Embed Size (px)
Citation preview

Pediatric Head and Neck Pediatric Head and Neck MalignanciesMalignancies
Elizabeth J. Rosen, MDElizabeth J. Rosen, MD
Ronald W. Deskin, MDRonald W. Deskin, MD
4/9/034/9/03

Pediatric CancerPediatric Cancer
22ndnd leading cause of death in age range of leading cause of death in age range of 5-14 years5-14 years
1/333 children diagnosed annually1/333 children diagnosed annually
11,000 new cases in children under 20 11,000 new cases in children under 20 years of age each yearyears of age each year
Head and Neck Malignancies make up 5% Head and Neck Malignancies make up 5% of pediatric cancer cases = 500 kids/yearof pediatric cancer cases = 500 kids/year

Pediatric CancerPediatric Cancer
Albright, et al in Archives of Oto-HNS Albright, et al in Archives of Oto-HNS June 2002June 2002– Overall annual incidence of pediatric Overall annual incidence of pediatric
cancercancer1973-1975 = 11.22 cases/100,000 person/years1973-1975 = 11.22 cases/100,000 person/years
1994-1996 = 14.03 cases/100,000 person years1994-1996 = 14.03 cases/100,000 person years
Increase of 25%Increase of 25%
– Annual incidence of pediatric H&N cancerAnnual incidence of pediatric H&N cancer1973-1975 = 1.10 cases/100,000 person/years1973-1975 = 1.10 cases/100,000 person/years
1994-1996 = 1.49 cases/100,000 person/years1994-1996 = 1.49 cases/100,000 person/years
Increase of 35%Increase of 35%

Pediatric Head and Neck Pediatric Head and Neck MalignanciesMalignancies
Lymphoma = 59%Lymphoma = 59%Rhabdomyosarcoma = 13%Rhabdomyosarcoma = 13%Thyroid Malignancies = 10%Thyroid Malignancies = 10%Nasopharyngeal Carcinoma = 5%Nasopharyngeal Carcinoma = 5%Neuroblastoma = 5%Neuroblastoma = 5%Nonrhabdomyosarcoma Soft-tissue Sarcoma Nonrhabdomyosarcoma Soft-tissue Sarcoma = 4.5%= 4.5%Salivary Gland Malignancies = 2.5%Salivary Gland Malignancies = 2.5%Malignant Teratoma = 1%Malignant Teratoma = 1%OthersOthers

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
Lymphoma = 11.5% of all pediatric Lymphoma = 11.5% of all pediatric cancerscancers
NHL occurs in 60% of lymphoma casesNHL occurs in 60% of lymphoma cases
M:F = 3:1M:F = 3:1
Peak incidence between 7-11 years of agePeak incidence between 7-11 years of age
Increased risk with T-cell deficiencyIncreased risk with T-cell deficiency– Congenital immunodeficiency syndromesCongenital immunodeficiency syndromes– Acquired immunodeficiency syndromeAcquired immunodeficiency syndrome– Immunosuppressive drug therapyImmunosuppressive drug therapy

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
Low-, intermediate-, and high-grade Low-, intermediate-, and high-grade lesions lesions
90% of children with NHL have high-grade 90% of children with NHL have high-grade disease at presentationdisease at presentation
High-gradeHigh-grade– Large cell lymphomaLarge cell lymphoma– Lymphoblastic lymphomaLymphoblastic lymphoma– Small cell noncleaved lymphomaSmall cell noncleaved lymphoma

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
Large cell lymphomaLarge cell lymphoma– 27% pediatric cases27% pediatric cases– t(2;5) anomalyt(2;5) anomaly– Rare presentation inRare presentation in
H&NH&N
From, Diagnostic Surgical Pathology of the Head and Neck, From, Diagnostic Surgical Pathology of the Head and Neck, W.B.Saunders, p 762.W.B.Saunders, p 762.

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
Lymphoblastic Lymphoblastic lymphomalymphoma– 29% pediatric29% pediatric
casescases– t(7 or 14)t(7 or 14)– Mediastinal massMediastinal mass
From, Diagnostic Surgical Pathology of theFrom, Diagnostic Surgical Pathology of the
Head and Neck, W.B.Saunders, p 759.Head and Neck, W.B.Saunders, p 759.

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
Small cell noncleavedSmall cell noncleaved– 34% pediatric cases34% pediatric cases– Burkitt’s lymphomaBurkitt’s lymphoma
Epstein-Barr virusEpstein-Barr virus
t(8;2,14,22)t(8;2,14,22)
MandibleMandible
Head and NeckHead and Neck
From, Surgical Pathology of the Head and Neck, From, Surgical Pathology of the Head and Neck,
Lippincott Williams & Wilkins, p 161.Lippincott Williams & Wilkins, p 161.

