Routine laboratory studies in pediatric ALL include the
following:
CBC count Peripheral blood smear Serum chemistries (eg,
potassium, phosphorus, calcium) Uric acid level
http://emedicine.medscape.com/article/990113-overview#showallhttp://emedicine.medscape.com/article/990113-overview#showallhttp://emedicine.medscape.com/article/990113-clinicalhttp://emedicine.medscape.com/article/990113-clinicalhttp://emedicine.medscape.com/article/990113-clinicalhttp://emedicine.medscape.com/article/990113-clinicalhttp://emedicine.medscape.com/article/990113-overview#showall
-
7/30/2019 Pediatric Medscape Lla
2/21
LDH level Coagulation studies (helpful in T-lineage ALL), such
as PT, aPTT, levels of fibrinogen and D-
dimer
Laboratory tests that help classify the type of ALL include the
following:
Immunophenotyping: To detect surface immunoglobulin on leukemic
blasts (diagnosis ofmature B-cell leukemia) or the expression of
T-cellassociated surface antigens (diagnosis of
T-lineage ALL)
Cytogenetic studies: To identify specific genetic alterations in
leukemic blasts Molecular studies (eg, FISH, RT-PCR, Southern blot
analysis): to identify translocations not
detected on routine karyotype analysis; to distinguish lesions
that appear cytogenetically
identical but are molecularly different
Minimal residual disease studies[2] : To detect chimeric
transcripts generated by fusiongenes, detect clonal TCR or
immunoglobulin heavy-chain (IgH) gene rearrangements, or
identify a phenotype specific to the leukemic blasts
Imaging studies
No other imaging studies than chest radiography to evaluate for
a mediastinal mass should be
required in pediatric ALL. However, the following radiologic
studies can be helpful:
Ultrasonography: To evaluate for testicular infiltration in boys
with enlarged testes; toevaluate for leukemic kidney involvement as
a risk assessment for tumor lysis syndrome
ECG, echocardiogram: To identify any preexisting cardiac
dysfunction before administrationof anthracyclines (baseline
studies); to monitor heart function during treatment with
anthracyclines
Procedures
Lumbar puncture with cytospin morphologic analysis: To assess
for CNS involvement beforeadministration of systemic chemotherapy;
to administer intrathecal chemotherapy
Bone marrow aspiration and biopsy: To confirm the diagnosis of
ALLCNS disease is divided into the following groups:
CNS 1: Absence of blasts on CSF cytospin preparation, regardless
of the WBC count CNS 2: WBC count of less than 5/mL and blasts on
cytospin findings, or WBC count of more
than 5/mL but negative by Steinherz-Bleyer algorithm findings
(if traumatic tap)
CNS 3: WBC count of 5/mL or more and blasts on cytospin findings
and/or clinical signs ofCNS leukemia (eg, facial nerve palsy,
brain/eye involvement, hypothalamic syndrome)
SeeWorkupfor more detail.
http://emedicine.medscape.com/article/990113-workuphttp://emedicine.medscape.com/article/990113-workuphttp://emedicine.medscape.com/article/990113-workuphttp://emedicine.medscape.com/article/990113-workup
-
7/30/2019 Pediatric Medscape Lla
3/21
Management
Leukemia is a systemic disease, and treatment is primarily based
on chemotherapy. However, the
different forms of ALL require different approaches for optimal
results. Treatment of subclinical CNS
leukemia is an essential component of ALL therapy.
Treatment for ALL typically consists of the following
phases:
Remission-induction phase (eg, dexamethasone or prednisone,
vincristine, asparaginase,daunorubicin)
Intensification/consolidation phase: Intensification
(cytarabine, cyclophosphamide,etoposide, dexamethasone,
asparaginase, doxorubicin, MTX, 6-MP, vincristine);
consolidation (MTX, 6-MP, cytarabine, cyclophosphamide)
Continuation therapy targeted at eliminating residual disease
(eg, MTX, 6-MP, vincristinepulses, glucocorticoid)
Intrathecal chemotherapy includes primarily MTX, which may also
be combined with hydrocortisone
and cytarabine (triple-intrathecal therapy).
Pharmacotherapy
Medications used in the treatment of pediatric ALL include the
following:
Antineoplastics (eg, vincristine, asparaginase, asparaginase
Erwinia chrysanthemi,daunorubicin, MTX, 6-MP, cytarabine,
etoposide, cyclophosphamide, nelarabine,
clofarabine)
Corticosteroids (eg, prednisone, dexamethasone) Antimicrobials
(eg, TMX/SMP, pentamidine) Antifungals (eg, fluconazole)
Treatment of T-cell ALL may benefit from the addition of
cyclophosphamide and intensive treatment
with asparaginase. Mature B-cell ALL needs to be treated in the
same way as disseminated Burkitt
lymphoma, with short-term intensive chemotherapy, including
high-dose MTX, cytarabine, and
cyclophosphamide over a 6-month period.
Blood transfusions or antibiotics may be required to deal with
complications of ALL therapy. Do not
administer folate supplementation owing to interactions with
MTX.
On January 25, 2013, the FDA approved imatinib in conjunction
with chemotherapy in children
with newly diagnosed Philadelphia chromosome (Ph)positive ALL in
children.[3, 4]
This approval
expanded the use of imatinib and chemotherapy in children with
leukemia; in 2011, imatinib plus
chemotherapy was approved for treatment of newly diagnosed
pediatric Ph-positive CML.
The agencys current approval was based on trial results by the
Childrens Oncology Group, which
showed, among other findings, that the combination of imatinib
and chemotherapy in pediatric
-
7/30/2019 Pediatric Medscape Lla
4/21
ALL doubled cure rates.[3]
The most common adverse effects observed with imatinib plus
chemotherapy were decreased levels of neutrophils and platelets,
as well as liver toxicity and
infection.[3, 4]
Nonpharmacologic therapy
Other treatments involved in managing pediatric ALL may include
the following:
Administration of IV fluids: Without potassium, with or without
sodium bicarbonate Cranial irradiation: Effectively prevents overt
CNS relapse but potentially causes
neurotoxicity and brain tumors; largely replaced by intensive
intrathecal and systemic
chemotherapy
Allogeneic SCT soon after first remission: Potentially prevents
relapse and/or mortality vschemotherapy alone
Surgical options
In generally, surgical care is not required in the treatment of
ALL. However, placement of a central
venous catheter is needed for administering chemotherapy, blood
products, and antibiotics, as well
as for obtaining blood samples.
SeeTreatmentandMedicationfor more detail.
Image library
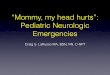
Bone marrow aspirate from a child with B-precursor acute
lymphoblastic leukemia. The marrow is replaced primarily with
small, immature lymphoblasts that
show open chromatin, scant cytoplasm, and a high
nuclear-cytoplasmic ratio.
Background
Acute lymphoblastic leukemia (ALL) is the most common malignancy
diagnosed in children,
representing nearly one third of all pediatric cancers. The
annual incidence of acute lymphoblastic
leukemia within the United States is 3.7-4.9 cases per 100,000
children age 0-14 years,[5]
with a peak
incidence in children aged 2-5 years.
Although a few cases are associated with inherited genetic
syndromes (eg,Down syndrome) or
congenital immunodeficiencies (eg,Wiskott-Aldrich syndrome,
ataxia-telangiectasia), the cause
remains largely unknown.[6]
With improvements in diagnosis and treatment, overall cure rates
for children with acutelymphoblastic leukemia have reached 90%.
