Embed Size (px)
Citation preview

Ranked in 2012 as a top pediatric cardiology and heart surgery program by U.S. News & World Report, Le Bonheur’s Heart Institute continues to improve the quality of life for hundreds of children with heart defects.
2012 highlights of the Heart Institute include:• State-of-the-art heart catheterization labs, including the only hybrid catheterization lab in the region. • The region’s only pediatric electrophysiologists.• Three-dimensional reconstruction capabilities and expertise in cardiac MRI.• Joint research with St. Jude Children’s Research Hospital to improve outcomes for children with cardiomyopathy.• Expertise in some of the most complex heart defects, including Ebstein’s Anomaly.• Our pediatric cardiac surgical teams performed more than 350 pediatric heart surgeries in 2012, up 48% from 2008.
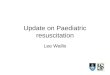
Interventional cardiologists in Le Bonheur’s catheterization lab used a new technique this summer to re-route hepatic
blood flow to the left pulmonary artery of an 18-year-old girl with a complex congenital heart condition – a complex single ventricle, status post bilateral cavo-pulmonary anastamoses with a Kawashima (because of interrupted IVC) with completion Fontan using an extra-hepatic conduit.
“She had developed extensive micro arterio-venous mal-formations (AVM) of the left lung. The AVMs formed secondary
due to lack of hepatic blood flow to the affected lung and would only resolve if the hepatic blood was re-routed to the left lung. The blood from the hepatic conduit streamed preferentially to the right lung at present,” said Shyam Sathanandam, MD. “Her oxygen satura-
tions were as low as 54 percent, and surgical conduit revision to re-route hepatic blood to the left lung carried great risk.”
The girl is a longtime patient of Le Bonheur Cardiothoracic Surgeon Chris Knott-Craig, MD, who conferred with Sathanandam about re-routing blood flow in the catheterization lab. Sathanandam planned the procedure for months, meticu-lously preparing for all scenarios he might encounter during this never before done procedure
in the cath lab.In the cath lab, Sathanandam and Cardiologist Rush
Waller, MD, initially stented the central pulmonary artery and dilated it to a large diameter.
After the stent was placed, the team pulled a wire through the struts of the stent from the left superior vena cava and snared it from a catheter introduced through the left hepatic vein. A wire rail was created. Incremental balloon sizes were used to dilate through the struts of the stent. Next, a Viabahn
Catheterization lab procedure lowers risk for heart patientCardiologists re-route hepatic blood flow to left pulmonary artery in special technique
Winter 2013
Heart UpdatePediatric
Referrals: 866-870-5570
www.lebonheur.org/heart
A pediatric partner of The University of Tennessee Health Science Center/College of Medicine and St. Jude Children’s Research Hospital
Memphis, Tennessee
100
98
96
94
92
90
88
86
84
82
80
Survival Rate by Procedure, 4 years
ASD VSD CoA AV Canal Aortic Valve Norwood TGA TOF Repair Surgery
LeB survival
STS survival
250
200
150
100
50
02008 2009 2010 2011 2012 Annualized
Non-CPB (non-cardiopulmonary bypass) CPB (cardiopulmonary bypass)
Cardiovascular Surgery Volumes2008-2012
Heart Institute highlights, outcomes: 2012
100
98
96
94
92
90
88
86
84
82
80category 1 category 2 category 3 category 4 category 5-6
Survival Rate by Complexity, 4 years
LeB survival
STS survival
continued on page 2
7.00
6.00
5.00
4.00
3.00
2.00
1.00
0.00
Comparative Case Mix Index 2010-2011, Cardiovascular Surgery Patients
LeB survival
?? ?
PHIS Hospitals
APR
DRG
Ped
s CM
I
Data Source: Pediatric Health Information Systems (PHIS), 2012.
400
350
300
250
200
150
100
50
0
Catheterization
2008 2009 2010 2011 2012 (Annualized)
Electrophysiology
Interventional Cardiac
Diagnostic Cardiac
The PHIS hospitals are 43 of the largest and most advanced children’s hospitals in America, and constitute the most demanding standards of pediatric service in America.

