Embed Size (px)
Citation preview
PEDIATRIC CARDIOLOGY PEDIATRIC CARDIOLOGY in the EDin the ED
Naminder Sandhu Naminder Sandhu & Roger Galbraith& Roger GalbraithOctober 27, 2011October 27, 2011
OBJECTIVES• Approach to the infant/neonate presenting with • Shock• CHF• Cyanosis
• Approach to children presenting with • Syncope• Palpitations• Chest pain
• Approach to the child with known CHD• Tips for looking at CXRs and ECGs
Pediatric ECGs
• Why do we do them?– Chest pain, suspected dysrhythmia, seizure,
syncope, drug exposure, electrical burns, abN lytes
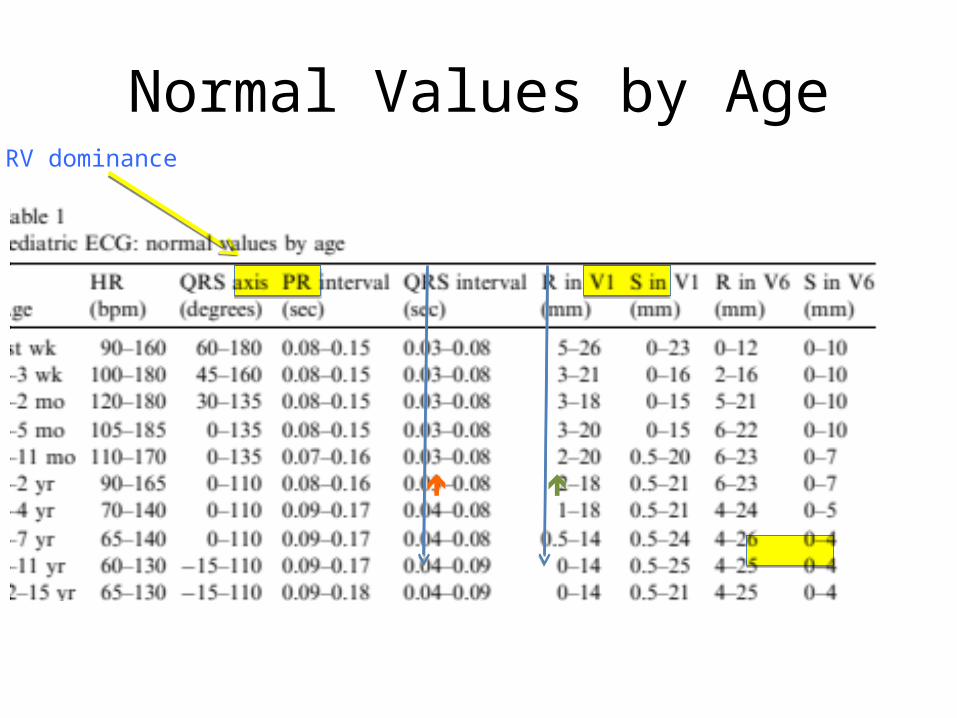
RV dominance
Normal Values by Age
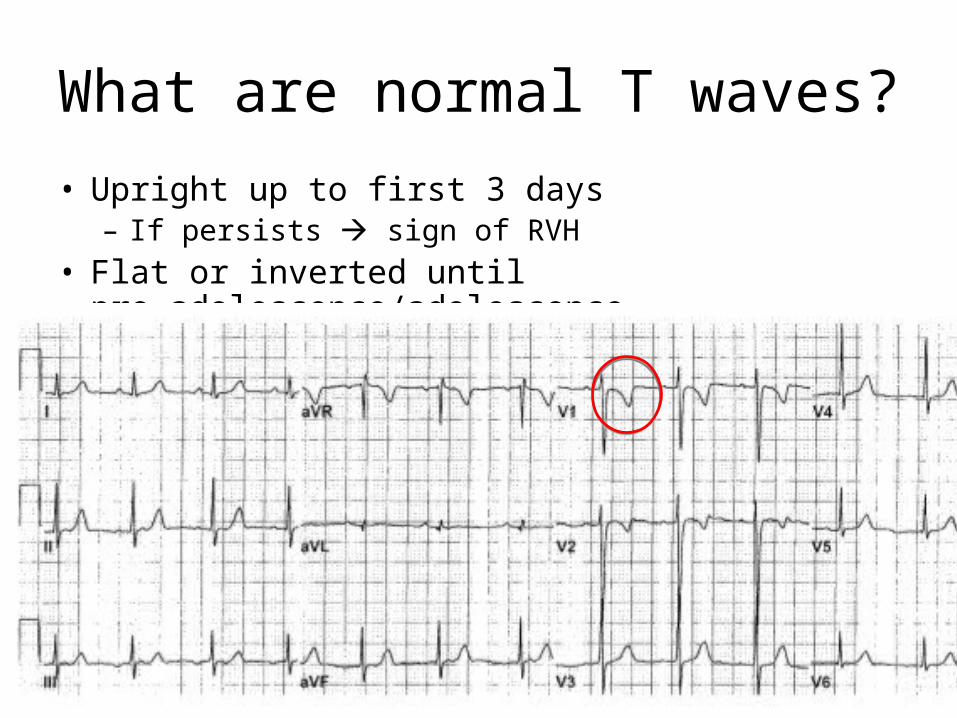
What are normal T waves?
• Upright up to first 3 days– If persists sign of RVH
• Flat or inverted until pre-adolescence/adolescence
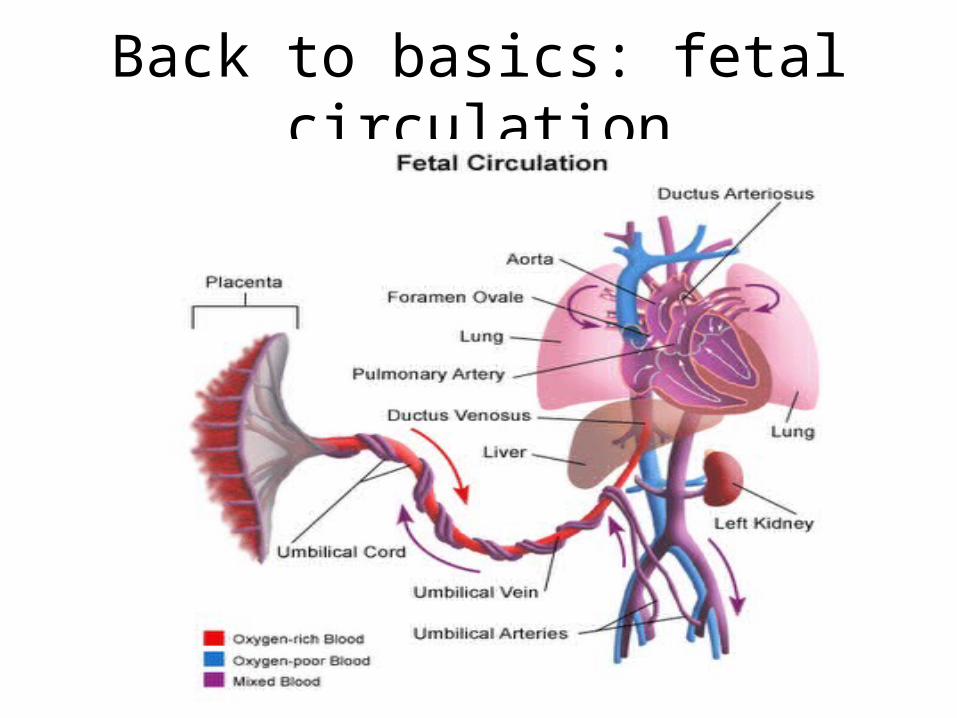
Back to basics: fetal circulation
And now for some cases...
Group 1:Alyssa JenErikGeoff
Group 2:Kristen JoeKipKasiaSean
Group 3:ChrisJason PujaJasmin
Group 4:PingAshleaMichaelAdam
Group 5:Russ MeiraMarshallJeff
CASE 1
• 3 week old with dyspnea, poor feeding• Brought to ED by mother for rapid breathing
and poor breast feeding, worsening over past few days
• Previously well with unremarkable prenatal history
• Becoming more lethargic (not interested in feeding)
CASE 1
• Afebrile, HR 180, RR 80, BP 85/50, sats 88%
• What is your broad ddx for neonatal shock?
Ddx cardiogenic shock
• Myocardial dysfunction– Myocarditis/pericarditis– Sepsis
• Arrhythmias – SVT
• Obstructed/impaired forward flow– AS, Ao Coarct, HLH
• Umm… why is the infant presenting now??