[7]The use of risk-adapted treatment protocols has
http://emedicine.medscape.com/article/990113-treatmenthttp://emedicine.medscape.com/article/990113-treatmenthttp://emedicine.medscape.com/article/990113-treatmenthttp://emedicine.medscape.com/article/990113-medicationhttp://emedicine.medscape.com/article/990113-medicationhttp://emedicine.medscape.com/article/990113-medicationhttp://emedicine.medscape.com/article/943216-overviewhttp://emedicine.medscape.com/article/943216-overviewhttp://emedicine.medscape.com/article/943216-overviewhttp://emedicine.medscape.com/article/888939-overviewhttp://emedicine.medscape.com/article/888939-overviewhttp://emedicine.medscape.com/article/888939-overviewhttp://refimgshow%281%29/http://emedicine.medscape.com/article/888939-overviewhttp://emedicine.medscape.com/article/943216-overviewhttp://emedicine.medscape.com/article/990113-medicationhttp://emedicine.medscape.com/article/990113-treatment
-
7/30/2019 Pediatric Medscape Lla
5/21
improved cure rates while limiting the toxicity of therapy. This
article summarizes the current
diagnosis and treatment of childhood acute lymphoblastic
leukemia.
Pathophysiology
In acute lymphoblastic leukemia (ALL), a lymphoid progenitor
cell becomes genetically altered andsubsequently undergoes
dysregulated proliferation, with clonal expansion. In ALL, the
transformed
lymphoid cells reflect the altered expression of genes usually
involved in the normal development of
B cells and T cells. Several studies indicate that leukemic stem
cells are present in certain types of
acute lymphoblastic leukemia.
Epidemiology
Annually, around 3000 children in the United States are
diagnosed with ALL. The annual incidence of
ALL within the United States is 3.7-4.9 cases per 100,000
children 0-14 years of age.[5]
with a similar
estimated worldwide incidence, although it has been questioned
whether the incidence may be less
in low-income countries.[8]
White children are more frequently affected than black children,
and
there is a slight male preponderance, which is most pronounced
for T-cell acute lymphoblastic
leukemia. The incidence of acute lymphoblastic leukemia peaks in
children aged 2-5 years and
subsequently decreases with age.
Although a few cases are associated with inherited genetic
syndromes (eg,Down syndrome) or
congenital immunodeficiencies (eg,Wiskott-Aldrich syndrome,
ataxia-telangiectasia), the cause
remains largely unknown.[6]
Environmental risk factors such as exposure to ionizing
radiation and
electromagnetic fields and parental use of alcohol and tobacco
have not been shown to cause
pediatric acute lymphoblastic leukemia. In addition, no direct
link has been established between
viral exposure and the development of childhood leukemia.
Prognosis
The likelihood of long-term cure in ALL depends on the clinical
and laboratory features and the
treatment. Prognostic risk assessment includes clinical features
(age and white blood cell [WBC]
count at diagnosis), biologic characteristics of the leukemic
blasts, response to the induction
chemotherapy, and minimal residual disease (MRD) burden. Based
on these criteria, patients can be
effectively stratified into low risk, average or standard risk,
high risk, and very high risk.[9]
Standard-risk patients are aged 1-9.9 years with WBC of less
than 50,000 at presentation, lackunfavorable cytogenetic features,
and show a good response to initial chemotherapy, with less
than
5% bone marrow blasts by 14 days and less than 0.01% blasts by
28 days (rapid early response). Low-
risk patients meet all these criteria and have favorable
cytogenetics (eg, trisomy 4, 10, 17). High-risk
patients do not meet these criteria or have extramedullary
involvement that makes it inappropriate
for them to be treated as standard risk. Very-high-risk patients
have unfavorable cytogenetic
features (Philadelphia chromosome, hypodiploidy (n < 44, MLL
gene rearrangement) or very poor
response to initial chemotherapy (induction failure with MRD
>1%).
Patients younger than 1 year with acute leukemia have disease
that is biologically distinct with a
poor outcome.[10]
http://emedicine.medscape.com/article/943216-overviewhttp://emedicine.medscape.com/article/943216-overviewhttp://emedicine.medscape.com/article/943216-overviewhttp://emedicine.medscape.com/article/888939-overviewhttp://emedicine.medscape.com/article/888939-overviewhttp://emedicine.medscape.com/article/888939-overviewhttp://emedicine.medscape.com/article/888939-overviewhttp://emedicine.medscape.com/article/943216-overview
-
7/30/2019 Pediatric Medscape Lla
6/21
The 5-year event-free survival (EFS) varies considerably
depending on risk category, from 95% (low
risk) to 30% (very high risk), with infant leukemia having the
worst outcomes: 20% for patients
younger than 90 days. Overall, the cure rate for childhood acute
lymphoblastic leukemia (ALL) is
more than 80%.
Five-year survival rates for children diagnosed with acute
lymphoblastic leukemia, the most common
type in this group, rose to 90% from 2000-2005, which was up
from 84% in 1990-
1994.[7]
Improvement in survival was observed for all age groups of
children, except for infants
younger than 1 year. In low-income countries (LIC), therapy
results for pediatric ALL have been less
encouraging due to delayed diagnosis, abandonment of therapy,
and death from toxicity due to
suboptimal supportive care. Nevertheless, improved supportive
care with intensive therapy
protocols has increased current 4-year event-free survival rates
to 61% in India[11]
, and over 78% in
Lebanon[12]
, demonstrating that pediatric ALL is potentially highly curable
in LIC.
An analysis of long-term survival among 21,626 people who were
treated for leukemia as children in
Clinical Oncology Group trials from 1990-2005 found that 10-year
survival rose to almost 84% in
1995-1999 from 80% in 1990-1994. The analysis also found that
survival improved for almost all
groups, including older children and black children.[7]
Acute complications may involve all organ systems and include
the following:
Tumor lysis syndrome Renal failure Sepsis Bleeding Thrombosis
Typhlitis Neuropathy Encephalopathy Seizures
In addition, lifelong follow-up is necessary,[1]
because survivors may experience late effects from
treatment for this condition, such as the following:
Secondary malignancy Short stature (if craniospinal radiation)
Growth hormone deficiency Learning disability Cognitive defects
-
7/30/2019 Pediatric Medscape Lla
7/21
Patient Education
Ensure that the patient's parents and guardians understand that
ALL usually does not have a known
cause, that accurate stratification helps guide therapy, and
that participating in institutional or
consortium-based protocol therapy may help lead to better
outcomes in the future. In addition,
parents and guardians must know the expected adverse effects of
each medication and be able to
recognize signs and symptoms that require immediate medical
attention, such as those for anemia,
thrombocytopenia, and infection. Furthermore, parents and
patients must know how to quickly
access medical help from the oncology team.
For patient education information, seeCancer and Tumors Center,
as well asLeukemia.
History
Children with acute lymphoblastic leukemia (ALL) often present
with signs and symptoms that reflect
bone marrow infiltration and/or extramedullary disease. When
leukemic blasts replace the bone
marrow, patients present with signs of bone marrow failure,
including anemia, thrombocytopenia,
and neutropenia.