endoprosthesis was placed through the strut of this stent, followed by a larger diameter endoprosthesis telescoped into the first one proximally and the extra-hepatic conduit distally. This pinned both the prostheses and made the assembly stable.
Hepatic venous blood from the liver streamed to the left superior vena cava through the two telescoped prostheses and then through the first stent in the central pulmonary artery to both lungs. This ingenious yet sim-ple technique allowed hepatic blood to enter the right and left pulmonary arteries without needing to perform a complex operation.
One month later, the patient’s oxygen saturation was up to 94 percent, and Sathanandam expects all the pulmonary AVMs to resolve with time.
continued from page 1
Meet the TeamThe Heart Institute at Le Bonheur Children’s Hospital uses
the combined expertise of an advanced pediatric cardiac team to provide specialized care for children with congenital heart disease.
Pediatric cardiologists, pediatric cardiothoracic surgeons, cardi-ac intensivists, pediatric intensivists and anesthesiologists make up the Heart Institute. Advanced practice nurses, perfusionists, cardiac nurses, respiratory therapists and lab and imaging technicians are specially trained in pediatric cardiology care.
Leaders of the Heart Institute include:
Thomas Chin, co-director of Heart Institute and chief of CardiologyChin attended medical school at the University of Michigan and completed a fellowship in pedi-atric cardiology at the University of California, Los Angeles. He is board certified in pediatrics with a cardiology subspecialty. Chin is also pro-fessor and director of Cardiology for UTHSC. His patient care emphasis focuses on non-invasive
imaging, fetal and developmental cardiology, cardiomyopathies and pulmonary hypertension.
Christopher Knott-Craig, co-director of Heart Institute and chief of Cardiovascular Surgery Knott-Craig graduated from the University of Cape Town in South Africa and completed train-ing in cardiac surgery at the Groote Schuur Hospital in South Africa. He is board certified by the South African Medical & Dental Council in cardiothoracic surgery. Knott-Craig is also
a professor for UTHSC School of Medicine. His areas of special focus include neonatal/infant cardiac surgery, Ebstein’s anomaly, Ross Procedure, minimally invasive valve surgery, cardiopulmonary bypass, ambulatory thoracic surgery, hyperhidrosis and pediatric congenital heart disease.
Mayte Figueroa, medical director of CVICUFigueroa is a graduate of Mount Sinai School of Medicine and completed pediatric cardiology fellowships at both Mount Sinai Hospital and the Medical University of South Carolina. Figueroa is board certified in pediatrics and has a cardiology subspecialty. She is also an associate professor at The University of Tennessee Health Science Center (UTHSC). Her areas of focus include
developmental cardiology, pediatric cardiomyopathy, cardiovascu-lar disease, non-invasive pediatric cardiology and pediatric cardiac critical care.
Vijay Joshi, medical director of Non-invasive CardiologyJoshi attended medical school at the University of Vermont and completed a fellowship in pediatric cardiology at Children’s Hospital of Philadelphia. He is board certified by the American Board of Pediatrics with a cardiology subspecialty, and is also an associate professor at UTHSC. His patient care emphasis is on echo-
cardiography, fetal echocardiography, heart operation planning and 3-D echocardiography, fetal cardiology, cardiovascular disease, non-invasive pediatric cardiology, pregnant women for fetal heart evaluations, exercise- or sports-related cardiology and cardiac MRI.
B. Rush Waller, medical director of Catheterization LabWaller studied at UTHSC and completed fellow-ships in pediatric cardiology and pediatric inter-ventional cardiology at the Medical University of South Carolina. Waller is an associate professor at UTHSC and is board certified by the American Board of Pediatrics with a cardiology subspecial-ty. His areas of focus include interventional pedi-
atric cardiology, including therapeutic catheterizations for critically ill neonates, critically ill preoperative patients and complex cases of adults with congenital heart disease and transcatheter closure of intracardiac shunts.
Glenn Wetzel, medical director of Pediatric Electrophysiology, director of Fellowship ProgramWetzel completed fellowship training inpediatric cardiology at University of California at Los Angeles. He is board certified by the American Board of Pediatrics and has a cardiol-ogy subspecialty. Wetzel is also a professor at UTHSC. His special interests include pediatric
electrophysiology (arrhythmias), radiofrequency ablation and cryoablation, cardiomyopathy, pediatric pacemakers and internal defibrillator devices (ICDs).