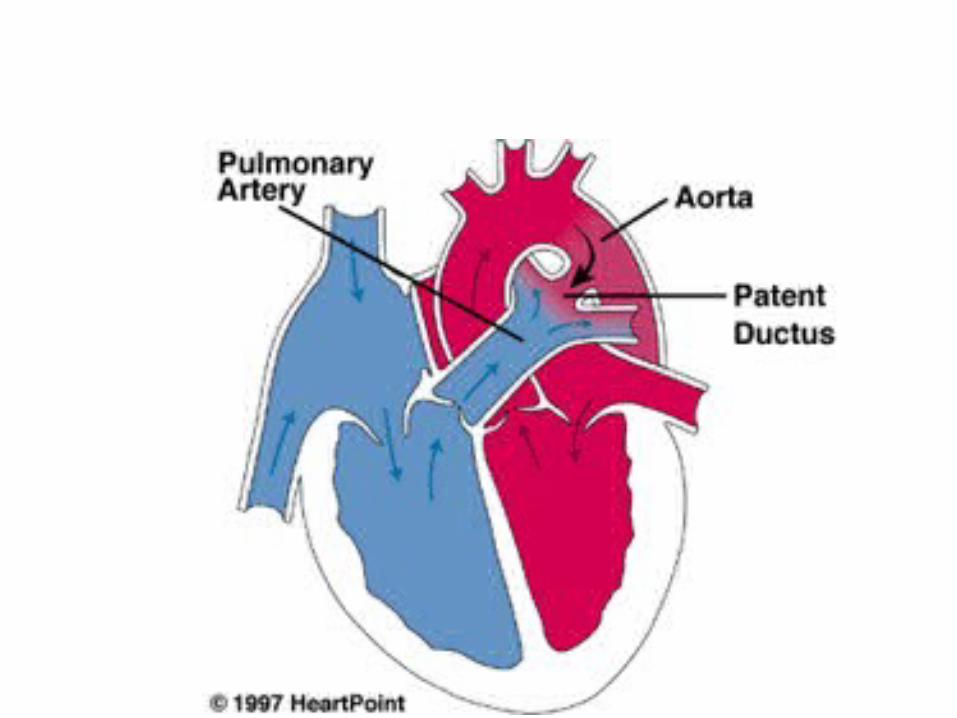
When does the duct close??
• Functional closure within several hours; anatomic closure up to 2 – 3 weeks
• Term infants: – 50% by 24hrs– 90% by 48hrs
• by 4 days in nearly all healthy infants prems
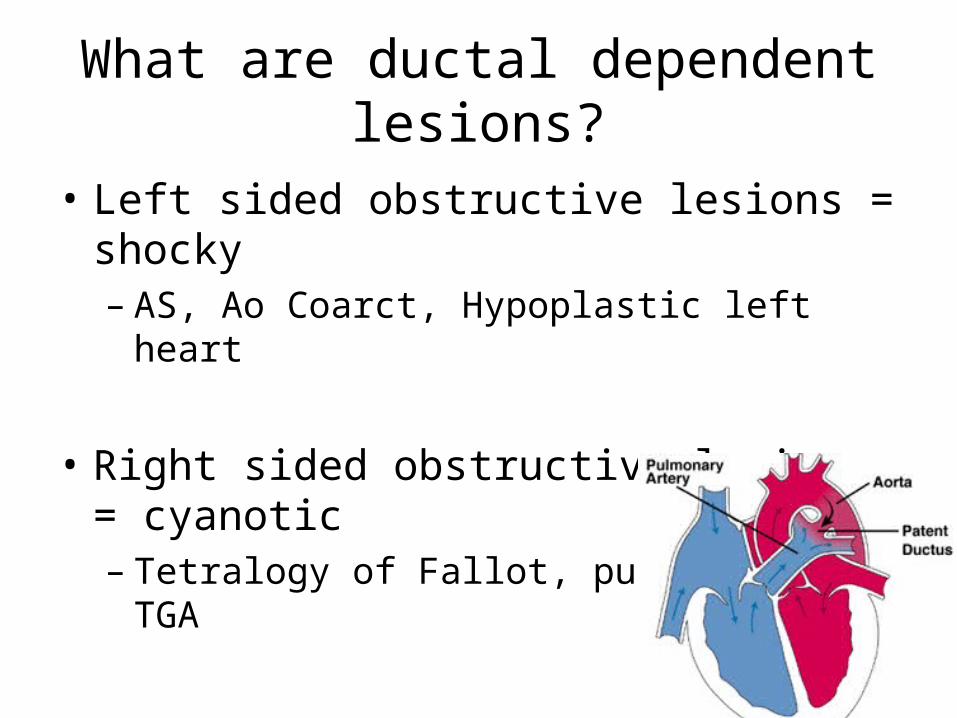
What are ductal dependent lesions?
• Left sided obstructive lesions = shocky– AS, Ao Coarct, Hypoplastic left heart
• Right sided obstructive lesions = cyanotic– Tetralogy of Fallot, pulm stenosis, TGA
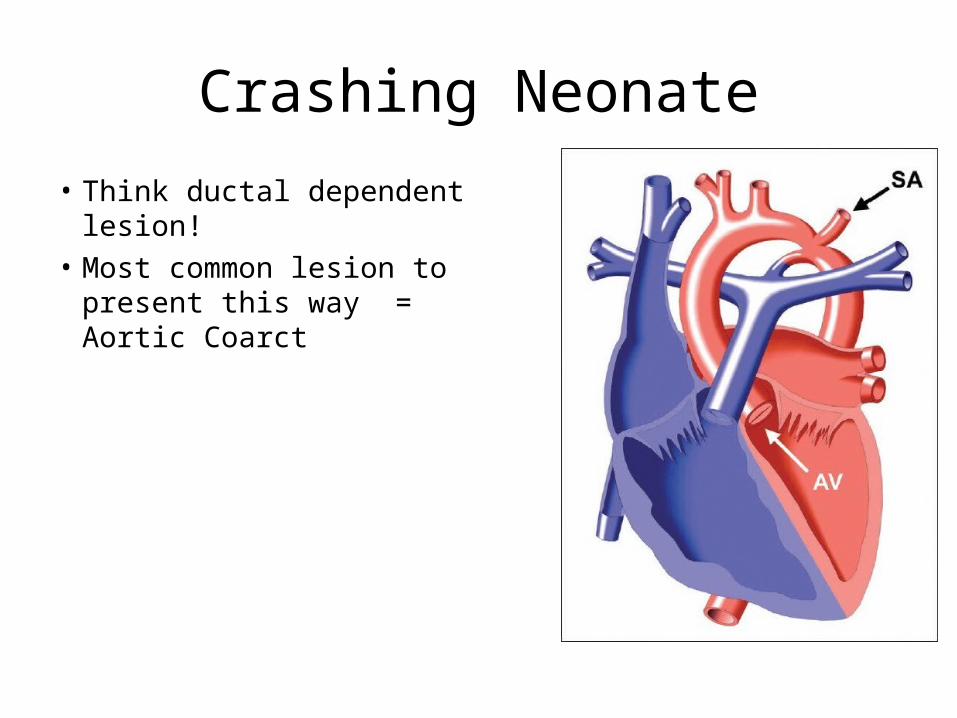
Crashing Neonate
• Think ductal dependent lesion!• Most common lesion to
present this way = Aortic Coarct
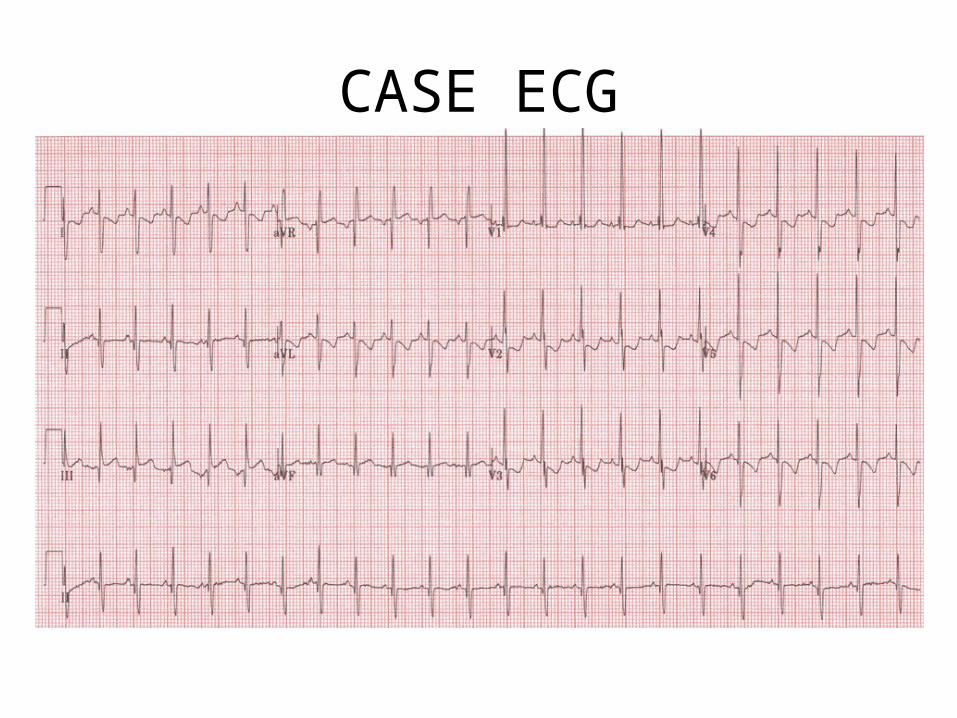
CASE ECG
Management of neonatal shock
• ABCs– Feel for femorals and check BP in four limbs!!!
