Embed Size (px)
Citation preview

PEDIATRIC GI:PEDIATRIC GI:EM GRAND EM GRAND
ROUNDSROUNDS
INSERVICE BIZZ-BUZZINSERVICE BIZZ-BUZZ
VERSUS REALITY VERSUS REALITY

WK Mallon WK Mallon MD DTMH MD DTMH
FAAEM FAAEM FACEPFACEP
Clinical Professor of Emergency Clinical Professor of Emergency MedicineMedicine
Department of Emergency MedicineDepartment of Emergency MedicineStony Brook University (SUNY) Stony Brook University (SUNY) Director : Division of International Director : Division of International
EMEM

DECLARATIODECLARATIONSNS
Emergency Medical Abstracts Emergency Medical Abstracts
Advisory BoardAdvisory Board Sonosite supported “Code Black” Sonosite supported “Code Black”
the documentarythe documentary (no salary)(no salary) EMRAP, NEMBR, LLSA productsEMRAP, NEMBR, LLSA products ACEP, AAEM, SOCHIMU “fellow” ACEP, AAEM, SOCHIMU “fellow” Past-President of Cal/ACEPPast-President of Cal/ACEP No stock, salary, or pharma No stock, salary, or pharma
payments payments


A 20 MINUTE MENUA 20 MINUTE MENU
IntussusceptionIntussusception Pyloric StenosisPyloric Stenosis Meckels DiverticulumMeckels Diverticulum Peds AppyPeds Appy Mesenteric AdenitisMesenteric Adenitis Epiploic AppendagitisEpiploic Appendagitis
INSERVICE RICH MATERIALINSERVICE RICH MATERIAL

HYPERTROPHIC PYLORIC HYPERTROPHIC PYLORIC STENOSIS STENOSIS
TYPICAL STORYTYPICAL STORY Eldest 1Eldest 1stst born male born male Age: 6-8weeksAge: 6-8weeks AfebrileAfebrile Projectile vomitingProjectile vomiting Palpable mobile “olive”Palpable mobile “olive” UTZ diagnosis v. clinicalUTZ diagnosis v. clinical DehydrationDehydration Surgical: pyloric Surgical: pyloric
myotomy via laporoscopy myotomy via laporoscopy
REALITYREALITY Epi variableEpi variable Age: more variableAge: more variable PremiesPremies URI: febrileURI: febrile Just N/V not projectileJust N/V not projectile No olive appreciatedNo olive appreciated UTZ not so easyUTZ not so easy Variable hydrationVariable hydration Medical RX: atropine Medical RX: atropine

PYLORIC STENOSIS: A RETROSPECTIVE STUDY OF AN AUSTRALIAN POPN
Gotley, L.M., et al, Emerg Med Australasia 21(5):407, October 2009BACKGROUND: The "classic" presentation of pyloric stenosis includes projectile vomiting, a palpable "olive," and visible peristalsis with a test feed in a six- to eight-week-old infant with hypochloremic metabolic alkalosis. Increasing availability of ultrasound might be associated with earlier diagnosis, in the absence of typical signs and symptoms.METHODS: These Australian authors performed an implicit chart review in 329 children given a diagnosis of idiopathic hypertrophic pyloric stenosis (HPS) after presentation to a tertiary pediatric hospital over an eleven-year period.RESULTS: The patients were predominantly male (84%); 12% had a family history of HPS and 19% were born prematurely. The median age at presentation was five weeks overall, and six weeks for preterm infants. The median symptom duration was one week. About 15% of the children failed to exhibit any of the classic findings, 40% had only one of these, and only 15% exhibited the entire classic triad. Vomiting was reported for most of the children (97%), and was described as projectile in 80%. About 60% had an elevated serum bicarbonate level and 30% had hypochloremia. Ultrasonography was performed in nearly 90% of cases. Over time, there was an increase in the performance of laparoscopic correction.CONCLUSIONS: In this series, most infants with idiopathic hypertrophic pyloric stenosis were male, and many were born prematurely. Most did not exhibit all of the classic signs and symptoms on presentation. The authors suggest consideration of HPS in all infants presenting with vomiting, particularly in those below three months of age. Copyright 2010 by Emergency Medical Abstracts - All Rights Reserved 4/10 - #17