In patients with B-precursor ALL, bone pain, arthritis, and
limping may be presenting symptoms and
in 5% of patients are the only symptoms, leading to delays in
diagnosis.[13]
Fevers, whether low- or
high-grade, are common at presentation, but despite neutropenia,
sepsis is rarely seen. Other
common clinical manifestations include fatigue, pallor,
petechiae, and bleeding. In addition,
leukemic spread may manifest as lymphadenopathy and
hepatosplenomegaly.
Mature-B ALL may be associated with extramedullary masses in the
abdomen or head and neck and
central nervous system (CNS) involvement.
In patients with T-lineage ALL, respiratory distress and stridor
secondary to a mediastinal mass may
be a presenting symptom.
Symptoms of CNS involvement, such as headache, vomiting,
lethargy, and nuchal rigidity are rarely
noted at initial diagnosis but are more common in T-lineage and
mature B cell ALL.[1]
Testicular
involvement at diagnosis is also rare; if present, it appears as
unilateral painless testicular
enlargement.
Physical Examination
Physical findings in children with acute lymphoblastic leukemia
(ALL) reflect bone marrow
infiltration, as well as extramedullary disease. Patients
commonly present with pallor caused by
anemia and petechiae and bruising secondary to thrombocytopenia.
Leukemic infiltration may
manifest as lymphadenopathy and hepatosplenomegaly. If it
involves the central nervous system
(CNS), papilledema, nuchal rigidity, and cranial nerve palsy is
sometimes found. Testicular
examination in males is critical; leukemic infiltration usually
manifests as unilateral painless
testicular enlargement.
The presence of stridor is cause for concern and may signify a
mediastinal mass, found in half of
patients with T-lineage ALL, with a risk of imminent respiratory
arrest. Attempts to lay the patient
http://www.emedicinehealth.com/collections/SU295.asphttp://www.emedicinehealth.com/collections/SU295.asphttp://www.emedicinehealth.com/collections/SU295.asphttp://www.emedicinehealth.com/articles/25755-1.asphttp://www.emedicinehealth.com/articles/25755-1.asphttp://www.emedicinehealth.com/articles/25755-1.asphttp://www.emedicinehealth.com/articles/25755-1.asphttp://www.emedicinehealth.com/collections/SU295.asp
-
7/30/2019 Pediatric Medscape Lla
8/21
flat or perform intubation should be avoided, and the patient
should commence steroid therapy and
be transferred to the PICU for close observation.
Diagnostic Considerations
Complete morphologic, immunologic, and genetic examination of
the leukemic cells is necessary toestablish the diagnosis of acute
lymphoblastic leukemia.
The following are other conditions to consider when evaluating a
child with suspected acute
lymphoblastic leukemia (ALL):
Acute anemia Aplastic anemia Idiopathic thrombocytopenic purpura
(ITP)
Differential Diagnoses
Aplastic Anemia Fanconi Anemia Imaging in Arrhythmogenic Right
Ventricular Dysplasia (ARVD) Juvenile Rheumatoid Arthritis
Leukocytosis Parvovirus B19 Infection Pediatric Acute Myelocytic
Leukemia Pediatric Mononucleosis and Epstein-Barr Virus Infection
Pediatric Neuroblastoma Pediatric Non-Hodgkin Lymphoma Pediatric
Osteomyelitis Pediatric Rhabdomyosarcoma
Approach Considerations
Upon initial evaluation, obtain a complete blood cell (CBC)
count. A hematologist or
hematopathologist must evaluate the peripheral smear for the
presence and morphology of
lymphoblasts. An elevated leukocyte count of more than 10 109/L
(>10 103/L) occurs in one
half of patients with acute lymphoblastic leukemia (ALL).
Neutropenia, anemia, and
thrombocytopenia are often observed secondary to inhibition of
normal hematopoiesis by leukemic
infiltration. It is important to recognize that 20% of patients
with ALL initially present with
pancytopenia and no evidence of peripheral blasts.[14]
http://emedicine.medscape.com/article/198759-overviewhttp://emedicine.medscape.com/article/198759-overviewhttp://emedicine.medscape.com/article/960401-overviewhttp://emedicine.medscape.com/article/960401-overviewhttp://emedicine.medscape.com/article/352591-overviewhttp://emedicine.medscape.com/article/352591-overviewhttp://emedicine.medscape.com/article/1007276-overviewhttp://emedicine.medscape.com/article/1007276-overviewhttp://emedicine.medscape.com/article/956278-overviewhttp://emedicine.medscape.com/article/956278-overviewhttp://emedicine.medscape.com/article/961063-overviewhttp://emedicine.medscape.com/article/961063-overviewhttp://emedicine.medscape.com/article/987228-overviewhttp://emedicine.medscape.com/article/987228-overviewhttp://emedicine.medscape.com/article/963894-overviewhttp://emedicine.medscape.com/article/963894-overviewhttp://emedicine.medscape.com/article/988284-overviewhttp://emedicine.medscape.com/article/988284-overviewhttp://emedicine.medscape.com/article/987540-overviewhttp://emedicine.medscape.com/article/987540-overviewhttp://emedicine.medscape.com/article/967095-overviewhttp://emedicine.medscape.com/article/967095-overviewhttp://emedicine.medscape.com/article/988803-overviewhttp://emedicine.medscape.com/article/988803-overviewhttp://emedicine.medscape.com/article/988803-overviewhttp://emedicine.medscape.com/article/967095-overviewhttp://emedicine.medscape.com/article/987540-overviewhttp://emedicine.medscape.com/article/988284-overviewhttp://emedicine.medscape.com/article/963894-overviewhttp://emedicine.medscape.com/article/987228-overviewhttp://emedicine.medscape.com/article/961063-overviewhttp://emedicine.medscape.com/article/956278-overviewhttp://emedicine.medscape.com/article/1007276-overviewhttp://emedicine.medscape.com/article/352591-overviewhttp://emedicine.medscape.com/article/960401-overviewhttp://emedicine.medscape.com/article/198759-overview
-
7/30/2019 Pediatric Medscape Lla
9/21
Various metabolic abnormalities may include increased serum
levels of uric acid, potassium,
phosphorus, calcium, and lactate dehydrogenase (LDH). The degree
of abnormality reflects the
leukemic cell burden and destruction (lysis). Although not
universally performed, coagulation studies
can be helpful in patients with T-lineage ALL and should include
tests of the prothrombin time (PT),
activated partial thromboplastin time (aPTT), fibrinogen level,
and D-dimer level to assess for
disseminated intravascular coagulation (DIC).
No other imaging studies than chest radiography to evaluate for
a mediastinal mass should be
required. However, if the physical examination reveals enlarged
testes, perform ultrasonography to
evaluate for testicular infiltration. In addition, if
anthracyclines are to be administered, obtain a
baseline echocardiogram and an electrocardiogram (ECG).
To assess for central nervous system (CNS) involvement and to
administer intrathecal
chemotherapy, lumbar puncture with cytospin morphologic analysis
is performed before systemic
chemotherapy is administered.
Immunophenotyping
Acute lymphoblastic leukemia (ALL) cells rearrange their
immunoglobulin and T-cell receptor (TCR)
genes and express antigen receptor molecules in ways that
correspond to such processes in normal
developing B and T lymphocytes, so that acute lymphoblastic
leukemia can be classified as B-lineage
or T-lineage ALL.