• Oxygen• IV access* and fluids, investigations and ?abx• PGE1 infusion
• Call cardiology/arrange transport• Also consider Sepsis, Metabolic, NAT, etc.
Alprostadil
• Indications: – Maintenance PDA– Severe PPHTN
• Infusion via peripheral or central line• Dilute to concentration of 10mcg/mL (in
dextrose or NS)• Infuse starting at 0.05mcg/kg/min – max
0.2mcg/kg/min• Effect within minutes
Side effects?
– Apnea– Fever– Flushing– Hypotension– Seizures
CASE 2• 3 month old girl with cyanosis this AM• She has had this happen before but often will resolve
on own• Today after feeding, seemed to be straining, noticed
lips were blue• Newly immigrated from Malaysia, no previous medical
problems• Exam: Sats 76%, RR 40, HR 166– Irritable ++– Deep resps with indrawing– Difficult resp/cardiac exam
Oxygen to the rescue!....
Cyanotic CHD
• Cyanotic heart lesions…. Do I really need to know them???
• ToF 10% CHD• TGA 5%• Tricuspid atresia 1-2%• TAPVR 1%• Truncus arteriosus <1%• Pulm atresia/stenosis <1%• Ebstein’s anomaly <1%
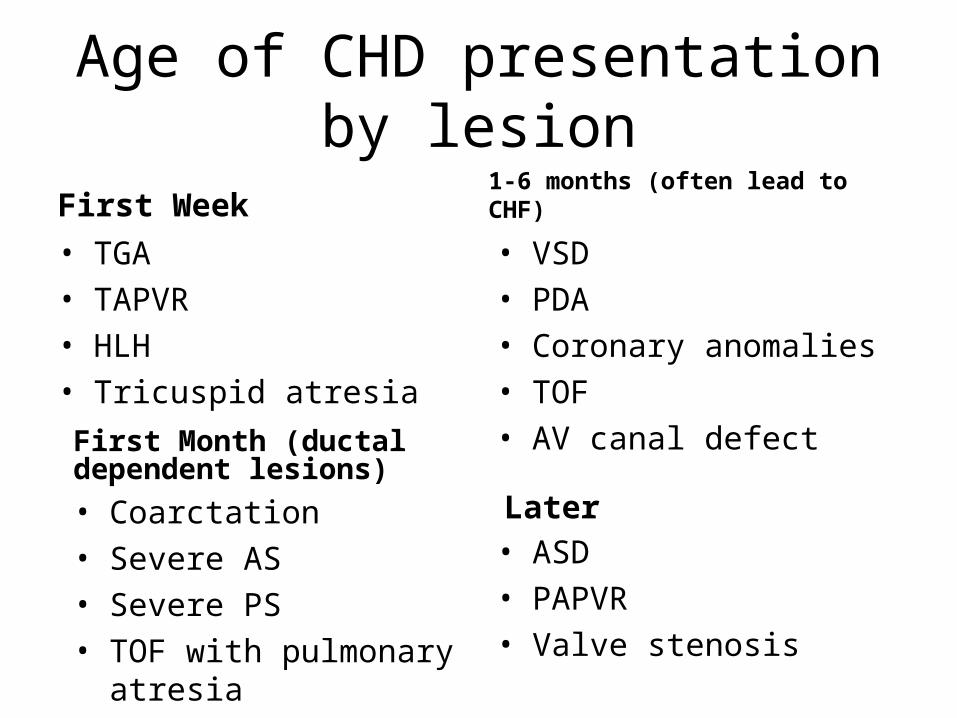
Age of CHD presentation by lesion
First Week• TGA• TAPVR• HLH• Tricuspid atresia
1-6 months (often lead to CHF)• VSD• PDA• Coronary anomalies• TOF• AV canal defectFirst Month (ductal dependent
lesions)• Coarctation• Severe AS• Severe PS• TOF with pulmonary atresia
Later• ASD• PAPVR• Valve stenosis
Is CXR useful?
• Pulmonary vascularity • Shape/size of heart
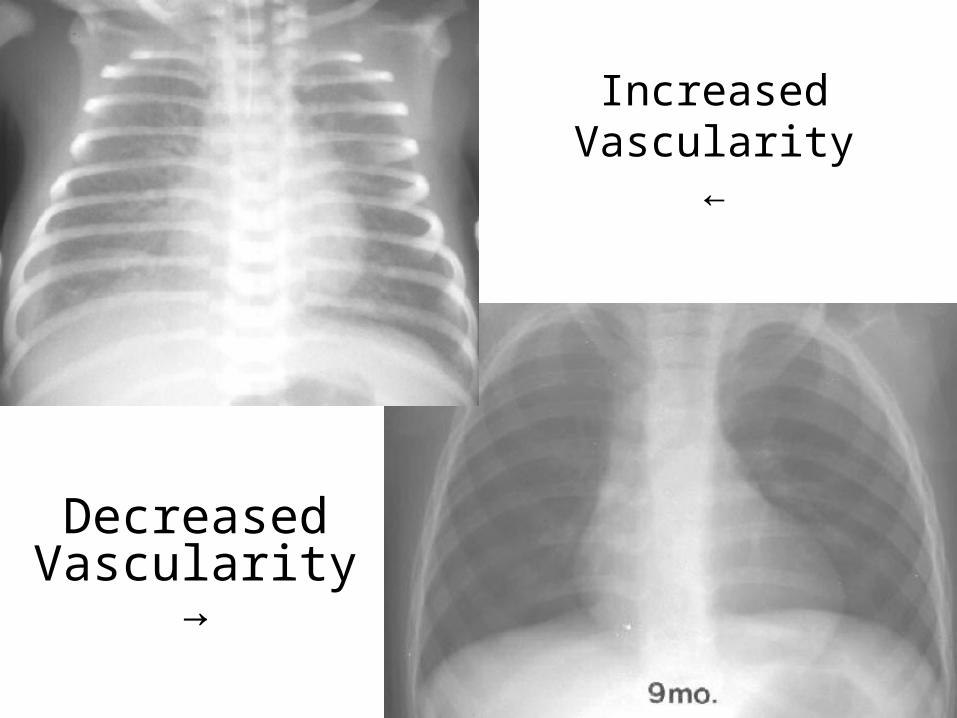
Increased Vascularity←
Decreased Vascularity
→
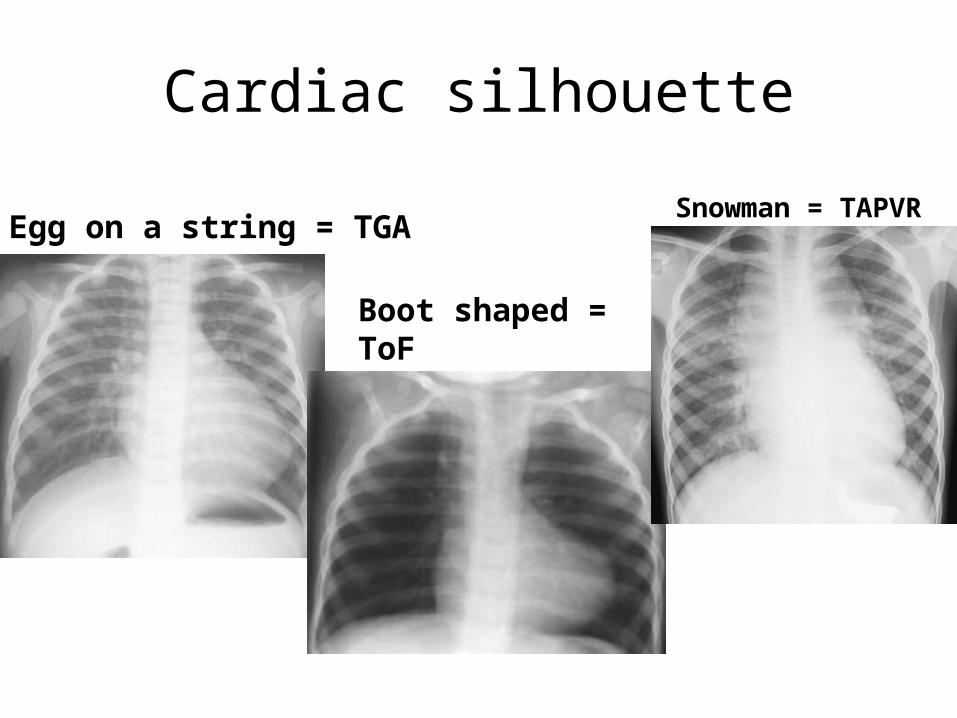
Cardiac silhouette
Egg on a string = TGASnowman = TAPVR
Boot shaped = ToF
So what’s going on with this girl?