INTUSSUSCEPTIONINTUSSUSCEPTIONTYPICAL STORYTYPICAL STORY
Age 4m-24mAge 4m-24m Intermittent crampingIntermittent cramping Normal between eventsNormal between events Vertical R sided massVertical R sided mass Afebrile (? Recent VAX)Afebrile (? Recent VAX) Paucity of gas RUQPaucity of gas RUQ Currant jelly stool in Currant jelly stool in
diaperdiaper UTZ shows target signUTZ shows target sign Admit peds surgeryAdmit peds surgery Air enema reductionAir enema reduction Watch for fixed leadsWatch for fixed leads
REALITYREALITY UncommonUncommon Age range greaterAge range greater Vexing diagnosis easily Vexing diagnosis easily
missedmissed Atypical HX: lethargyAtypical HX: lethargy No episodes in the EDNo episodes in the ED No mass No mass May be febrile: URI, or VAXMay be febrile: URI, or VAX Currant jelly: late & Currant jelly: late &
unreliableunreliable UTZ may not be diagnosticUTZ may not be diagnostic After reduction ? D/CAfter reduction ? D/C Fixed leads missed Fixed leads missed


PAEDIATRIC INTUSSUSCEPTION: EPIDEMIOLOGY AND OUTCOMEBlanch, A.J.M., et al, Emerg Med Australasia 19(1):45, February 2007BACKGROUND: Several studies have reported that the "classic" signs and symptoms of intussusception (abdominal pain, red currant jelly stool, vomiting and a palpable abdominal mass) are often not present on presentation.METHODS: These Australian authors performed a chart review for 141 presentations of intussusception in 135 children aged one month to nearly twelve years (median, nine months) managed at a tertiary pediatric hospital over a ten-year period.RESULTS: Nearly two-thirds of the patients were aged one year or younger, and only eight (6%) were aged four years or older. The male:female ratio was 2:1. Fewer than half the patients (46%) had at least three of the four "classic" signs and symptoms. The most common findings were vomiting (78%), "legs drawn up" and/or abdominal pain (69%) and lethargy-irritability (67%). A palpable abdominal mass was documented in 50%, and rectal bleeding and/or currant jelly stool in only 35%. Other findings included pallor and/or sweating (42%), diarrhea (23%), poor feeding (17%) and abdominal distention (10%). A provisional diagnosis of intussusception was made from one hour to 183 days after presentation (median, 15 hours), and was confirmed by ultrasonography in two-thirds of the cases from two hours to 183 days after symptom onset (median, 19 hours). In 46% of the episodes, intussusception was not the initial diagnosis, and the correct diagnosis was delayed beyond 24 hours in 43%. Surgery was required in 21 patients.CONCLUSIONS: The authors suggest a high index of suspicion of intussusception in young children with vomiting and/or abdominal pain, even in the absence of other "classic" signs and symptoms. 12 references (andrew [email protected])

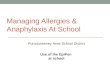
INTUSSUSCEPTIONINTUSSUSCEPTION

ULTRASOUND ULTRASOUND FINDINGSFINDINGS

VALIDATION OF US AS A FIRST-LINE DIAGNOSTIC TEST FOR ASSESSMENT OF PEDIATRIC ILEOCOLIC INTUSSUSCEPTION
Hryhorczuk, A.L., et al, Ped Radiol 39:1075, October 2009BACKGROUND: Ultrasonography (US) was first suggested as a diagnostic modality for intussusception in the 1980s, but is not widely used for this purpose.METHODS: This study, from the University of Michigan, reports on the use of US in 814 children aged 10 years and younger between 2001 and 2007, following explicit training of ultrasonographers and radiologists in use of US as the primary diagnostic test in cases of possible intussusception. The final diagnosis in those with a positive US was based on a subsequent enema (except for one child who went straight to surgery); an enema was also done in 27 (3%) of those with a negative US, while the other 97% were classified as "true negative" if they "did not return" (although the nature of any follow-up is not described).RESULTS: A total of 12.2% of the children were given an ultimate diagnosis of intussusception. Overall, 13.8% of the US studies were considered positive for intussusception, and 16.7% of the negative US studies were felt to demonstrate other clinically relevant findings. Two studies (0.25%) were considered nondiagnostic. There were 15 false- positive and (reportedly) 2 false-negative US studies, such that sensitivity and specificity were each 97.9%, with positive and negative predictive values of 86.6% and 99.7%, respectively.CONCLUSIONS: The authors note that many of the US studies (exact percentage not detailed) were performed at night or on a weekend, and interpreted by a resident or general emergency radiologist. Although their study suffers from severe work-up bias, they feel that ultrasonography, which is noninvasive, is highly accurate, and therefore an ideal first-line imaging technique for the assessment of possible intussusception in children. 14 references ([email protected] -