The diagnosis of mature B-cell leukemia, which accounts for only
1-3% of childhood ALL, depends on
the detection of surface immunoglobulin on leukemic blasts.
Lymphoblasts with this phenotype have
a distinctive morphology, with deeply basophilic cytoplasm
containing prominent vacuoles,
designated L3 in the French-American-British (FAB) system (see
Histologic Features). Mature B-cell
ALL should be differentiated from other B-lineage ALL.
B-lineage ALL accounts for 80% of childhood ALL and involves
lymphoblasts that have cell-surface
expression of 2 or more B-lineageassociated antigens (ie, CD19,
CD20, CD24, CD22, CD21, or
CD79).[6] CD10 is commonly expressed, which makes it a useful
diagnostic marker, and the presence
of aberrant myeloid markers (eg, CD7) is occasionally noted but
has little prognostic impact. B-cell
precursors of ALL can be further subclassified as early
preB-cell, preB-cell, or transitional preB-
cell, but distinguishing these subtypes is usually not
clinically relevant.
-
7/30/2019 Pediatric Medscape Lla
10/21
T-lineage ALL is identified by the expression of
T-cellassociated surface antigens, of which
cytoplasmic CD3 is specific. T-cell acute lymphoblastic leukemia
cases can be classified by early, mid,
or late thymocytes. The prognosis of patients with T-cell ALL
has historically been worse than that of
patients with B-lineage ALL. However, the outlook for patients
with T-cell leukemia is comparable to
that of precursor B-cell ALL when intensive chemotherapy is
used.
Cytogenetic and Molecular Studies
In more than 90% of pediatric acute lymphoblastic leukemia (ALL)
cases, specific genetic alterations
can be found in the leukemic blasts, which have important
diagnostic, therapeutic, and prognostic
implications. In addition, molecular techniques, including
fluorescence in situ hybridization (FISH),
reverse transcriptase-polymerase chain reaction (RT-PCR), and
Southern blot analysis help identify
translocations not detected on routine karyotype analysis and to
distinguish lesions that appear
cytogenetically identical but are molecularly different.
Of the many abnormalities described, t(12;21)(p13;q22) or
ETV6-RUNX1 (formerly known as TEL-
AML1) and hyperdiploidy (>50 chromosomes/cell) account for
50% of chromosomal abnormalities
found and confer a favorable prognosis. Trisomy 4, trisomy 10,
and trisomy 17 (triple trisomy) may
be seen in some hyperdiploid cells and share the favorable
outcome. Hypodiploidy (< 44
chromosomes/cell), t(4;11)(q21;q23) MLL-AF4 or MLL gene
rearrangement, and t(9;22)(q34;q11), or
Philadelphia chromosome positivity confer a poor prognosis.
Minimal Residual Disease Studies
Traditionally, the response to leukemia treatment has been
assessed morphologically, which can be
challenging when looking for small numbers of leukemic cells,
especially in bone marrow specimens
recovering from chemotherapy or after transplantation.
Molecular analysis plays a promising role in the diagnosis and
treatment of acute lymphoblastic
leukemia (ALL) and in monitoring patients' responses to
therapy.
Studies of minimal residual disease (MRD) may be based on the
detection of chimeric transcripts
generated by fusion genes, the detection of clonal TCR or
immunoglobulin heavy-chain (IgH) gene
rearrangements, or the identification of a phenotype specific to
the leukemic blasts.[2]
The methods for detecting MRD have been shown to have a much
higher sensitivity than that of
morphology. All studies using MRD techniques have shown
significant correlations between end-of-
-
7/30/2019 Pediatric Medscape Lla
11/21
induction leukemia burden and outcome.[15] As a result, current
treatment protocols use MRD
measurements for acute lymphoblastic leukemia risk
assignment.[16]
Ultrasonography
Perform testicular ultrasonography if the testes are enlarged
upon physical examination.
Some clinicians use renal ultrasonography to evaluate for
leukemic kidney involvement as an
assessment of risk for tumor lysis syndrome.
Bone Marrow Aspiration and Biopsy
Bone marrow aspirate and biopsy results confirm the diagnosis of
acute lymphoblastic leukemia
(ALL). In addition, special stains (immunohistochemistry),
immunophenotyping, cytogenetic analysis,
and molecular analysis help in classifying each case. See the
images below for examples of bone
marrow aspirate findings.
Bone marrow aspirate from a child with B-precursor acute
lymphoblastic leukemia. The marrow is
replaced primarily with small, immature lymphoblasts that show
open chromatin, scant cytoplasm,
and a high nuclear-cytoplasmic ratio.
Bone marrow aspirate from a child with T-cell acute
lymphoblastic leukemia. The marrow is replaced
with lymphoblasts of various sizes. No myeloid or erythroid
precursors are seen. Megakaryocytes are
absent.
Bone marrow aspirate from a child with B-cell acute
lymphoblastic leukemia. The lymphoblasts are
large and have basophilic cytoplasm with prominent vacuoles.
Histologic Features
According to the French-American-British (FAB) classification
system, acute lymphoblastic leukemia
(ALL) is classified into 3 groups based on morphology, as
follows:
L1: The lymphoblast cells are usually small, with scant
cytoplasm and inconspicuous nucleoli. L1
accounts for 85% of all cases of childhood acute lymphoblastic
leukemia.
-
7/30/2019 Pediatric Medscape Lla
12/21
L2: The lymphoblast cells are larger than in L1. The cells
demonstrate considerable heterogeneity in
size, with prominent nucleoli, and abundant cytoplasm. L2
accounts for 14% of all childhood acute
lymphoblastic leukemia.
L3: The lymphoblast cells are large and notable for their deep
cytoplasmic basophilia. They
frequently have prominent cytoplasmic vacuolation and are
morphologically identical to Burkitt
lymphoma cells. L3 accounts for 1% of childhood acute
lymphoblastic leukemia cases.
Although the FAB system was used in the past, it is no longer
useful (except for L3), because current
standard diagnosis is based on immunophenotype and molecular
techniques.
pproach Considerations
Leukemia is a systemic disease, and treatment is primarily based
on chemotherapy. Thus, surgical
care is generally not required in the treatment of acute
lymphoblastic leukemia, except for the
placement of a central venous catheter. Such catheters are used
for administering chemotherapy,
blood products, and antibiotics, and for obtaining blood
samples.
Different forms of acute lymphoblastic leukemia (ALL) require
different approaches for optimal
results. Acute lymphoblastic leukemia treatment typically
consists of a remission-induction phase,
intensification (consolidation) phase, and continuation therapy
targeted at eliminating residual
disease. The addition of cyclophosphamide and intensive
treatment with asparaginase is also
beneficial in the treatment of T-cell acute lymphoblastic
leukemia. Mature B-cell ALL needs to be
treated like disseminated Burkitt lymphoma, with short-term
intensive chemotherapy, including
high-dose methotrexate (MTX), cytarabine, and cyclophosphamide
over a 6-month period.
Initially transfer children to a facility in which they can be
in the care of a pediatric oncologist,
preferably a center that participates in multi-institutional
clinical trials. Immediately admit any
patient who is neutropenic and who develops chills or fever to
administer intravenous (IV) broad-
spectrum antibiotics. Frequent hospitalizations may be required
to deal with complications of acute
lymphoblastic leukemia therapy, including the need for blood
transfusions or antibiotics.