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
Presentation in the H&N in 5-10% of casesPresentation in the H&N in 5-10% of cases– Cervical lymphadenopathyCervical lymphadenopathy– Salivary gland, larynx, sinuses, orbit, scalpSalivary gland, larynx, sinuses, orbit, scalp– Waldeyer’s ringWaldeyer’s ring
Asymmetric tonsils-how concerning is it?Asymmetric tonsils-how concerning is it?
– Associated symptomsAssociated symptomsFever, night sweats, weight lossFever, night sweats, weight loss

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
EvaluationEvaluation– H&PH&P– BiopsyBiopsy
TonsillectomyTonsillectomyLymph nodeLymph node
– Staging w/uStaging w/uBlood studiesBlood studiesLumbar punctureLumbar punctureBone marrow biopsyBone marrow biopsyCT chest/abdomen/pelvisCT chest/abdomen/pelvisBone scanBone scan

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
Multiagent ChemotherapyMultiagent Chemotherapy– CyclophosphamideCyclophosphamide– DoxorubicinDoxorubicin– VincristineVincristine– PrednisonePrednisone– +/- Methotrexate+/- Methotrexate
– XRT—not routinely usedXRT—not routinely used

Non-Hodgkin’s LymphomaNon-Hodgkin’s Lymphoma
SurvivalSurvival– Overall Stage I and II NHL = 85-95%Overall Stage I and II NHL = 85-95%– Overall Stage III and IV NHL = 65-75%Overall Stage III and IV NHL = 65-75%– Stage III and IV BL = 75-85%Stage III and IV BL = 75-85%

Hodgkin’s DiseaseHodgkin’s Disease
Less common than NHLLess common than NHL
More frequently in 15-20 y/o populationMore frequently in 15-20 y/o population
4% under 10 years 4% under 10 years
M:F = 3:1M:F = 3:1
Association with EBVAssociation with EBV

Hodgkin’s DiseaseHodgkin’s Disease
Nodular SclerosingNodular Sclerosing
From, Diagnostic Surgical Pathology of the Head and Neck, From, Diagnostic Surgical Pathology of the Head and Neck, W.B.Saunders, p 750 & 764.W.B.Saunders, p 750 & 764.
Lymphocyte PredominantLymphocyte Predominant

Hodgkin’s DiseaseHodgkin’s Disease
Mixed CellularityMixed Cellularity
From, Diagnostic Surgical Pathology of the Head and Neck, From, Diagnostic Surgical Pathology of the Head and Neck, W.B.Saunders, p 750.W.B.Saunders, p 750.
Lymphocyte DepletedLymphocyte Depleted

Hodgkin’s DiseaseHodgkin’s Disease
PresentationPresentation– Asymmetric lymphadenopathy—90%Asymmetric lymphadenopathy—90%
Firm, rubberyFirm, rubbery
Supraclavicular fossaSupraclavicular fossa
– Spleen, liverSpleen, liver– Constitutional symptoms—1/3 of casesConstitutional symptoms—1/3 of cases
Fever, night sweats, anorexia, weakness, weight Fever, night sweats, anorexia, weakness, weight lossloss

Hodgkin’s DiseaseHodgkin’s Disease
EvaluationEvaluation– H&PH&P– Biopsy = Reed-Biopsy = Reed-
Sternberg cellsSternberg cells– Staging w/uStaging w/u
Similar to NHLSimilar to NHLLaparotomyLaparotomy
– ControversialControversial
From, Principles and Practice of PediatricFrom, Principles and Practice of PediatricOncology, Lippincott Williams & Wilkins,Oncology, Lippincott Williams & Wilkins,P 640.P 640.