Two studies conducted by researchers at Le Bonheur Children’s aim to better prepare caregivers for high-risk emergencies in the Cardiovascular
Intensive Care Unit (CVICU). Published in the latest edition of Pediatric Cardiology, both studies focus on the use of simulation-based training modules.
The first study’s findings suggest that simulation -based training is an effective method for improving the knowledge, ability and confidence levels of novice ECMO special-ists and physician trainees. Currently, training for ECMO— a form of temporary cardiopulmonary support – primarily uses didactic education and occasionally includes various hands-on training modules. Simulation courses with mannequins are available at a few centers as supplemental training, but simulation-based training is not required for certification. Results from the Le Bonheur study showed the simulation-based training is helpful and improves knowledge, ability and confidence for ECMO providers.
“ECMO is a complex life-saving medical therapy requiring rapid clinical decision-making skills in the event of a technical emergency. We have devel-oped a novel ECMO simulation training module and bedside safety checklists of common ECMO emergencies to train novice learners and to assist expert caregivers in this intricate management,” said Samir Shah, MD, a Le Bonheur intensivist and one of the researchers.
A second study proves that simulation-based team training is effective in increasing teamwork and collaboration among multidisciplinary teams in the CVICU during an emergency. The study’s training course simulated a post-pediatric surgery cardiac arrest, a high-risk clinical situation with high morbidity and mortality. Findings show that participation in the simulation-based training improve teamwork, confidence and communication during these high-risk events.
“We want to design innovative training for our staff that can, ultimately, improve patient safety and outcomes in the critical care environment,” said Mayte Figueroa, medical director of Le Bonheur’s CVICU and a primary researcher for both studies.
Studies show benefit of ECMO simulaton
Le Bonheur interventions cardiologists planned for months before using the cath lab to reroute blood flow on an 18-year-old patient

Interventional cardiologists successfully completed
Le Bonheur’s first Melody® valve procedure on May 23, 2012.
Shyam Sathanandam, MD, and Rush Waller, MD, implanted
the transcatheter pulmonary device in Le Bonheur’s catheteriza-
tion lab in a 32-year-old adult congenital heart patient under
minimal sedation.
The patient, 32-year-old Ashley Batchelor, was born with
Tetralogy of Fallot and had open
heart surgery soon after birth. She
underwent another operation at age
5 to receive a donor pulmonary valve
and then enjoyed a normal child-
hood despite having to limit physi-
cal activity, which caused her to feel
light-headed or nauseous. Ashley
married, moved to Memphis and
delivered a baby, Bailey, in 2007.
Ashley continued to see cardiolo-
gists annually for her heart defect.
By the time her child was 3, she grew
tired and lethargic, but dismissed her
symptoms as the result of juggling
work and family. After struggling to conceive a second child and
still not feeling like herself, Ashley’s OB/GYN recommended she
see experts at Le Bonheur’s Heart Institute.
Pediatric Cardiologist Ryan Jones, MD, found that one part
of her heart was enlarged, and an artery was smaller than normal.
A large percentage of the blood being pumped to the lung arter-
ies was regurgitating back into the right ventricle, the pumping
chamber for the blood going to the lungs.
“It made sense why I was so tired. And why I couldn’t have a
second baby,” said Ashley. “My heart couldn’t handle a pregnancy.”
Jones, along with Sathanandam and Waller, thought Ashley
would be a perfect candidate for the Melody valve — a new device
that could help Ashley and eliminate the need for a donor valve.
The Melody® valve is a valve harvested from a cow’s jugular
vein and sewn into a large stent. This valved stent is then deliv-
ered through a vein in the leg or neck to the heart and then
expanded and implanted with a large angioplasty balloon catheter.
It is primarily intended for use in patients
who have undergone multiple surgeries
that include using donor grafts to con-
nect the right ventricle to the pulmonary
arteries. The valve is indicated when these
donor grafts or valves fail.