Because of the use of MTX, avoid folate supplementation.
Tumor Lysis Syndrome
Before and during the initial induction phase of chemotherapy,
patients may developtumor lysis
syndrome, which refers to the metabolic derangements caused by
the systemic and rapid release of
intracellular contents as chemotherapy destroys leukemic blasts.
Because some cells can die before
therapy, such metabolic changes can occur even before therapy
begins.
Primary features of tumor lysis syndrome include hyperuricemia
(due to metabolism of purines),
hyperphosphatemia, hypocalcemia, and hyperkalemia. Hyperuricemia
can lead to crystal formation
with tubular obstruction and acute renal failure requiring
dialysis. Therefore, electrolyte and uric
acid levels should be closely monitored throughout initial
therapy.
To prevent complications of tumor lysis syndrome, patients
should initially receive intravenous (IV)
fluids at twice the maintenance rates, without potassium.
http://emedicine.medscape.com/article/282171-overviewhttp://emedicine.medscape.com/article/282171-overviewhttp://emedicine.medscape.com/article/282171-overviewhttp://emedicine.medscape.com/article/282171-overviewhttp://emedicine.medscape.com/article/282171-overviewhttp://emedicine.medscape.com/article/282171-overview
-
7/30/2019 Pediatric Medscape Lla
13/21
Sodium bicarbonate may be added to the IV fluid to achieve
moderate alkalinization of the urine (pH
level, 7.5-8) to enhance the excretion of uric acid. A urine pH
level higher than this should be
avoided to prevent crystallization of hypoxanthine or calcium
phosphate.
The standard prophylactic treatment for malignancy-associated
hyperuricemia includes allopurinol.
By blocking the enzyme xanthine oxidase, allopurinol blocks uric
acid formation. Patients at high risk
for tumor lysis still need to excrete preexisting uric acid,
which is unaffected by the use of
allopurinol.
Rasburicase, a recombinant urate oxidase, has demonstrated
increased efficacy in pediatric patients
at high risk for tumor lysis by catalyzing the enzymatic
oxidation of uric acid to a much more urine
soluble product, allantoin. Its expense means that use is
usually limited to patients at high risk of
tumor lysis syndrome (eg, T-cell leukemia with
hyperleukocytosis).
Chemotherapy
The phases and duration of chemotherapy for acute lymphoblastic
leukemia (ALL) are briefly
discussed in this section.
Phases of therapy
The treatment of childhood acute lymphoblastic leukemia, with
the exception of mature B-cell acute
lymphoblastic leukemia, has 5 components: induction,
consolidation, interim maintenance, delayed
intensification, and maintenance.
The goal of induction is to achieve remission, previously
defined as less than 5% blasts in the bone
marrow. Induction therapy generally consists of 3 or 4 drugs,
which includes a glucocorticoid,vincristine, asparaginase, and
possibly an anthracycline. This type of therapy induces
complete
remission based on morphology in more than 98% of patients.
However, the measurement of
minimal residual disease (MRD) by flow cytometry or polymerase
chain reaction (PCR) has been
shown to be much more specific and sensitive than the
morphologic examination of blast cells, and
the goal is to have less than 0.1% and preferably less than
0.01% at the end of induction.
Current childhood acute lymphoblastic leukemia clinical trials
incorporate MRD as a criterion for
determining rapid early responder versus slow early responder
status during induction
chemotherapy. Based on MRD measurements, treatment may be
intensified in patients with high
amounts of residual blasts at the end of induction therapy
(>1%).
Consolidation therapy is given soon after remission is achieved
to further reduce the leukemic cell
burden before the emergence of drug resistance and relapse in
sanctuary sites (ie, testes, central
nervous system [CNS]). In this phase of therapy, the patient is
given different drugs (eg
cyclophosphamide, cytarabine and/or 6-mercaptopurine [6-MP]).
Consolidation therapy appears to
improve the long-term survival of patients with standard-risk
disease.
In interim maintenance, nonmyelosuppressive chemotherapy (eg,
vincristine and intravenous MTX)
are administered to maintain remission and allow the bone marrow
to recover. This occurs for 4-8
weeks and is followed by delayed intensification, which is aimed
at treating any remaining resistant
-
7/30/2019 Pediatric Medscape Lla
14/21
leukemia cells. The addition of intensive reinduction and
reconsolidation therapy (collectively known
as delayed intensification) is beneficial for patients in all
risk groups.
The last (and longest) phase of treatment is maintenance. This
consists of intrathecal MTX every 3
months, monthly vincristine and steroid pulses, daily 6-MP, and
weekly MTX.
Duration of therapy
Whereas mature B-cell acute lymphoblastic leukemia (ALL) is
treated with a 6- to 8-month course of
intensive therapy, achieving acceptable cure rates for patients
with B-lineage and T-lineage ALL
requires approximately 2-2.5 years of continuation therapy.
Attempts to reduce this time resulted in
high relapse rates after therapy was stopped. In the United
States, in current ALL clinical trials, the
total duration of therapy for girls is 2 years from the start of
interim maintenance; for boys, it is 3
years from the start of interim maintenance.
Most contemporary protocols include a continuation phase based
on weekly orally administered
MTX given with daily, orally administered 6-MP, and monthly
pulses of vincristine and a
glucocorticoid. Although these pulses improve outcomes, they are
associated with avascular necrosis
of the bone and vincristine neuropathy, and the current
Children's Oncology Group standard risk ALL
trial is evaluating whether these last 2 agents can be given
every 3 months. A single-institution trial
has shown that patients with high-risk ALL may benefit from
intensified continuation therapy that
includes the rotational use of drug pairs.
The use of continuous dexamethasone in adolescents has been
associated with an unacceptably high
rate of osteonecrosis of the hips of around 40%,[17]
and this medication is therefore omitted from
induction and continuation therapy in older children.
Management of CNS Disease
Central nervous system (CNS) disease is divided into the
following:
CNS 1 - Absence of blasts on cytospin preparation of
cerebrospinal fluid (CSF), regardless ofthe number of white blood
cells (WBCs)
CNS 2 - WBC count of less than 5/mL and blasts on cytospin
findings, or WBC count of morethan 5/mL but negative by
Steinherz-Bleyer algorithm findings* (if traumatic tap)
CNS 3 - WBC count of 5/mL or more and blasts on cytospin
findings and/or clinical signs ofCNS leukemia, such as facial nerve
palsy, brain/eye involvement, and hypothalamic
syndrome (Additional intrathecal therapy is only given for CNS 3
disease.)
*If the patient has blasts in the peripheral blood and thelumbar
punctureis traumatic (containing
5/mL WBCs and blasts), treat as CNS 3 if the CSF WBC count
divided by the CSF red blood cell (RBC)
count is greater than 2 times the blood WBC count divided by the
blood RBC count.
Treatment of subclinical CNS leukemia is an essential component
of acute lymphoblastic leukemia
therapy.
Cranial irradiation
http://emedicine.medscape.com/article/80773-overviewhttp://emedicine.medscape.com/article/80773-overviewhttp://emedicine.medscape.com/article/80773-overviewhttp://emedicine.medscape.com/article/80773-overview
-
7/30/2019 Pediatric Medscape Lla
15/21
Although cranial irradiation effectively prevents overt CNS
relapse, concern about subsequent
neurotoxicity and brain tumors has led irradiation to be
replaced with intensive intrathecal and
systemic chemotherapy for most patients. This strategy has
produced excellent survival outcomes,
with CNS relapse rates of less than 2%.