TET SPELL
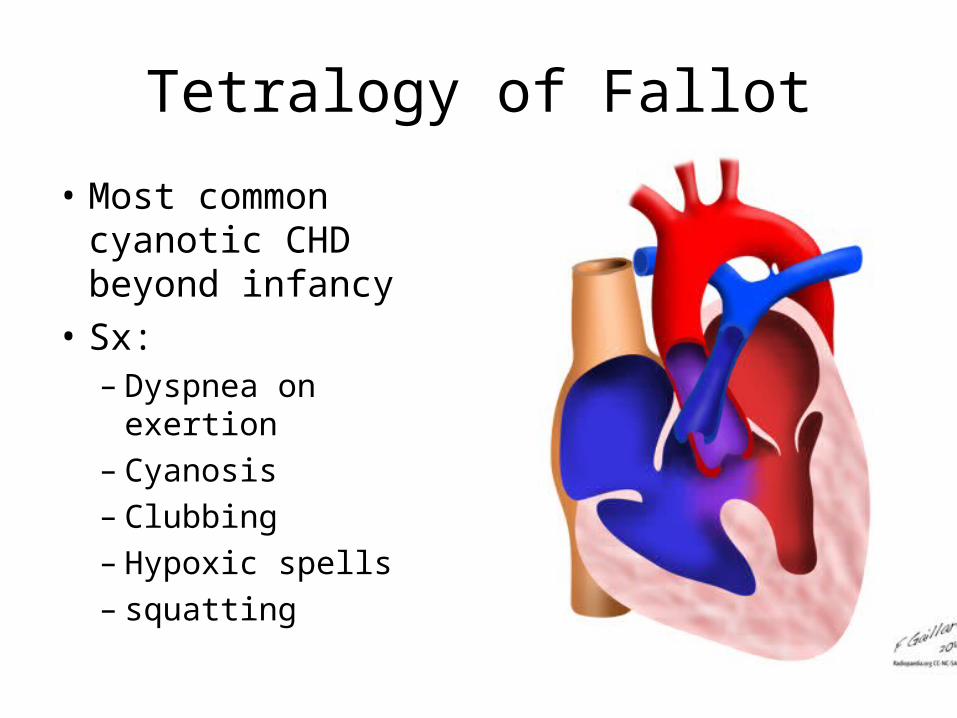
Tetralogy of Fallot
• Most common cyanotic CHD beyond infancy
• Sx:– Dyspnea on exertion– Cyanosis– Clubbing – Hypoxic spells– squatting
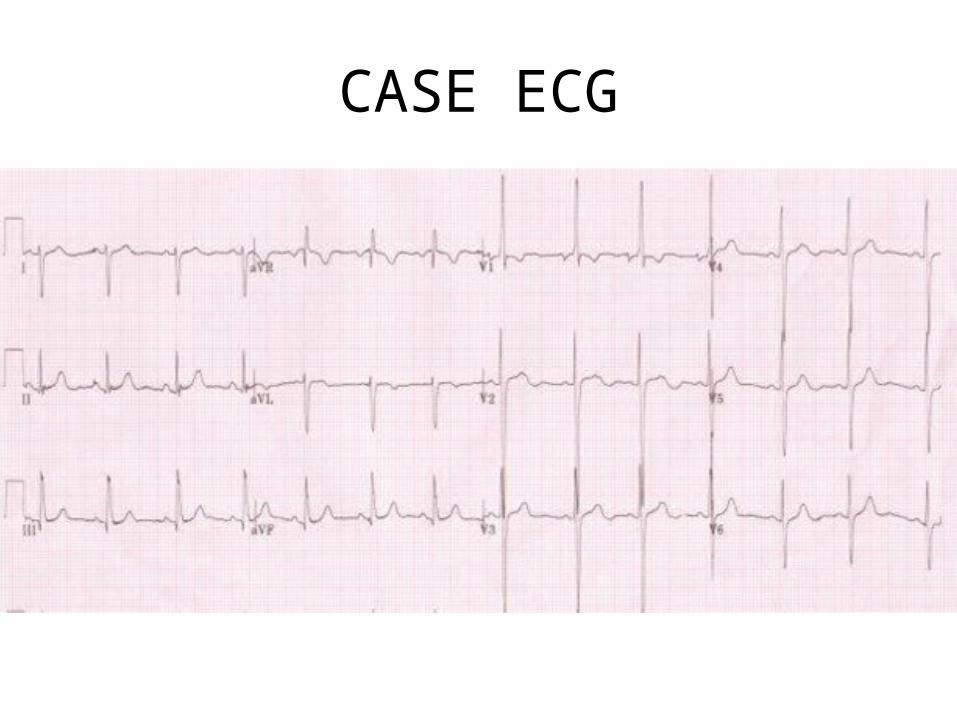
CASE ECG
Tet spell
• Episode of severe hypoxia due to R to L shunting and pulmonary blood flow
• Characteristics:– Paroxysm of hyperpnea– Irritability and prolonged crying– Increasing cyanosis– Decreased intensity murmur
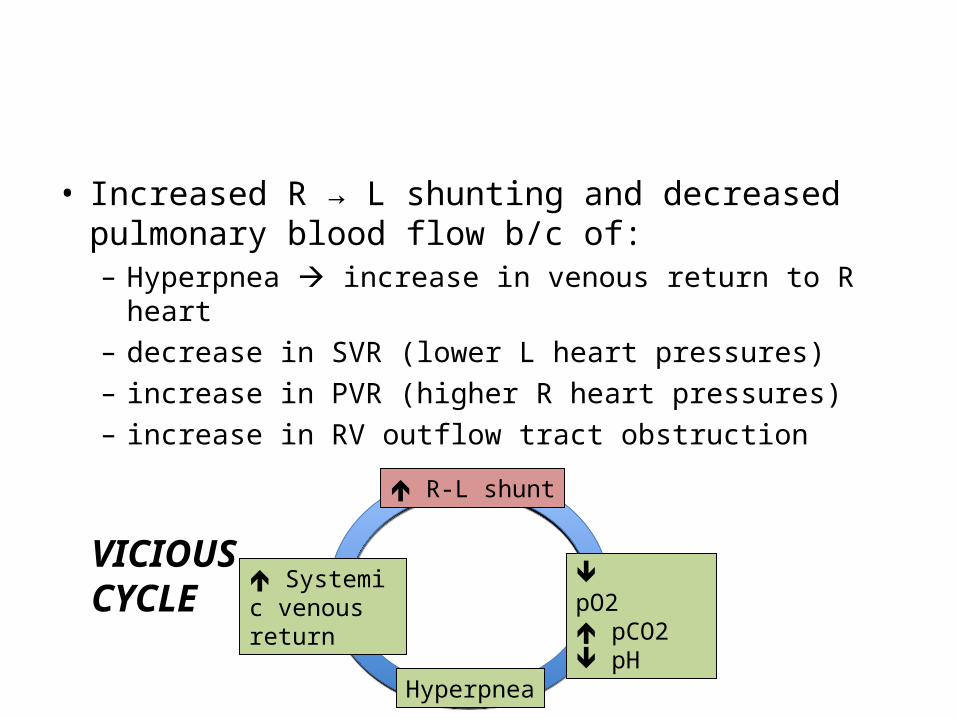
• Increased R → L shunting and decreased pulmonary blood flow b/c of:– Hyperpnea increase in venous return to R heart– decrease in SVR (lower L heart pressures) – increase in PVR (higher R heart pressures)– increase in RV outflow tract obstruction
R-L shunt
pO2pCO2pH
Hyperpnea
Systemic venous return
VICIOUSCYCLE
• Seizures• Syncope• Stroke• DEATH
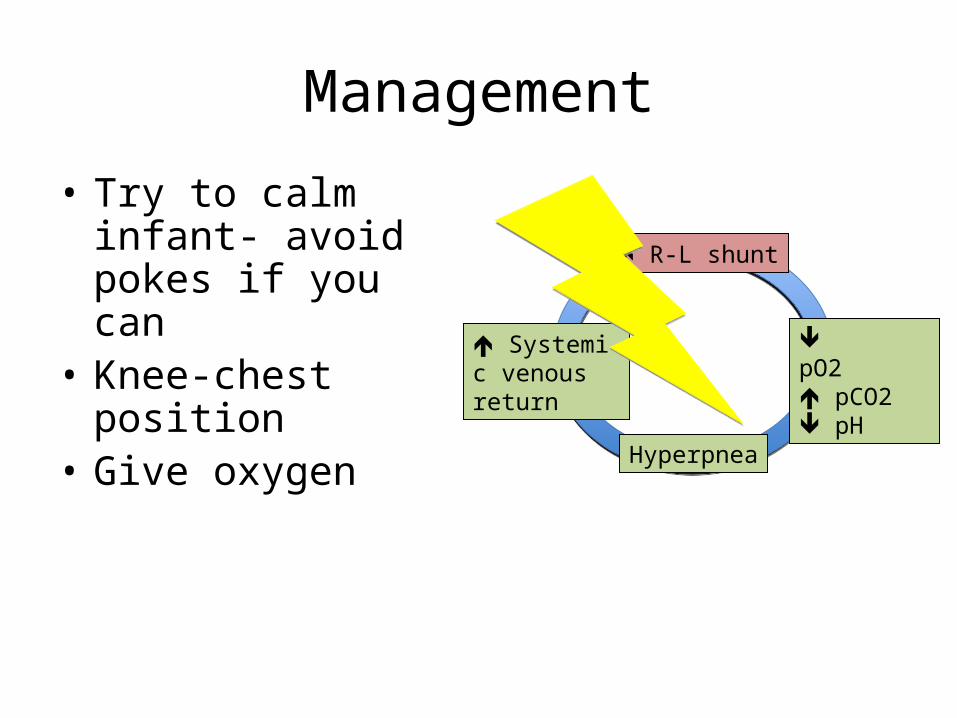
Management
• Try to calm infant- avoid pokes if you can
• Knee-chest position• Give oxygen
R-L shunt
pO2pCO2pH
Hyperpnea
Systemic venous return
Then what??