“Ashley was an excellent candidate for
the Melody® valve because her donor valve
was no longer functioning, her right
ventricle was enlarged, she was symptom-
atic, and she had a good landing zone for
the large stent containing the new valve,”
Waller said. “This procedure prevented her
from having to have open-heart surgery.”
Sathanandam added that the Melody
valve gives patients “trans-catheter replacement of the pulmonary
valve that requires no cutting or stitching. The patients are typi-
cally discharged home the next day.”
Since the procedure, Ashley has been doing great. She does
not get short of breath and runs regularly on the treadmill for
30-40 minutes. She feels like a new person and is able to bal-
ance her life as a mom, a wife and as a pharmacist. Since Ashley’s
procedure in May, Sathanandam and Waller have successfully
implanted the Melody valve in several other patients — all of
whom describe complete resolution of symptoms.
Case Study: Melody valve eliminates need for donor valve
CVICU earns national honor
Le Bonheur’s Cardiovascular Intensive Care Unit has
earned a gold-level Beacon Award for Excellence from
the American Association of Critical Care Nurses. Le Bonheur
is just one of a few pediatric CVICUs to receive this award.
The award recognizes unit caregivers who successfully
improve patient outcomes, provide exceptional patient care
and align practices with AACN’s standards for a healthy work
environment.
“Our team is dedicated to providing the highest quality
care and committed to achieving the best outcomes in a
family-centered environment. The
Beacon Award for Excellence validates
our successful patient outcomes and
established practices,” said Mayte
Figueroa, MD, FACC, medical director
of Cardiovascular Critical Care Services.
Le Bonheur joins multi-center trial studying pulmonary hypertension treatment
L e Bonheur’s Heart Institute has joined a national pharmacokinetics
clinical trial aimed at finding better treatment for children between 6
months and 18 years of age with pulmonary artery hypertension.
The trial, sponsored by Eli Lilly and Co., will enroll patients to study the
pharmacokinetics of the drug Tadalafil in children with pulmonary hyperten-
sion. In a subsequent phase of the trial, the safety and effectiveness of the
drug in treating pulmonary hypertension in children will be determined.
Patients enrolled in this study will be under the close care of physicians and
the research staff, and will be monitored with echocardiograms, exercise
tests and blood testing. The principal investigator on this study in Memphis
is Thomas Chin, MD, the co-investigator is Alex Arevalo, MD, and the trial
coordinator is Neysa Rhoads.
Le Bonheur joins a handful of other select pediatric centers across the
country, including the Children’s Hospital of Philadelphia, the Children’s
Hospital of Denver, Sibley Children’s Hospital in Atlanta and Texas Children’s
Hospital in Houston. Physicians interested in enrolling their patients can
contact Chin at 901-287-5092.

Non-Profit Org.
US POSTAGEPAID
Memphis, TNPermit No. 3093
848 Adams Avenue
Memphis Tennessee 38103
Pediatric Heart Update is a publication of the Heart Institute at Le Bonheur Children’s Hospital
Thomas Chin, MD, co-director, Heart InstituteChris Knott-Craig, MD, co-director, Heart Institute
Bruce Alpert, MDMohammed Alsheikh-Ali, MDAlex Arevalo, MDJean Ballweg, MDMayte Figueroa, MDSteven Goldberg, MDRyan Jones, MDVijay Joshi, MDDai Kimura, MDTK Susheel Kumar, MDKelvin Lee, MDRonak Naik, MDShyam Sathanandam, MDAndreas Schwingshackl, MDSamir Shah, MDB. Rush Waller, MDGlenn Wetzel, MD, PhD
Ebstein’s research helps establish best practice
After following neonates with Ebstein’s Anomaly for nearly 20 years, the surgical team at
Le Bonheur’s Heart Institute has published a review of best treatments for the defect.
The results were published this past year in the World Journal for Pediatric and Congenital Heart Surgery in “Surgical Decision Making in Neonatal Ebstein’s Anomaly.” The study presented an algo-rithm for choosing the best management option for neonates based on analysis of the Heart Institute’s experience.
“Our extensive work with Ebstein’s Anomaly helped us establish what we consider best practice in treating neo-nates,” said Christopher Knott-Craig, MD, chief of Cardiovascular Surgery and co-director of Le Bonheur’s Heart Institute.