ROTASHIELD, ROTAREX, ROTASHIELD, ROTAREX, AND ROTATEQ VACCINESAND ROTATEQ VACCINES
Rotavirus diarrhea causes 800,000 Rotavirus diarrhea causes 800,000 deaths/yr deaths/yr
Rotavirus vaccine would save livesRotavirus vaccine would save lives Peyer’s patch hypertrophy (i.e. it works)Peyer’s patch hypertrophy (i.e. it works) Resultant intussusception…..Resultant intussusception….. Rotashield WITHDRAWN 1999Rotashield WITHDRAWN 1999 Merck’s Rotateq: bovine and less Merck’s Rotateq: bovine and less
intussusception, and ACIP/CDC recommend intussusception, and ACIP/CDC recommend it! it!
GSK’s Rotarix: European rival vaccine GSK’s Rotarix: European rival vaccine (new) (new)

““Meniscus” “Coiled Meniscus” “Coiled Spring”Spring”

MECKEL’S MECKEL’S DIVERTICULUMDIVERTICULUM
TYPICAL STORY TYPICAL STORY Rule of TWOsRule of TWOs 2 years old, 2% of pop2 years old, 2% of popnn 1 out of 2: major LGIB 1 out of 2: major LGIB
pedspeds 2 feet from IC junction2 feet from IC junction Range 2-200cm from IC Range 2-200cm from IC
jn. jn. 2 mucosal types2 mucosal types Type and cross for 2 unitsType and cross for 2 units 2 serial Hgb at least2 serial Hgb at least Consider 2 linesConsider 2 lines
REALITYREALITY Age range greaterAge range greater They don’t ALL bleedThey don’t ALL bleed Blood loss may suggest Blood loss may suggest
more minor causes more minor causes Multiple visits comonMultiple visits comon Polyp history negativePolyp history negative Lower GI scope negativeLower GI scope negative Diagnosis is difficultDiagnosis is difficult Cancers ?Cancers ?

A CASEA CASE 47 yo male: CC: crampy abdominal pain47 yo male: CC: crampy abdominal pain VS: 245/160 88 22 98.9VS: 245/160 88 22 98.9 Exam unremarkable, Abdo UTZ Exam unremarkable, Abdo UTZ
unremarkable, post pain meds BP decreasedunremarkable, post pain meds BP decreased Chem 7, CBC, LFTs all normalChem 7, CBC, LFTs all normal 210/140, given HCTZ, passed on DIP U/A pend210/140, given HCTZ, passed on DIP U/A pend
Nursing intake hx: Meckel’s Diverticulum Nursing intake hx: Meckel’s Diverticulum found age 12 (not in physician note) found age 12 (not in physician note)

QUESTIONSQUESTIONS
Dip U/A negative except 1+ protein Dip U/A negative except 1+ protein 25 mg of HCTZ: Will that work 25 mg of HCTZ: Will that work
here? here? More history that you’d like?More history that you’d like? Meckel’s and HTN: Any link?Meckel’s and HTN: Any link? Is UTZ enough of a work up?Is UTZ enough of a work up?
THE OUTCOME WAS:THE OUTCOME WAS:

PARAGANGLIONIC PARAGANGLIONIC PHEOCHROMOCYTOMAPHEOCHROMOCYTOMA


PHEO: RULE OF 10sPHEO: RULE OF 10s
10% malignant 10% malignant 10% bilateral10% bilateral 10% extra-adrenal10% extra-adrenal 10% calcified10% calcified 10% children10% children 10% familial10% familial Talked about 10 TIMES more Talked about 10 TIMES more
often than clinically foundoften than clinically found