Hodgkin’s DiseaseHodgkin’s Disease

Hodgkin’s DiseaseHodgkin’s Disease
Localized diseaseLocalized disease– Extended field XRTExtended field XRT
Disseminated diseaseDisseminated disease– MOPP = nitrogen mustard, vinblastine, MOPP = nitrogen mustard, vinblastine,
procarbazine, prednisoneprocarbazine, prednisone– ABVD = adriamycin bleomycin, vincristine, ABVD = adriamycin bleomycin, vincristine,
dacarbazinedacarbazine

Hodgkin’s DiseaseHodgkin’s Disease
SurvivalSurvival– Stages I, II, and III = 90%Stages I, II, and III = 90%– Stage IV = 75-80%Stage IV = 75-80%

RhabdomyosarcomaRhabdomyosarcoma
Most common soft tissue sarcoma in Most common soft tissue sarcoma in childrenchildren
4.5 cases/1,000,000 children under 14 4.5 cases/1,000,000 children under 14 yearsyears
Majority diagnosed before age 10Majority diagnosed before age 10
M:F = 1.5:1M:F = 1.5:1

RhabdomyosarcomaRhabdomyosarcoma
EmbryonalEmbryonal– Most common in kids:Most common in kids:
60-70% of cases60-70% of cases
– Chromosome 11p15 Chromosome 11p15 deletiondeletion
– Lack of gene Lack of gene
amplificationamplification– Hyperdiploid DNAHyperdiploid DNA
From, Surgical Pathology of the Head and Neck, LippincottFrom, Surgical Pathology of the Head and Neck, Lippincott
Williams & Wilkins, p 157.Williams & Wilkins, p 157.

RhabdomyosarcomaRhabdomyosarcoma
AlveolarAlveolar– 20% of pediatric cases20% of pediatric cases– Chromosomal translocation: Chromosomal translocation:
t(2;13) or t(1;13)t(2;13) or t(1;13)
– Gene amplificationGene amplification– Tetraploid DNATetraploid DNA
From, Surgical Pathology of the Head and Neck, Lippincott Williams & Wilkins,From, Surgical Pathology of the Head and Neck, Lippincott Williams & Wilkins,
p 157.p 157.

RhabdomyosarcomaRhabdomyosarcoma
BotryoidBotryoid– 5-10% of pediatric 5-10% of pediatric
casescases– Grape-like tumor Grape-like tumor
massesmasses
PleomorphicPleomorphic– Rare in childrenRare in children
From, Diagnostic Surgical Pathology of the Head and Neck,From, Diagnostic Surgical Pathology of the Head and Neck,
W.B.Saunders, p 554.W.B.Saunders, p 554.

RhabdomyosarcomaRhabdomyosarcoma
Most common site of presentation is Most common site of presentation is H&N--40% of casesH&N--40% of cases
1/3 of cases involve the orbit1/3 of cases involve the orbit
Oral cavity & oropharynx, face & neck, Oral cavity & oropharynx, face & neck, middle ear & mastoid, nose & paranasal middle ear & mastoid, nose & paranasal sinusessinuses
Localized swelling, proptosis, nasal Localized swelling, proptosis, nasal obstruction, epistaxis, otorrhea, hearing obstruction, epistaxis, otorrhea, hearing loss, fetor and cranial nerve deficitsloss, fetor and cranial nerve deficits

RhabdomyosarcomaRhabdomyosarcoma
EvaluationEvaluation– H & PH & P– Biopsy Biopsy – CT/MRI of primaryCT/MRI of primary– Metastatic w/u Metastatic w/u
Chest CTChest CT
Bone scanBone scan
Bone marrow biopsyBone marrow biopsy

RhabdomyosarcomaRhabdomyosarcoma
Intergroup Rhabdomyosarcoma Study Intergroup Rhabdomyosarcoma Study Clinical Grouping Classification (IRSCGC)Clinical Grouping Classification (IRSCGC)

RhabdomyosarcomaRhabdomyosarcoma

RhabdomyosarcomaRhabdomyosarcoma
TreatmentTreatment– SurgerySurgery
Goal = complete excision with marginGoal = complete excision with margin
Consider morbidity of surgeryConsider morbidity of surgery– Cranial nervesCranial nerves– CosmesisCosmesis
DebulkingDebulking
Exception is orbital rhabdomyosarcoma—surgery Exception is orbital rhabdomyosarcoma—surgery offers no advantage over chemo/XRToffers no advantage over chemo/XRT

RhabdomyosarcomaRhabdomyosarcoma
TreatmentTreatment– ChemotherapyChemotherapy
Low-risk: vincristine, dactinomycin, +/- Low-risk: vincristine, dactinomycin, +/- cyclophosphamidecyclophosphamide
Intermediate- and High-risk: vincristine, Intermediate- and High-risk: vincristine, dactinomycin and cyclophosphamidedactinomycin and cyclophosphamide

RhabdomyosarcomaRhabdomyosarcoma
TreatmentTreatment– Radiation TherapyRadiation Therapy
Postoperative microscopic diseasePostoperative microscopic disease– 4,000-4,500 cGy4,000-4,500 cGy
Gross diseaseGross disease– 4,500-5,000 cGy4,500-5,000 cGy
Hyperfractionated XRTHyperfractionated XRT
BrachytherapyBrachytherapy