Whether cranial irradiation is necessary for patients with very
high-risk acute lymphoblastic
leukemia (patients with BCR-ABL or MLL gene rearrangements) is
unclear. Pui et al conducted a
clinical trial in children with newly diagnosed acute
lymphoblastic leukemia and determined that
prophylactic cranial irradiation can be safely omitted from
treatment to avoid irradiation
consequences with effective risk-adjusted chemotherapy.[18]
The investigators reported that patients
who did not receive prophylactic cranial irradiation had
significantly longer continuous complete
remission relative to historical controls. In addition, patients
with CNS leukemia or traumatic lumbar
puncture with blast cells at diagnosis or those with a high
level of minimal residual disease after 6
weeks of remission induction were significantly associated with
poorer event-free survival.[18]
Risk
factors for CNS relapse included genetic abnormality, CNS
involvement at diagnosis, and T-cell
immunophenotype.
Management of High-Risk Patients
Optimal treatment for patients with very high-risk acute
lymphoblastic leukemia (ALL) has not been
determined; however, some centers recommend allogeneic stem cell
transplantation (SCT) soon
after first remission is achieved. It is important to know that
for the subset of patients with BCR-
ABL gene rearrangement, the addition of imatinib to intensified
chemotherapy produced survival
results equivalent to allogeneic SCT.[19]
A review of 1041 patients with ALL and induction failure showed
this population to be highlyheterogeneous in their clinical
features. Those patients with T-cell ALL appeared to have a
better
outcome with allogeneic stem-cell transplantation, whereas for
patients with precursor B-cell ALL
and either an age of less than 6 years or high hyperdiploidy,
the value of transplantation was less
certain.[20]
For patients without a matched family donor, transplantation of
marrow from an unrelated donor
would therefore no longer be a reasonable treatment option for
that subset, although it may be so
for other very-high-risk patients. Results of SCT, often
reported from single institutions, have been
inconsistent and sometimes disappointing. Large,
multi-institutional, controlled trials are clearly
needed to determine the effectiveness of this therapy for
patients without a matched donor.
Treatment of Relapse
In general, relapsed acute lymphoblastic leukemia (ALL) cells
acquire resistance to exposed
chemotherapy drugs. However, patients who relapse late (ie, 6 mo
or longer after completion of
therapy) can often be re-treated with more intensive
chemotherapy. Patients who relapse early
(ie, either during or just after completing therapy) may benefit
from (SCT). It is very important that
patients who go for SCT have MRD of less than 0.1%; otherwise,
they inevitably relapse. Overall, the
outcome of patients with relapse is poor.
Molecular Targeted Therapy
-
7/30/2019 Pediatric Medscape Lla
16/21
A drug targeted at the underlying molecular defect that is
unique to certain leukemias can have
potent and specific antileukemic activity while producing
minimal toxicity to normal cells.[21]
The best example of molecular targeted therapy is imatinib
mesylate, a selectiveBCR-ABL tyrosine
kinase inhibitor, that is standard front-line treatment for
Ph-positive chronic myeloid leukemia
(CML). Combination regimens with imatinib and conventional
chemotherapy have shown efficacy in
Ph-positive acute lymphoblastic leukemia, justifying its use as
front-line therapy for Ph-positive
acute lymphoblastic leukemia[22, 19]
Imatinib is approved for children newly diagnosed with Ph+ ALL.
Its approval was based on a trial
involving 92 patients in which children (1 year or older) and
young adults were divided into 5 groups
to receive different durations of imatinib therapy along with
conventional chemotherapy. Among
the 50 children receiving the longest duration of imatinib, the
4-year progression-free survival rate
was 70%. Increasing duration of imatinib therapy was associated
with lower overall mortality.[19]
Genetic Studies and Future Challenges
More than 80% of children with acute lymphoblastic leukemia
(ALL) now can be cured.[1]
However,
the cause of treatment failure in the remaining 20% of patients
is largely unknown.
More recently, poor outcome has been correlated with alteration
ofIKZF1, which encodes the
lymphoid transcription factor IKAROS.[23]
In addition, Janus kinase mutations have been associated
with a high risk of treatment failure.[24]
Because of the diverse nature of the disease, use of
risk-directed therapy for all patients on the basis
of molecular and pharmacogenetic characterization of the
leukemic cells at the time of diagnosis is
favored.
Studies using microarray gene expression, multiparameter
flow-cytometry, quantitative reverse-
transcriptase polymerase chain reaction (RT-PCR), genomics,
proteomics, and bioinformatics hold
promise for providing important clues to the mechanisms behind
leukemogenesis and response and
resistance to therapy. Future goals include the use of these
technologies to identify biologic subsets
of acute lymphoblastic leukemia that require specifically
targeted therapies.
Consultations
Numerous consultations may be obtained, depending on the
clinical circumstances of patients with
newly diagnosed acute lymphoblastic leukemia (ALL), including
the following:
Pediatric oncologist: Refer all patients to a subspecialist to
direct their care. Pediatric surgeon: Patients require placement of
a central venous catheter. Psychosocial team: Involve psychologists
and social workers in the care of patients with
acute lymphoblastic leukemia to aid them and their families in
navigating all of the difficult
issues surrounding their care.
-
7/30/2019 Pediatric Medscape Lla
17/21
Radiation oncologist: Consultation may be appropriate if there
is extramedullary disease notresponding to induction therapy (eg,
testicular involvement) or that associated with high-risk
disease (eg, CNS-3 in patients with T-lineage ALL).
Other subspecialists: Consultations with other specialists (ie,
infectious disease specialist,nephrologist) may be appropriate,
depending on the clinical circumstances.
Long-Term Monitoring
Frequent clinic visits are required to administer outpatient
chemotherapy, to monitor blood counts,
and to evaluate new symptoms. In addition, all patients should
be on trimethoprim-
sulfamethoxazole (TMP-SMZ) or a similar agent, such as monthly
IV pentamidine, to
prevent Pneumocystis cariniipneumonia (PCP). Patients with
infant leukemia may benefit from
being on oral fluconazole prophylaxis to reduce the risk of
candidiasis.
Medication Summary
Drugs commonly used during remission induction therapy include
dexamethasone or prednisone,
vincristine, asparaginase, and daunorubicin. Consolidation
therapy often includes methotrexate
(MTX) and 6-mercaptopurine (6-MP) or cyclophosphamide and
cytarabine. Drugs used for
intensification include cytarabine, cyclophosphamide, etoposide,
dexamethasone, asparaginase,
doxorubicin, MTX, 6-MP, and vincristine. Continuation therapy is
based on oral 6-MP and MTX with
pulses of vincristine and glucocorticoid (prednisone or
dexamethasone). Intrathecal chemotherapy
includes primarily MTX, which may also be combined with
hydrocortisone and cytarabine (triple-
intrathecal therapy). Imatinib is also approved for children
newly diagnosed with Ph+ ALL.