The authors looked at 48 neonates diagnosed with Ebstein’s Anomaly, all treated between 1994 and 2011. Of these, two died before intervention and 46 were either initially managed medically or underwent surgical intervention during the neonatal period.
Based on the neonates’ outcomes, researchers found that most symptomatic neonates with Ebstein’s will require early operation. Those with anatomic pulmo-nary atresia and mild tricuspid regurgitation may be best served initially with a modified Blalock-Taussig shunt and reduction atrioplasty.
Those with functional pulmonary atresia and severe tricuspid regurgitation may be best served with liga-tion of the main pulmonary artery and placement of a Blalock-Taussig shunt to pro-vide the best initial palliation. The review showed others should receive either biven-tricular repair or a single- ventricle palliation.
/ lebonheurchildrens@LeBonheurChild /lebonheurchildrens
100
95
90
85
80
75
70
65
60
Ebstein’s repair survival by age group, 4 years
neonate infant child adult
LeB survival
STS survival
Le Bonheur Heart Institute Publications: 2012Alpert BS. Validation of the Nihon Kohden PVM-2701/Impulse-1 automated device by both AAMI (2002) and ISO standards testing. Blood Press Monit. 2012;17:207-209.
Chan SY, Figueroa M, Spentzas T, Powell A, Holloway R, Shah S. Prospective assessment of novice learners in a simulation-based extracorporeal membrane oxygenation (ECMO) education program. Pediatr Cardiol. 2012, August.
Figueroa MI, Sepanski R, Goldberg SP, Shah S. Improving teamwork, confidence, and collaboration among members of a pediatric cardiovascular intensive care unit multidisciplinary team using simulation-based team training. Pediatr Cardiol. 2012, September.
Arevalo AR, Boston US, Goldberg SP, Becker JA, KnottCraig CJ. Starnes procedure in a neonate with pulmonary atresia and intact ventricular septum. Ann Thorac Surg. 2012;93:1703-1704.
Yohannan TM, Goldberg SP, Stamps JK, Mathis CA, Anthony Jr CL, Lasater OE, Knott-Craig CJ. Cardiac myxolipoma in a child: diagnosis and surgical management. Congenit Heart Dis. 2012, May.
GoldbergSP, Knott-CraigCJ, Joshi VM,Figueroa MI, Ballweg JA, Chin TK. Apical left ventriculotomy is safe in infants and young children requiring cardiac surgery. World J Pediatric Congenit Heart Surg 2012;3(4), 459-62
Jones RC, Rajasekaran S, Rayburn M, Tobias JD, Kelsey RM, Wetzel GT, Cabrera AG. Initial experience with conivaptan use in critically ill infants with cardiac disease. J Pediatr Pharmacol Ther. 2012 Jan;17(1):78-83. doi: 10.5863/1551-6776-17.1.78.
Knott-CraigCJ, GoldbergSP.Strategies to prevent complications from resternotomy [letter]. Ann Thorac Surg 2012;94:334-35.
Philip RR, Boston US, BallwegJA, GoldbergSP, Knott-Craig CJ. Iatrogenic pseudoaneurysm of the innominate artery in a neonate. J Card Surg2012;27(2):242-44
Knott-CraigCJ, GoldbergSP, BallwegJA, Boston US. Surgical decision making in neonatal Ebstein’s anomaly: an algorithmic approach based on 48 consecutive neonates. World J Pediatric Congenit Heart Surg2012;3(1)16-20
BallwegJA, GoldbergSP, Boston US, Joshi VM, Knott-Craig CJ. Technical modification to improve valve stability after aortic root replacement. SA Heart 2012 (submitted)
Kelsey RM, Alpert BS, Dahmer MK, Krushkal J, Quasney MW: Alpha-Adrenergic Receptor GenePolymorphisms and Cardiovascular Reactivity to Stress in Black Adolescents and Young AdultsPsychophysiology: 2012;49:401-412.
McCarville MB, Kaste SC, Hoffer FA, Khan RB, Walton RC, Alpert BS, Furman WL, Li C, Xiong X: Contrast Enhanced Sonography of Malignant Pediatric Abdominal and Pelvic Solid Tumors: Preliminary Safety and Feasibility Data. Pediatr Radiol: Pediatr Radiol 2012 Jul;42(7):824-33. Epub 2012 Jan 17.