RhabdomyosarcomaRhabdomyosarcoma
SurvivalSurvival– Before 1970 = 33%Before 1970 = 33%– Currently = 70%Currently = 70%– Intergroup Rhabdomyosarcoma StudyIntergroup Rhabdomyosarcoma Study– Prognostic factorsPrognostic factors
Tumor sizeTumor size
Regional node statusRegional node status
Margins after surgeryMargins after surgery
Genetic factorsGenetic factors

NeuroblastomaNeuroblastoma
Most common extracranial solid tumor in Most common extracranial solid tumor in childrenchildren
8-10% of childhood cancers8-10% of childhood cancers
90-95% of cases diagnosed before age 1090-95% of cases diagnosed before age 10
More common in boys and CaucasiansMore common in boys and Caucasians
? Genetic or environmental factors? Genetic or environmental factors

NeuroblastomaNeuroblastoma
““Small blue round cell” tumorSmall blue round cell” tumor
Immunohistochemical stains: Immunohistochemical stains: neurofilament proteins, neurofilament proteins, synaptophysin, NSEsynaptophysin, NSE
Electron microscopy: Electron microscopy: neurosecretory granules, neurosecretory granules, microtubules and filamentsmicrotubules and filaments
Chromosome 1 deletions or Chromosome 1 deletions or N-N-mycmyc oncogene amplification oncogene amplification
From, Principles and Practice of Pediatric Oncology, Lippincott Williams & Wilkins,From, Principles and Practice of Pediatric Oncology, Lippincott Williams & Wilkins,
p 903.p 903.

NeuroblastomaNeuroblastoma
2-5% in the H&N region—most often as 2-5% in the H&N region—most often as lateral neck masslateral neck mass
Airway obstruction, aspiration, dysphagia, Airway obstruction, aspiration, dysphagia, Horner’s syndrome, proptosis, periorbital Horner’s syndrome, proptosis, periorbital ecchymosis, opthalmoplegia, conjunctival ecchymosis, opthalmoplegia, conjunctival or eyelid edema, papilledemaor eyelid edema, papilledema
Heterochromia iridesHeterochromia irides

NeuroblastomaNeuroblastoma
EvaluationEvaluation– H & PH & P– BiopsyBiopsy– Urine catecholamine studiesUrine catecholamine studies– Metastatic w/uMetastatic w/u
CXRCXR
Bone marrow biopsyBone marrow biopsy
Bone scanBone scan
CT or MRI CT or MRI

NeuroblastomaNeuroblastoma

NeuroblastomaNeuroblastoma
TreatmentTreatment– SurgerySurgery– ChemotherapyChemotherapy
Intermediate- or High-riskIntermediate- or High-risk
Low-risk with recurrenceLow-risk with recurrence
Cyclophosphamide, ifosfamide, doxorubicin, Cyclophosphamide, ifosfamide, doxorubicin, teniposide, etoposide, cisplatin or carboplatinteniposide, etoposide, cisplatin or carboplatin
– Radiation TherapyRadiation TherapyLimited useLimited use

NeuroblastomaNeuroblastoma
Prognostic FactorsPrognostic Factors– Age at diagnosisAge at diagnosis– Stage at diagnosisStage at diagnosis
Overall, Stage I or II = 75-90%Overall, Stage I or II = 75-90%
Infants: Stage III = 80-90%; Stage IV = 60-Infants: Stage III = 80-90%; Stage IV = 60-75%75%
Children: Stage III = 50%; Stage IV = 15%Children: Stage III = 50%; Stage IV = 15%

EsthesioneuroblastomaEsthesioneuroblastoma
100 pediatric cases in the literature100 pediatric cases in the literature
Teenagers, boys > girlsTeenagers, boys > girls
PresentationPresentation
HistologyHistology
StagingStaging
TreatmentTreatment

EsthesioneuroblastomaEsthesioneuroblastoma
HistologyHistology
From, Surgical Pathology of the Head and Neck, Lippincott Williams & Wilkins, p 86.From, Surgical Pathology of the Head and Neck, Lippincott Williams & Wilkins, p 86.