J Gastrointest Surg. 2011 Jan;15(1):101-9. doi: 10.1007/s11605-010-1312-x. Epub 2010 Sep 8.
Neuroendocrine tumors of Meckel's diverticulum: lessons from a single institution study of eight cases. Poncet G1, et al
INTRODUCTION: Endocrine tumors of Meckel's diverticulum are rare. Their clinical and pathological characteristics are not well known, making it difficult to assess the best strategy for therapeutic management. MATERIALS AND METHODS: Eight cases of endocrine tumors of Meckel's diverticulum, submitted to surgical resection in our institution between 1977 and 2009, were studied. Clinical charts were reviewed; classification, grading, and staging were performed according to recent international recommendations. Five cases, including two associated with the carcinoid syndrome, were revealed by mesenteric mass or liver metastases; three cases were diagnosed incidentally at laparotomy or laparoscopy.RESULTS: All cases presented as typical well-differentiated midgut endocrine tumors. Five cases were associated with mesenteric lymph node metastases; three presented with liver metastases. Seven cases were classified as well-differentiated endocrine carcinomas, one as well-differentiated endocrine tumor of benign behavior. DISCUSSION: All tumors >1 cm, but one, had regional or distant disease. All patients had complete surgical resection of the primary. One patient deceased after 25 months; the others were alive after 12-101 months. CONCLUSION:In conclusion, endocrine tumors of Meckel's diverticulum are rarely symptomatic and often diagnosed at an advanced stage. All tumors measuring more than 1 cm in diameter must be resected according to oncological principles.


IF HALF OF LGIB IN IF HALF OF LGIB IN PEDS ARE MECKEL’S, PEDS ARE MECKEL’S,
WHAT ARE THE WHAT ARE THE OTHER CASES ?OTHER CASES ?
Motrin (ibuprofen) induced UGIB with Motrin (ibuprofen) induced UGIB with BRBPR or melena BRBPR or melena
AVM’s : Osler-Weber-Rendu AKA HHTAVM’s : Osler-Weber-Rendu AKA HHT Peutz-Jueger SyndromePeutz-Jueger Syndrome Gardener’s and other familial polyposesGardener’s and other familial polyposes Kids that are anticoagulated or on Kids that are anticoagulated or on
steroids with UGIBs steroids with UGIBs

APPY MIMICSAPPY MIMICS
All that moans in the RLQ All that moans in the RLQ is not acute appendicitis !is not acute appendicitis !

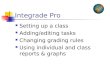
EPIPLOIC EPIPLOIC APPENDAGITISAPPENDAGITIS

EPIPLOIC EPIPLOIC APPENDAGITISAPPENDAGITIS
More L than R (more a mimic of More L than R (more a mimic of diverticulitis)diverticulitis)
Sudden onsetSudden onset More localizedMore localized Benign course with less fever, N, VBenign course with less fever, N, V No migrationNo migration Remains a justification for CT as an Remains a justification for CT as an
emerging NONSURGICAL mimicemerging NONSURGICAL mimic Ovoid with enhanced rim (1.5-3.5 cm…Ovoid with enhanced rim (1.5-3.5 cm…
small)small) Ultrasound diagnosis also possibleUltrasound diagnosis also possible
Son HJ J Clin Gastro 34(4):445 2002 & also Son HJ J Clin Gastro 34(4):445 2002 & also Legome EL J Emerg Med 22(1):9 2002 Legome EL J Emerg Med 22(1):9 2002

MESENTERIC ADENITISMESENTERIC ADENITIS
5-15 years of age5-15 years of age A commonA common peds appy mimic!peds appy mimic! Self limitedSelf limited Pain stays diffusePain stays diffuse Fever commonFever common Viral history variableViral history variable Diagnosis of EXCLUSION only Diagnosis of EXCLUSION only

MESENTERIC ADENITIS MESENTERIC ADENITIS UTZUTZ
Short axis < 5mmShort axis < 5mm Cluster of 3 or moreCluster of 3 or more R/O lymphoma…R/O lymphoma… Adults with nodesAdults with nodes are often still appy!are often still appy! Need to see theNeed to see the appendix clearly toappendix clearly to avoid missing appy….avoid missing appy….
Hernandez JA et al, Ped Radiol 35:292 2005Hernandez JA et al, Ped Radiol 35:292 2005