• IV access & fluids • Sedate with morphine• Bicarbonate• Phenylephrine• Propranolol 0.2mg/kg over 5 min
• ICU/cardiology
CASE 3• 2 month old presenting in December with cough,
congestion, dyspnea, poor feeding x 4 days• Hx– Difficulty feeding, decreased u/o, lethargic– Sick contacts: older brother with cold
• P/E– Afebrile, HR 160, RR70, BP 80/50, sats 90%– Nurses describes infant with nasal congestion, moderate
indrawing
• Sounds like bronchiolitis….but how do you know it’s not CHF??
Presentation: what’s the diff?
• Poor feeding, failure to thrive, tachypnea, diaphoresis, wheeze
• Two bigs: Big heart, big liver• Two fasts: Fast RR, Fast HR
Ddx CHF
• Cardiac – Structural
1) Overcirculation (L-R shunts): VSD, large PDA, AV canal defect
2) Forward flow obstruction: Ao stenosis, CoA, HLH3) Myocardial dysfunction: anomalous coronary (Eg
ALCAPA), myocarditis, cardiomyopathies
– Electrical
• Extracardiac: AVMs
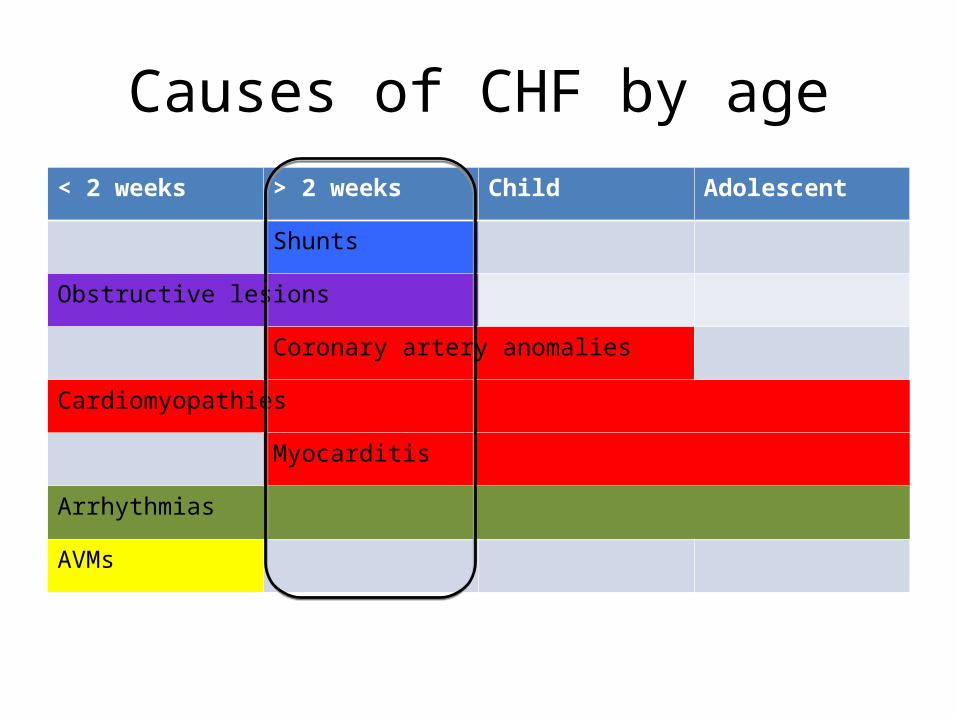
Causes of CHF by age< 2 weeks > 2 weeks Child Adolescent
Shunts
Obstructive lesions
Coronary artery anomalies
Cardiomyopathies