EsthesioneuroblastomaEsthesioneuroblastoma
100 pediatric cases in the literature100 pediatric cases in the literature
Teenagers, boys > girlsTeenagers, boys > girls
PresentationPresentation
HistologyHistology
StagingStaging
TreatmentTreatment

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma
5% of pediatric H&N malignancies5% of pediatric H&N malignanciesTeenagers, M=F, African AmericansTeenagers, M=F, African AmericansSignificantly higher incidence in ChineseSignificantly higher incidence in Chinese– HLA-A2, HLA-B-Sin 2HLA-A2, HLA-B-Sin 2– Smoke, dust, nitrosamine rich salted fishSmoke, dust, nitrosamine rich salted fish
EBVEBV
From, Diagnostic Surgical Pathology of From, Diagnostic Surgical Pathology of
the the Head and Neck, W.B.Saunders, p 43.Head and Neck, W.B.Saunders, p 43.

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma
WHO ClassificationWHO Classification– Type I – squamous cell Type I – squamous cell
carcinomacarcinoma– Type II – non-keratinizing Type II – non-keratinizing
squamous cell carcinomasquamous cell carcinoma– Type III – undifferentiated Type III – undifferentiated
or lymphoepitheliomaor lymphoepithelioma
From, Diagnostic Surgical Pathology of the Head From, Diagnostic Surgical Pathology of the Head and Neck, and Neck, W.B.Saunders, p 43W.B.Saunders, p 43

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma
PresentationPresentation– Neck mass and hearing lossNeck mass and hearing loss– Nasal obstruction, rhinorrhea, epistaxis, Nasal obstruction, rhinorrhea, epistaxis,
headache, otalgiaheadache, otalgia– Cranial neuropathyCranial neuropathy
Abducens palsyAbducens palsy
CN III, IV, VCN III, IV, V
CN IX, X, XIICN IX, X, XII

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma
EvaluationEvaluation– H & PH & P– EndoscopyEndoscopy– BiopsyBiopsy– CT/MRI for local extentCT/MRI for local extent– Metastatic w/uMetastatic w/u
CT chest/abdomenCT chest/abdomen
Bone scanBone scan

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma
TreatmentTreatment– Radiation TherapyRadiation Therapy
Primary and local lymphaticsPrimary and local lymphatics
6,500-7,000 cGy6,500-7,000 cGy
– ChemotherapyChemotherapyAdvanced diseaseAdvanced disease
Vincristine, doxorubicin, cyclophosphamide, Vincristine, doxorubicin, cyclophosphamide, cisplatin, 5-fluorouracilcisplatin, 5-fluorouracil
– SurgerySurgery

Nasopharyngeal CarcinomaNasopharyngeal Carcinoma
SurvivalSurvival– Overall 5-year = 40%Overall 5-year = 40%
– Prognostic FactorsPrognostic FactorsPositivePositive
– Locally confined diseaseLocally confined disease– Ipsilateral nodesIpsilateral nodes
NegativeNegative– Bilateral nodesBilateral nodes– CNS penetrationCNS penetration

Soft-tissue SarcomasSoft-tissue Sarcomas
4.5% of pediatric H&N malignancies4.5% of pediatric H&N malignanciesDiverse group of tumorsDiverse group of tumors
fibrosarcomafibrosarcoma epitheloid sarcomaepitheloid sarcomasynovial sarcomasynovial sarcoma chondrosarcomachondrosarcomadermatofibrosarcoma protuberansdermatofibrosarcoma protuberansosteosarcomaosteosarcoma leiomyosarcomaleiomyosarcomahemangiopericytomahemangiopericytomaliposarcomaliposarcoma clear-cell clear-cell sarcomasarcoma

Soft-tissue SarcomasSoft-tissue Sarcomas
PresentationPresentation
EvaluationEvaluation
StagingStaging
TreatmentTreatment
SurvivalSurvival

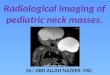
Primitive Neuroectodermal Primitive Neuroectodermal TumorsTumors
RareRare
42% involve the H&N region42% involve the H&N region
““small blue round cell” tumorsmall blue round cell” tumor
From, Diagnostic Surgical Pathology of the Head and Neck, W.B.Saunders, p 527.From, Diagnostic Surgical Pathology of the Head and Neck, W.B.Saunders, p 527.

Primitive Neuroectodermal Primitive Neuroectodermal TumorsTumors
PresentationPresentation
EvaluationEvaluation
StagingStaging
TreatmentTreatment
SurvivalSurvival

ConclusionConclusion
Rare diseasesRare diseases
Broad differential diagnosisBroad differential diagnosis
High index of suspicionHigh index of suspicion
Early diagnosisEarly diagnosis
Accurate stagingAccurate staging
Multimodality therapyMultimodality therapy
Improved prognosisImproved prognosis