David Gallick, Bruce A. Friedman, Bruce S. Alpert, John D. Seller, David E. Quinn, David Osborn, members of the AAMI Sphygmomanometer Committee: Response to – Blood Pressure Monitoring: Blood Press Monit 2012, 17:45.
Alpert BS, Validation of the Nihon Kohden PVM-2701/Impulse-1 automated device by both AAMI (2002) and ISO Standards testing. Blood Press Monit 2012, 17:207-209.
Alpert BS. Are kiosk blood pressure readings trustworthy? Blood Press Monit 2012, 17:257-258.
Lee KC, Danton GH, Kardon RE. Three-Dimensional Computed Tomographic Analysis of a Rare Left Coronary to Left Ventricle Fistula. Pediatr Cardiol. 2012.
Gregory T. Armstrong, Vijaya M. Joshi, Liang Zhu, Deokumar Srivastava, Nan Zhang, Kirsten K Ness, Dennis C. Stokes, Matthew T. Krasin, James A. Fowler, Leslie L. Robison, Melissa M. Hudson, and Daniel M. Green. Elevated Tricuspid Regurgitant Jet Velocity by Doppler Echocardiography in Adult Survivors of Childhood Cancer: A Report from the St. Jude Lifetime Cohort Study. Accepted for publication J Clinical Oncology /2012/430702
Gregory T. Armstrong, Juan Carlos Plana, Nan Zhang, Deokumar Srivastava, Daniel M Green, Kirsten K Ness, F. Daniel Donovan, Monika L Metzger, Alejandro Arevalo, Jean-Bernard Durand, Vijaya Joshi, Melissa M Hudson, Leslie L Robison, and Scott Flamm. Screening Adult Survivors of Childhood Cancer for Cardiomyopathy: Comparison of Echocardiography and Cardiac MRI. J Clin Oncol 8.10.2012 Vol30 No23pp2876-2884
Kevin Krull, Noah D. Sabin, Daniel Green, Alejandro Arevalo, Matthew Krasin, Melissa Hudson. Neurocognitive Function and CNS Integrity in Adult Survivors of Childhood Hodgkin LymphomaJ Clin Oncol Sept. 4th, 2012. Volume 42
Stephen Cyran, Ronak Naik, Devyani Chowdhury. Stress echocardiography: a useful tool in children with aortic stenosis. Journal of the American College of Cardiology, Volume 59, Issue 13, Supplement, 27 March 2012, Page E801
Shyam K Sathanandam, Matthew J. Gillespie, Yoav Dori, Matthew A. Harris, Andrew C. Glatz, and Jonathan J. Rome: Bilateral Branch Pulmonary Artery Melody Valve Implantation for Treatment of Complex Right Ventricular Outflow Tract Dysfunction in a High-Risk Patient. Circ Cardiovasc Interv. 2012;4:e21-e23
Book ChaptersKnott-Craig CJ, Goldberg SP. Early presentation of Ebstein’s Anomaly. In: da Cruz E, Hraska V, Ivy DD, Jaggers J, eds. Pediatric Cardiology, Cardiac Surgery, and Intensive Care. Springer-Verlag, London 2012 (in press…due out 7/31/2013)
Knott-Craig CJ, Goldberg SP. The Ross procedure in children. In: Franco KL, Thourani VH, eds. Cardiothoracic Surgery Review. Philadelphia, PA: Lippincott, Williams, & Wilkins, 2012
Morgenstein BZ, Gallick D, Alpert BS. Casual Blood Pressure Methodology. In PediatricHypertension, Flynn JT, Ingelfinger JR, Portman R, editors. Humana Press, 2012, in press.
Sathanandam, Shyam. Evaluation and Therapy: Neonatal Critical Heart Disease. Shaddy R, Rychick J, Marie Gleason, eds. Pediatric Practice: Cardiology. McGraw-Hill Publishers, NY, NY.
Sathanandam, Shyam. Cardiology. Shah B, Lucchesi M, eds. The Atlas of Pediatric Emergency Medicine, Second Edition.