Myocarditis
Arrhythmias
AVMs
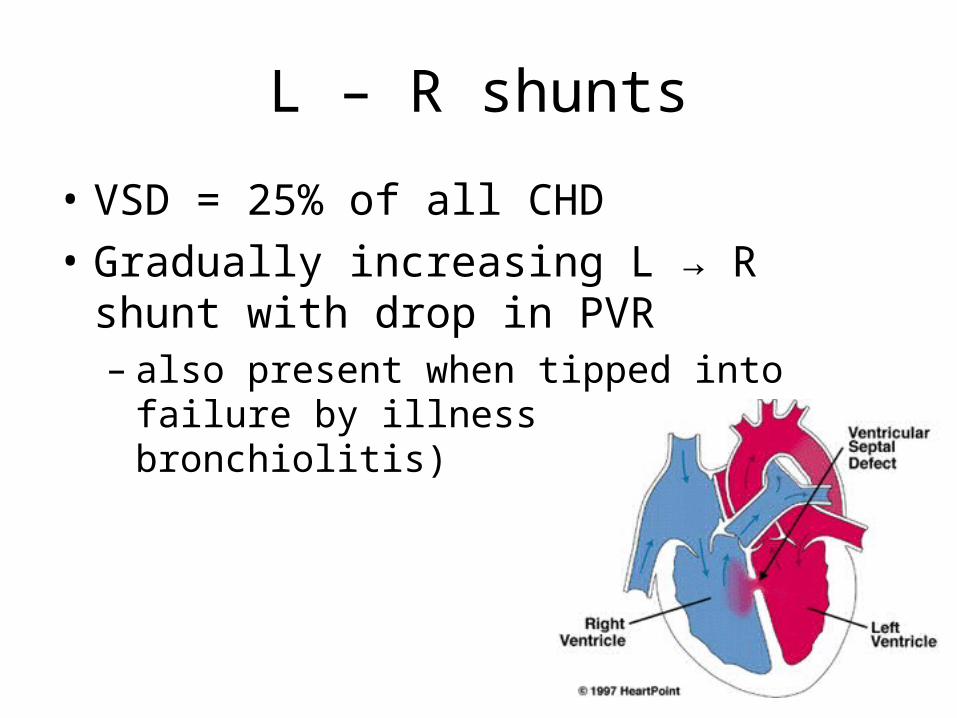
L – R shunts
• VSD = 25% of all CHD• Gradually increasing L → R shunt with drop in
PVR – also present when tipped into failure by illness
(e.g. bronchiolitis)
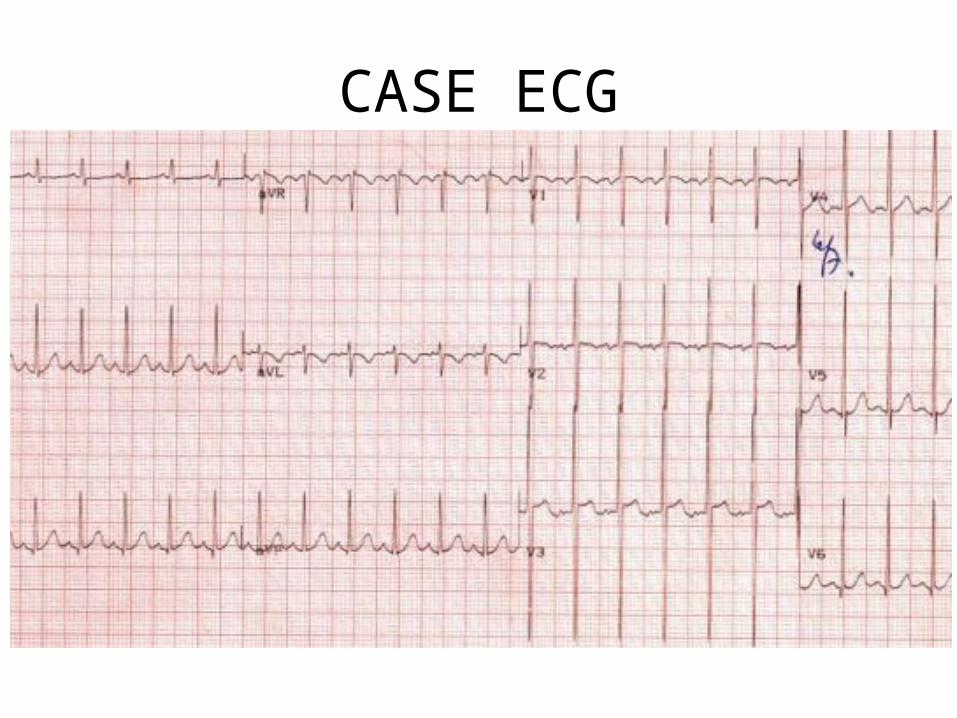
CASE ECG
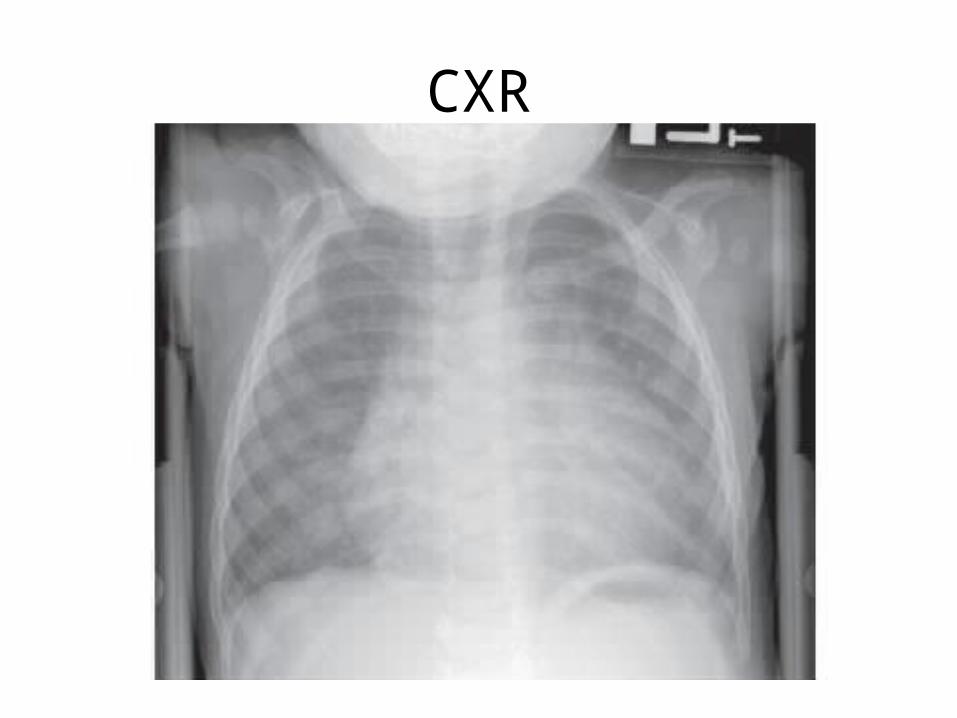
CXR
So what’s the plan?
• Oxygen• IV access • Elevate head of bed• Admit• Supportive therapy for bronchiolitis (that’s a
whole other talk….)• Diuretics
CASE 4• 4 year old complaining that her heart feels funny– Chest pain? Palpitations?
• Started this morning and ?comes and goes; URTI symptoms x 2 days
• Feels “dizzy” sometimes, no syncope• PmHx: known to have an ASD, followed every 1 –
2 years by Cardiology• On exam: HR 128, BP 80/50, RR 30, Sats 95%,
afebrile– Nurse says no acute distress
CASE 4
• Child has nasal congestion• Normal heart sounds, no rubs, no extra
sounds, 2/6 SEM at LUSB• Clear lung fields
• You get an ECG… what worrisome findings are you looking for?
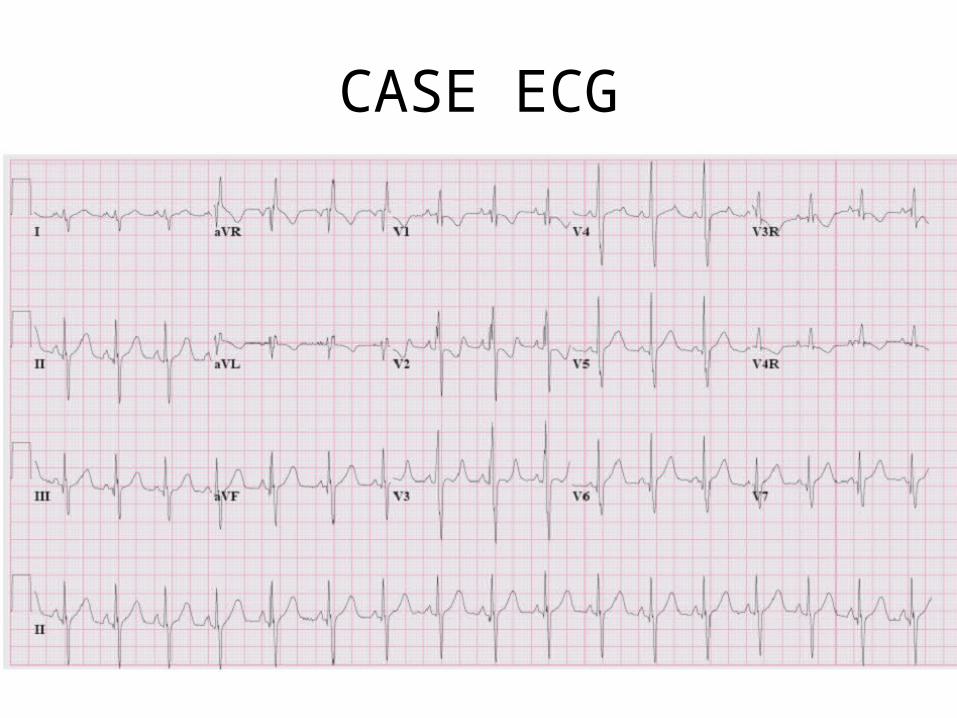
CASE ECG
What’s going on?