It is important to note that corticosteroids can adversely
suppress the function of the hypothalamic-
pituitary-adrenal (HPA) axis and such suppression can have
adverse effects on a patient's ability to
respond to different stresses, such as severe infection. A
Cochrane Database review of 7 studies
showed adrenal insufficiency occurred in nearly all ALL patients
in the first days after cessation of
glucocorticoid therapy. Although the majority of patients
recovered within a few weeks, a small
number of patients had adrenal insufficiency lasting up to 34
weeks.[25]
Antineoplastic Agents
Class Summary
Cancer chemotherapy is based on an understanding of tumor cell
growth and how drugs affect this
growth. After cells divide, they enter a period of growth (ie,
phase G1), followed by DNA synthesis
(ie, phase S). The next phase is a premitotic phase (ie, G2),
then finally a mitotic cell division (ie,
phase M).
Cell-division rates vary for different tumors. Most common
cancers grow slowly compared with
normal tissues, and the rate may be decreased in large tumors.
This difference allows normal cells to
recover from chemotherapy more quickly than malignant ones and
is the rationale behind current
cyclic dosage schedules.
Antineoplastic agents interfere with cell reproduction. Some
agents act at specific phases of the cell
cycle, whereas others (ie, alkylating agents, anthracyclines,
cisplatin) are not phase-specific. Cellular
-
7/30/2019 Pediatric Medscape Lla
18/21
apoptosis (ie, programmed cell death) is another potential
mechanism of many antineoplastic
agents.
View full drug information
Vincristine (Vincasar PFS)
Vincristine is a chemotherapeutic agent derived from the
periwinkle plant. This agent acts by
inhibiting microtubule formation in mitotic spindles, causing
metaphase arrest.
View full drug information
Asparaginase (Elspar)
Extracts of Escherichia coli or Erwinia L-asparaginase impair
asparagine synthesis. Asparaginase is
lethal to lymphoblasts that cannot synthesize the essential
amino acid asparagine.
View full drug information
Asparaginase Erwinia chrysanthemi (Erwinaze)
Catalyzes deamidation of asparagine to aspartic acid and
ammonia, thereby reducing circulating
levels of asparagine. Lack of asparagine synthetase activity
results in cytotoxicity specific forleukemic cells that depend on
an exogenous source of the amino acid asparagine. Indicated as
part
of a multiagent chemotherapeutic regimen for patients with acute
lymphoblastic leukemia (ALL)
who have developed hypersensitivity to E coliderived
asparaginase. It is estimated that 15-20% of
patients with ALL develop a hypersensitivity to E coliderived
asparaginase, which extrapolates to
approximately 450-600 children in the United States
annually.
View full drug information
Daunorubicin (Cerubidine)
Daunorubicin is an anthracycline that intercalates with DNA and
interferes with DNA synthesis.
View full drug information
Methotrexate (Trexall)
Methotrexate is a folate analogue that competitively inhibits
dihydrofolate reductase, thus inhibiting
DNA, RNA, and protein synthesis.
http://reference.medscape.com/drug/oncovin-vincasar-pfs-vincristine-342097#1http://reference.medscape.com/drug/oncovin-vincasar-pfs-vincristine-342097#1http://reference.medscape.com/drug/oncovin-vincasar-pfs-vincristine-342097#1http://reference.medscape.com/drug/oncovin-vincasar-pfs-vincristine-342097#1http://reference.medscape.com/drug/elspar-l-asparaginase-342099#1http://reference.medscape.com/drug/elspar-l-asparaginase-342099#1http://reference.medscape.com/drug/elspar-l-asparaginase-342099#1http://reference.medscape.com/drug/elspar-l-asparaginase-342099#1http://reference.medscape.com/drug/erwinaze-asparaginase-erwinia-chrysanthemi-999704#1http://reference.medscape.com/drug/erwinaze-asparaginase-erwinia-chrysanthemi-999704#1http://reference.medscape.com/drug/erwinaze-asparaginase-erwinia-chrysanthemi-999704#1http://reference.medscape.com/drug/erwinaze-asparaginase-erwinia-chrysanthemi-999704#1http://reference.medscape.com/drug/daunorubicin-342118#1http://reference.medscape.com/drug/daunorubicin-342118#1http://reference.medscape.com/drug/daunorubicin-342118#1http://reference.medscape.com/drug/daunorubicin-342118#1http://reference.medscape.com/drug/trexall-methotrexate-343201#1http://reference.medscape.com/drug/trexall-methotrexate-343201#1http://reference.medscape.com/drug/trexall-methotrexate-343201#1http://reference.medscape.com/drug/trexall-methotrexate-343201#1http://reference.medscape.com/drug/trexall-methotrexate-343201#1http://reference.medscape.com/drug/trexall-methotrexate-343201#1http://reference.medscape.com/drug/daunorubicin-342118#1http://reference.medscape.com/drug/daunorubicin-342118#1http://reference.medscape.com/drug/erwinaze-asparaginase-erwinia-chrysanthemi-999704#1http://reference.medscape.com/drug/erwinaze-asparaginase-erwinia-chrysanthemi-999704#1http://reference.medscape.com/drug/elspar-l-asparaginase-342099#1http://reference.medscape.com/drug/elspar-l-asparaginase-342099#1http://reference.medscape.com/drug/oncovin-vincasar-pfs-vincristine-342097#1http://reference.medscape.com/drug/oncovin-vincasar-pfs-vincristine-342097#1
-
7/30/2019 Pediatric Medscape Lla
19/21
View full drug information
Mercaptopurine (Purinethol)
Mercaptopurine is a synthetic purine analogue that kills cells
by incorporating into DNA as a false
base.
View full drug information
Cytarabine
Cytarabine is a synthetic analogue of nucleoside deoxycytidine.
This agent undergoes
phosphorylation to arabinofuranosyl-cytarabine-triphosphate
(ara-CTP), a competitive inhibitor of
DNA polymerase.
View full drug information
Etoposide (Toposar)
Etoposide inhibits topoisomerase II and breaks DNA strands,
causing cell proliferation to arrest in the
late S or early G2 portion of the cell cycle.
View full drug information
Cyclophosphamide
Cyclophosphamide is chemically related to the nitrogen mustards.
When this drug is used as an
alkylating agent, the mechanism of action of its active
metabolites may involve cross-linking of DNA,
which may interfere with the growth of normal and neoplastic
cells.
View full drug information
Nelarabine (Arranon)
Nelarabine is a prodrug of 9-beta-D-arabinofuranosylguanine
(ara-G). This agent is converted to the
active arabinofuranosyl-guanine-5'-triphosphate (ara-GTP), a
T-cellselective nucleoside analogue.
Leukemic blast cells accumulate ara-GTP, which allows for
incorporation into DNA, leading to
inhibition of DNA synthesis and cell death.