DOES THIS CHILD HAVE APPENDICITIS? A SYSTEMATIC REVIEW OF CLINICAL PREDICTION RULES IN KIDS WITH ACUTE
ABDOMINAL PAIN
Kulik, D.M., et al, J Clin Epid 66(1):95, January 2013BACKGROUND: The lifetime risk of acute appendicitis, the most common reason for abdominal surgery in children, is 7-9% and perforation rates have been reported to be 12-30%. Because the clinical diagnosis can be challenging in children, several clinical prediction rules (CPRs) have been proposed. METHODS: These Canadian authors, coordinated at the Hospital for Sick Children in Toronto, reviewed the findings of twelve prospective or retrospective derivation (5) or validation (7) studies involving six published CPRs for suspected acute appendicitis in a total of 4,201 children. RESULTS: The CPRs evaluated included the MANTRELS/Alvarado and Modified MANTRELS/Alvarado instruments, the Pediatric Appendicitis Score (PAS), the Modified Lindberg instrument, and CPRs proposed by Lintula and Kharbanda. Sensitivities for appendicitis ranged from 72% to 100% (median 90%), and negative likelihood ratios were reported to be 0-0.34 (median 0.11). Several studies that met criteria for the highest methodologic quality were performed to validate the performance of the PAS and the Alvarado instruments. However, the reported sensitivity of the instruments failed to consistently meet the benchmark that was set (greater than 95%), and it was determined that the PAS and Alvarado rules would have overdiagnosed appendicitis by an average of 35% and 32%, respectively. CONCLUSIONS: This study highlights the limitations of published CPRs for pediatric appendicitis. The authors feel that diagnostic accuracy might be improved by consideration of these instruments in combination with other modalities such as diagnostic ultrasound or a period of observation in the ED. They also cite their potential utility in the process of shared decision-making. 38 references ([email protected] – no reprints)

MANAGING RADIATION EXPOSURE IN CHILDREN--REEXAMINING THE ROLE OF ULTRASOUND IN THE DIAGNOSIS
OF APPENDICITIS
Thirumoorthi, A., et al, J Pediatr Surg 47(12):2268, December 2012BACKGROUND: Risks of computed tomography (CT) radiation exposure for the diagnosis of acute pediatric appendicitis must be balanced against the risks of misdiagnosis when using other imaging methods. Consequently, there is a need to determine the diagnostic value of ultrasound (US) as an alternate imaging method for acute pediatric appendicitis.METHODS: The authors, from New York University Medical Center, conducted a two-center, seven-year, retrospective review of all pediatric US evaluations for appendicitis (365 females, 437 males). The study’s initiation coincided with institution of a new imaging protocol to reduce radiation exposure by use of US as the initial imaging modality, followed by CT when US was non-diagnostic. RESULTS: During the study period, 601 pediatric appendectomies were performed, and 46% were diagnosed using the imaging protocol. US was used to diagnose 72% of the cases, and the remainder were diagnosed with US and CT. The protocol had a 94% sensitivity, a specificity of 98%, a 95% positive predictive value, and a 97% negative predictive value. The missed appendicitis rate was 0%, and the negative appendectomy rate was 1.8%. No missed cases of appendicitis were reported in children discharged based solely on ultrasound without surgery. Use of the new protocol increased from 7% in 2003 to 88% in 2010. Although most patients were imaged with ultrasound alone, children over the age of 9 years were significantly more likely than younger children to be evaluated by US followed by CT (79% vs. 21%, p=0.004).CONCLUSIONS: Acute cases of pediatric appendicitis can be accurately identified by US, followed by CT when US results are non-diagnostic

THE DIFFICULT APPY THE DIFFICULT APPY DXDX
Appy in pregnancy (does it move?)Appy in pregnancy (does it move?) ImmunocompromisedImmunocompromised Children (hence peds GI talk)Children (hence peds GI talk) ElderlyElderly Atypical presentationAtypical presentation Retrocecal AppyRetrocecal Appy Perforated AppyPerforated Appy Intermittent Appy ?Intermittent Appy ? Partially treated Appy? Partially treated Appy?
THE THE
EARLY EARLY A P P YA P P Y