• Cardiac– Arrhythmia– Myocarditis/pericarditis– Ischemia, HOCM, etc etc etc
• Non-cardiac
• Then again kid says he feels funny…. You get another ECG
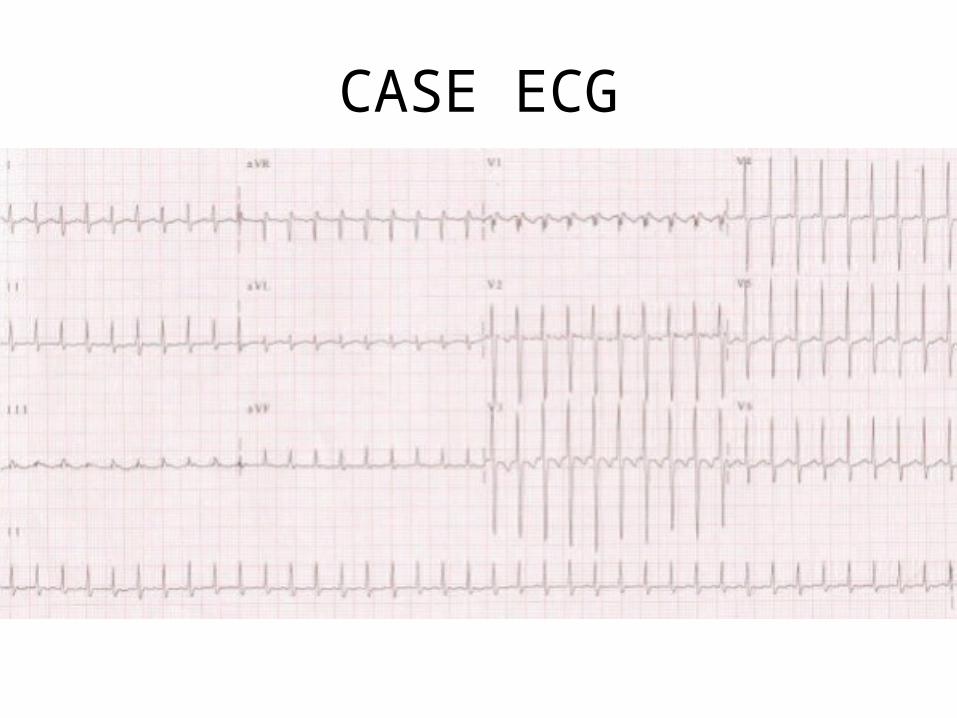
CASE ECG
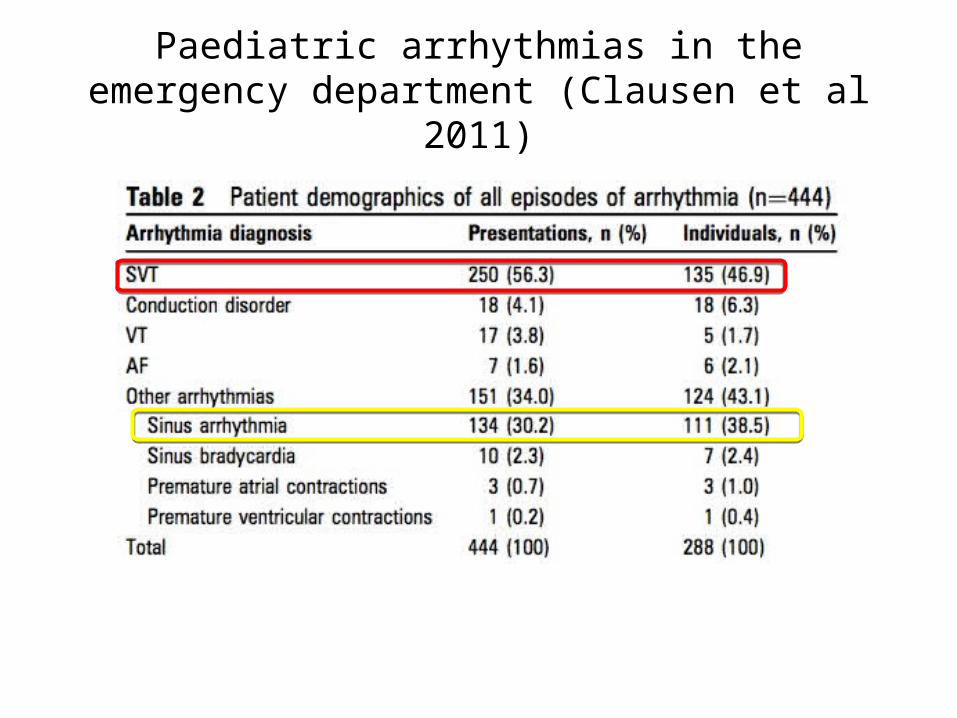
Paediatric arrhythmias in the emergency department (Clausen et al 2011)
SVT
• In infants:– 50% = idiopathic – 25% congenital heart disease – 10-20% WPW syndrome
• HR >220 infants, >180 children• Complications:– Syncope– Shock– CHF
How do you treat stable SVT?
• Stable – Vagal maneuvers: What can you try?
• Blow through plugged straw• Ice on face (don’t cover mouth) – no more than 15 – 30 sec!• Bear down, try to puff up stomach• Stand upside down• Orbital pressure = NO!
– Adenosine • Unstable– SVT with poor perfusion… PALS
Approach syncope…. Similar to adults
• Benign– Orthostatic, vasovagal, breath-holding
• Pathologic– Neuro: Seizures– Cardiac (<5%)
• Myocardial: HOCM, myocarditis• Aortic disease: Aortic stenosis, aneurysm, dissection• Conduction: LQTS, heart block, WPW, ARVD• Coronary artery disease: anomalous origin, aneurysms• Other: pulm HTN, electrolyte abN
SCD in athletes <35 yo
• HCM – 36% • Anomalous origin of a coronary artery – 17% • Myocarditis – 6% • Arrhythmogenic right ventricular dysplasia – 4% • MVP – 4% • Aortic stenosis – 3% • Coronary atherosclerosis – 3%• Other – 12%
Cardiac warning signs
• History of known heart disease• Sudden fainting without prodrome• Syncope during exercise, emotional stimulus• Incontinence during syncope• Family history of sudden death (including
single person MVC, drowning)• Family/personal history of deafness
Long QTS
• What is prolonged QT interval in kids?– Up to 490ms in neonate 440 ms adolescents
• Find a LQT? – Extended electrolytes, drug history– Refer to cardiology urgently– B blockers– ICDs
A shout out to acquired cardiac disease
• Myocarditis• Pericarditis• Endocarditis• Kawasaki disease• Rheumatic heart disease
Myocarditis… same as in adults?
• Spectrum of presentation– Beware non-cardiac presentations eg. Pneumonia,
wheeze not responsive to bronchodilators
• Most common cause dilated CM in kids• Usually infectious, presents in the winter
following viral prodrome
CASE 5• A 4 month old infant presents with increasing cyanosis • Had low grade fever, cough, rhinorrhea and poor
feeding for preceding 4 days• Today developed increased WOB and progressively
worsening cyanosis• Mom says has a history of tricuspid atresia and a “BT
shunt”• T 38.3, HR 170, RR 70, BP 80/50, sats 75%, infant is
crying, cyanotic, grunting and has retractions• Other than change your pants, what should you do???
What could be going on?
• 50% of patients with CHD that presented to the ED required admission
• 10% of those admitted died
• Patients often have complex physiology and are at risk of decompensation for a number of reasons.
• So, yes, you should sweat ...• A little
• Most common presentations of CHD patients to the ED are for:– Respiratory tract infection– Dehydration– CHF– Arrhythmia– Tet spell– Endocarditis
Huh? A what shunt now??