Nelarabine was approved by the US Food and Drug Administration
[FDA] as an orphan drug to treat
T-cell lymphoblastic lymphoma (a type of non-Hodgkin lymphoma
[NHL]) that does not respond orthat relapses with at least 2
chemotherapy regimens.
http://reference.medscape.com/drug/purinethol-6mercaptopurine-mercaptopurine-342094#1http://reference.medscape.com/drug/purinethol-6mercaptopurine-mercaptopurine-342094#1http://reference.medscape.com/drug/purinethol-6mercaptopurine-mercaptopurine-342094#1http://reference.medscape.com/drug/purinethol-6mercaptopurine-mercaptopurine-342094#1http://reference.medscape.com/drug/cytosar-u-depocyt-cytarabine-342089#1http://reference.medscape.com/drug/cytosar-u-depocyt-cytarabine-342089#1http://reference.medscape.com/drug/cytosar-u-depocyt-cytarabine-342089#1http://reference.medscape.com/drug/cytosar-u-depocyt-cytarabine-342089#1http://reference.medscape.com/drug/vepesid-toposar-etoposide-342098#1http://reference.medscape.com/drug/vepesid-toposar-etoposide-342098#1http://reference.medscape.com/drug/vepesid-toposar-etoposide-342098#1http://reference.medscape.com/drug/vepesid-toposar-etoposide-342098#1http://reference.medscape.com/drug/cytoxan-cyclophosphamide-342214#1http://reference.medscape.com/drug/cytoxan-cyclophosphamide-342214#1http://reference.medscape.com/drug/cytoxan-cyclophosphamide-342214#1http://reference.medscape.com/drug/cytoxan-cyclophosphamide-342214#1http://reference.medscape.com/drug/arranon-nelarabine-342090#1http://reference.medscape.com/drug/arranon-nelarabine-342090#1http://reference.medscape.com/drug/arranon-nelarabine-342090#1http://reference.medscape.com/drug/arranon-nelarabine-342090#1http://reference.medscape.com/drug/arranon-nelarabine-342090#1http://reference.medscape.com/drug/arranon-nelarabine-342090#1http://reference.medscape.com/drug/cytoxan-cyclophosphamide-342214#1http://reference.medscape.com/drug/cytoxan-cyclophosphamide-342214#1http://reference.medscape.com/drug/vepesid-toposar-etoposide-342098#1http://reference.medscape.com/drug/vepesid-toposar-etoposide-342098#1http://reference.medscape.com/drug/cytosar-u-depocyt-cytarabine-342089#1http://reference.medscape.com/drug/cytosar-u-depocyt-cytarabine-342089#1http://reference.medscape.com/drug/purinethol-6mercaptopurine-mercaptopurine-342094#1http://reference.medscape.com/drug/purinethol-6mercaptopurine-mercaptopurine-342094#1
-
7/30/2019 Pediatric Medscape Lla
20/21
View full drug information
Clofarabine (Clolar)
Clofarabine is a purine nucleoside antimetabolite that inhibits
DNA synthesis and is indicated for
relapsed or refractory acute lymphoblastic leukemia in pediatric
patients. Pools of cellular
deoxynucleotide triphosphate are decreased by inhibiting
ribonucleotide reductase and terminating
DNA chain elongation and repair. This agent also disrupts
mitochondrial membrane integrity.
View full drug information
Imatinib (Gleevec)
Imatinib is a selective BCR-ABL tyrosine kinase inhibitor. It is
approved for children newly diagnosed
with Philadelphia chromosome positive acute lymphoblastic
leukemia (Ph+ ALL).
Corticosteroids
Class Summary
These agents have anti-inflammatory properties and cause
profound and varied metabolic effects.
Corticosteroids modify the bodys immune response to diverse
stimuli. These agents are significantly
toxic to lymphoblasts, and two thirds of patients with pediatric
ALL who receive steroid therapy
alone go into remission.
View full drug information
Prednisone
Prednisone is a corticosteroid and an important chemotherapeutic
agent in the treatment of acute
lymphoblastic leukemia (ALL). This agent is used in induction
therapy and is also given as
intermittent pulses during continuation therapy.
View full drug information
Dexamethasone (Baycadron, Maxidex, Ozurdex)
Dexamethasone is another corticosteroid that acts as an
important chemotherapeutic agent in the
treatment of ALL. Like prednisone, this agent is used in
induction and reinduction therapy and is also
given as intermittent pulses during continuation therapy.
Antimicrobials
Class Summary
http://reference.medscape.com/drug/clolar-clofarabine-342196#1http://reference.medscape.com/drug/clolar-clofarabine-342196#1http://reference.medscape.com/drug/clolar-clofarabine-342196#1http://reference.medscape.com/drug/clolar-clofarabine-342196#1http://reference.medscape.com/drug/gleevec-imatinib-342239#1http://reference.medscape.com/drug/gleevec-imatinib-342239#1http://reference.medscape.com/drug/gleevec-imatinib-342239#1http://reference.medscape.com/drug/gleevec-imatinib-342239#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741#1http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741#1http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741#1http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741#1http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741#1http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/prednisone-intensol-342747#1http://reference.medscape.com/drug/gleevec-imatinib-342239#1http://reference.medscape.com/drug/gleevec-imatinib-342239#1http://reference.medscape.com/drug/clolar-clofarabine-342196#1http://reference.medscape.com/drug/clolar-clofarabine-342196#1
-
7/30/2019 Pediatric Medscape Lla
21/21
Prophylactic antimicrobial drugs are given to prevent infection
in patients receiving chemotherapy.
View full drug information
Sulfamethoxazole and trimethoprim (Septra, Bactrim)
Sulfamethoxazole and trimethoprim inhibits bacterial growth by
inhibiting synthesis of dihydrofolic
acid. All immunocompromised patients can be given cotrimoxazole
to prevent Pneumocystis carinii
pneumonia (PCP).
View full drug information
Pentamidine
Immunocompromised patients who do not tolerate cotrimoxazole due
to myelosuppression may
receive IV pentamidine to prevent Pneumocystis carinii pneumonia
(PCP).
Antifungals
Class Summary
These agents may change the permeability of the fungal cell,
resulting in a fungicidal effect.
View full drug information
Fluconazole
Fluconazole may be used in patients at high risk (eg, infant
ALL) to prevent fungal infections. It is a
synthetic triazole that inhibits fungal cell growth by
inhibiting CYP-dependent synthesis of
ergosterol, a vital component of fungal cell membranes.
http://reference.medscape.com/drug/bactrim-trimethoprim-sulfamethoxazole-342543#1http://reference.medscape.com/drug/bactrim-trimethoprim-sulfamethoxazole-342543#1http://reference.medscape.com/drug/bactrim-trimethoprim-sulfamethoxazole-342543#1http://reference.medscape.com/drug/bactrim-trimethoprim-sulfamethoxazole-342543#1http://reference.medscape.com/drug/nebupent-pentam-pentamidine-342568#1http://reference.medscape.com/drug/nebupent-pentam-pentamidine-342568#1http://reference.medscape.com/drug/nebupent-pentam-pentamidine-342568#1http://reference.medscape.com/drug/nebupent-pentam-pentamidine-342568#1http://reference.medscape.com/drug/diflucan-fluconazole-342587#1http://reference.medscape.com/drug/diflucan-fluconazole-342587#1http://reference.medscape.com/drug/diflucan-fluconazole-342587#1http://reference.medscape.com/drug/diflucan-fluconazole-342587#1http://reference.medscape.com/drug/diflucan-fluconazole-342587#1http://reference.medscape.com/drug/diflucan-fluconazole-342587#1http://reference.medscape.com/drug/nebupent-pentam-pentamidine-342568#1http://reference.medscape.com/drug/nebupent-pentam-pentamidine-342568#1http://reference.medscape.com/drug/bactrim-trimethoprim-sulfamethoxazole-342543#1http://reference.medscape.com/drug/bactrim-trimethoprim-sulfamethoxazole-342543#1