• Used primarily as palliation in defects with single ventricle pathology (ie. HLH, tricuspid atresia)– Try to bypass part of heart to offset workload on
single overworked/impaired ventricle (usu RV)
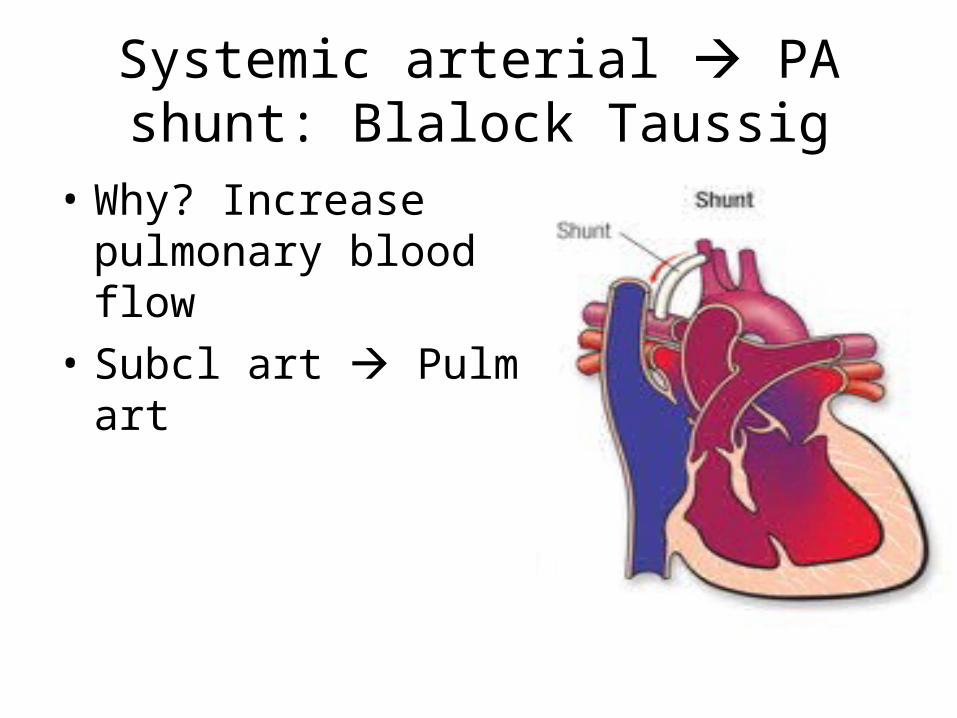
Systemic arterial PA shunt: Blalock Taussig
• Why? Increase pulmonary blood flow
• Subcl art Pulm art
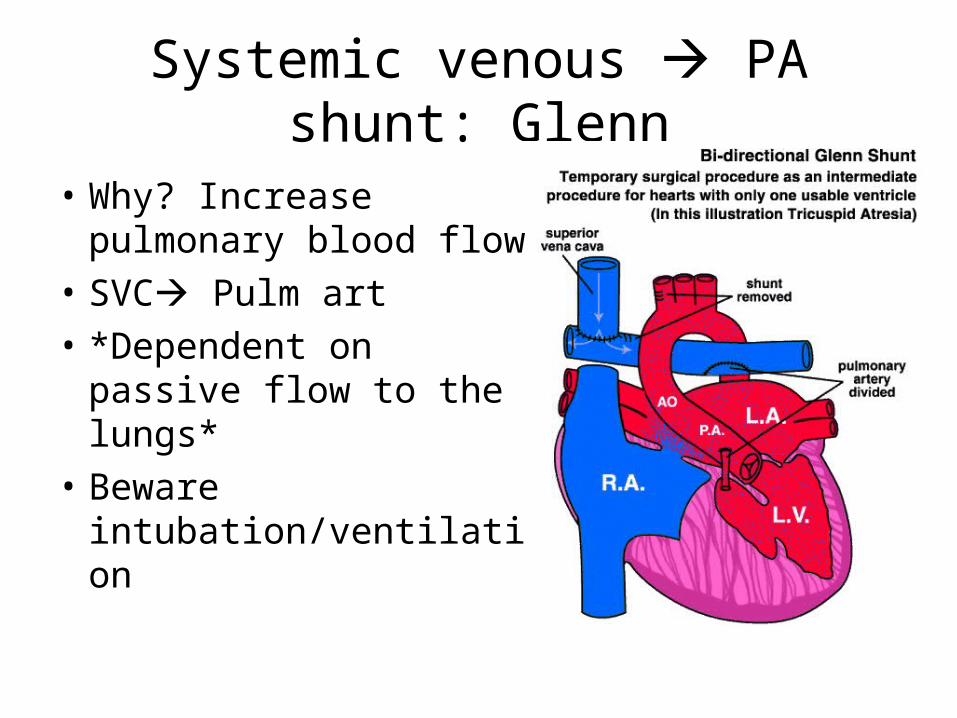
Systemic venous PA shunt: Glenn
• Why? Increase pulmonary blood flow
• SVC Pulm art• *Dependent on passive
flow to the lungs*• Beware
intubation/ventilation
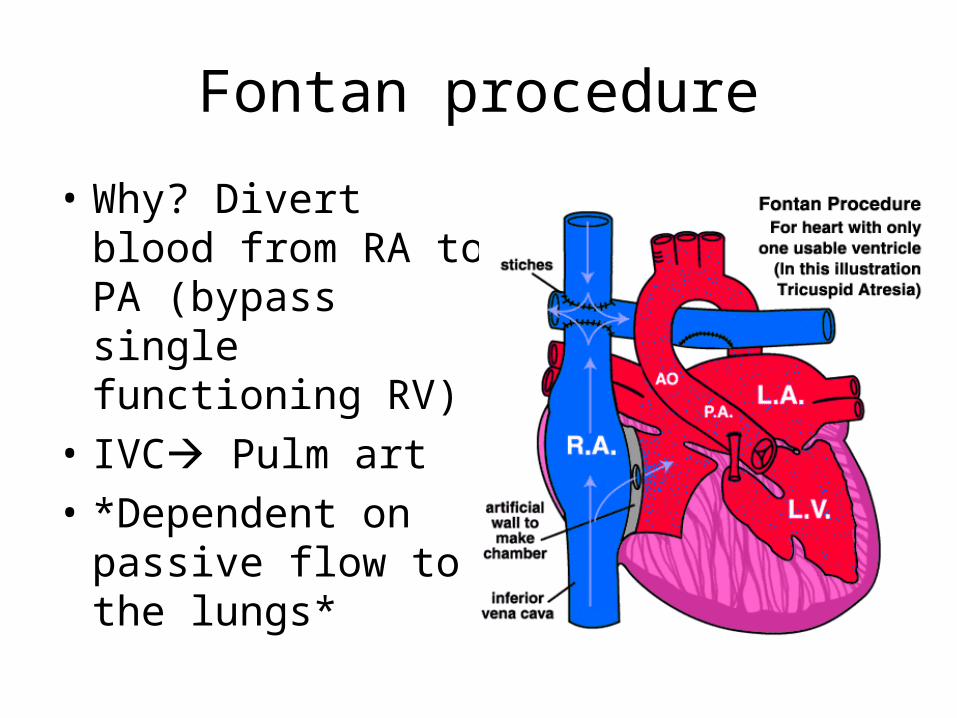
Fontan procedure
• Why? Divert blood from RA to PA (bypass single functioning RV)
• IVC Pulm art• *Dependent on
passive flow to the lungs*
Risks of shunts
• Clotting/ obstruction• Reduced flow (from
hypovolemia/dehydration)• Coronary steal• Over circulation in the pulmonary system– Beware too much oxygen
Bottom line• If not sure, ask the parents what normal sats
should be• You probably wont have enough time or
information to figure out exactly what’s causing their problem- an extensive inpatient work-up is often required
• Low threshold for admission, possibly ICU• Low threshold for cardiology consult• Don’t be stingy with fluids and oxygen, they often
need one or both, just monitor their response closely
Take home points• Shock
– Do a good cardiac exam to r/o cardiogenic shock– If concerned about duct dependent lesion, think PGE1!
• Cyanosis– Try oxygen first… of course– You don’t need to figure out exact CHD – that’s what echo is for– If concerned about duct dependent lesion, think PGE1!
• CHF:– Symptoms may be subtle – exam is important
• JVPs don’t exist in our world – check the liver instead– Always consider on ddx for common presentations eg dyspnea– Different causes based on age (eg. L – R shunts)
Take home points• Palpitations/chest pain/ syncope– Approach similar to adults except chest pain/syncope
rarely cardiac• Acquired heart disease– Most common is myocarditis – keep your eye out for
it– Prevent it by looking our for Kawasaki disease
• Known CHD– If all else fails, ask the family and consult cardiology;
low threshold for admission– Be kind with your fluids and careful with oxygen
Thanks!
• Dr. Roger Galbraith• Dr. Joyce Harder• Drs. Mark Bromley and Jay Green
References
• Emergency Medicine Reports, Jan 2005: 10(1)• Park MK. The Pediatric Cardiology Handbook 3rd
Ed. (2003). Philadelphia: Mosby.• Sharieff GQ et al. The Pediatric ECG. Emerg Med
Clin N Am. 2006; 24: 195-208.• Durani Y et al. Myocarditis and pericarditis in
children. Pediatr Clin N Am 57. 2010; 1281–1303.